Lack of Durable Remission with Conventional-Dose Total Skin Electron Therapy for the Management of Sezary Syndrome and Multiply Relapsed Mycosis Fungoides

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Characterisitics of Eligible Patients
2.2. Conventional-Dose Total Skin Electron Therapy
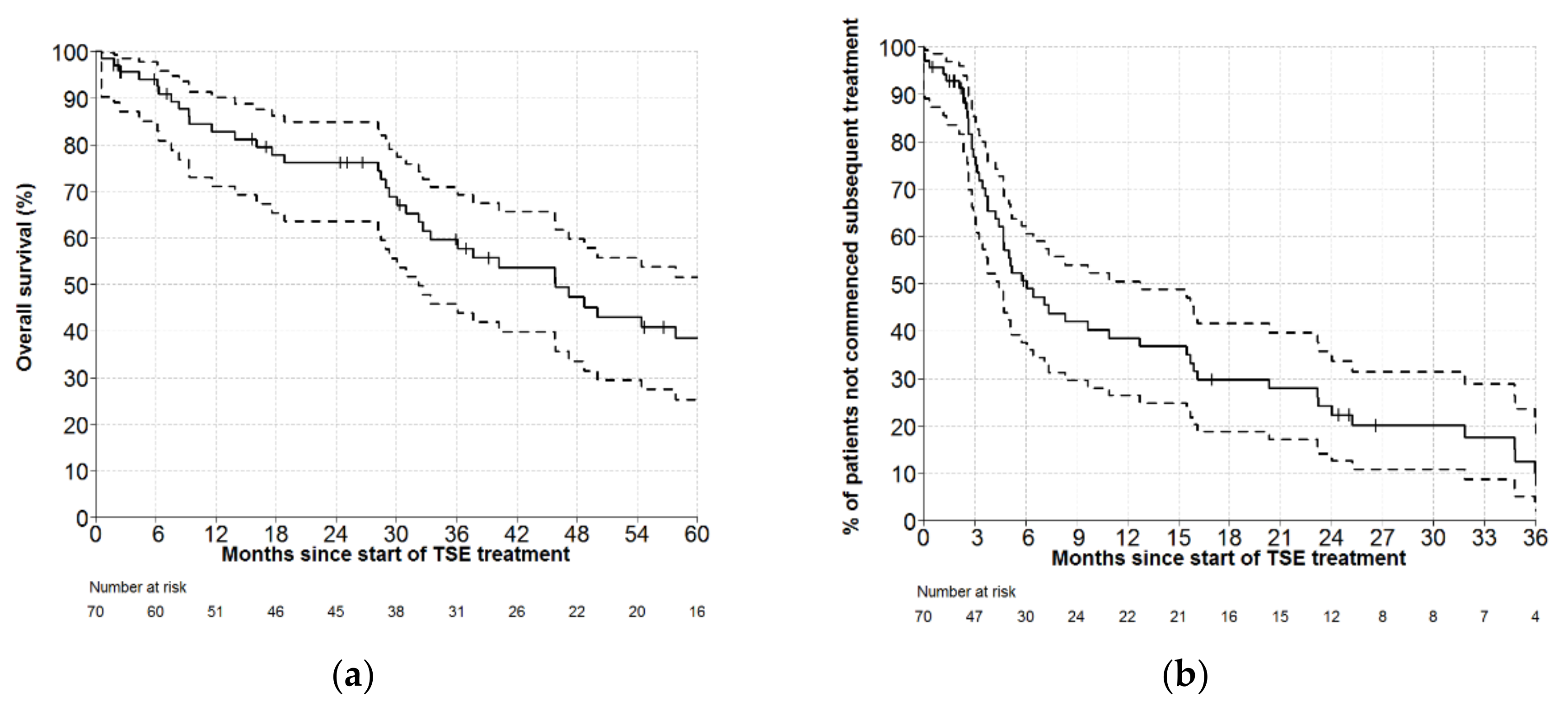
2.3. Overall Survival of the Whole Cohort
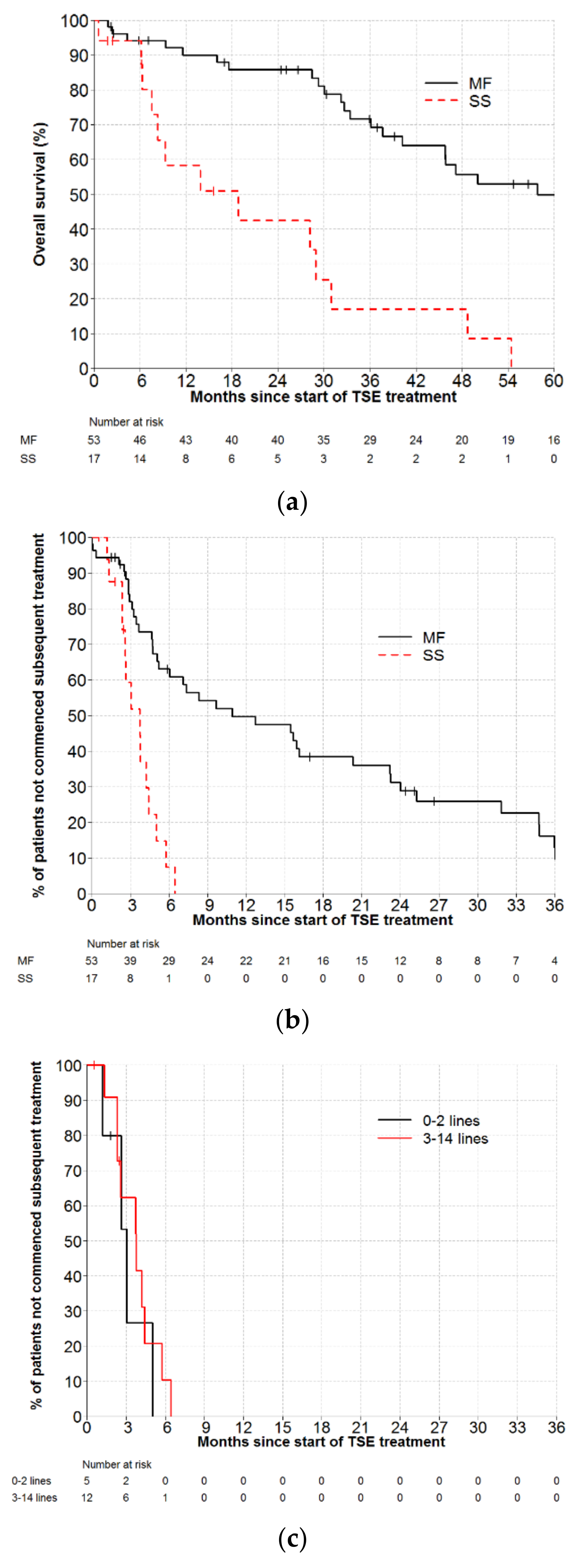
2.4. Overall Survival and Time to Next Treatment in Patients with Sezary Syndrome
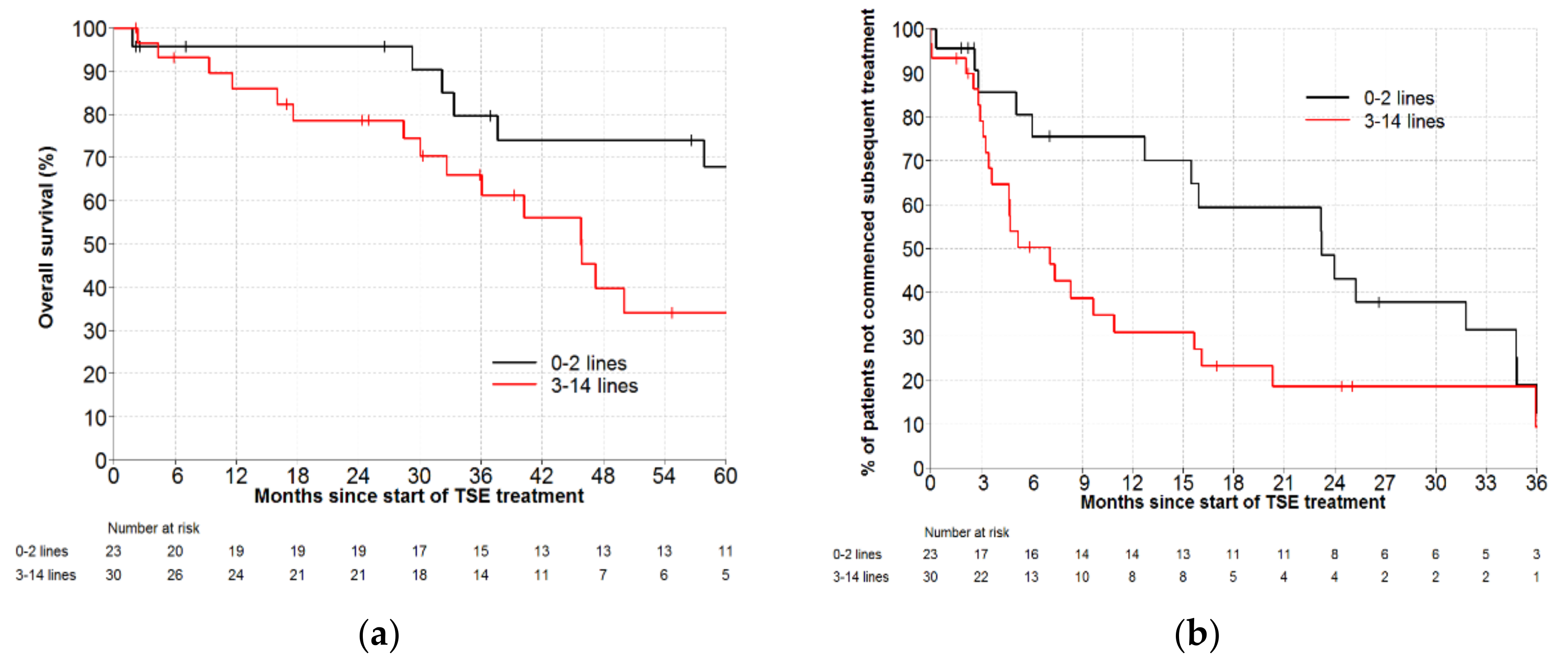
2.5. Overall Survival and Time to Next Treatment in Heavily Pre-Treated Patients with Mycosis Fungoides, According to Number of Prior Lines of Therapy
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hughes, C.F.; Khot, A.; McCormack, C.; Lade, S.; Westerman, D.A.; Twigger, R.; Buelens, O.; Newland, K.; Tam, C.; Dickinson, M.; et al. Lack of durable disease control with chemotherapy for mycosis fungoides and Sezary syndrome: A comparative study of systemic therapy. Blood 2015, 125, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Quaglino, P.; Maule, M.; Prince, H.M.; Porcu, P.; Horwitz, S.; Duvic, M.; Talpur, R.; Vermeer, M.; Bagot, M.; Guitart, J.; et al. Global patterns of care in advanced stage mycosis fungoides/Sezary syndrome: A multicenter retrospective follow-up study from the Cutaneous Lymphoma International Consortium. Ann. Oncol. 2017, 28, 2517–2525. [Google Scholar] [CrossRef] [PubMed]
- Photiou, L.; van der Weyden, C.; McCormack, C.; Miles Prince, H. Systemic treatment options for advanced-stage Mycosis Fungoides and Sezary syndrome. Curr. Oncol. Rep. 2018, 20, 32. [Google Scholar] [CrossRef] [PubMed]
- Whittaker, S.J.; Foss, F.M. Efficacy and tolerability of currently available therapies for the Mycosis Fungoides and Sezary syndrome variants of cutaneous T-cell lymphoma. Cancer Treat. Rev. 2007, 33, 146–160. [Google Scholar] [CrossRef]
- Trautinger, F.; Eder, J.; Assaf, C.; Bagot, M.; Cozzio, A.; Dummer, R.; Gniadecki, R.; Klemke, C.D.; Ortiz-Romero, P.L.; Papadavid, E.; et al. European Organisation for Research and Treatment of Cancer consensus recommendations for the treatment of Mycosis Fungoides/Sezary syndrome—Update 2017. Eur. J. Cancer 2017, 77, 57–74. [Google Scholar] [CrossRef]
- Gilson, D.; Whittaker, S.J.; Child, F.J.; Scarisbrick, J.J.; Illidge, T.M.; Parry, E.J.; Mohd Mustapa, M.F.; Exton, L.S.; Kanfer, E.; Rezvani, K.; et al. British Association of Dermatologists and U.K. Cutaneous Lymphoma Group guidelines for the management of primary cutaneous lymphomas 2018. Br. J. Dermatol. 2018, 180, 496–526. [Google Scholar] [CrossRef] [Green Version]
- Chowdhary, M.; Song, A.; Zaorsky, N.G.; Shi, W. Total skin electron beam therapy in mycosis fungoides-a shift towards lower dose? Chin. Clin. Oncol. 2019, 8, 9. [Google Scholar] [CrossRef]
- Elsayad, K.; Bauch, J.; Moustakis, C.; Reinartz, G.; Kriz, J.; Haverkamp, U.; Eich, H.T.T. Total Skin Electron Beam Therapy for Mycosis Fungoides and Sézary Syndrome: The Influence of Delivered Radiation Dose on the Clinical Outcome. Int. J. Radiat. Oncol. Biol. Phys. 2015, 93, E450. [Google Scholar] [CrossRef]
- Hoppe, R.T.; Fuks, Z.; Bagshaw, M.A. The rationale for curative radiotherapy in mycosis fungoides. Int. J. Radiat. Oncol. Biol. Phys. 1977, 2, 843–851. [Google Scholar] [CrossRef]
- Jones, G.W.; Tadros, A.; Hodson, D.I.; Rosenthal, D.; Roberts, J.; Thorson, B. Prognosis with newly diagnosed mycosis fungoides after total skin electron radiation of 30 or 35 GY. Int. J. Radiat. Oncol. Biol. Phys. 1994, 28, 839–845. [Google Scholar] [CrossRef]
- Jones, G.W.; Rosenthal, D.; Wilson, L.D. Total skin electron radiation for patients with erythrodermic cutaneous T-cell lymphoma (Mycosis fungoides and the Sezary syndrome). Cancer 1999, 85, 1985–1995. [Google Scholar] [CrossRef]
- Hanel, W.; Briski, R.; Ross, C.W.; Anderson, T.F.; Kaminski, M.S.; Hristov, A.C.; Wilcox, R.A. A retrospective comparative outcome analysis following systemic therapy in Mycosis fungoides and Sezary syndrome. Am. J. Hematol. 2016, 91, E491–E495. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.H.; Ortiz-Romero, P.L.; Pro, B.; Sokol, L.; Scarisbrick, J.; Musiek, A.; Vermeer, M.; Dummer, R.; Halwani, A.; Fierro, M.; et al. Time to next treatment in patients with previously treated Cutaneous T-Cell Lymphoma (CTCL) receiving mogamulizumab or vorinostat: A post-hoc analaysis of the MAVORIC study. Hematol. Oncol. 2019, 37, 285–286. [Google Scholar] [CrossRef]
- Horwitz, S.M.; Scarisbrick, J.J.; Dummer, R.; Duvic, M.; Kim, Y.H.; Walewski, J.; Whittaker, S.; Quaglino, P.; Zinzani, P.L.; Wolter, P.; et al. Updated analyses of the international, open-label, randomized, phase 3 alcanza study: Longer-term evidence for superiority of brentuximab vedotin versus methotrexate or bexarotene for CD30-positive Cutaneous T-Cell Lymphoma (CTCL). Blood 2017, 130, 1509. [Google Scholar]
- Gao, C.; McCormack, C.; van der Weyden, C.; Goh, M.S.; Campbell, B.; Twigger, R.; Buelens, O.; Harrison, S.J.; Khoo, C.; Lade, S.; et al. Prolonged survival with the early use of a novel extracorporeal photopheresis regimen in patients with Sézary syndrome. Blood 2019. [Google Scholar] [CrossRef] [PubMed]
- Specht, L.; Dabaja, B.; Illidge, T.; Wilson, L.D.; Hoppe, R.T. Modern radiation therapy for primary cutaneous lymphomas: Field and dose guidelines from the International Lymphoma Radiation Oncology Group. Int. J. Radiat. Oncol. Biol. Phys. 2015, 92, 32–39. [Google Scholar] [CrossRef]
- Kamstrup, M.R.; Lindahl, L.M.; Gniadecki, R.; Iversen, L.; Skov, L.; Petersen, P.M.; Loft, A.; Specht, L. Low-dose total skin electron beam therapy as a debulking agent for cutaneous T-cell lymphoma: An open-label prospective phase II study. Br. J. Dermatol. 2012, 166, 399–404. [Google Scholar] [CrossRef]
- Kamstrup, M.R.; Gniadecki, R.; Iversen, L.; Skov, L.; Petersen, P.M.; Loft, A.; Specht, L. Low-dose (10-Gy) total skin electron beam therapy for cutaneous T-cell lymphoma: An open clinical study and pooled data analysis. Int. J. Radiat. Oncol. Biol. Phys. 2015, 92, 138–143. [Google Scholar] [CrossRef]
- Hoppe, R.T.; Harrison, C.; Tavallaee, M.; Bashey, S.; Sundram, U.; Li, S.; Million, L.; Dabaja, B.; Gangar, P.; Duvic, M.; et al. Low-dose total skin electron beam therapy as an effective modality to reduce disease burden in patients with mycosis fungoides: Results of a pooled analysis from 3 phase-II clinical trials. J. Am. Acad. Dermatol. 2015, 72, 286–292. [Google Scholar] [CrossRef]
- Morris, S.; Scarisbrick, J.; Frew, J.; Irwin, C.; Grieve, R.; Humber, C.; Kuciejewska, A.; Bayne, S.; Weatherhead, S.; Child, F.; et al. The results of low-dose Total Skin Electron Beam radiation therapy (TSEB) in patients with Mycosis Fungoides from the UK Cutaneous Lymphoma Group. Int. J. Radiat. Oncol. Biol. Phys. 2017, 99, 627–633. [Google Scholar] [CrossRef]
- Kamstrup, M.R.; Specht, L.; Skovgaard, G.L.; Gniadecki, R. A prospective, open-label study of low-dose total skin electron beam therapy in mycosis fungoides. Int. J. Radiat. Oncol. Biol. Phys. 2008, 71, 1204–1207. [Google Scholar] [CrossRef] [PubMed]
- Elsayad, K.; Kriz, J.; Moustakis, C.; Scobioala, S.; Reinartz, G.; Haverkamp, U.; Willich, N.; Weishaupt, C.; Stadler, R.; Sunderkotter, C.; et al. Total skin electron beam for primary cutaneous T-cell lymphoma. Int. J. Radiat. Oncol. Biol. Phys. 2015, 93, 1077–1086. [Google Scholar] [CrossRef] [PubMed]
- Rivers, C.I.; Singh, A.K. Total skin electron beam therapy for Mycosis Fungoides revisited with adjuvant systemic therapy. Clin. Lymphoma Myeloma Leuk 2019, 19, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Georgakopoulos, I.; Papadavid, E.; Platoni, K.; Dilvoi, M.; Patatoukas, G.; Kypraiou, E.; Nikolaou, V.; Efstathopoulos, E.; Kelekis, N.; Kouloulias, V. Clinical application of Total Skin Electron Beam (TSEB) therapy for the management of T cell cutaneous lymphomas. The evolving role of low dose (12Gy) treatment schedule. Clin. Transl. Radiat. Oncol. 2019, 15, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Taverniers, A.; Du-Thanh, A.; Charissoux, M.; Kerr, C.; Dereure, O. Low- vs. middle-dose total skin electron beam therapy for Mycosis Fungoides: An efficiency-based retrospective survey of skin response. Acta Derm. Venereol. 2019, 99, 544–550. [Google Scholar] [CrossRef]
- Dault, J.B.; Slade, A.N.; Zhao, S.; Song, S. Comparison of low-dose and standard-dose total skin electron beam therapy in Mycosis Fungoides. Leuk. Lymphoma 2019. [Google Scholar] [CrossRef]
- Scarisbrick, J.J.; Quaglino, P.; Prince, H.M.; Papadavid, E.; Hodak, E.; Bagot, M.; Servitje, O.; Berti, E.; Ortiz-Romero, P.; Stadler, R.; et al. The PROCLIPI international registry of early-stage Mycosis Fungoides identifies substantial diagnostic delay in most patients. Br. J. Dermatol. 2019, 181, 350–357. [Google Scholar] [CrossRef]
- Olsen, E.; Vonderheid, E.; Pimpinelli, N.; Willemze, R.; Kim, Y.; Knobler, R.; Zackheim, H.; Duvic, M.; Estrach, T.; Lamberg, S.; et al. Revisions to the staging and classification of Mycosis Fungoides and Sezary syndrome: A proposal of the International Society for Cutaneous Lymphomas (ISCL) and the cutaneous lymphoma task force of the European Organization of Research and Treatment of Cancer (EORTC). Blood 2007, 110, 1713–1722. [Google Scholar] [CrossRef]
- Olsen, E.A.; Whittaker, S.; Kim, Y.H.; Duvic, M.; Prince, H.M.; Lessin, S.R.; Wood, G.S.; Willemze, R.; Demierre, M.-F.; Pimpinelli, N.; et al. Clinical end points and response criteria in Mycosis Fungoides and Sézary syndrome: A consensus statement of the international society for cutaneous lymphomas, the United States Cutaneous Lymphoma Consortium, and the cutaneous lymphoma task force of the European Organisation for Research and Treatment of Cancer. J. Clin. Oncol. 2011, 29, 2598–2607. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2015; Available online: http://www.R-project.org/.




{kind=link}
{kind=link}
{kind=link}
| Variable | Total (n = 70) | MF (n = 53) | SS (n = 17) |
|---|---|---|---|
| Gender | |||
| Female | 28 (40.0%) | 19 (35.8%) | 9 (52.9%) |
| Male | 42 (60.0%) | 34 (64.2%) | 8 (47.1%) |
| Age at diagnosis (years) | |||
| Median (range) | 66 (14–81) | 63 (14–81) | 68 (49–81) |
| Diagnosis | |||
| Mycosis fungoides (MF) | 52 (74.3%) | 52 (98.1%) | 0 (0.0%) |
| Peripheral T-cell lymphoma, not otherwise specified (PTCL-NOS) | 1 (1.4%) | 1 (1.9%) | 0 (0.0%) |
| Sezary syndrome (SS) | 17 (24.3%) | 0 (0.0%) | 17 (100.0%) |
| Subtype | |||
| Folliculotropic | 7 (10.0%) | 7 (13.2%) | 0 (0.0%) |
| Poikilodermatous | 1 (1.4%) | 1 (1.9%) | 0 (0.0%) |
| Subtype not specified | 62 (88.6%) | 45 (84.9%) | 17 (100.0%) |
| Large cell transformation | |||
| Prior to cdTSE | 7 (10.0%) | 6 (11.3%) | 1 (5.9%) |
| After cdTSE | 11 (15.7%) | 9 (17.0%) | 2 (11.8%) |
| Stage at diagnosis (missing n = 1) 1 | |||
| IA | 5 (7.1%) | 5 (9.4%) | 0 (0.0%) |
| IB | 24 (34.3%) | 23 (43.4%) | 1 (5.9%) |
| IIA | 2 (2.9%) | 2 (3.8%) | 0 (0.0%) |
| IIB | 17 (24.3%) | 16 (30.2%) | 1 (5.9%) |
| III | 10 (14.3%) | 4 (7.5%) | 6 (35.3%) |
| IVA1 | 8 (11.4%) | 1 (1.9%) | 7 (41.2%) |
| IVA2 | 2 (2.9%) | 1 (1.9%) | 1 (5.9%) |
| IVB | 2 (2.9%) | 1 (1.9%) | 1 (5.9%) |
| ECOG at diagnosis (missing n = 3) | |||
| 0 | 57 (85.1%) | 47 (92.2%) | 10 (62.5%) |
| 1 | 10 (14.9%) | 4 (7.8%) | 6 (37.5%) |
| T Stage at cdTSE | |||
| 1 | 1 (1.4%) | 1 (1.9%) | 0 (0.0%) |
| 2 | 34 (48.6%) | 32 (60.4%) | 2 (11.8%) 2 |
| 3 | 15 (21.4%) | 14 (26.4%) | 1 (5.9%) 2 |
| 4 | 20 (28.6%) | 6 (11.3%) | 14 (82.4%) |
| ECOG at cdTSE (missing n = 7) | |||
| 0 | 36 (57.1%) | 33 (71.7%) | 3 (17.6%) |
| 1 | 21 (33.3%) | 10 (21.7%) | 11 (64.7%) |
| 2 | 4 (6.3%) | 2 (4.3%) | 2 (11.8%) |
| 3 | 2 (3.2%) | 1 (2.2%) | 1 (5.9%) |
| Treatment lines prior to cdTSE | |||
| Median (range) | 4 (0–14) | 3 (0–14) | 7 (0–13) |
| Fractionation schedule | |||
| 5 fractions per week | 33 (47.1%) | 22 (41.5%) | 11 (64.7%) |
| 4 fractions per week | 1 (1.4%) | 1 (1.9%) | 0 (0.0%) |
| 3 fractions per week | 34 (48.6%) | 28 (52.8%) | 6 (35.3%) |
| 2 fractions per week | 2 (2.9%) | 2 (3.8%) | 0 (0.0%) |
| Unscheduled treatment disruptions or failure to complete cdTSE | |||
| Yes 3 | 8 (11.4%) | 5 (9.4%) | 3 (17.6%) |
| Skin response following cdTSE (missing n = 3) | |||
| Overall skin response (complete or partial) | 62 (92.5%) | 48 (92.2%) | 14 (93.8%) |
| Stable disease | 4 (6.0%) | 3 (5.9%) | 1 (6.3%) |
| Progression | 1 (1.5%) | 1 (2.0%) | 0 (0.0%) |
| Therapy | Total (n = 70) | MF (n = 53) | SS (n = 17) |
|---|---|---|---|
| Phototherapy 1 | 43 (61.4%) | 34 (64.2%) | 9 (52.9%) |
| Methotrexate | 34 (48.6%) | 21 (39.6%) | 13 (76.5%) |
| Systemic corticosteroids | 32 (45.7%) | 20 (37.7%) | 12 (70.6%) |
| Interferon | 23 (32.9%) | 14 (26.4%) | 9 (52.9%) |
| Localised radiotherapy | 20 (28.6%) | 19 (35.8%) | 1 (5.9%) |
| Multi-agent chemotherapy | 16 (22.9%) | 8 (15.1%) | 8 (47.1%) |
| Histone deacetylase (HDAC) inhibitor | 13 (18.6%) | 7 (13.2%) | 6 (35.3%) |
| Single-agent chemotherapy | 11 (15.7%) | 7 (13.2%) | 4 (23.5%) |
| Extracorporeal photopheresis | 9 (12.9%) | 0 (0%) | 9 (52.9%) |
| Haematopoietic stem cell transplant 2 | 5 (7.1%)4 | 3 (5.7%) | 2 (11.8%) |
| Immunosuppressant 3 | 5 (7.1%) | 4 (7.5%) | 1 (5.9%) |
| Monoclonal antibodies 4 | 5 (7.1%) | 3 (5.7%) | 2 (11.8%) |
| Retinoid | 5 (7.1%) | 3 (5.7%) | 2 (11.8%) |
| Denileukin difitox | 2 (2.9%) | 0 (0%) | 2 (11.8%) |
| Bromodomain and extra-terminal motif (BET) inhibitor | 1 (1.4%) | 1 (1.9%) | 0 (0%) |
| Bortezomib | 1 (1.4%) | 1 (1.9%) | 0 (0%) |
| No prior therapy (cdTSE first-line) | 7 (10.0%) | 6 (11.3%) | 1 (5.9%) |
| Treatment | n | Median TTNT (Months) | TTNT 95% CI (Months) | 1-Year Free from Further Treatment (%) | 2-Years Free from Further Treatment (%) | Median Number of Previous Lines of Therapy |
|---|---|---|---|---|---|---|
| a-interferon | 68 | 8.7 | 6.0–18.0 | 41.7 | 29.1 | 1 |
| Low-dose methotrexate | 83 | 5.0 | 3.6–6.5 | 25.1 | 21.2 | 1 |
| Histone deacetylase (HDAC) inhibitors | 74 | 4.5 | 4.0–6.1 | 20.0 | 14.5 | 2 |
| Bexarotene | 20 | 7.3 | 2.6–110.8 | 47.4 | 36.8 | 1 |
| Alemtuzumab | 16 | 4.1 | 2.7–6.5 | 27.8 | 27.8 | 2.5 |
| Denileukin diftitox | 22 | 5.1 | 2.7–6.5 | 22.7 | 22.7 | 3 |
| Chemotherapy | 143 | 3.9 | 3.2–5.1 | 10.7 | 5.4 | 3 |
| Extracorporeal photophoresis (ECP) | 53 | 9.2 | 5.9–12.8 | 39.1 | 25.7 | 1 |
| Autologous SCT | 19 | 7.8 | 4.7–24.4 | 41.5 | 28.4 | 2 |
| Allogeneic SCT | 9 | 34.6 | 11.5–NA | 80.0 | 53.3 | 5 |
| cdTSE for MF 1 (current study) | 23 | 23.2 | 12.7–34.8 | 76 | 43 | 0–2 |
| 30 | 7.1 | 3.4–10.9 | 31 | 19 | 3–14 | |
| cdTSE for SS (current study) | 17 | 3.7 | 2.3–4.4 | 0 | 0 | 7 |
| Skin Stage | Description |
|---|---|
| T1 | Limited patches, papules, and/or plaques covering <10% of the skin surface. May further stratify into T1a (patch only) vs. T1b (plaque ± patch). |
| T2 | Patches, papules or plaques covering ≥10% of the skin surface. May further stratify into T2a (patch only) vs. T2b (plaque ± patch). |
| T3 | One or more tumours (≥1 cm diameter) |
| T4 | Confluence of erythema covering ≥80% body surface area |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campbell, B.A.; Ryan, G.; McCormack, C.; Tangas, E.; Bressel, M.; Twigger, R.; Buelens, O.; van der Weyden, C.; Prince, H.M. Lack of Durable Remission with Conventional-Dose Total Skin Electron Therapy for the Management of Sezary Syndrome and Multiply Relapsed Mycosis Fungoides. Cancers 2019, 11, 1758. https://doi.org/10.3390/cancers11111758
Campbell BA, Ryan G, McCormack C, Tangas E, Bressel M, Twigger R, Buelens O, van der Weyden C, Prince HM. Lack of Durable Remission with Conventional-Dose Total Skin Electron Therapy for the Management of Sezary Syndrome and Multiply Relapsed Mycosis Fungoides. Cancers. 2019; 11(11):1758. https://doi.org/10.3390/cancers11111758
Chicago/Turabian StyleCampbell, Belinda A., Gail Ryan, Christopher McCormack, Eleanor Tangas, Mathias Bressel, Robert Twigger, Odette Buelens, Carrie van der Weyden, and H. Miles Prince. 2019. "Lack of Durable Remission with Conventional-Dose Total Skin Electron Therapy for the Management of Sezary Syndrome and Multiply Relapsed Mycosis Fungoides" Cancers 11, no. 11: 1758. https://doi.org/10.3390/cancers11111758