
Synergistic Antinociceptive Effects of Indomethacin–Pregabalin and Meloxicam–Pregabalin in Paclitaxel-Induced Neuropathic Pain

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Drugs and Treatment
2.3. Measurement of Antinociceptive Activity
2.3.1. Paclitaxel-Induced Neuropathic Pain Model
2.3.2. Carrageenan-Induced Inflammatory Pain Model
2.4. Assessment of Anti-Mechanical Allodynia Effect
2.5. Data Analysis
2.5.1. Isobolographic Analysis
2.5.2. Statistical Analysis
3. Results
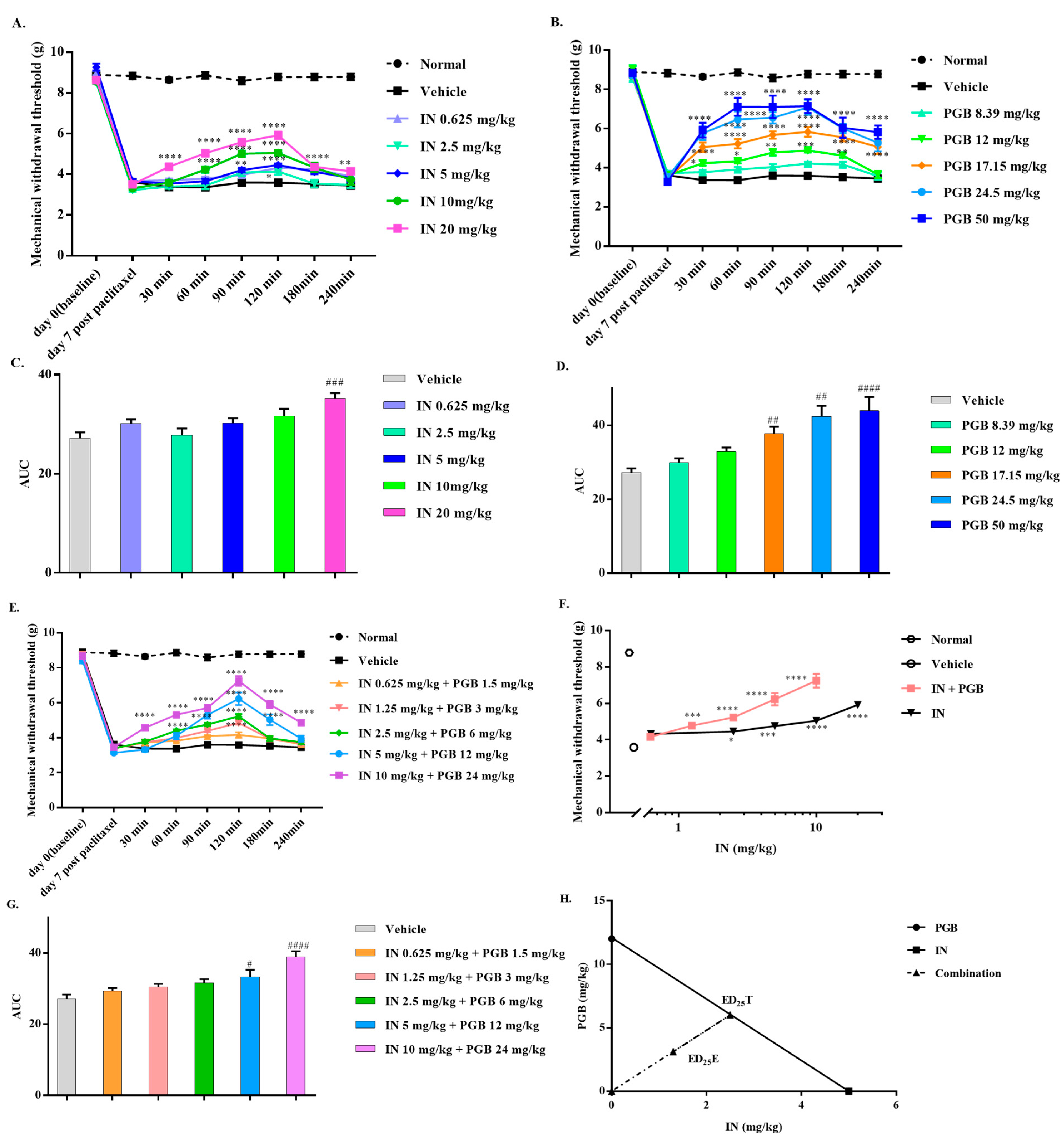
3.1. The Synergistic Antinociceptive Effects of the Combination Treatment of Indomethacin and Pregabalin on Paclitaxel-Induced Neuropathic Pain
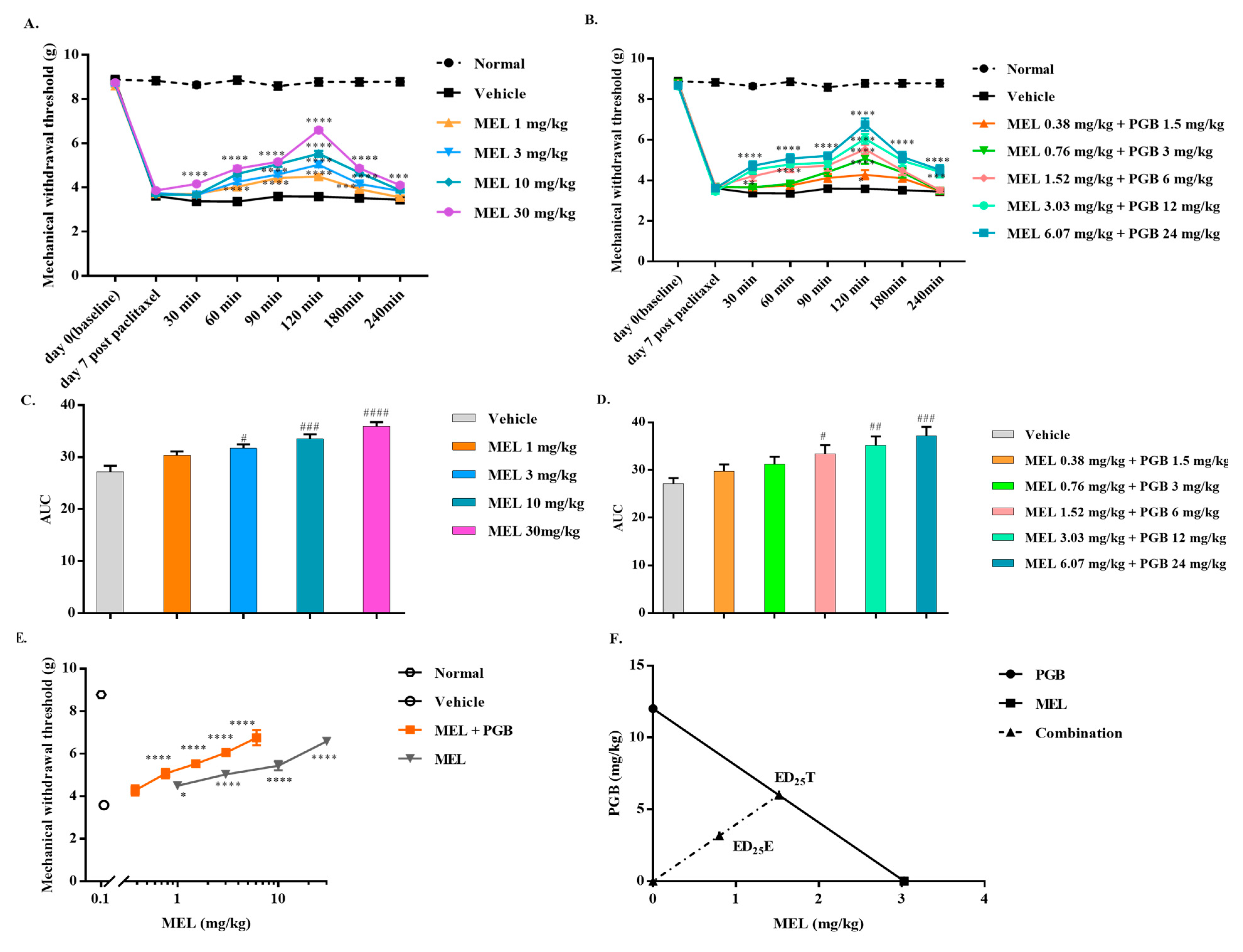
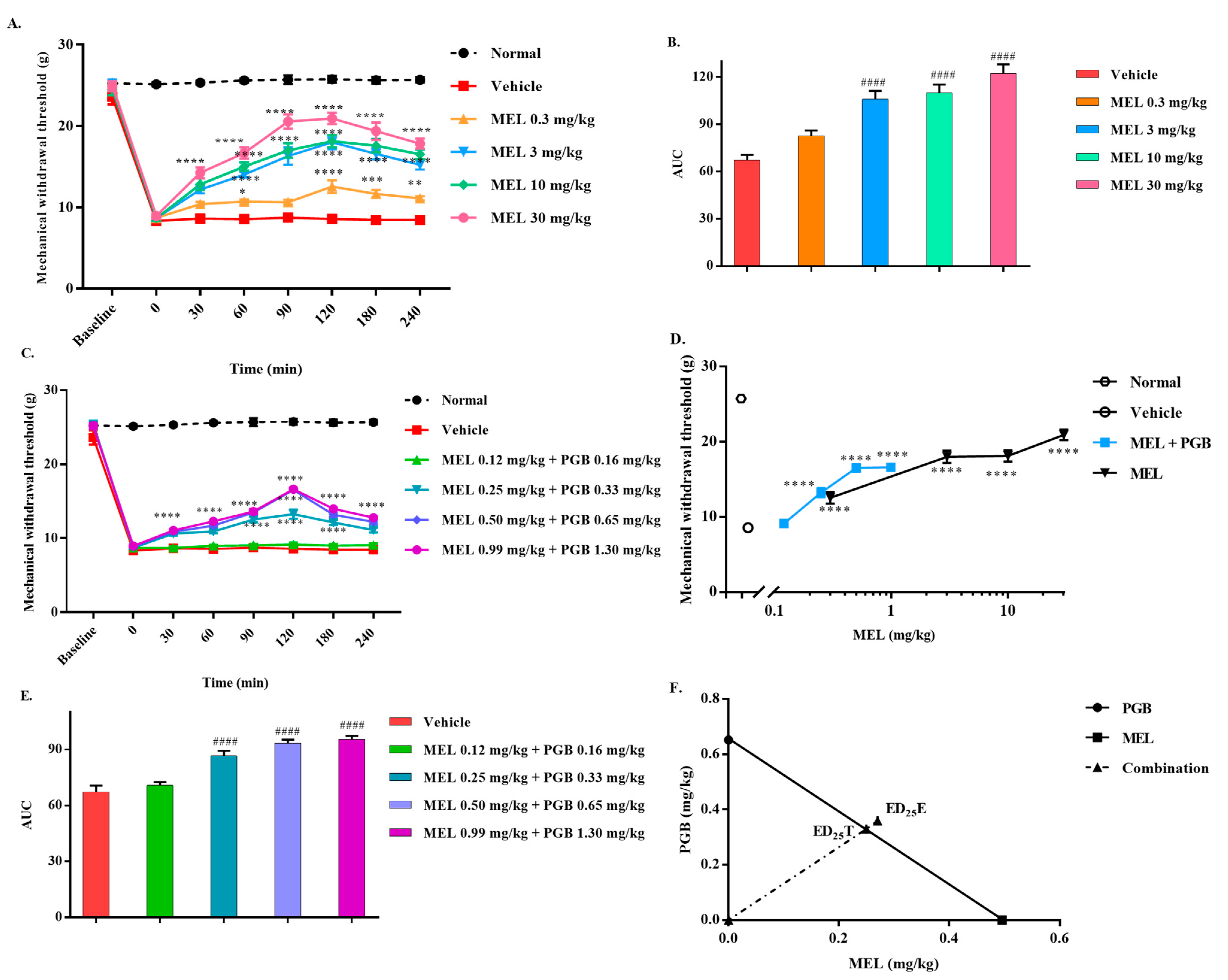
3.2. The Synergistic Antinociceptive Effects of the Combination Treatment of Meloxicam and Pregabalin on Paclitaxel-Induced Neuropathic Pain
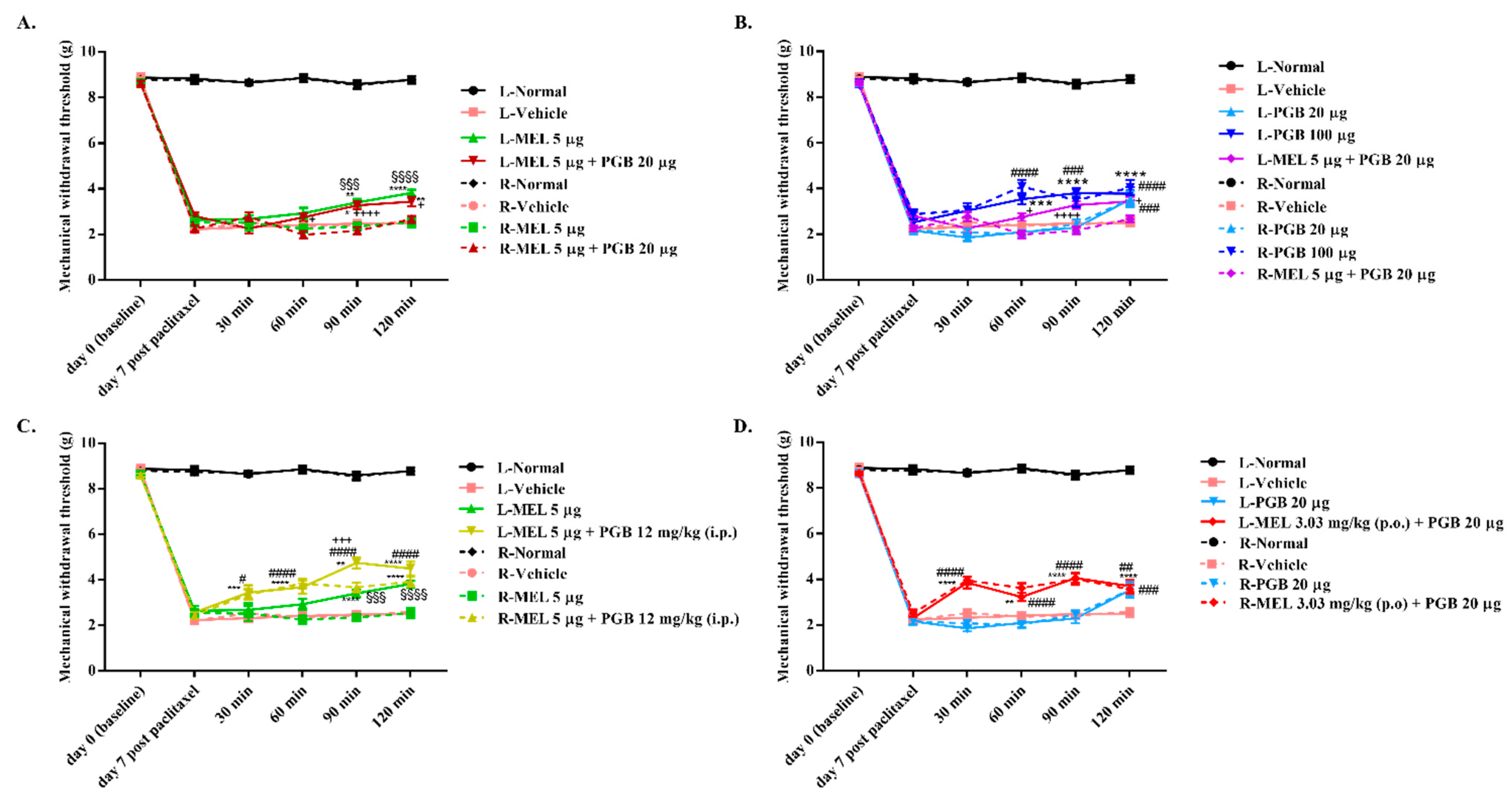
3.3. The Locus of the Antinociceptive Effect Mediated by the Combination of Meloxicam and Pregabalin in Paclitaxel-Induced Neuropathic Pain
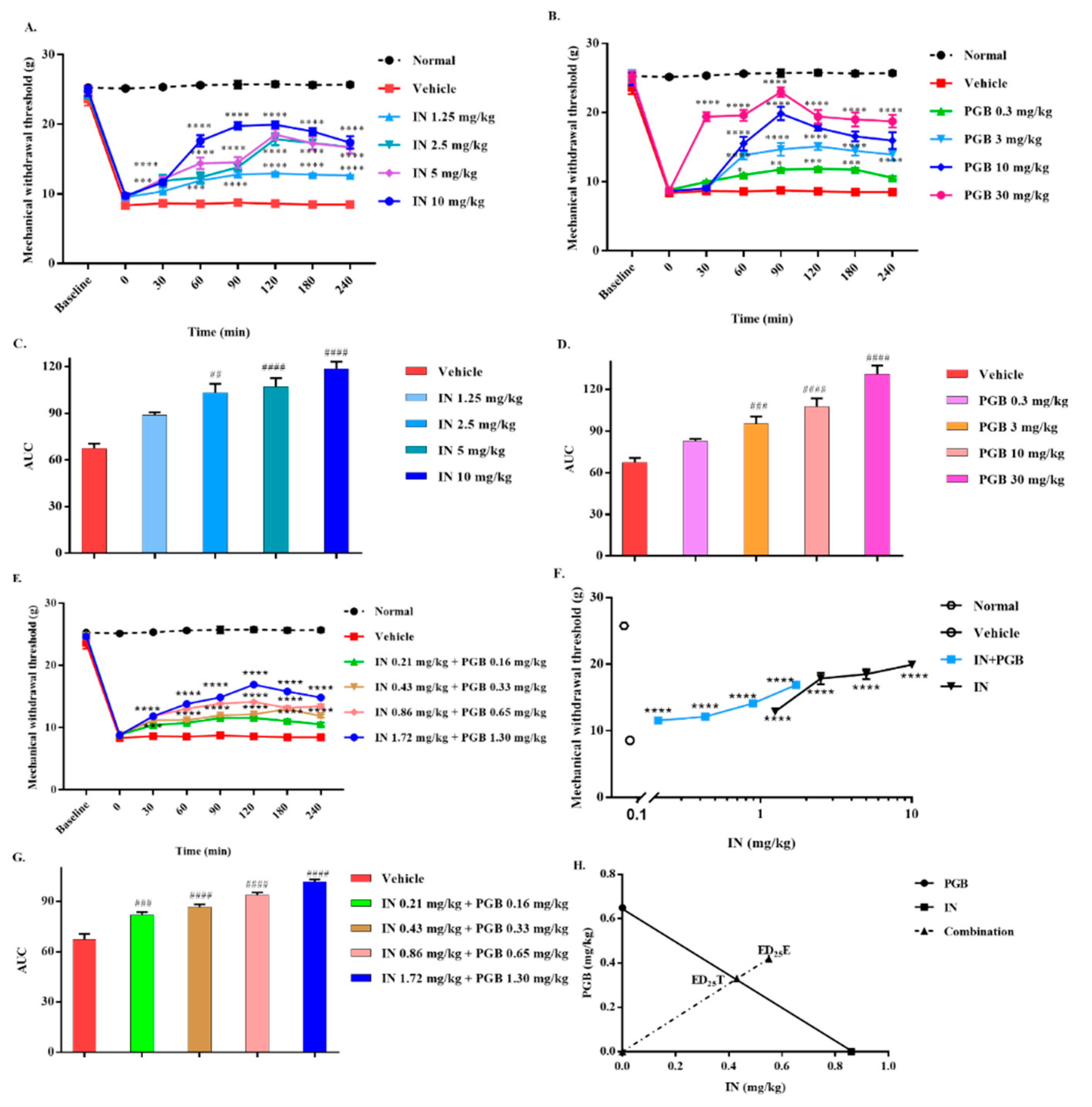
3.4. The Antagonistic Antinociceptive Effects of the Combination Treatment of Indomethacin and Pregabalin in Carrageenan-Induced Inflammatory Pain in Rats
3.5. The Antagonistic Antinociceptive Effects of the Combination Treatment of Meloxicam and Pregabalin in Carrageenan-Induced Inflammatory Pain in Rats
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lu, Y.; Zhang, P.; Zhang, Q.; Yang, C.; Qian, Y.; Suo, J.; Tao, X.; Zhu, J. Duloxetine Attenuates Paclitaxel-Induced Peripheral Nerve Injury by Inhibiting p53-Related Pathways. J. Pharmacol. Exp. Ther. 2020, 373, 453–462. [Google Scholar] [CrossRef] [PubMed]
- Dougherty, P.M.; Cata, J.P.; Cordella, J.V.; Burton, A.; Weng, H.R. Taxol-induced sensory disturbance is characterized by preferential impairment of myelinated fiber function in cancer patients. Pain 2004, 109, 132–142. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.J.; Sedhom, R.; Gupta, A. Chemotherapy-Induced Peripheral Neuropathy. JAMA Oncol. 2019, 5, 750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cata, J.; Weng, H.; Lee, B.; Reuben, J.; Dougherty, P. Clinical and experimental findings in humans and animals with chemotherapy-induced peripheral neuropathy. Minerva Anestesiol. 2006, 72, 151–169. [Google Scholar] [PubMed]
- Cioroiu, C.; Weimer, L.H. Update on Chemotherapy-Induced Peripheral Neuropathy. Curr. Neurol. Neurosci. Rep. 2017, 17, 47. [Google Scholar] [CrossRef]
- Seretny, M.; Currie, G.L.; Sena, E.S.; Ramnarine, S.; Grant, R.; MacLeod, M.R.; Colvin, L.A.; Fallon, M. Incidence, prevalence, and predictors of chemotherapy-induced peripheral neuropathy: A systematic review and meta-analysis. Pain 2014, 155, 2461–2470. [Google Scholar] [CrossRef] [Green Version]
- Gewandter, J.S.; Kleckner, A.S.; Marshall, J.H.; Brown, J.S.; Curtis, L.H.; Bautista, J.; Dworkin, R.H.; Kleckner, I.R.; Kolb, N.; Mohile, S.G.; et al. Chemotherapy-induced peripheral neuropathy (CIPN) and its treatment: An NIH Collaboratory study of claims data. Support. Care Cancer 2020, 28, 2553–2562. [Google Scholar] [CrossRef]
- Dranitsaris, G.; Yu, B.; King, J.; Kaura, S.; Zhang, A. Nab-paclitaxel, docetaxel, or solvent-based paclitaxel in metastatic breast cancer: A cost-utility analysis from a Chinese health care perspective. Clinicoecon. Outcomes Res. 2015, 7, 249–256. [Google Scholar] [CrossRef] [Green Version]
- Beijers, A.J.; Jongen, J.L.; Vreugdenhil, G. Chemotherapy-induced neurotoxicity: The value of neuroprotective strategies. Neth. J. Med. 2012, 70, 18–25. [Google Scholar]
- Onakpoya, I.J.; Thomas, E.T.; Lee, J.J.; Goldacre, B.; Heneghan, C.J. Benefits and harms of pregabalin in the management of neuropathic pain: A rapid review and meta-analysis of randomised clinical trials. BMJ Open 2019, 9, e023600. [Google Scholar] [CrossRef] [Green Version]
- Rivat, C. Neuropathic Pain: When Nerve Lesion Turns off Peripheral Analgesia. Anesthesiology 2016, 125, 627–629. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.Y.; Mi, W.L.; Wu, G.C.; Wang, Y.Q.; Mao-Ying, Q.L. Prevention and Treatment for Chemotherapy-Induced Peripheral Neuropathy: Therapies Based on CIPN Mechanisms. Curr. Neuropharmacol. 2019, 17, 184–196. [Google Scholar] [CrossRef] [PubMed]
- Finnerup, N.B.; Attal, N.; Haroutounian, S.; McNicol, E.; Baron, R.; Dworkin, R.H.; Gilron, I.; Haanpää, M.; Hansson, P.; Jensen, T.S.; et al. Pharmacotherapy for neuropathic pain in adults: A systematic review and meta-analysis. Lancet Neurol. 2015, 14, 162–173. [Google Scholar] [CrossRef] [Green Version]
- Kiguchi, N.; Sakaguchi, H.; Kadowaki, Y.; Saika, F.; Fukazawa, Y.; Matsuzaki, S.; Kishioka, S. Peripheral administration of interleukin-13 reverses inflammatory macrophage and tactile allodynia in mice with partial sciatic nerve ligation. J. Pharmacol. Sci. 2017, 133, 53–56. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.B.; Tran, P.B.; Gillard, S.E.; Hurley, R.W.; Hammond, D.L.; Miller, R.J. Chemokines and glycoprotein120 produce pain hypersensitivity by directly exciting primary nociceptive neurons. J. Neurosci. 2001, 21, 5027–5035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, N.; Inan, S.; Cowan, A.; Sun, R.; Wang, J.M.; Rogers, T.J.; Caterina, M.; Oppenheim, J.J. A proinflammatory chemokine, CCL3, sensitizes the heat- and capsaicin-gated ion channel TRPV1. Proc. Natl. Acad. Sci. USA 2005, 102, 4536–4541. [Google Scholar] [CrossRef] [Green Version]
- White, F.A.; Sun, J.; Waters, S.M.; Ma, C.; Ren, D.; Ripsch, M.; Steflik, J.; Cortright, D.N.; Lamotte, R.H.; Miller, R.J. Excitatory monocyte chemoattractant protein-1 signaling is up-regulated in sensory neurons after chronic compression of the dorsal root ganglion. Proc. Natl. Acad. Sci. USA 2005, 102, 14092–14097. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.Y.; Kam, Y.L.; Oh, J.; Kim, D.H.; Choi, J.S.; Choi, H.Y.; Han, S.; Youn, I.; Choo, H.P.; Yune, T.Y. HYP-17, a novel voltage-gated sodium channel blocker, relieves inflammatory and neuropathic pain in rats. Pharmacol. Biochem. Behav. 2017, 153, 116–129. [Google Scholar] [CrossRef]
- Obreja, O.; Rathee, P.K.; Lips, K.S.; Distler, C.; Kress, M. IL-1 β potentiates heat-activated currents in rat sensory neurons: Involvement of IL-1RI, tyrosine kinase, and protein kinase C. FASEB J. 2002, 16, 1497–1503. [Google Scholar] [CrossRef]
- Kiguchi, N.; Kobayashi, D.; Saika, F.; Matsuzaki, S.; Kishioka, S. Pharmacological Regulation of Neuropathic Pain Driven by Inflammatory Macrophages. Int. J. Mol. Sci. 2017, 18, 2296. [Google Scholar] [CrossRef] [Green Version]
- Cuesta, S.A.; Meneses, L. The Role of Organic Small Molecules in Pain Management. Molecules 2021, 26, 4029. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Bah, M. NSAIDs in the Treatment of Postoperative Pain. Curr. Pain Headache Rep. 2016, 20, 62. [Google Scholar] [CrossRef] [PubMed]
- Moriya, S.; Hasegawa, M.; Inamasu, J.; Kogame, H.; Hirose, Y.; Higashi, R.; Ito, M.; Imai, F. Neuroprotective effects of pregabalin in a rat model of intracisternal facial nerve avulsion. J. Neurosurg. Sci. 2017, 61, 495–503. [Google Scholar] [CrossRef] [PubMed]
- Di Cesare Mannelli, L.; Maresca, M.; Micheli, L.; Farina, C.; Scherz, M.; Ghelardini, C. A rat model of FOLFOX-induced neuropathy: Effects of oral dimiracetam in comparison with duloxetine and pregabalin. Cancer Chemother. Pharmacol. 2017, 80, 1091–1103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abu-Rish, E.Y.; Mansour, A.T.; Mansour, H.T.; Dahabiyeh, L.A.; Aleidi, S.M.; Bustanji, Y. Pregabalin inhibits in vivo and in vitro cytokine secretion and attenuates spleen inflammation in Lipopolysaccharide/Concanavalin A -induced murine models of inflammation. Sci. Rep. 2020, 10, 4007. [Google Scholar] [CrossRef] [Green Version]
- Ha, K.Y.; Kim, Y.H.; Rhyu, K.W.; Kwon, S.E. Pregabalin as a neuroprotector after spinal cord injury in rats. Eur. Spine J. 2008, 17, 864–872. [Google Scholar] [CrossRef] [Green Version]
- Hurley, R.W.; Chatterjea, D.; Rose Feng, M.; Taylor, C.P.; Hammond, D.L. Gabapentin and pregabalin can interact synergistically with naproxen to produce antihyperalgesia. Anesthesiology 2002, 97, 1263–1273. [Google Scholar] [CrossRef]
- Narai, Y.; Imamachi, N.; Saito, Y. Gabapentin augments the antihyperalgesic effects of diclofenac sodium through spinal action in a rat postoperative pain model. Anesth. Analg. 2012, 115, 189–193. [Google Scholar] [CrossRef]
- Espinosa-Juarez, J.V.; Jaramillo-Morales, O.A.; Corona-Ramos, J.N.; Medina-Lopez, J.R.; Lopez-Munoz, F.J. Antinociceptive Interactions Between Meloxicam and Gabapentin in Neuropathic Pain Depend on the Ratio used in Combination in Rats. Drug Dev. Res. 2016, 77, 134–142. [Google Scholar] [CrossRef]
- Lin, W.Y.; Cheng, Y.T.; Huang, Y.H.; Lin, F.S.; Sun, W.Z.; Yen, C.T. Synergistic symptom-specific effects of ketorolac-tramadol and ketorolac-pregabalin in a rat model of peripheral neuropathy. J. Chin. Med. Assoc. 2019, 82, 457–463. [Google Scholar] [CrossRef]
- DiGiovanni, M.; Parker, J. Is pregabalin effective in reducing pain caused by arthritis? Evidence-Based Practice 2020, 23, 41–42. [Google Scholar] [CrossRef]
- Mortreux, M.; Semple, C.; Riveros, D.; Nagy, J.A.; Rutkove, S.B. Electrical impedance myography for the detection of muscle inflammation induced by lambda-carrageenan. PLoS ONE 2019, 14, e0223265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donvito, G.; Wilkerson, J.L.; Damaj, M.I.; Lichtman, A.H. Palmitoylethanolamide Reverses Paclitaxel-Induced Allodynia in Mice. J. Pharmacol. Exp. Ther. 2016, 359, 310–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qabazard, B.; Masocha, W.; Khajah, M.; Phillips, O.A. H2S donor GYY4137 ameliorates paclitaxel-induced neuropathic pain in mice. Biomed. Pharmacother. 2020, 127, 110210. [Google Scholar] [CrossRef]
- Montes, G.C.; Hammes, N.; da Rocha, M.D.; Montagnoli, T.L.; Fraga, C.A.; Barreiro, E.J.; Sudo, R.T.; Zapata-Sudo, G. Treatment with Adenosine Receptor Agonist Ameliorates Pain Induced by Acute and Chronic Inflammation. J. Pharmacol. Exp. Ther. 2016, 358, 315–323. [Google Scholar] [CrossRef] [Green Version]
- Vieira, M.C.; Monte, F.B.M.; Eduardo Dematte, B.; Montagnoli, T.L.; Montes, G.C.; da Silva, J.S.; Mendez-Otero, R.; Trachez, M.M.; Sudo, R.T.; Zapata-Sudo, G. Antinociceptive Effect of Lodenafil Carbonate in Rodent Models of Inflammatory Pain and Spinal Nerve Ligation-Induced Neuropathic Pain. J. Pain Res. 2021, 14, 857–866. [Google Scholar] [CrossRef]
- Tallarida, R.J. The interaction index: A measure of drug synergism. Pain 2002, 98, 163–168. [Google Scholar] [CrossRef]
- Chou, T.C. Theoretical basis, experimental design, and computerized simulation of synergism and antagonism in drug combination studies. Pharmacol. Rev. 2006, 58, 621–681. [Google Scholar] [CrossRef]
- De Paz-Campos, M.A.; Ortiz, M.I.; Chavez Pina, A.E.; Zazueta-Beltran, L.; Castaneda-Hernandez, G. Synergistic effect of the interaction between curcumin and diclofenac on the formalin test in rats. Phytomedicine 2014, 21, 1543–1548. [Google Scholar] [CrossRef]
- Tallarida, R.J. Statistical analysis of drug combinations for synergism. Pain 1992, 49, 93–97. [Google Scholar] [CrossRef]
- Mezzanotte, J.N.; Grimm, M.; Shinde, N.V.; Nolan, T.; Worthen-Chaudhari, L.; Williams, N.O.; Lustberg, M.B. Updates in the Treatment of Chemotherapy-Induced Peripheral Neuropathy. Curr. Treat. Options Oncol. 2022, 23, 29–42. [Google Scholar] [CrossRef] [PubMed]
- Freeman, R. The treatment of neuropathic pain. CNS Spectr. 2005, 10, 698–706. [Google Scholar] [CrossRef] [PubMed]
- Dworkin, R.H.; O’Connor, A.B.; Audette, J.; Baron, R.; Gourlay, G.K.; Haanpaa, M.L.; Kent, J.L.; Krane, E.J.; Lebel, A.A.; Levy, R.M.; et al. Recommendations for the pharmacological management of neuropathic pain: An overview and literature update. Mayo Clin. Proc. 2010, 85, S3–S14. [Google Scholar] [CrossRef] [Green Version]
- Yan, Y.Y.; Li, C.Y.; Zhou, L.; Ao, L.Y.; Fang, W.R.; Li, Y.M. Research progress of mechanisms and drug therapy for neuropathic pain. Life Sci. 2017, 190, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Dworkin, R.H.; O’Connor, A.B.; Backonja, M.; Farrar, J.T.; Finnerup, N.B.; Jensen, T.S.; Kalso, E.A.; Loeser, J.D.; Miaskowski, C.; Nurmikko, T.J.; et al. Pharmacologic management of neuropathic pain: Evidence-based recommendations. Pain 2007, 132, 237–251. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.; Dickenson, A.H. Neuropharmacological basis for multimodal analgesia in chronic pain. Postgrad. Med. 2021, 134, 245–259. [Google Scholar] [CrossRef] [PubMed]
- Ellis, A.; Bennett, D.L. Neuroinflammation and the generation of neuropathic pain. Br. J. Anaesth. 2013, 111, 26–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baba, H.; Kohno, T.; Moore, K.A.; Woolf, C.J. Direct activation of rat spinal dorsal horn neurons by prostaglandin E2. J. Neurosci. 2001, 21, 1750–1756. [Google Scholar] [CrossRef]
- Sammons, M.J.; Raval, P.; Davey, P.T.; Rogers, D.; Parsons, A.A.; Bingham, S. Carrageenan-induced thermal hyperalgesia in the mouse: Role of nerve growth factor and the mitogen-activated protein kinase pathway. Brain Res. 2000, 876, 48–54. [Google Scholar] [CrossRef]
- Kuedo, Z.; Sangsuriyawong, A.; Klaypradit, W.; Tipmanee, V.; Chonpathompikunlert, P. Effects of Astaxanthin from Litopenaeus Vannamei on Carrageenan-Induced Edema and Pain Behavior in Mice. Molecules 2016, 21, 382. [Google Scholar] [CrossRef] [Green Version]
- Tanabe, M.; Takasu, K.; Takeuchi, Y.; Ono, H. Pain relief by gabapentin and pregabalin via supraspinal mechanisms after peripheral nerve injury. J. Neurosci. Res. 2008, 86, 3258–3264. [Google Scholar] [CrossRef] [PubMed]
- Vanegas, H.; Vazquez, E.; Tortorici, V. NSAIDs, Opioids, Cannabinoids and the Control of Pain by the Central Nervous System. Pharmaceuticals 2010, 3, 1335–1347. [Google Scholar] [CrossRef] [PubMed]
- Shim, H.S.; Bae, C.; Wang, J.; Lee, K.H.; Hankerd, K.M.; Kim, H.K.; Chung, J.M.; La, J.H. Peripheral and central oxidative stress in chemotherapy-induced neuropathic pain. Mol. Pain. 2019, 15, 1744806919840098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Starobova, H.; Vetter, I. Pathophysiology of Chemotherapy-Induced Peripheral Neuropathy. Front. Mol. Neurosci. 2017, 10, 174. [Google Scholar] [CrossRef]
- Vichaya, E.G.; Chiu, G.S.; Krukowski, K.; Lacourt, T.E.; Kavelaars, A.; Dantzer, R.; Heijnen, C.J.; Walker, A.K. Mechanisms of chemotherapy-induced behavioral toxicities. Front. Neurosci. 2015, 9, 131. [Google Scholar] [CrossRef] [Green Version]
- McLeary, F.; Davis, A.; Rudrawar, S.; Perkins, A.; Anoopkumar-Dukie, S. Mechanisms underlying select chemotherapeutic-agent-induced neuroinflammation and subsequent neurodegeneration. Eur. J. Pharmacol. 2019, 842, 49–56. [Google Scholar] [CrossRef] [Green Version]
- Makker, P.G.; Duffy, S.S.; Lees, J.G.; Perera, C.J.; Tonkin, R.S.; Butovsky, O.; Park, S.B.; Goldstein, D.; Moalem-Taylor, G. Characterisation of Immune and Neuroinflammatory Changes Associated with Chemotherapy-Induced Peripheral Neuropathy. PLoS ONE 2017, 12, e0170814. [Google Scholar] [CrossRef]
- Burkholder, D.; Koehler, P.; Boes, C. Trigeminal Neuralgia and Multiple Sclerosis: A Historical Perspective. Can. J. Neurol. Sci. 2017, 44, 589–593. [Google Scholar] [CrossRef] [Green Version]
- Ericson, H.; Abu Hamdeh, S.; Freyhult, E.; Stiger, F.; Backryd, E.; Svenningsson, A.; Gordh, T.; Kultima, K. Cerebrospinal fluid biomarkers of inflammation in trigeminal neuralgia patients operated with microvascular decompression. Pain 2019, 160, 2603–2611. [Google Scholar] [CrossRef]
- Blaes, F. Diagnosis and therapeutic options for peripheral vasculitic neuropathy. Ther. Adv. Musculoskelet Dis. 2015, 7, 45–55. [Google Scholar] [CrossRef] [Green Version]
- Kawano, T.; Eguchi, S.; Iwata, H.; Yamanaka, D.; Tateiwa, H.; Locatelli, F.M.; Yokoyama, M. Pregabalin can prevent, but not treat, cognitive dysfunction following abdominal surgery in aged rats. Life Sci. 2016, 148, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Janjic, J.M.; Vasudeva, K.; Saleem, M.; Stevens, A.; Liu, L.; Patel, S.; Pollock, J.A. Low-dose NSAIDs reduce pain via macrophage targeted nanoemulsion delivery to neuroinflammation of the sciatic nerve in rat. J. Neuroimmunol. 2018, 318, 72–79. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups (n = 8) | Dose (mg/kg) | Antinociceptive Effect (%) a | |
|---|---|---|---|
| Indomethacin | Pregabalin | Combination | |
| (1) | 10.00 | 24 | 72.69 ± 7.17 |
| (2) | 5.00 | 12 | 58.89 ± 6.40 |
| (3) | 2.50 | 6 | 35.50 ± 1.74 |
| (4) | 1.25 | 3 | 25.96 ± 2.51 |
| (5) | 0.63 | 1.5 | 14.61 ± 3.61 |
| Meloxicam | Pregabalin | Combination | |
| (1) | 6.07 | 24 | 61.98 ± 7.02 |
| (2) | 3.03 | 12 | 50.04 ± 3.16 |
| (3) | 1.52 | 6 | 36.13 ± 2.56 |
| (4) | 0.76 | 3 | 27.10 ± 4.34 |
| (5) | 0.38 | 1.5 | 11.87 ± 4.77 |
| Groups (n = 6) | Dose (mg/kg) | Antinociceptive Effect (%) b | |
|---|---|---|---|
| Indomethacin | Pregabalin | Combination | |
| (1) | 1.72 | 1.30 | 51.14 ± 1.14 |
| (2) | 0.86 | 0.65 | 33.66 ± 0.58 |
| (3) | 0.43 | 0.33 | 20.64 ± 0.75 |
| (4) | 0.21 | 0.16 | 16.92 ± 1.45 |
| Meloxicam | Pregabalin | Combination | |
| (1) | 0.12 | 1.30 | 47.25 ± 0.91 |
| (2) | 0.25 | 0.65 | 47.14 ± 1.00 |
| (3) | 0.50 | 0.33 | 27.23 ± 2.10 |
| (4) | 0.99 | 0.16 | 2.78 ± 4.43 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, Y.; Liu, W.; Liang, L.; Ye, J.; Huang, C.; Zhuang, T.; Zhang, G. Synergistic Antinociceptive Effects of Indomethacin–Pregabalin and Meloxicam–Pregabalin in Paclitaxel-Induced Neuropathic Pain. Biomedicines 2022, 10, 1413. https://doi.org/10.3390/biomedicines10061413
Ma Y, Liu W, Liang L, Ye J, Huang C, Zhuang T, Zhang G. Synergistic Antinociceptive Effects of Indomethacin–Pregabalin and Meloxicam–Pregabalin in Paclitaxel-Induced Neuropathic Pain. Biomedicines. 2022; 10(6):1413. https://doi.org/10.3390/biomedicines10061413
Chicago/Turabian StyleMa, Yurong, Wenwen Liu, Lingzhi Liang, Jiaqi Ye, Chaonan Huang, Tao Zhuang, and Guisen Zhang. 2022. "Synergistic Antinociceptive Effects of Indomethacin–Pregabalin and Meloxicam–Pregabalin in Paclitaxel-Induced Neuropathic Pain" Biomedicines 10, no. 6: 1413. https://doi.org/10.3390/biomedicines10061413