
Breastfeeding during COVID-19: A Narrative Review of the Psychological Impact on Mothers

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
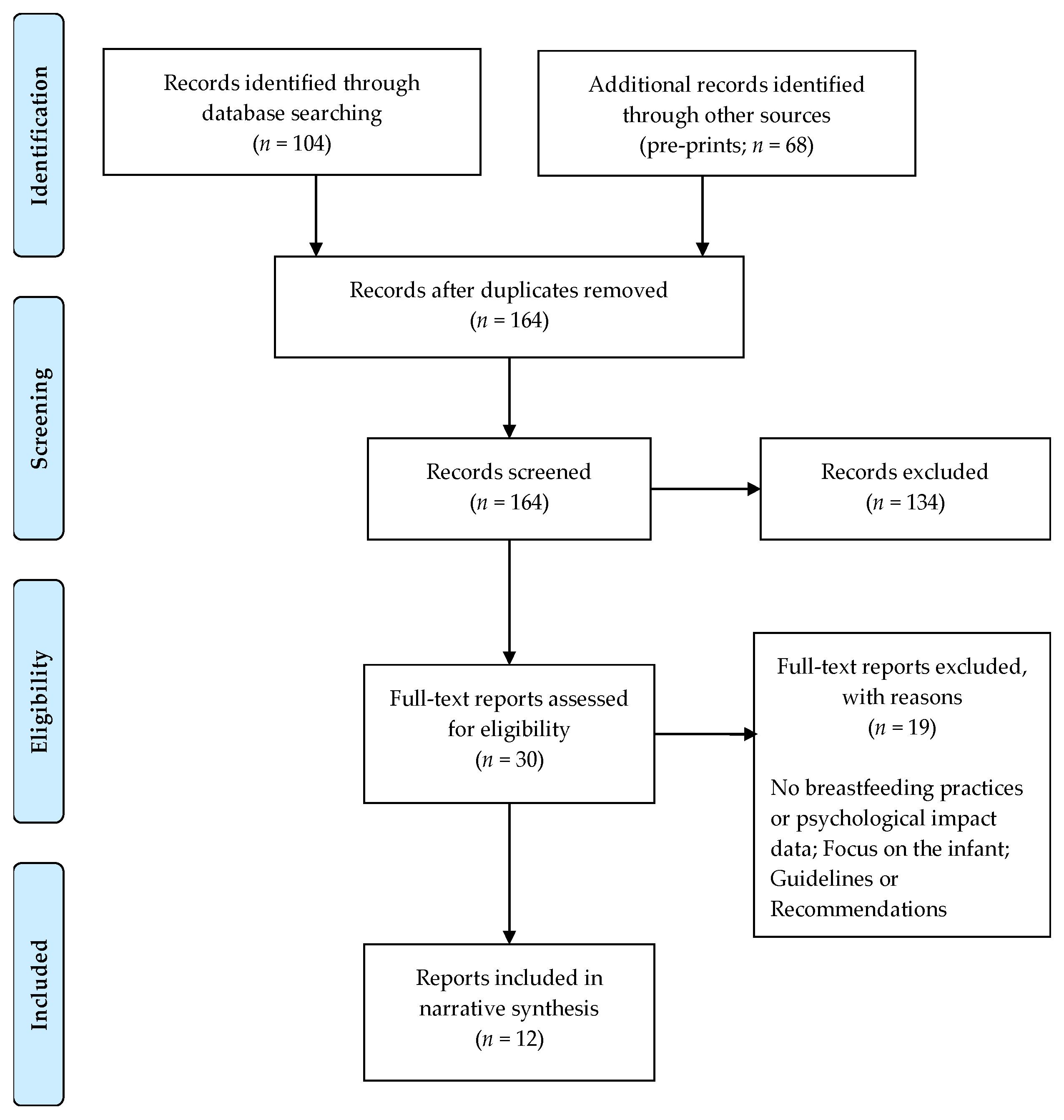
2. Methods
3. Results
3.1. Impact of COVID-19 Pandemic on Planned Breastfeeding Practices
3.1.1. General Impact of COVID-19 on Planned Breastfeeding
3.1.2. Impact of COVID-19 on Planned Feeding Methods—Moving from Other Methods to Breastfeeding
3.1.3. Impact of COVID-19 on Mothers Who Tested Positive for COVID-19
3.1.4. Impact of COVID-19 on Breastfeeding Experience
3.2. Breastfeeding Safety Concerns
3.3. Impact of COVID-19 on Perceptions of Support
3.4. The Psychological Outcomes of Mothers
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Ceulemans, M.; Verbakel, J.Y.; Van Calsteren, K.; Eerdekens, A.; Allegaert, K.; Foulon, V. SARS-CoV-2 infections and impact of the COVID-19 pandemic in pregnancy and breastfeeding: Results from an observational study in primary care in Belgium. Int. J. Environ. Res. Public Health 2020, 17, 6766. [Google Scholar] [CrossRef] [PubMed]
- Stube, A. Should infants be separated from mothers with COVID-19? First, do no harm. Breastfeed. Med. 2020, 15, 351–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caparros-Gonzalez, R.A.; Alderdice, F. The COVID-19 pandemic and perinatal mental health. J. Reprod. Infant Psychol. 2020, 38, 223–225. [Google Scholar] [CrossRef] [PubMed]
- Holcomb, J. Resisting guilt: Mothers’ breastfeeding intentions and formula use. Sociol. Focus 2017, 50, 361–374. [Google Scholar] [CrossRef]
- Leurer, M.D.; Misskey, E. The psychosocial and emotional experience of breastfeeding. Glob. Qual. Nurs. Res. 2015, 2, 2333393615611654. [Google Scholar] [CrossRef] [Green Version]
- Kelleher, C.M. The physical challenges of early breastfeeding. Soc. Sci. Med. 2006, 63, 2727–2738. [Google Scholar] [CrossRef] [PubMed]
- Kong, S.K.F.; Lee, D.T.F. Factors influencing decision to breastfeed. J. Adv. Nur. 2004, 46, 369–379. [Google Scholar] [CrossRef]
- Radzyminski, S.; Callister, L.C. Mother’s beliefs, attitudes, and decision making related to infant feeding choices. J. Perinat. Educ. 2016, 25, 18–28. [Google Scholar] [CrossRef] [Green Version]
- Wennberg, A.L.; Jonsson, S.; Janke, J.Z.; Hörnsten, Å. Online perceptions of mothers about breastfeeding and introducing formula: Qualitative study. JMIR Public Health Surveill. 2017, 3, e88. [Google Scholar] [CrossRef] [Green Version]
- Motrico, M.; Mateus, V.; Bina, R.; Felice, E.; Bramante, A.; Kalcev, G.; Mauri, M.; Martins, S.; Mesquita, A. Good practices in perinatal mental health during the COVID-19 pandemic: A report from task-force RISEUP-PPD COVID-19. Clin. Salud 2020, 31, 155–160. [Google Scholar] [CrossRef]
- Busch-Hallen, J.; Walters, D.; Rowe, S.; Chowdhury, A.; Arabi, M. Impact of COVID-19 on maternal and child health. Lancet Glob. Health 2020, 8, e1257. [Google Scholar] [CrossRef]
- Brown, A.; Shenker, N. Experiences of breastfeeding during COVID-19: Lessons for future practical and emotional support. Matern. Child. Nutr. 2020, 17, e13088. [Google Scholar] [CrossRef]
- Brett, M.; Baxendale, S. Motherhood and memory: A review. Psychoneuroendocrinology 2001, 26, 339–362. [Google Scholar] [CrossRef]
- Brunton, P.J.; Russell, J.A. Prenatal social stress in the rat programmes neuroendocrine and behavioural responses to stress in the adult offspring: Sex-specific effects. J. Neuroendocr. 2010, 22, 258–271. [Google Scholar] [CrossRef]
- Deems, N.P.; Leuner, B. Pregnancy, postpartum and parity: Resilience and vulnerability in brain health and disease. Front. Neuroendocr. 2020, 57, 100820. [Google Scholar] [CrossRef]
- Kendell, R.E.; Chalmers, J.C.; Platz, C. Epidemiology of puerperal psychoses. Br. J. Psychiatry 1987, 150, 662–673. [Google Scholar] [CrossRef]
- Fisher, J.; Cabral de Mello, M.; Patel, V.; Rahman, A.; Tran, T.; Holton, S.; Holmes, W. Prevalence and determinants of common perinatal mental disorders in women in low- and lower-middle-income countries: A systematic review. Bull. World Health Organ. 2012, 90, 139G–149G. [Google Scholar] [CrossRef]
- Howard, L.M.; Molyneaux, E.; Dennis, C.L.; Rochat, T.; Stein, A.; Milgrom, J. Non-psychotic mental disorders in the perinatal period. Lancet 2014, 384, 1775–1788. [Google Scholar] [CrossRef]
- Davenport, M.H.; Meyer, S.; Meah, V.L.; Strynadka, M.C.; Khurana, R. Moms are not OK: COVID-19 and maternal mental health. Front. Glob. Womens Health 2020, 1, 1. [Google Scholar] [CrossRef]
- Krol, K.M.; Grossmann, T. Psychological effects of breastfeeding on children and mothers. Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz 2018, 61, 977–985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Figueiredo, B.; Dias, C.C.; Brandão, S.; Canário, C.; Nunes-Costa, R. Breastfeeding and postpartum depression: State of the art review. J. Pediatr. 2013, 89, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Gregory, E.F.; Butz, A.M.; Ghazarian, S.R.; Gross, S.M.; Johnson, S.B. Are unmet breastfeeding expectations associated with maternal depressive symptoms? Acad. Pediatr. 2015, 15, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Fakari, F.R.; Simbar, M. Coronavirus pandemic and worries during pregnancy; a letter to editor. Arch. Acad. Emerg. Med. 2020, 8, e21. [Google Scholar]
- Caparros-Gonzalez, R.A.; Pérez-Morente, M.A.; Hueso-Montoro, C.; Álvarez-Serrano, M.A.; de la Torre-Luque, A. Congenital, intrapartum and postnatal maternal-fetal-neonatal SARS-CoV-2 infections: A narrative review. Nutrients 2020, 12, 3570. [Google Scholar] [CrossRef]
- Chen, H.; Guo, J.; Wang, C.; Luo, F.; Yu, X.; Zhang, W.; Li, J.; Zhao, D.; Xu, D.; Gong, Q.; et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: A retrospective review of medical records. Lancet 2020, 395, 809–815. [Google Scholar] [CrossRef] [Green Version]
- Groß, R.; Conzelmann, C.; Müller, J.A.; Stenger, S.; Steinhart, K.; Kirchhoff, F.; Münch, J. Detection of SARS-CoV-2 in human breastmilk. Lancet 2020, 395, 1757–1758. [Google Scholar] [CrossRef]
- Wu, Y.; Liu, C.; Dong, L.; Zhang, C.; Chen, Y.; Liu, J.; Zhang, C.; Duan, C.; Zhang, H.; Mol, B.W.; et al. Coronavirus disease 2019 among pregnant Chinese women: Case series data on the safety of vaginal birth and breastfeeding. BJOG 2020, 127, 1109–1115. [Google Scholar] [CrossRef] [PubMed]
- Dimopoulou, D.; Triantafyllidou, P.; Daskalaki, A.; Syridou, G.; Papaevangelou, V. Breastfeeding during the novel coronavirus (COVID-19) pandemic: Guidelines and challenges. J. Matern. Fetal Neonatal Med. 2020, 1–7. [Google Scholar] [CrossRef]
- Dashraath, P.; Wong, J.L.J.; Lim, M.X.K.; Lim, L.M.; Li, S.; Biswas, A.; Choolani, M.; Mattar, C.; Su, L.L. Coronavirus disease 2019 (COVID-19) pandemic and pregnancy. Am. J. Obs. Gynecol. 2020, 222, 521–531. [Google Scholar] [CrossRef]
- Chandrasekharan, P.; Vento, M.; Trevisanuto, D.; Partridge, E.; Underwood, M.A.; Wiedeman, J.; Katheria, A.; Lakshminrusimha, S. Neonatal resuscitation and postresuscitation care of infants born to mothers with suspected or confirmed SARS-CoV-2 infection. Am. J. Perinatol. 2020, 37, 813–824. [Google Scholar] [CrossRef] [Green Version]
- Tomori, C.; Gribble, K.; Palmquist, A.E.L.; Ververs, M.-T.; Gross, M.S. When separation is not the answer: Breastfeeding mothers and infants affected by COVID-19. Matern. Child. Nutr. 2020, 16, e13033. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization, WHO. Clinical Management of Severe Acute Respiratory Infection (SARI) When COVID-19 DISEASE IS SUSPECTED: Interim Guidance. Available online: https://www.who.int/docs/default-source/coronaviruse/clinical-management-of-novel-cov.pdf?sfvrsn=bc7da517_10&download=true (accessed on 13 November 2020).
- Melo, M.C.A.; Soares, D.S. Impact of social distancing on mental health during the COVID-19 pandemic: An urgent discussion. Int. J. Soc. Psychiatry 2020, 66, 625–626. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzla, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceulemans, M.; Hompes, T.; Foulon, V. Mental health status of pregnant and breastfeeding women during the COVID-19 pandemic: A call for action. Int. J. Gynecol. Obs. 2020, 151, 146–147. [Google Scholar] [CrossRef] [PubMed]
- Vazquez-Vazquez, A.; Dib, S.; Rougeaux, E.; Wells, J.C.; Fewtrell, M. The impact of the Covid-19 lockdown on the experiences and feeding practices of new mothers in the UK: Preliminary data from the COVID-19 New Mum Study. Appetite 2021, 156, 104985. [Google Scholar] [CrossRef] [PubMed]
- Burgess, A.; Breman, R.B.; Bradley, D.; Dada, S.; Burcher, P. Pregnant women’s reports of the impact of COVID-19 on pregnancy, prenatal Care, and infant feeding plans. Mcn Am. J. Matern. Child. Nurs. 2020, 46, 21–29. [Google Scholar] [CrossRef]
- Oncel, M.Y.; Akın, I.M.; Kanburoglu, M.K.; Tayman, C.; Coskun, S.; Narter, F.; Er, I.; Oncan, T.G.; Memisoglu, A.; Cetinkaya, M.; et al. A multicenter study on epidemiological and clinical characteristics of 125 newborns born to women infected with COVID-19 by Turkish Neonatal Society. Eur. J. Pediatr. 2020, 1–10. [Google Scholar] [CrossRef]
- Hull, N.; Kam, R.L.; Gribble, K.D. Providing breastfeeding support during the COVID-19 pandemic: Concerns of mothers who contacted the Australian Breastfeeding Association. medRxiv (pre-print) 2020. [Google Scholar] [CrossRef]
- Kumar, S.; Rathore, P.; Shweta, V.K.; Haokip, N.; Thankachan, A.; Bhatnagar, S.; Kumar, B. Why I can’t breastfeed my new-born baby? Psychosocial dilemma of a COVID-positive post-LSCS mother. Indian J. Palliat. Care 2020, 26, S150–S152. [Google Scholar] [CrossRef]
- Snyder, K.; Worlton, G. Social support during COVID-19: Perspectives of breastfeeding mothers. Breastfeed. Med. 2020. [Google Scholar] [CrossRef]
- Popofsky, S.; Noor, A.; Leavens-Maurer, J.; Quintos-Alagheband, M.L.; Mock, A.; Vinci, A.; Magri, E.; Akerman, M.; Noyola, E.; Rigaud, M.; et al. Impact of maternal severe acute respiratory syndrome coronavirus 2 detection on breastfeeding due to infant separation at birth. Pediatrics 2021, 226, 64–70. [Google Scholar] [CrossRef]
- Zanardo, V.; Tortora, D.; Guerrini, P.; Garani, G.; Severino, L.; Soldera, G.; Straface, G. Infant feeding initiation practices in the context of COVID-19 lockdown. Early Hum. Dev. 2021, 152, 105286. [Google Scholar] [CrossRef] [PubMed]
- Spatz, D.L.; Froh, E.B. Birth and breastfeeding in the hospital setting during the COVID-19 pandemic. Mcn Am. J. Matern. Child. Nurs. 2021, 46, 30–35. [Google Scholar] [CrossRef]
- Dib, S.; Rougeaux, E.; Vázquez-Vázquez, A.; Wells, J.C.K.; Fewtrell, M. Maternal mental health and coping during the COVID-19 lockdown in the UK: Data from the COVID-19 New Mum Study. Int. J. Gynaecol. Obs. 2020, 151, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Howard, L.M.; Khalifeh, H. Perinatal mental health: A review of progress and challenges. World Psychiatry 2020, 19, 313–327. [Google Scholar] [CrossRef]
- Lancaster, C.A.; Gold, K.J.; Flynn, H.A.; Yoo, H.; Marcus, S.M.; Davis, M.M. Risk factors for depressive symptoms during pregnancy: A systematic review. Am. J. Obs. Gynecol. 2010, 202, 5–14. [Google Scholar] [CrossRef] [Green Version]
- Biaggi, A.; Conroy, S.; Pawlby, S.; Pariante, C.M. Identifying the women at risk of antenatal anxiety and depression: A systematic review. J. Affect. Disord. 2016, 191, 62–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uvnäs-Moberg, K. Oxytocin may mediate the benefits of positive social interaction and emotions. Psychoneuroendocrinology 1998, 23, 819–835. [Google Scholar] [CrossRef]
- Uvnäs-Moberg, K.; Widström, A.M.; Marchini, G.; Winberg, J. Release of GI hormones in mother and infant by sensory stimulation. Acta Paediatr. 1987, 76, 851–860. [Google Scholar] [CrossRef] [PubMed]
- Kim, P.; Feldman, R.; Mayes, L.C.; Eicher, V.; Thompson, N.; Leckman, J.F.; Swain, J.E. Breastfeeding, brain activation to own infant cry, and maternal sensitivity. J. Child. Psychol. Psychiatry 2011, 52, 907–915. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dias, C.C.; Figueiredo, B. Breastfeeding and depression: A systematic review of the literature. J. Affect Disord. 2015, 171, 142–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watkinson, M.; Murray, C.; Simpson, J. Maternal experiences of embodied emotional sensations during breast feeding: An Interpretative Phenomenological Analysis. Midwifery 2016, 36, 53–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sighaldeh, S.S.; Kalan, M.E. Care of newborns born to mothers with COVID-19 infection; a review of existing evidence. J. Matern. Fetal Neonatal Med. 2020, 1–13. [Google Scholar] [CrossRef]
- Palmquist, A.E.L.; Holdren, S.M.; Fair, C.D. It was all taken away: Lactation, embodiment, and resistance among mothers caring for their very-low-birth-weight infants in the neonatal intensive care unit. Soc. Sci. Med. 2020, 244, 112648. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention, CDC. Coronavirus Disease 2019 (COVID-19): Considerations for Inpatient Obstetric Healthcare Settings. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/inpatient-obstetric-healthcare-guidance.html (accessed on 13 November 2020).
- Royal College of Obstetricians and Gynecologists, RCOG. Coronavirus (COVID-19) Infection in Pregnancy: Information for Healthcare Professionals. Available online: https://www.rcog.org.uk/coronavirus-pregnancy (accessed on 13 November 2020).
- Spatz, D.L. Getting it right—The critical window to effectively establish lactation. Infant 2020, 16, 58–60. [Google Scholar]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Benzies, K.M.; Premji, S.; Hayden, K.A.; Serrett, K. State-of-the-evidence reviews: Advantages and challenges of including grey literature. Worldviews Evid. Based Nurs. 2006, 3, 55–61. [Google Scholar] [CrossRef]


{kind=link}
| Study | Country | Study Design | Participants (N) | Mean Maternal Age (Years) | Infant’s Age | COVID-19 Diagnosis | Mental Health Outcomes | Main Findings |
| [2] | Belgium | Cross-sectional | 3445 | Yes | Experience of anxiety and depression symptoms | |||
| [36] | Belgium | Cross-sectional | 3823 | 32 | n = 8 | No | Overall, the COVID-19 pandemic only affected the duration and frequency of feeds; Perception of reduced support | |
| [37] | United Kingdom | Cross-sectional | 1049 (before lockdown) | 31.7 | M = 5.9 months | No | Yes | Reported loss of motherhood experiences; Perception of insufficient feeding support |
| 316 (during lockdown) | 31.4 | M = 1.27 months | No | |||||
| [13] | United Kingdom | Mixed methods | 1290 | 30.92 | M = 13.24 weeks | Unclear | No | Women reported both positive and negative breastfeeding experiences during the COVID-19 pandemic |
| [38] * | United States | Cross-sectional descriptive | 258 | 30.7 | N.A. | No | No | Women reported changing their breastfeeding plans due to the COVID-19 pandemic |
| [39] | Turkey | Multicenter cohort | 125 | 30–39 weeks | n = 125 | No | Lower rates of breastfeeding compared to formula and expressed breastmilk | |
| [40] ** | Australia | Cross-sectional | 336 | n = 25 | Yes | Significant anxiety related to breastfeeding | ||
| [41] | India | Case report | 1 | 26 | 28 weeks | n = 1 | Yes | Feelings of guilt and decreased perception of efficacy |
| [42] | United States | Cross-sectional phenomenological qualitative | 29 | 29.93 | M = 3,86 months | Yes | Heightened stress; Negative influence of COVID-19 pandemic on support | |
| Study | Country | Study Design | Participants (N) | Mean Maternal Age (Years) | Infant’s Age | COVID-19 Diagnosis | Mental Health Outcomes | Relevant Results |
| [43] | United States | Observational longitudinal cohort | 85 | n = 85 | No | Separation of mother–infant impacted negatively on breastfeeding rates | ||
| [44] | Italy | Non-concurrent case control | 152 (delivered during lockdown) | 33.47 | No | Lower depression symptoms in mothers who breastfed | ||
| 147 (delivered in 2019) | 33.18 | Yes | ||||||
| [45] | United States | Case series | 3 | 29 | Up to 67 days | No | No | Mothers experienced disruptions in support |
| 31 | Up to 58 days | No | ||||||
| 33 | Up to 40 days | No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pacheco, F.; Sobral, M.; Guiomar, R.; de la Torre-Luque, A.; Caparros-Gonzalez, R.A.; Ganho-Ávila, A. Breastfeeding during COVID-19: A Narrative Review of the Psychological Impact on Mothers. Behav. Sci. 2021, 11, 34. https://doi.org/10.3390/bs11030034
Pacheco F, Sobral M, Guiomar R, de la Torre-Luque A, Caparros-Gonzalez RA, Ganho-Ávila A. Breastfeeding during COVID-19: A Narrative Review of the Psychological Impact on Mothers. Behavioral Sciences. 2021; 11(3):34. https://doi.org/10.3390/bs11030034
Chicago/Turabian StylePacheco, Francisca, Mónica Sobral, Raquel Guiomar, Alejandro de la Torre-Luque, Rafael A. Caparros-Gonzalez, and Ana Ganho-Ávila. 2021. "Breastfeeding during COVID-19: A Narrative Review of the Psychological Impact on Mothers" Behavioral Sciences 11, no. 3: 34. https://doi.org/10.3390/bs11030034