
Reactivity of the Oxytocinergic and Neuroendocrine System Following the Adult Attachment Projective Picture System in Men of Recent Fatherhood: Results from an Exploratory Pilot Study with a Cross-Sectional Design
 , , , ,
, , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
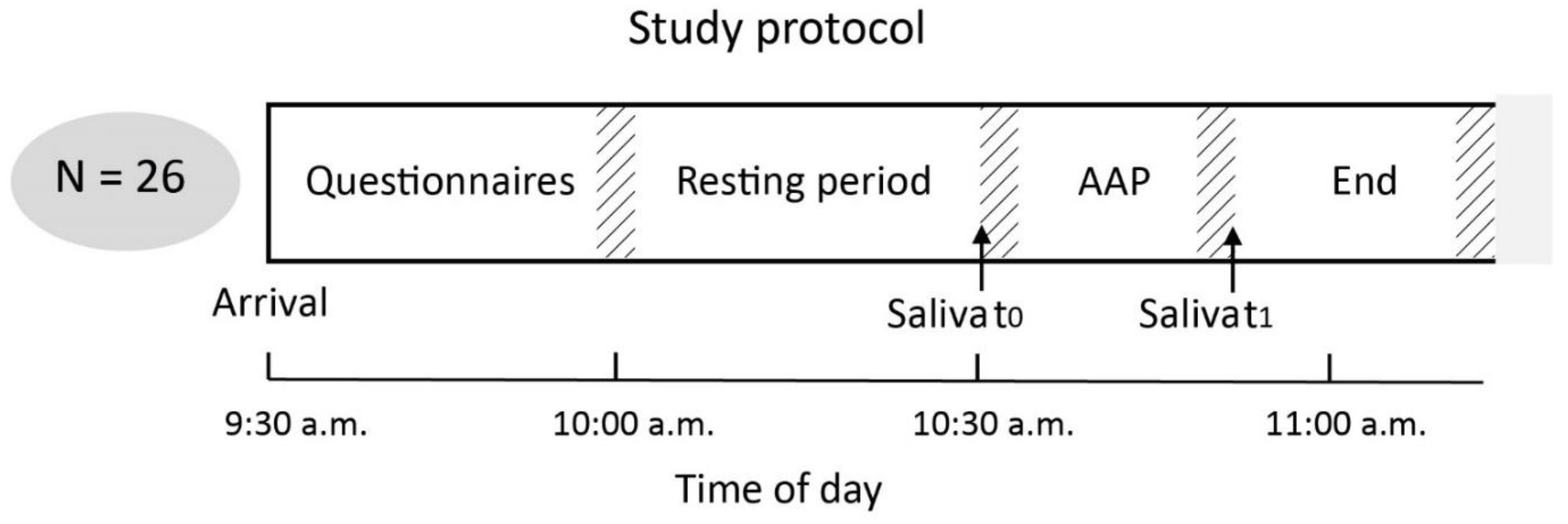
2.1. Recruitment and Study Design
2.2. Assessment of Attachment Representation Using the AAP
2.3. Sample Preparation
2.4. Quantification of Biomarkers in Saliva
2.5. Statistical Data Analyses
3. Results
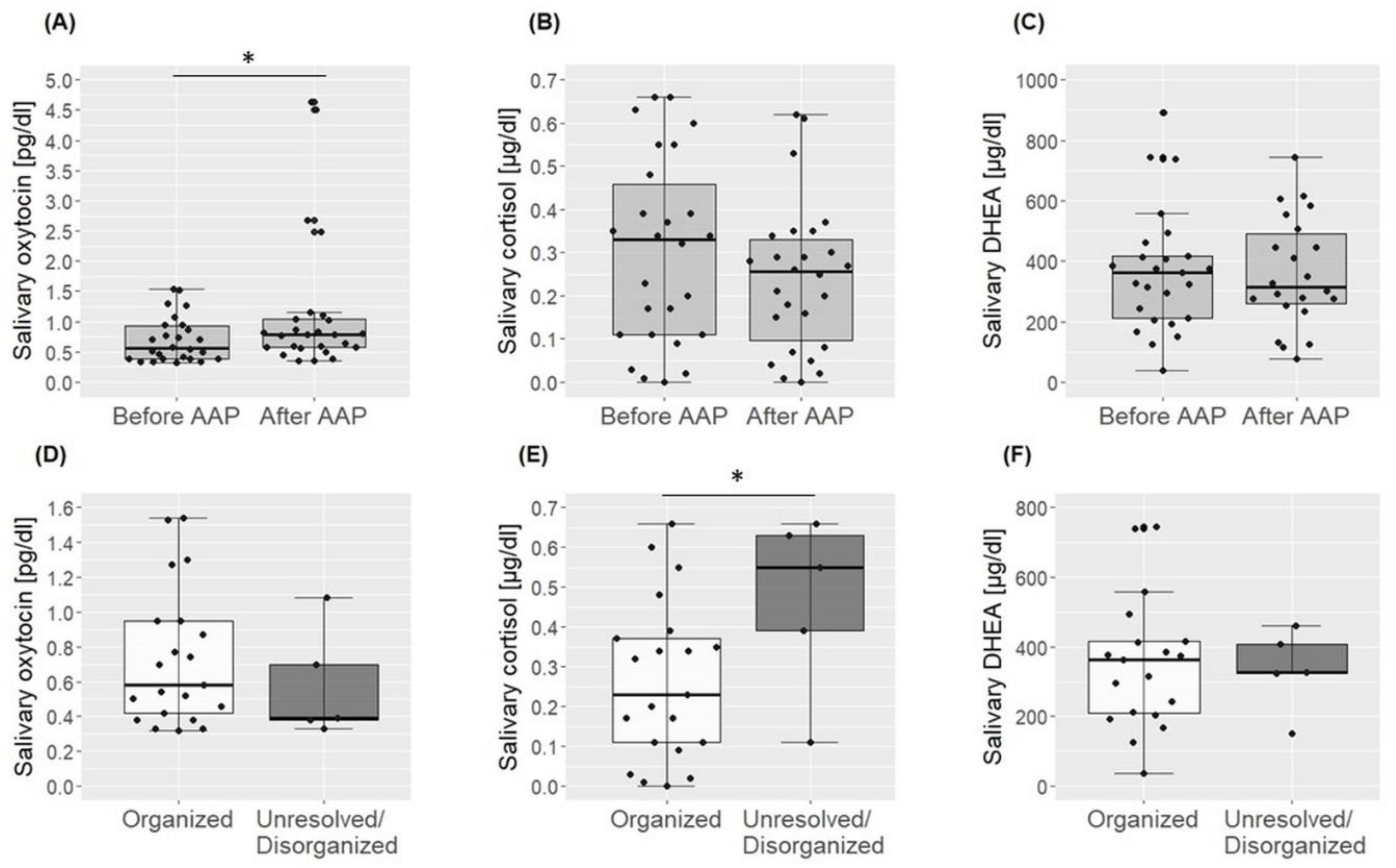
3.1. Reactivity Measures of Oxytocin, Cortisol and DHEA
3.2. Basal Levels of Oxytocin, Cortisol and DHEA
3.3. Correlations among Salivary Biomarkers
4. Discussion
5. Limitations and Future Directions
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bowlby, J. Attachment and Loss, 2nd ed.; Basic Books: New York, NY, USA, 1999; ISBN 978-0-465-00543-7. [Google Scholar]
- Wichmann, T.; Buchheim, A.; Menning, H.; Schenk, I.; George, C.; Pokorny, D. A Reaction Time Experiment on Adult Attachment: The Development of a Measure for Neurophysiological Settings. Front. Hum. Neurosci. 2016, 10, 548. [Google Scholar] [CrossRef] [PubMed]
- Scheidt, C.E.; Waller, E.; Malchow, H.; Ehlert, U.; Becker-Stoll, F.; Schulte-Mönting, J.; Lücking, C.H. Attachment Representation and Cortisol Response to the Adult Attachment Interview in Idiopathic Spasmodic Torticollis. Psychother. Psychosom. 2000, 69, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Pierrehumbert, B.; Torrisi, R.; Ansermet, F.; Borghini, A.; Halfon, O. Adult Attachment Representations Predict Cortisol and Oxytocin Responses to Stress. Attach. Hum. Dev. 2012, 14, 453–476. [Google Scholar] [CrossRef] [PubMed]
- Maunder, R.G.; Hunter, J.J. Attachment and Psychosomatic Medicine: Developmental Contributions to Stress and Disease. Psychosom. Med. 2001, 63, 556–567. [Google Scholar] [CrossRef]
- Buchheim, A.; Erk, S.; George, C.; Kächele, H.; Kircher, T.; Martius, P.; Pokorny, D.; Ruchsow, M.; Spitzer, M.; Walter, H. Neural Correlates of Attachment Trauma in Borderline Personality Disorder: A Functional Magnetic Resonance Imaging Study. Psychiatry Res. 2008, 163, 223–235. [Google Scholar] [CrossRef]
- Bakermans-Kranenburg, M.J.; van IJzendoorn, M.H. The First 10,000 Adult Attachment Interviews: Distributions of Adult Attachment Representations in Clinical and Non-Clinical Groups. Attach. Hum. Dev. 2009, 11, 223–263. [Google Scholar] [CrossRef]
- George, C.; West, M. The Development and Preliminary Validation of a New Measure of Adult Attachment: The Adult Attachment Projective. Attach. Hum. Dev. 2001, 3, 30–61. [Google Scholar] [CrossRef]
- George, C.; West, M. The Adult Attachment Projective Picture System: Integrating Attachment Into Clinical Assessment. J. Personal. Assess. 2011, 93, 407–416. [Google Scholar] [CrossRef]
- Buchheim, A.; Erk, S.; George, C.; Kächele, H.; Martius, P.; Pokorny, D.; Spitzer, M.; Walter, H. Neural Response during the Activation of the Attachment System in Patients with Borderline Personality Disorder: An FMRI Study. Front. Hum. Neurosci. 2016, 10, 389. [Google Scholar] [CrossRef]
- Krause, S.; Pokorny, D.; Schury, K.; Doyen-Waldecker, C.; Hulbert, A.-L.; Karabatsiakis, A.; Kolassa, I.-T.; Gündel, H.; Waller, C.; Buchheim, A. Effects of the Adult Attachment Projective Picture System on Oxytocin and Cortisol Blood Levels in Mothers. Front. Hum. Neurosci. 2016, 10, 627. [Google Scholar] [CrossRef] [Green Version]
- Landgraf, R.; Neumann, I.D. Vasopressin and Oxytocin Release within the Brain: A Dynamic Concept of Multiple and Variable Modes of Neuropeptide Communication. Front. Neuroendocrinol. 2004, 25, 150–176. [Google Scholar] [CrossRef] [PubMed]
- Raam, T. Oxytocin-Sensitive Neurons in Prefrontal Cortex Gate Social Recognition Memory. J. Neurosci. 2020, 40, 1194–1196. [Google Scholar] [CrossRef] [PubMed]
- Strathearn, L. Maternal Neglect: Oxytocin, Dopamine and the Neurobiology of Attachment. J. Neuroendocrinol. 2011, 23, 1054–1065. [Google Scholar] [CrossRef]
- Heinrichs, M.; Domes, G. Neuropeptides and Social Behaviour: Effects of Oxytocin and Vasopressin in Humans. Prog. Brain Res. 2008, 170, 337–350. [Google Scholar] [CrossRef] [PubMed]
- Toepfer, P.; Heim, C.; Entringer, S.; Binder, E.; Wadhwa, P.; Buss, C. Oxytocin Pathways in the Intergenerational Transmission of Maternal Early Life Stress. Neurosci. Biobehav. Rev. 2017, 73, 293–308. [Google Scholar] [CrossRef]
- Ross, H.E.; Young, L.J. Oxytocin and the Neural Mechanisms Regulating Social Cognition and Affiliative Behavior. Front. Neuroendocrinol. 2009, 30, 534–547. [Google Scholar] [CrossRef]
- Kosfeld, M.; Heinrichs, M.; Zak, P.J.; Fischbacher, U.; Fehr, E. Oxytocin Increases Trust in Humans. Nature 2005, 435, 673–676. [Google Scholar] [CrossRef]
- Torner, L.; Plotsky, P.M.; Neumann, I.D.; de Jong, T.R. Forced Swimming-Induced Oxytocin Release into Blood and Brain: Effects of Adrenalectomy and Corticosterone Treatment. Psychoneuroendocrinology 2017, 77, 165–174. [Google Scholar] [CrossRef]
- Neumann, I.D.; Wigger, A.; Torner, L.; Holsboer, F.; Landgraf, R. Brain Oxytocin Inhibits Basal and Stress-Induced Activity of the Hypothalamo-Pituitary-Adrenal Axis in Male and Female Rats: Partial Action within the Paraventricular Nucleus. J. Neuroendocrinol. 2000, 12, 235–243. [Google Scholar] [CrossRef]
- Legros, J.J. Inhibitory Effect of Oxytocin on Corticotrope Function in Humans: Are Vasopressin and Oxytocin Ying-Yang Neurohormones? Psychoneuroendocrinology 2001, 26, 649–655. [Google Scholar] [CrossRef]
- Kamin, H.S.; Kertes, D.A. Cortisol and DHEA in Development and Psychopathology. Horm. Behav. 2017, 89, 69–85. [Google Scholar] [CrossRef]
- Dutheil, F.; de Saint Vincent, S.; Pereira, B.; Schmidt, J.; Moustafa, F.; Charkhabi, M.; Bouillon-Minois, J.-B.; Clinchamps, M. DHEA as a Biomarker of Stress: A Systematic Review and Meta-Analysis. Front. Psychiatry 2021, 12, 688367. [Google Scholar] [CrossRef] [PubMed]
- Heinrichs, M.; Baumgartner, T.; Kirschbaum, C.; Ehlert, U. Social Support and Oxytocin Interact to Suppress Cortisol and Subjective Responses to Psychosocial Stress. Biol. Psychiatry 2003, 54, 1389–1398. [Google Scholar] [CrossRef]
- Brown, C.A.; Cardoso, C.; Ellenbogen, M.A. A Meta-Analytic Review of the Correlation between Peripheral Oxytocin and Cortisol Concentrations. Front. Neuroendocrinol. 2016, 43, 19–27. [Google Scholar] [CrossRef]
- Engert, V.; Koester, A.M.; Riepenhausen, A.; Singer, T. Boosting Recovery Rather than Buffering Reactivity: Higher Stress-Induced Oxytocin Secretion Is Associated with Increased Cortisol Reactivity and Faster Vagal Recovery after Acute Psychosocial Stress. Psychoneuroendocrinology 2016, 74, 111–120. [Google Scholar] [CrossRef]
- Pierrehumbert, B.; Torrisi, R.; Laufer, D.; Halfon, O.; Ansermet, F.; Beck Popovic, M. Oxytocin Response to an Experimental Psychosocial Challenge in Adults Exposed to Traumatic Experiences during Childhood or Adolescence. Neuroscience 2010, 166, 168–177. [Google Scholar] [CrossRef]
- de Jong, T.R.; Menon, R.; Bludau, A.; Grund, T.; Biermeier, V.; Klampfl, S.M.; Jurek, B.; Bosch, O.J.; Hellhammer, J.; Neumann, I.D. Salivary Oxytocin Concentrations in Response to Running, Sexual Self-Stimulation, Breastfeeding and the TSST: The Regensburg Oxytocin Challenge (ROC) Study. Psychoneuroendocrinology 2015, 62, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Bernhard, A.; van der Merwe, C.; Ackermann, K.; Martinelli, A.; Neumann, I.D.; Freitag, C.M. Adolescent Oxytocin Response to Stress and Its Behavioral and Endocrine Correlates. Horm. Behav. 2018, 105, 157–165. [Google Scholar] [CrossRef]
- Bauman, M.D.; Lavenex, P.; Mason, W.A.; Capitanio, J.P.; Amaral, D.G. The Development of Mother-Infant Interactions after Neonatal Amygdala Lesions in Rhesus Monkeys. J. Neurosci. 2004, 24, 711–721. [Google Scholar] [CrossRef]
- Buchheim, A.; Erk, S.; George, C.; Kachele, H.; Ruchsow, M.; Spitzer, M.; Kircher, T.; Walter, H. Measuring Attachment Representation in an FMRI Environment: A Pilot Study. Psychopathology 2006, 39, 144–152. [Google Scholar] [CrossRef]
- Fuchshuber, J.; Tatzer, J.; Hiebler-Ragger, M.; Trinkl, F.; Kimmerle, A.; Rinner, A.; Buchheim, A.; Schrom, S.; Rinner, B.; Leber, K.; et al. The Influence of an Attachment-Related Stimulus on Oxytocin Reactivity in Poly-Drug Users Undergoing Maintenance Therapy Compared to Healthy Controls. Front. Psychiatry 2020, 11, 460506. [Google Scholar] [CrossRef] [PubMed]
- Buchheim, A.; Ziegenhain, U.; Kindler, H.; Waller, C.; Gündel, H.; Karabatsiakis, A.; Fegert, J. Identifying Risk and Resilience Factors in the Intergenerational Cycle of Maltreatment: Results From the TRANS-GEN Study Investigating the Effects of Maternal Attachment and Social Support on Child Attachment and Cardiovascular Stress Physiology. Front. Hum. Neurosci. 2022, 16, 890262. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [CrossRef]
- George, C.; West, M.L. The Adult Attachment Projective Picture System: Attachment Theory and Assessment in Adults; Guilford Press: New York, NY, USA, 2012; ISBN 978-1-4625-0425-1. [Google Scholar]
- Buchheim, A.; George, C. Attachment Disorganization in Borderline Personality Disorder and Anxiety Disorder. In Disorganized Attachment and Caregiving; The Guilford Press: New York, NY, USA, 2011; pp. 343–382. ISBN 978-1-60918-128-4. [Google Scholar]
- Jobst, A.; Padberg, F.; Mauer, M.-C.; Daltrozzo, T.; Bauriedl-Schmidt, C.; Sabass, L.; Sarubin, N.; Falkai, P.; Renneberg, B.; Zill, P.; et al. Lower Oxytocin Plasma Levels in Borderline Patients with Unresolved Attachment Representations. Front. Hum. Neurosci. 2016, 10, 125. [Google Scholar] [CrossRef] [PubMed]
- Plasencia, G.; Luedicke, J.M.; Nazarloo, H.P.; Carter, C.S.; Ebner, N.C. Plasma Oxytocin and Vasopressin Levels in Young and Older Men and Women: Functional Relationships with Attachment and Cognition. Psychoneuroendocrinology 2019, 110, 104419. [Google Scholar] [CrossRef]
- Gander, M.; Buchheim, A. Attachment Classification, Psychophysiology and Frontal EEG Asymmetry across the Lifespan: A Review. Front. Hum. Neurosci. 2015, 9, 79. [Google Scholar] [CrossRef]
- Rifkin-Graboi, A. Attachment Status and Salivary Cortisol in a Normal Day and during Simulated Interpersonal Stress in Young Men. Stress 2008, 11, 210–224. [Google Scholar] [CrossRef]
- Adam, E.K.; Gunnar, M.R. Relationship Functioning and Home and Work Demands Predict Individual Differences in Diurnal Cortisol Patterns in Women. Psychoneuroendocrinology 2001, 26, 189–208. [Google Scholar] [CrossRef]
- Oskis, A.; Loveday, C.; Hucklebridge, F.; Thorn, L.; Clow, A. Anxious Attachment Style and Salivary Cortisol Dysregulation in Healthy Female Children and Adolescents. J. Child. Psychol. Psychiatry 2011, 52, 111–118. [Google Scholar] [CrossRef]
- Smyth, N.; Thorn, L.; Oskis, A.; Hucklebridge, F.; Evans, P.; Clow, A. Anxious Attachment Style Predicts an Enhanced Cortisol Response to Group Psychosocial Stress. Stress 2015, 18, 143–148. [Google Scholar] [CrossRef] [Green Version]
- Bryant, R.A.; Chan, L. Thinking of Attachments Reduces Noradrenergic Stress Response. Psychoneuroendocrinology 2015, 60, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Horvat-Gordon, M.; Granger, D.A.; Schwartz, E.B.; Nelson, V.J.; Kivlighan, K.T. Oxytocin Is Not a Valid Biomarker When Measured in Saliva by Immunoassay. Physiol. Behav. 2005, 84, 445–448. [Google Scholar] [CrossRef] [PubMed]
- Carter, C.S.; Pournajafi-Nazarloo, H.; Kramer, K.M.; Ziegler, T.E.; White-Traut, R.; Bello, D.; Schwertz, D. Oxytocin: Behavioral Associations and Potential as a Salivary Biomarker. Ann. N. Y. Acad. Sci. 2007, 1098, 312–322. [Google Scholar] [CrossRef] [PubMed]
- Lebowitz, E.R.; Leckman, J.F.; Feldman, R.; Zagoory-Sharon, O.; McDonald, N.; Silverman, W.K. Salivary Oxytocin in Clinically Anxious Youth: Associations with Separation Anxiety and Family Accommodation. Psychoneuroendocrinology 2016, 65, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.; Kagerbauer, S.M.; Gempt, J.; Podtschaske, A.; Hapfelmeier, A.; Schneider, G. Oxytocin Levels in Saliva Correlate Better than Plasma Levels with Concentrations in the Cerebrospinal Fluid of Patients in Neurocritical Care. J. Neuroendocrinol. 2018, 30, e12596. [Google Scholar] [CrossRef] [PubMed]
- White-Traut, R.; Watanabe, K.; Pournajafi-Nazarloo, H.; Schwertz, D.; Bell, A.; Carter, C.S. Detection of Salivary Oxytocin Levels in Lactating Women. Dev. Psychobiol. 2009, 51, 367–373. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Total | Organized | Unresolved/ Disorganized | t-Test/ MWU-Test/ χ2-Test | |
|---|---|---|---|---|
| Sociodemographic and Clinical Characteristics | N = 26 | n = 21 | n = 5 | |
| Age in years, M (SD) | 33 (5.2) | 31.86 (4.14) | 38 (6.63) | t24 = −2.66, p = 0.014 |
| Academic education, n, yes (%) | 15 (57.7) | 12 (57.1) | 3 (60) | χ2 = 0.01, p = 0.91 |
| Family income < 4000 € per month (self-report), n (%) | 11 (42) | 10 (47.6) | 1 (20) | χ2 = 1.26, p = 0.26 |
| Cigarette smoking a, yes, n (%) | 7 (26.9) | 3 (14.3) | 4 (80) | χ2 = 7.9, p = 0.005 |
| BMI, kg/m2, M (SD) | 26.7 (5.4) | 26.93 (5.84) | 25.54 (2.72) | U = 52, z = −0.03, p = 0.97 |
| Migration background, yes, n (%) | 5 (19.2) | 3 (14.3) | 2 (40) | χ2 = 1.72, p = 0.19 |
| Number of children, M (SD) | 1.7 (0.56) | 1.61 (0.59) | 1.8 (0.45) | t24 = −0.64, p = 0.53 |
| Lifetime psychiatric diagnosis, yes, n (%) | 3 (1.5) | 2 (9.5) | 1 (20) | χ2 = 0.43, p = 0.51 |
| Duration AAP (min), M (SD) | 17.64 (5.42) | 17.25 (5.29) | 19.26 (6.3) | t24 = −0.74, p = 0.47 |
| Attachment representation, n (%) | ||||
| Secure (F) | 5 (19.2) | NA | NA | |
| Preoccupied (E) | 7 (26.9) | NA | NA | |
| Dismissing (D) | 9 (34.6) | NA | NA | |
| Unresolved (U) | 5 (19.2) | NA | NA | |
| Biological Markers | ||||
| Oxytcin t0, 1 M (SD) | 0.70 (0.38) | 0.73 (0.39) | 0.58 (0.32) | t24 = 0.82, p = 0.42 |
| Oxytocin t1, M (SD) | 1.15 (1.14) | 1.06 (1.02) | 1.54 (1.67) | U = 41, z = −0.75, p = 0.49 |
| Cortisol t0, M (SD) | 0.28 (0.21) | 0.24 (0.18) | 0.47 (0.23) | t24 = −2.48, p = 0.021 |
| Cortisol t1, M (SD) | 0.24 (0.17) | 0.22 (0.17) | 0.34 (0.18) | t24 = −1.4, p = 0.17 |
| DHEA t0 b, M (SD) | 368.76 (202.73) | 377.46 (220.51) | 333.92 (117.21) | t23 = 0.42, p = 0.68 |
| DHEA t1 c, M (SD) | 391.64 (231.22) | 381.45 (197.36) | 428.34 (355.45) | t21 = 0.39, p = 0.70 |
| Oxytocin response %, M (SD) | 84.06 (183.52) | 72.76 (197.41) | 131.51 (110.27) | U = 84, z = −2, p = 0.041 |
| Cortisol response %, M (SD) | 10.23 (66.17) | 16.80 (70.63) | −17.32 (35.26) | U = 36, z = −1.1, p = 0.31 |
| DHEA response % c, M (SD) | 62.77 (289.01) | 70.75 (325.51) | 34.06 (88.18) | U = 51, z = 0.45, p = 0.69 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karabatsiakis, A.; de Punder, K.; Doyen-Waldecker, C.; Ramo-Fernández, L.; Krause, S.; Gumpp, A.M.; Bach, A.M.; Fegert, J.M.; Kolassa, I.-T.; Gündel, H.; et al. Reactivity of the Oxytocinergic and Neuroendocrine System Following the Adult Attachment Projective Picture System in Men of Recent Fatherhood: Results from an Exploratory Pilot Study with a Cross-Sectional Design. Brain Sci. 2022, 12, 1314. https://doi.org/10.3390/brainsci12101314
Karabatsiakis A, de Punder K, Doyen-Waldecker C, Ramo-Fernández L, Krause S, Gumpp AM, Bach AM, Fegert JM, Kolassa I-T, Gündel H, et al. Reactivity of the Oxytocinergic and Neuroendocrine System Following the Adult Attachment Projective Picture System in Men of Recent Fatherhood: Results from an Exploratory Pilot Study with a Cross-Sectional Design. Brain Sciences. 2022; 12(10):1314. https://doi.org/10.3390/brainsci12101314
Chicago/Turabian StyleKarabatsiakis, Alexander, Karin de Punder, Cornelia Doyen-Waldecker, Laura Ramo-Fernández, Sabrina Krause, Anja Maria Gumpp, Alexandra Maria Bach, Jörg Michael Fegert, Iris-Tatjana Kolassa, Harald Gündel, and et al. 2022. "Reactivity of the Oxytocinergic and Neuroendocrine System Following the Adult Attachment Projective Picture System in Men of Recent Fatherhood: Results from an Exploratory Pilot Study with a Cross-Sectional Design" Brain Sciences 12, no. 10: 1314. https://doi.org/10.3390/brainsci12101314