The Validity and Predictive Value of Blood-Based Biomarkers in Prediction of Response in the Treatment of Metastatic Non-Small Cell Lung Cancer: A Systematic Review

 , , and
, , and
Abstract
:1. Introduction
2. Results
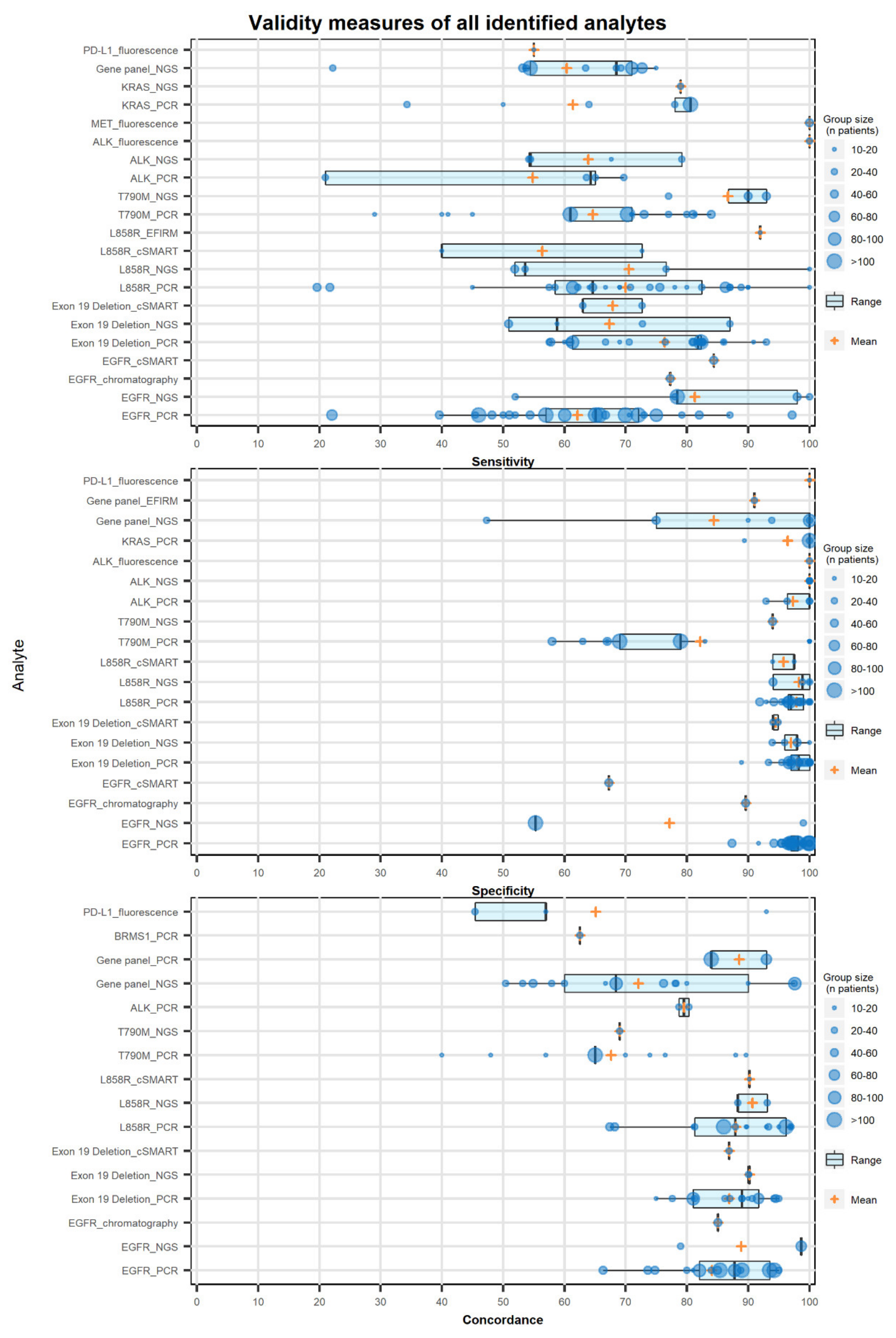
2.1. Extracted Data on the Validity of the Biomarker
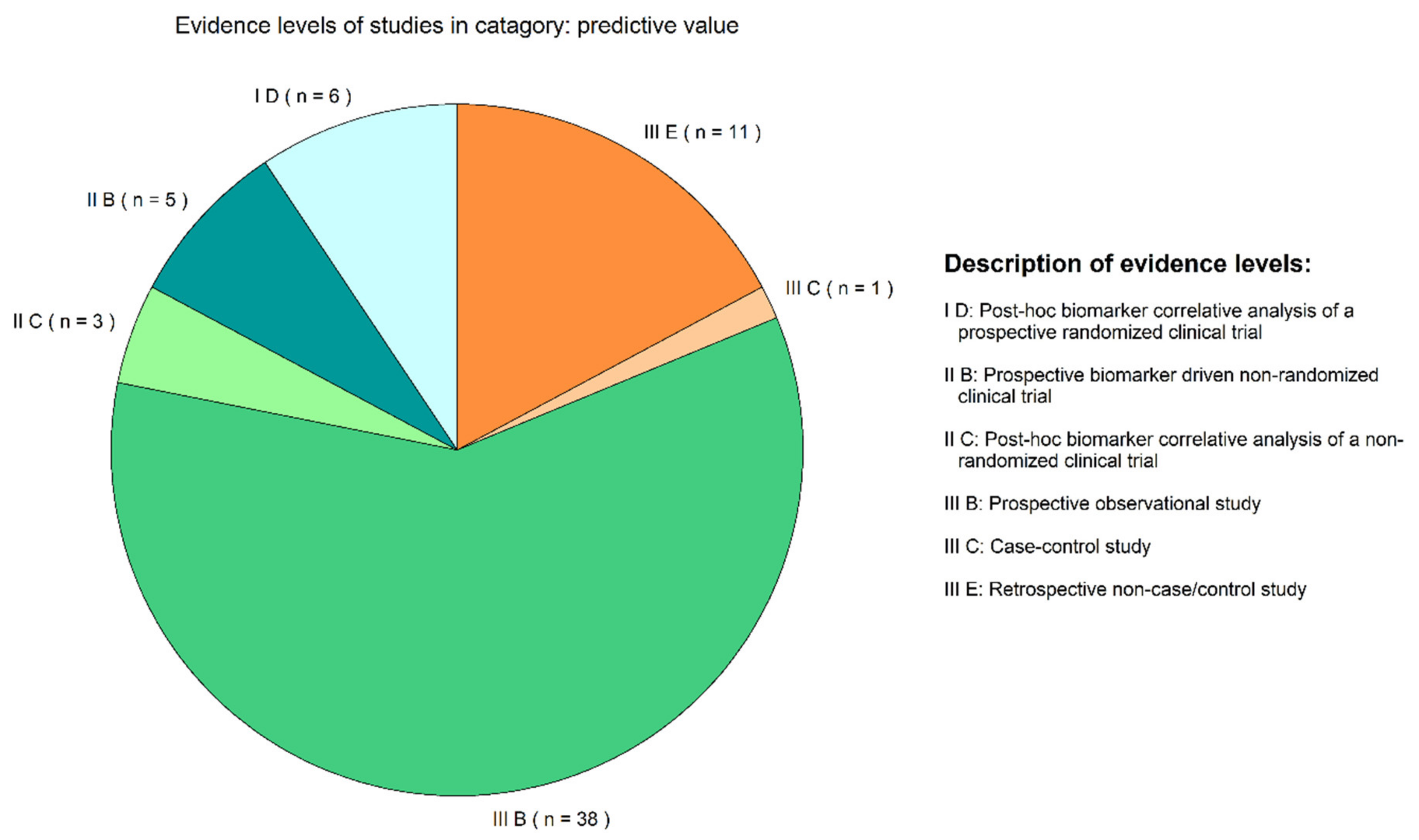
2.2. Study Evidence Levels for Predictive Biomarkers
2.3. Evidence of Predictive Value of a Biomarker Based on LBs
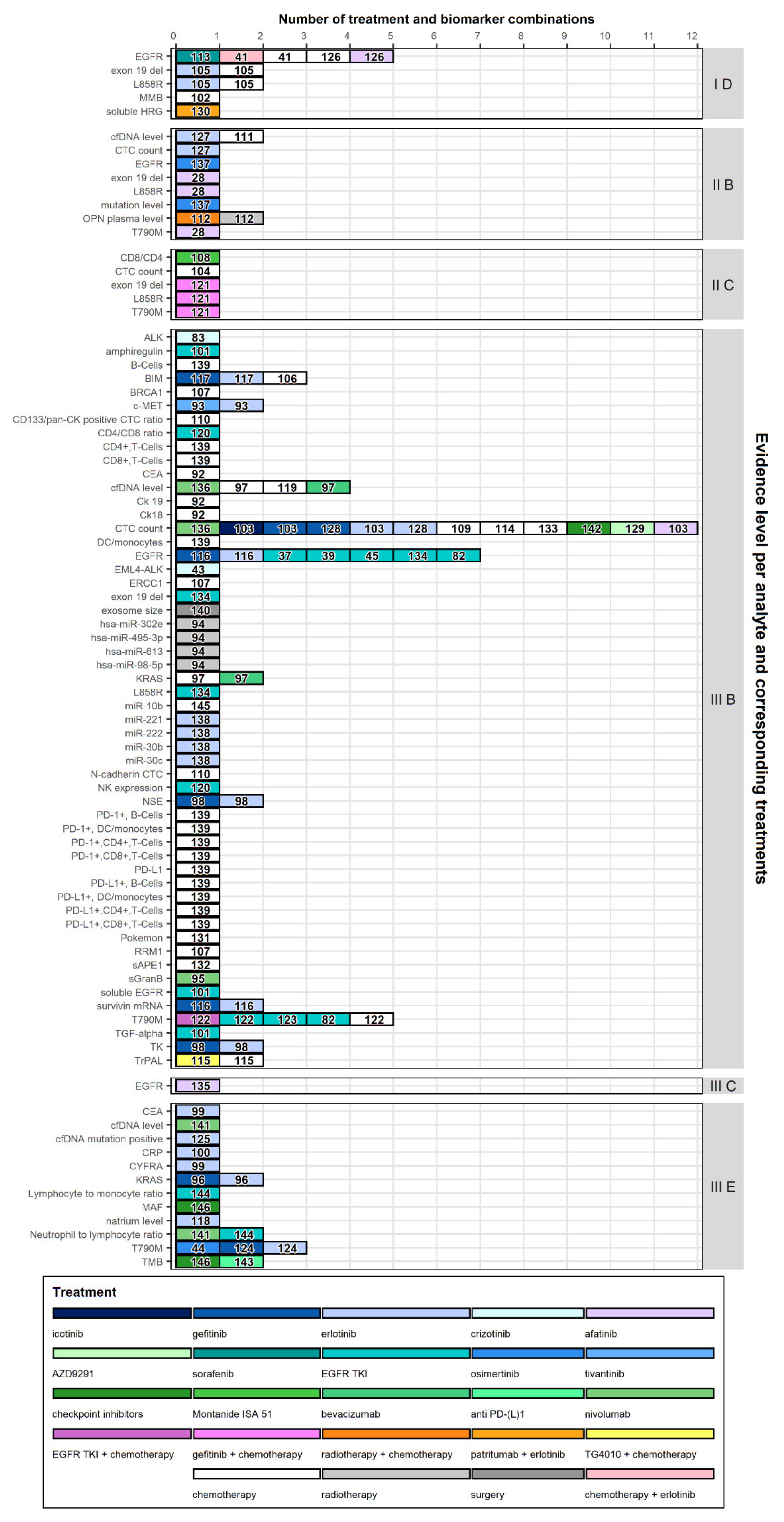
2.4. Evidence Level Per Analyte and Therapy
3. Discussion
4. Materials and Methods
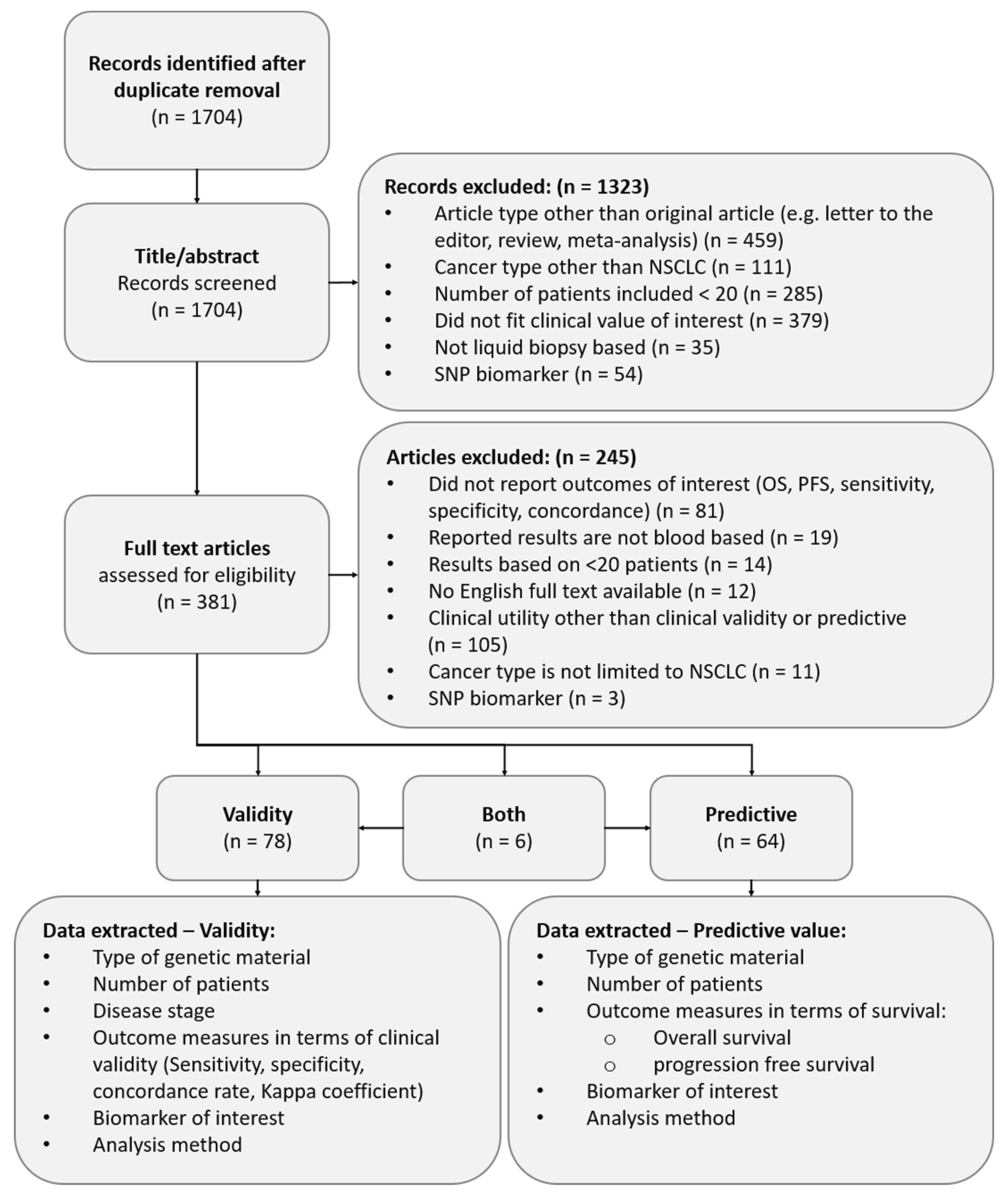
4.1. Eligibility Criteria
4.2. Search
4.3. Study Selection
4.4. Data Extraction
4.5. Evidence Classification
4.6. Data Interpretation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Global Cancer Observatory: Cancer Today; International Agency for Research on Cancer. Estimated Number of New Cases in 2018. Available online: http://gco.iarc.fr/ (accessed on 18 January 2019).
- Global Cancer Observatory: Cancer Today; International Agency for Research on Cancer. Estimated Number of Deaths in 2018. Available online: http://gco.iarc.fr (accessed on 18 January 2019).
- Organisation, N.C.C. Guideline Non Small Cell Lung Carcinoma; IKNL Oncoline: Utrecht, The Netherlands, 2015; Available online: www.oncoline.nl.
- Pakkala, S.; Ramalingam, S.S. Personalized therapy for lung cancer: Striking a moving target. JCI Insight 2018, 3, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, X.; Chen, H. Tumor heterogeneity and resistance to EGFR-targeted therapy in advanced nonsmall cell lung cancer: Challenges and perspectives. OncoTargets Ther. 2014, 7, 1689–1704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deng, Q.; Xie, B.; Wu, L.; Ji, X.; Li, C.; Feng, L.; Fang, Q.; Bao, Y.; Li, J.; Jin, S.; et al. Competitive evolution of NSCLC tumor clones and the drug resistance mechanism of first-generation EGFR-TKIs in Chinese NSCLC patients. Heliyon 2018, 4, e01031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ricordel, C.; Friboulet, L.; Facchinetti, F.; Soria, J.C. Molecular mechanisms of acquired resistance to third-generation EGFR-TKIs in EGFR T790M-mutant lung cancer. Ann. Oncol. 2018, 29, i28–i37. [Google Scholar] [CrossRef] [PubMed]
- Nosaki, K.; Satouchi, M.; Kurata, T.; Yoshida, T.; Okamoto, I.; Katakami, N.; Imamura, F.; Tanaka, K.; Yamane, Y.; Yamamoto, N.; et al. Re-biopsy status among non-small cell lung cancer patients in Japan: A retrospective study. Lung Cancer 2016, 101, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Uozu, S.; Imaizumi, K.; Yamaguchi, T.; Goto, Y.; Kawada, K.; Minezawa, T.; Okamura, T.; Akao, K.; Hayashi, M.; Isogai, S.; et al. Feasibility of tissue re-biopsy in non-small cell lung cancers resistant to previous epidermal growth factor receptor tyrosine kinase inhibitor therapies. BMC Pulm. Med. 2017, 17, 175. [Google Scholar] [CrossRef] [Green Version]
- Zanwar, S.; Noronha, V.; Joshi, A.; Patil, V.M.; Chougule, A.; Kumar, R.; More, S.; Goud, S.; Janu, A.; Mahajan, A.; et al. Repeat biopsy in epidermal growth factor receptor mutation-positive nonsmall cell lung cancer: Feasibility, limitations, and clinical utility in Indian patients. Indian J. Cancer 2017, 54, 280–284. [Google Scholar] [CrossRef]
- Ijzerman, M.J.; Berghuis, A.M.S.; De Bono, J.S.; Terstappen, L.W.M.M. Health economic impact of liquid biopsies in cancer management. Expert Rev. Pharm. Outcomes Res. 2018, 18, 593–599. [Google Scholar] [CrossRef]
- Buder, A.; Tomuta, C.; Filipits, M. The potential of liquid biopsies. Curr. Opin. Oncol. 2016, 28, 130–134. [Google Scholar] [CrossRef]
- Siravegna, G.; Marsoni, S.; Siena, S.; Bardelli, A. Integrating liquid biopsies into the management of cancer. Nat. Rev. Clin. Oncol. 2017, 14, 531–548. [Google Scholar] [CrossRef]
- Alegre, E.; Fusco, J.P.; Restituto, P.; Salas-Benito, D.; Rodriguez-Ruiz, M.E.; Andueza, M.P.; Pajares, M.J.; Patino-Garcia, A.; Pio, R.; Lozano, M.D.; et al. Total and mutated EGFR quantification in cell-free DNA from non-small cell lung cancer patients detects tumor heterogeneity and presents prognostic value. Tumour Biol. 2016, 37, 13687–13694. [Google Scholar] [CrossRef] [PubMed]
- Arriola, E.; Paredes-Lario, A.; Garcia-Gomez, R.; Diz-Tain, P.; Constenla, M.; Garcia-Giron, C.; Marquez, G.; Reck, M.; Lopez-Vivanco, G. Comparison of plasma ctDNA and tissue/cytology-based techniques for the detection of EGFR mutation status in advanced NSCLC: Spanish data subset from ASSESS. Clin. Transl. Oncol. 2018, 20, 1261–1267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balgkouranidou, I.; Chimonidou, M.; Milaki, G.; Tsarouxa, E.G.; Kakolyris, S.; Welch, D.R.; Georgoulias, V.; Lianidou, E.S. Breast cancer metastasis suppressor-1 promoter methylation in cell-free DNA provides prognostic information in non-small cell lung cancer. Br. J. Cancer 2014, 110, 2054–2062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chai, X.; Ren, P.; Wei, B.; Ma, J.; Mai, L.; Cram, D.S.; Song, Y.; Guo, Y. A comparative study of EGFR oncogenic mutations in matching tissue and plasma samples from patients with advanced non-small cell lung carcinoma. Clin. Chim. Acta 2016, 457, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Zhang, J.; Guan, T.; Yang, F.; Lou, F.; Chen, W.; Zhao, M.; Zhang, J.; Chen, S.; Wang, J. Comparison of plasma to tissue DNA mutations in surgical patients with non–small cell lung cancer. J. Thorac. Cardiovasc. Surg. 2017, 154, 1123–1131.e1122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, K.Z.; Lou, F.; Yang, F.; Zhang, J.B.; Ye, H.; Chen, W.; Guan, T.; Zhao, M.Y.; Su, X.X.; Shi, R.; et al. Circulating Tumor DNA Detection in Early-Stage Non-Small Cell Lung Cancer Patients by Targeted Sequencing. Sci. Rep. 2016, 6, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cui, S.; Zhang, W.; Xiong, L.; Pan, F.; Niu, Y.; Chu, T.; Wang, H.; Zhao, Y.; Jiang, L. Use of capture-based next-generation sequencing to detect ALK fusion in plasma cell-free DNA of patients with non-small-cell lung cancer. Oncotarget 2017, 8, 2771–2780. [Google Scholar] [CrossRef] [Green Version]
- Douillard, J.Y.; Ostoros, G.; Cobo, M.; Ciuleanu, T.; McCormack, R.; Webster, A.; Milenkova, T. First-line gefitinib in Caucasian EGFR mutation-positive NSCLC patients: A phase-IV, open-label, single-arm study. Br. J. Cancer 2014, 110, 55–62. [Google Scholar] [CrossRef] [Green Version]
- Duan, H.; Lu, J.; Lu, T.; Gao, J.; Zhang, J.; Xu, Y.; Wang, M.; Wu, H.; Liang, Z.; Liu, T. Comparison of EGFR mutation status between plasma and tumor tissue in non-small cell lung cancer using the Scorpion ARMS method and the possible prognostic significance of plasma EGFR mutation status. Int. J. Clin. Exp. Pathol. 2015, 8, 13136–13145. [Google Scholar]
- Guibert, N.; Delaunay, M.; Lusque, A.; Boubekeur, N.; Rouquette, I.; Clermont, E.; Mourlanette, J.; Gouin, S.; Dormoy, I.; Favre, G.; et al. PD-L1 expression in circulating tumor cells of advanced non-small cell lung cancer patients treated with nivolumab. Lung Cancer 2018, 120, 108–112. [Google Scholar] [CrossRef]
- Guibert, N.; Hu, Y.; Feeney, N.; Kuang, Y.; Plagnol, V.; Jones, G.; Howarth, K.; Beeler, J.F.; Paweletz, C.P.; Oxnard, G.R. Amplicon-based next-generation sequencing of plasma cell-free DNA for detection of driver and resistance mutations in advanced non-small cell lung cancer. Ann. Oncol. 2018, 29, 1049–1055. [Google Scholar] [CrossRef] [PubMed]
- Guibert, N.; Pradines, A.; Farella, M.; Casanova, A.; Gouin, S.; Keller, L.; Favre, G.; Mazieres, J. Monitoring KRAS mutations in circulating DNA and tumor cells using digital droplet PCR during treatment of KRAS-mutated lung adenocarcinoma. Lung Cancer 2016, 100, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Guo, N.; Lou, F.; Ma, Y.; Li, J.; Yang, B.; Chen, W.; Ye, H.; Zhang, J.B.; Zhao, M.Y.; Wu, W.J.; et al. Circulating tumor DNA detection in lung cancer patients before and after surgery. Sci. Rep. 2016, 6, 33519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, J.Y.; Choi, J.J.; Kim, J.Y.; Han, Y.L.; Lee, G.K. PNA clamping-assisted fluorescence melting curve analysis for detecting EGFR and KRAS mutations in the circulating tumor DNA of patients with advanced non-small cell lung cancer. BMC Cancer 2016, 16, 627. [Google Scholar] [CrossRef] [Green Version]
- He, J.; Tan, W.; Tang, X.; Ma, J. Variations in EGFR ctDNA Correlates to the Clinical Efficacy of Afatinib in Non Small Cell Lung Cancer with Acquired Resistance. Pathol. Oncol. Res. 2017, 23, 307–315. [Google Scholar] [CrossRef]
- Ilie, M.; Szafer-Glusman, E.; Hofman, V.; Chamorey, E.; Lalvee, S.; Selva, E.; Leroy, S.; Marquette, C.H.; Kowanetz, M.; Hedge, P.; et al. Detection of PD-L1 in circulating tumor cells and white blood cells from patients with advanced non-small-cell lung cancer. Ann. Oncol. 2018, 29, 193–199. [Google Scholar] [CrossRef]
- Ilie, M.; Szafer-Glusman, E.; Hofman, V.; Long-Mira, E.; Suttmann, R.; Darbonne, W.; Butori, C.; Lalvee, S.; Fayada, J.; Selva, E.; et al. Expression of MET in circulating tumor cells correlates with expression in tumor tissue from advanced-stage lung cancer patients. Oncotarget 2017, 8, 26112–26121. [Google Scholar] [CrossRef] [Green Version]
- Jenkins, S.; Yang, J.C.; Ramalingam, S.S.; Yu, K.; Patel, S.; Weston, S.; Hodge, R.; Cantarini, M.; Janne, P.A.; Mitsudomi, T.; et al. Plasma ctDNA Analysis for Detection of the EGFR T790M Mutation in Patients with Advanced Non-Small Cell Lung Cancer. J. Thorac. Oncol. 2017, 12, 1061–1070. [Google Scholar] [CrossRef] [Green Version]
- Kasahara, N.; Kenmotsu, H.; Serizawa, M.; Umehara, R.; Ono, A.; Hisamatsu, Y.; Wakuda, K.; Omori, S.; Nakashima, K.; Taira, T.; et al. Plasma epidermal growth factor receptor mutation testing with a chip-based digital PCR system in patients with advanced non-small cell lung cancer. Lung Cancer 2017, 106, 138–144. [Google Scholar] [CrossRef]
- Krug, A.K.; Enderle, D.; Karlovich, C.; Priewasser, T.; Bentink, S.; Spiel, A.; Brinkmann, K.; Emenegger, J.; Grimm, D.G.; Castellanos-Rizaldos, E.; et al. Improved EGFR mutation detection using combined exosomal RNA and circulating tumor DNA in NSCLC patient plasma. Ann. Oncol. 2018, 29, 700–706. [Google Scholar] [CrossRef] [Green Version]
- Lam, D.C.L.; Tam, T.C.C.; Lau, K.M.K.; Wong, W.M.; Hui, C.K.M.; Lam, J.C.M.; Wang, J.K.L.; Lui, M.M.S.; Ho, J.C.M.; Ip, M.S.M. Plasma EGFR mutation detection associated with survival outcomes in advanced-stage lung cancer. Clin. Lung Cancer 2015, 16, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.Y.; Qing, X.; Xiumin, W.; Yali, B.; Chi, S.; Bak, S.H.; Lee, H.Y.; Sun, J.M.; Lee, S.H.; Ahn, J.S.; et al. Longitudinal monitoring of EGFR mutations in plasma predicts outcomes of NSCLC patients treated with EGFR TKIs: Korean Lung Cancer Consortium (KLCC-12-02). Oncotarget 2016, 7, 6984–6993. [Google Scholar] [CrossRef] [Green Version]
- Li, F.; Huang, J.; Ji, D.; Meng, Q.; Wang, C.; Chen, S.; Wang, X.; Zhu, Z.; Jiang, C.; Shi, Y.; et al. Utility of urinary circulating tumor DNA for EGFR mutation detection in different stages of non-small cell lung cancer patients. Clin. Transl. Oncol. 2017, 19, 1283–1291. [Google Scholar] [CrossRef]
- Li, X.; Ren, R.; Ren, S.; Chen, X.; Cai, W.; Zhou, F.; Zhang, Y.; Su, C.; Zhao, C.; Li, J.; et al. Peripheral blood for epidermal growth factor receptor mutati detection in non-small cell lung cancer patients. Transl. Oncol. 2014, 7, 341–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, L.; Liu, H.; Shao, D.; Liu, Z.; Wang, J.; Deng, Q.; Tang, H.; Yang, H.; Zhang, Y.; Qiu, Y.; et al. Development and clinical validation of a circulating tumor DNA test for the identification of clinically actionable mutations in nonsmall cell lung cancer. Genes Chromosomes Cancer 2018, 57, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Ma, M.; Shi, C.; Qian, J.; Teng, J.; Zhong, H.; Han, B. Comparison of plasma and tissue samples in epidermal growth factor receptor mutation by ARMS in advanced non-small cell lung cancer. Gene 2016, 592, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Mayo-de-Las-Casas, C.; Jordana-Ariza, N.; Garzon-Ibanez, M.; Balada-Bel, A.; Bertran-Alamillo, J.; Viteri-Ramirez, S.; Reguart, N.; Munoz-Quintana, M.A.; Lianes-Barragan, P.; Camps, C.; et al. Large scale, prospective screening of EGFR mutations in the blood of advanced NSCLC patients to guide treatment decisions. Ann. Oncol. 2017, 28, 2248–2255. [Google Scholar] [CrossRef]
- Mok, T.; Wu, Y.L.; Lee, J.S.; Yu, C.J.; Sriuranpong, V.; Sandoval-Tan, J.; Ladrera, G.; Thongprasert, S.; Srimuninnimit, V.; Liao, M.; et al. Detection and dynamic changes of EGFR mutations from circulating tumor DNA as a predictor of survival outcomes in NSCLC Patients treated with first-line intercalated erlotinib and chemotherapy. Clin. Cancer Res. 2015, 21, 3196–3203. [Google Scholar] [CrossRef] [Green Version]
- Muller, J.N.; Falk, M.; Talwar, J.; Neemann, N.; Mariotti, E.; Bertrand, M.; Zacherle, T.; Lakis, S.; Menon, R.; Gloeckner, C.; et al. Concordance between Comprehensive Cancer Genome Profiling in Plasma and Tumor Specimens. J. Thorac. Oncol. 2017, 12, 1503–1511. [Google Scholar] [CrossRef] [Green Version]
- Nilsson, R.J.; Karachaliou, N.; Berenguer, J.; Gimenez-Capitan, A.; Schellen, P.; Teixido, C.; Tannous, J.; Kuiper, J.L.; Drees, E.; Grabowska, M.; et al. Rearranged EML4-ALK fusion transcripts sequester in circulating blood platelets and enable blood-based crizotinib response monitoring in non-small-cell lung cancer. Oncotarget 2016, 7, 1066–1075. [Google Scholar] [CrossRef] [Green Version]
- Oxnard, G.R.; Thress, K.S.; Alden, R.S.; Lawrance, R.; Paweletz, C.P.; Cantarini, M.; Yang, J.C.; Barrett, J.C.; Janne, P.A. Association Between Plasma Genotyping and Outcomes of Treatment with Osimertinib (AZD9291) in Advanced Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2016, 34, 3375–3382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Que, D.; Xiao, H.; Zhao, B.; Zhang, X.; Wang, Q.; Xiao, H.; Wang, G. EGFR mutation status in plasma and tumor tissues in non-small cell lung cancer serves as a predictor of response to EGFR-TKI treatment. Cancer Biol. Ther. 2016, 17, 320–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reck, M.; Hagiwara, K.; Han, B.; Tjulandin, S.; Grohe, C.; Yokoi, T.; Morabito, A.; Novello, S.; Arriola, E.; Molinier, O.; et al. ctDNA Determination of EGFR Mutation Status in European and Japanese Patients with Advanced NSCLC: The ASSESS Study. J. Thorac. Oncol. 2016, 11, 1682–1689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reckamp, K.L.; Melnikova, V.O.; Karlovich, C.; Sequist, L.V.; Camidge, D.R.; Wakelee, H.; Perol, M.; Oxnard, G.R.; Kosco, K.; Croucher, P.; et al. A highly sensitive and quantitative test platform for detection of NSCLC EGFR mutations in urine and plasma. J. Thorac. Oncol. 2016, 11, 1690–1700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sacher, A.G.; Paweletz, C.; Dahlberg, S.E.; Alden, R.S.; O’Connell, A.; Feeney, N.; Mach, S.L.; Janne, P.A.; Oxnard, G.R. Prospective Validation of Rapid Plasma Genotyping for the Detection of EGFR and KRAS Mutations in Advanced Lung Cancer. JAMA Oncol. 2016, 2, 1014–1022. [Google Scholar] [CrossRef] [Green Version]
- Schwaederle, M.C.; Patel, S.P.; Husain, H.; Ikeda, M.; Lanman, R.B.; Banks, K.C.; Talasaz, A.; Bazhenova, L.; Kurzrock, R. Utility of Genomic Assessment of Blood-Derived Circulating Tumor DNA (ctDNA) in Patients with Advanced Lung Adenocarcinoma. Clin. Cancer Res. 2017, 23, 5101–5111. [Google Scholar] [CrossRef] [Green Version]
- Shi, C.; Zheng, Y.; Li, Y.; Sun, H.; Liu, S. Association between clinical characteristics and the diagnostic accuracy of circulating single-molecule amplification and resequencing technology on detection epidermal growth factor receptor mutation status in plasma of lung adenocarcinoma. J. Clin. Lab. Anal. 2018, 32, e22271. [Google Scholar] [CrossRef] [Green Version]
- Sim, W.C.; Loh, C.H.; Toh, G.L.X.; Lim, C.W.; Chopra, A.; Chang, A.Y.C.; Goh, L.L. Non-invasive detection of actionable mutations in advanced non-small-cell lung cancer using targeted sequencing of circulating tumor DNA. Lung Cancer 2018, 124, 154–159. [Google Scholar] [CrossRef]
- Sundaresan, T.K.; Sequist, L.V.; Heymach, J.V.; Riely, G.J.; Janne, P.A.; Koch, W.H.; Sullivan, J.P.; Fox, D.B.; Maher, R.; Muzikansky, A.; et al. Detection of T790M, the Acquired Resistance EGFR Mutation, by Tumor Biopsy versus Noninvasive Blood-Based Analyses. Clin. Cancer Res. 2016, 22, 1103–1110. [Google Scholar] [CrossRef] [Green Version]
- Sung, J.S.; Chong, H.Y.; Kwon, N.J.; Kim, H.M.; Lee, J.W.; Kim, B.; Lee, S.B.; Park, C.W.; Choi, J.Y.; Chang, W.J.; et al. Detection of somatic variants and EGFR mutations in cell-free DNA from non-small cell lung cancer patients by ultra-deep sequencing using the ion ampliseq cancer hotspot panel and droplet digital polymerase chain reaction. Oncotarget 2017, 8, 106901–106912. [Google Scholar] [CrossRef] [Green Version]
- Thompson, J.C.; Yee, S.S.; Troxel, A.B.; Savitch, S.L.; Fan, R.; Balli, D.; Lieberman, D.B.; Morrissette, J.D.; Evans, T.L.; Bauml, J.; et al. Detection of therapeutically targetable driver and resistance mutations in lung cancer patients by next-generation sequencing of cell-free circulating tumor DNA. Clin. Cancer Res. 2016, 22, 5772–5782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thress, K.S.; Brant, R.; Carr, T.H.; Dearden, S.; Jenkins, S.; Brown, H.; Hammett, T.; Cantarini, M.; Barrett, J.C. EGFR mutation detection in ctDNA from NSCLC patient plasma: A cross-platform comparison of leading technologies to support the clinical development of AZD9291. Lung Cancer 2015, 90, 509–515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uchida, J.; Kato, K.; Kukita, Y.; Kumagai, T.; Nishino, K.; Daga, H.; Nagatomo, I.; Inoue, T.; Kimura, M.; Oba, S.; et al. Diagnostic accuracy of noninvasive genotyping of EGFR in lung cancer patients by deep sequencing of plasma cell-free DNA. Clin. Chem. 2015, 61, 1191–1196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vazquez, S.; Casal, J.; Afonso Afonso, F.J.; Firvida, J.L.; Santome, L.; Baron, F.; Lazaro, M.; Pena, C.; Amenedo, M.; Abdulkader, I.; et al. EGFR testing and clinical management of advanced NSCLC: A Galician Lung Cancer Group study (GGCP 048-10). Cancer Manag. Res. 2016, 8, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Wan, R.; Wang, Z.; Lee, J.J.; Wang, S.; Li, Q.; Tang, F.; Wang, J.; Sun, Y.; Bai, H.; Wang, D.; et al. Comprehensive Analysis of the Discordance of EGFR Mutation Status between Tumor Tissues and Matched Circulating Tumor DNA in Advanced Non–Small Cell Lung Cancer. J. Thorac. Oncol. 2017, 12, 1376–1387. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Han, X.; Hu, X.; Wang, X.; Zhao, L.; Tang, L.; Feng, Y.; Wu, D.; Sun, Y.; Shi, Y. Clinical significance of pretreatment plasma biomarkers in advanced non-small cell lung cancer patients. Clin. Chim. Acta 2014, 430, 63–70. [Google Scholar] [CrossRef]
- Wang, Y.; Tian, P.W.; Wang, W.Y.; Wang, K.; Zhang, Z.; Chen, B.J.; He, Y.Q.; Li, L.; Liu, H.; Chuai, S.; et al. Noninvasive genotyping and monitoring of anaplastic lymphoma kinase (ALK) rearranged non-small cell lung cancer by capture-based next-generation sequencing. Oncotarget 2016, 7, 65208–65217. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, K.; Fukuhara, T.; Tsukita, Y.; Morita, M.; Suzuki, A.; Tanaka, N.; Terasaki, H.; Nukiwa, T.; Maemondo, M. EGFR Mutation Analysis of Circulating Tumor DNA Using an Improved PNA-LNA PCR Clamp Method. Can. Respir. J. 2016, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Wei, F.; Strom, C.M.; Cheng, J.; Lin, C.C.; Hsu, C.Y.; Soo Hoo, G.W.; Chia, D.; Kim, Y.; Li, F.; Elashoff, D.; et al. Electric Field–Induced Release and Measurement Liquid Biopsy for Noninvasive Early Lung Cancer Assessment. J. Mol. Diagn. 2018, 20, 738–742. [Google Scholar] [CrossRef] [Green Version]
- Wei, Z.; Wang, W.; Shu, Z.; Zhou, X.; Zhang, Y. Correlation between circulating tumor dna levels and response to tyrosine kinase inhibitors (TKI) treatment in non-small cell lung cancer. Med Sci. Monit. 2017, 23, 3627–3634. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.L.; Lee, V.; Liam, C.K.; Lu, S.; Park, K.; Srimuninnimit, V.; Wang, J.; Zhou, C.; Appius, A.; Button, P.; et al. Clinical utility of a blood-based EGFR mutation test in patients receiving first-line erlotinib therapy in the ENSURE, FASTACT-2, and ASPIRATION studies. Lung Cancer 2018, 126, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.L.; Tong, R.Z.; Zhang, Y.; Hu, B.B.; Zheng, K.; Ding, Z.Y.; Peng, F.; Gong, Y.L.; Liu, Y.M.; Lu, Y. Conventional real-time PCR-based detection of T790M using tumor tissue or blood in patients with EGFR TKI-resistant NSCLC. OncoTargets Ther. 2017, 10, 3307–3312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, S.; Lou, F.; Wu, Y.; Sun, D.Q.; Zhang, J.B.; Chen, W.; Ye, H.; Liu, J.H.; Wei, S.; Zhao, M.Y.; et al. Circulating tumor DNA identified by targeted sequencing in advanced-stage non-small cell lung cancer patients. Cancer Lett. 2016, 370, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Shen, X.; Li, R.; Shen, J.; Zhang, H.; Yu, L.; Liu, B.; Wang, L. The detection and significance of EGFR and BRAF in cell-free DNA of peripheral blood in NSCLC. Oncotarget 2017, 8, 49773–49782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao, Y.; Liu, J.; Li, L.; Yuan, Y.; Nan, K.; Wu, X.; Zhang, Z.; Wu, Y.; Li, X.; Zhu, J.; et al. Detection of circulating tumor DNA in patients with advanced non-small cell lung cancer. Oncotarget 2017, 8, 2130–2140. [Google Scholar] [CrossRef] [Green Version]
- Yu, H.; Liu, M.; Qiu, H.; Yang, K. Urinary and Plasma Cell-Free DNA Comparison for Lung Cancer Patients Treated With Epidermal Growth Factor Receptor-Thyroxine Kinase Inhibitors. Am. J. Med. Sci. 2019, 357, 29–36. [Google Scholar] [CrossRef]
- Yu, Q.; Huang, F.; Zhang, M.; Ji, H.; Wu, S.; Zhao, Y.; Zhang, C.; Wu, J.; Wang, B.; Pan, B.; et al. Multiplex picoliter-droplet digital PCR for quantitative assessment of EGFR mutations in circulating cell-free DNA derived from advanced non-small cell lung cancer patients. Mol. Med. Rep. 2017, 16, 1157–1166. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; He, B.; Cui, J.; Zhao, M.; Zhang, Z. Comparison of circulating DNA from plasma and urine for EGFR mutations in NSCLC patients. Cancer Biomark. 2018, 23, 427–436. [Google Scholar] [CrossRef]
- Zhang, Y.; Xu, Y.; Zhong, W.; Zhao, J.; Chen, M.; Zhang, L.; Li, L.; Wang, M. Total DNA input is a crucial determinant of the sensitivity of plasma cell-free DNA EGFR mutation detection using droplet digital PCR. Oncotarget 2017, 8, 5861–5873. [Google Scholar] [CrossRef]
- Zheng, D.; Ye, X.; Zhang, M.Z.; Sun, Y.; Wang, J.Y.; Ni, J.; Zhang, H.P.; Zhang, L.; Luo, J.; Zhang, J.; et al. Plasma EGFR T790M ctDNA status is associated with clinical outcome in advanced NSCLC patients with acquired EGFR-TKI resistance. Sci. Rep. 2016, 6. [Google Scholar] [CrossRef] [Green Version]
- Zhu, G.; Ye, X.; Dong, Z.; Lu, Y.C.; Sun, Y.; Liu, Y.; McCormack, R.; Gu, Y.; Liu, X. Highly sensitive droplet digital PCR method for detection of EGFR-activating mutations in plasma cell-free DNA from patients with advanced non-small cell lung cancer. J. Mol. Diagn. 2015, 17, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.J.; Zhang, H.B.; Liu, Y.H.; Zhang, F.L.; Zhu, Y.Z.; Li, Y.; Bai, J.P.; Liu, L.R.; Qu, Y.C.; Qu, X.; et al. Quantitative cell-free circulating EGFR mutation concentration is correlated with tumor burden in advanced NSCLC patients. Lung Cancer 2017, 109, 124–127. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.J.; Zhang, H.B.; Liu, Y.H.; Zhu, Y.Z.; Chen, J.; Li, Y.; Bai, J.P.; Liu, L.R.; Qu, Y.C.; Qu, X.; et al. Association of mutant EGFR L858R and exon 19 concentration in circulating cell-free DNA using droplet digital PCR with response to EGFR-TKIs in NSCLC. Oncol. Lett. 2017, 14, 2537–2579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.L.; Huang, W.C.; Lin, F.M.; Hsieh, H.B.; Hsieh, C.H.; Hsieh, R.K.; Chen, K.W.; Yen, M.H.; Lee, J.; Su, S.; et al. Novel circulating tumor cell-based blood test for the assessment of PD-L1 protein expression in treatment-naive, newly diagnosed patients with non-small cell lung cancer. Cancer Immunol. Immunother. CII 2019, 68, 1087–1094. [Google Scholar] [CrossRef] [Green Version]
- Ding, P.N.; Becker, T.M.; Bray, V.J.; Chua, W.; Ma, Y.F.; Lynch, D.; Po, J.; Luk, A.W.S.; Caixeiro, N.; de Souza, P.; et al. The predictive and prognostic significance of liquid biopsy in advanced epidermal growth factor receptor-mutated non-small cell lung cancer: A prospective study. Lung Cancer 2019, 134, 187–193. [Google Scholar] [CrossRef]
- Garcia, J.; Wozny, A.S.; Geiguer, F.; Delherme, A.; Barthelemy, D.; Merle, P.; Tissot, C.; Jones, F.S.; Johnson, C.; Xing, X.; et al. Profiling of circulating tumor DNA in plasma of non-small cell lung cancer patients, monitoring of epidermal growth factor receptor p.T790M mutated allelic fraction using beads, emulsion, amplification, and magnetics companion assay and evaluation in future application in mimicking circulating tumor cells. Cancer Med. 2019, 8, 3685–3697. [Google Scholar] [CrossRef]
- He, W.; Xu, D.; Wang, Z.; Wu, H.; Xiang, X.; Tang, B.; Jiang, W.; Cui, Y.; Wang, H.; Jiang, N.; et al. Three-dimensional nanostructured substrates enable dynamic detection of ALK-rearrangement in circulating tumor cells from treatment-naive patients with stage III/IV lung adenocarcinoma. J. Transl. Med. 2019, 17, 32. [Google Scholar] [CrossRef]
- Li, B.T.; Janku, F.; Jung, B.; Hou, C.; Madwani, K.; Alden, R.; Razavi, P.; Reis-Filho, J.S.; Shen, R.; Isbell, J.M.; et al. Ultra-deep next-generation sequencing of plasma cell-free DNA in patients with advanced lung cancers: Results from the actionable genome consortium. Ann. Oncol. 2019, 30, 597–603. [Google Scholar] [CrossRef]
- O’Kane, G.M.; Liu, G.; Stockley, T.L.; Shabir, M.; Zhang, T.; Law, J.H.; Le, L.W.; Sacher, A.; Shepherd, F.A.; Bradbury, P.A.; et al. The presence and variant allele fraction of EGFR mutations in ctDNA and development of resistance. Lung Cancer 2019, 131, 86–89. [Google Scholar] [CrossRef]
- Park, C.K.; Kim, J.E.; Kim, M.S.; Kho, B.G.; Park, H.Y.; Kim, T.O.; Shin, H.J.; Cho, H.J.; Choi, Y.D.; Oh, I.J.; et al. Feasibility of liquid biopsy using plasma and platelets for detection of anaplastic lymphoma kinase rearrangements in non-small cell lung cancer. J. Cancer Res. Clin. Oncol. 2019, 145, 2071–2082. [Google Scholar] [CrossRef] [Green Version]
- Soria-Comes, T.; Palomar-Abril, V.; Ureste, M.M.; Guerola, M.T.; Maiques, I.C.M. Real-World Data of the Correlation between EGFR Determination by Liquid Biopsy in Non-squamous Non-small Cell Lung Cancer (NSCLC) and the EGFR Profile in Tumor Biopsy. Pathol. Oncol. Res. 2019, 1–7. [Google Scholar] [CrossRef]
- Usui, K.; Yokoyama, T.; Naka, G.; Ishida, H.; Kishi, K.; Uemura, K.; Ohashi, Y.; Kunitoh, H. Plasma ctDNA monitoring during epidermal growth factor receptor (EGFR)-Tyrosine kinase inhibitor treatment in patients with EGFR-mutant non-small cell lung cancer (JP-CLEAR trial). Jpn. J. Clin. Oncol. 2019, 49, 554–558. [Google Scholar] [CrossRef]
- Wang, L.; Hu, X.; Guo, Q.; Huang, X.; Lin, C.H.; Chen, X.; Li, M.; Yao, Q.; Zhou, Q.; Wang, J.; et al. CLAmp-seq: A Novel Amplicon-Based NGS Assay with Concatemer Error Correction for Improved Detection of Actionable Mutations in Plasma cfDNA from Patients with NSCLC. Small Methods 2019, 4, 1900357. [Google Scholar] [CrossRef]
- Yang, K.; Li, J.; Zhao, J.; Ren, P.; Wang, Z.; Wei, B.; Dong, B.; Sun, R.; Wang, X.; Groen, H.J.M.; et al. Developing Ultrasensitive Library-Aliquot-Based Droplet Digital PCR for Detecting T790M in Plasma-Circulating Tumor DNA of Non-small-Cell-Lung-Cancer Patients. Anal. Chem. 2018, 90, 11203–11209. [Google Scholar] [CrossRef] [PubMed]
- Ye, Y.; Luo, Z.; Shi, D. Use of cell free DNA as a prognostic biomarker in non-small cell lung cancer patients with bone metastasis. Int. J. Biol. Markers 2019, 34, 381–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, M.; Li, L.; Wang, A.; Zhang, L.; Xu, J.; Liu, H. The clinical significance of detection of EGFR mutation in peripheral blood of patients with advanced non-small cell lung cancer. Acta Med. Mediterr. 2019, 35, 333–338. [Google Scholar] [CrossRef]
- Zhang, S.; Chen, Z.; Huang, C.; Ding, C.; Li, C.; Chen, J.; Zhao, J.; Miao, L. Ultrasensitive and quantitative detection of: EGFR mutations in plasma samples from patients with non-small-cell lung cancer using a dual PNA clamping-mediated LNA-PNA PCR clamp. Analyst 2019, 144, 1718–1724. [Google Scholar] [CrossRef]
- Yoshida, H.; Kim, Y.H.; Ozasa, H.; Nagai, H.; Sakamori, Y.; Tsuji, T.; Nomizo, T.; Funazo, T.; Yasuda, Y.; Hirai, T. EGFR T790M detection in circulating tumor DNA from non-small cell lung cancer patients using the PNA-LNA clamp method. Anticancer Res. 2017, 37, 2721–2725. [Google Scholar] [CrossRef]
- Arrieta, O.; Pineda, B.; Muniz-Hernandez, S.; Flores, D.; Ordonez, G.; Borbolla-Escoboza, J.R.; Orta, D. Molecular detection and prognostic value of epithelial markers mRNA expression in peripheral blood of advanced non-small cell lung cancer patients. Cancer Biomark. Sect. A Dis. Markers 2014, 14, 215–223. [Google Scholar] [CrossRef]
- Azuma, K.; Hirashima, T.; Yamamoto, N.; Okamoto, I.; Takahashi, T.; Nishio, M.; Hirata, T.; Kubota, K.; Kasahara, K.; Hida, T.; et al. Phase II study of erlotinib plus tivantinib (ARQ 197) in patients with locally advanced or metastatic EGFR mutation-positive non-small-cell lung cancer just after progression on EGFR-TKI, gefitinib or erlotinib. ESMO Open 2016, 1, e000063. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Xu, Y.; Liao, X.; Liao, R.; Zhang, L.; Niu, K.; Li, T.; Li, D.; Chen, Z.; Duan, Y.; et al. Plasma miRNAs in predicting radiosensitivity in non-small cell lung cancer. Tumor Biol. 2016, 37, 11927–11936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costantini, A.; Julie, C.; Dumenil, C.; Helias-Rodzewicz, Z.; Tisserand, J.; Dumoulin, J.; Giraud, V.; Labrune, S.; Chinet, T.; Emile, J.F.; et al. Predictive role of plasmatic biomarkers in advanced non-small cell lung cancer treated by nivolumab. Oncoimmunology 2018, 7, e1452581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Re, M.; Tiseo, M.; Bordi, P.; D’Incecco, A.; Camerini, A.; Petrini, I.; Lucchesi, M.; Inno, A.; Spada, D.; Vasile, E.; et al. Contribution of KRAS mutations and c.2369C > T (p.T790M) EGFR to acquired resistance to EGFR-TKIs in EGFR mutant NSCLC: A study on circulating tumor DNA. Oncotarget 2017, 8, 13611–13619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dowler Nygaard, A.; Spindler, K.L.; Pallisgaard, N.; Andersen, R.F.; Jakobsen, A. Levels of cell-free DNA and plasma KRAS during treatment of advanced NSCLC. Oncol. Rep. 2014, 31, 969–974. [Google Scholar] [CrossRef] [Green Version]
- Fiala, O.; Pesek, M.; Finek, J.; Benesova, L.; Minarik, M.; Bortlicek, Z.; Topolcan, O. The role of neuron-specific enolase (NSE) and thymidine kinase (TK) levels in prediction of efficacy ofEGFR-TKIs in patients with advanced-stage NSCLC [corrected]. Anticancer Res. 2014, 34, 5193–5198. [Google Scholar]
- Fiala, O.; Pesek, M.; Finek, J.; Benesova, L.; Minarik, M.; Bortlicek, Z.; Topolcan, O. Predictive role of CEA and CYFRA 21-1 in patients with advanced-stage NSCLC treated with erlotinib. Anticancer Res. 2014, 34, 3205–3210. [Google Scholar]
- Fiala, O.; Pesek, M.; Finek, J.; Topolcan, O.; Racek, J.; Minarik, M.; Benesova, L.; Bortlicek, Z.; Poprach, A.; Buchler, T. High serum level of C-reactive protein is associated with worse outcome of patients with advanced-stage NSCLC treated with erlotinib. Tumour Biol. 2015, 36, 9215–9222. [Google Scholar] [CrossRef]
- Haghgoo, S.M.; Khosravi, A.; Mortaz, E.; Pourabdollah-Toutkaboni, M.; Seifi, S.; Sabour, S.; Allameh, A. Prognostic value of rare and complex mutations in EGFR and serum levels of soluble EGFR and its ligands in non-small cell lung carcinoma patients. Clin. Biochem. 2017, 50, 293–300. [Google Scholar] [CrossRef]
- Jiang, T.; Li, X.; Wang, J.; Su, C.; Han, W.; Zhao, C.; Wu, F.; Gao, G.; Li, W.; Chen, X.; et al. Mutational Landscape of cfDNA Identifies Distinct Molecular Features Associated With Therapeutic Response to First-Line Platinum-Based Doublet Chemotherapy in Patients with Advanced NSCLC. Theranostics 2017, 7, 4753–4762. [Google Scholar] [CrossRef]
- Jiang, T.; Zhao, J.; Zhao, C.; Li, X.; Shen, J.; Zhou, J.; Ren, S.; Su, C.; Zhou, C.; O’Brien, M. Dynamic Monitoring and Predictive Value of Circulating Tumor Cells in EGFR-Mutated Advanced Non-Small-Cell Lung Cancer Patients Treated With First-Line EGFR Tyrosine Kinase Inhibitors. Clin. Lung Cancer 2018, 20, 124–133. [Google Scholar] [CrossRef]
- Juan, O.; Vidal, J.; Gisbert, R.; Munoz, J.; Macia, S.; Gomez-Codina, J. Prognostic significance of circulating tumor cells in advanced non-small cell lung cancer patients treated with docetaxel and gemcitabine. Clin. Transl. Oncol. 2014, 16, 637–643. [Google Scholar] [CrossRef] [PubMed]
- Karachaliou, N.; Mayo-de las Casas, C.; Queralt, C.; De Aguirre, I.; Melloni, B.; Cardenal, F.; Garcia-Gomez, R.; Massuti, B.; Sanchez, J.M.; Porta, R.; et al. Association of EGFR L858R Mutation in Circulating Free DNA With Survival in the EURTAC Trial. JAMA Oncol. 2015, 1, 149–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.H.; Lin, Y.L.; Hsu, W.H.; Chen, H.Y.; Chang, Y.C.; Yu, C.J.; Shih, J.Y.; Lin, C.C.; Chen, K.Y.; Ho, C.C.; et al. Bcl-2-like protein 11 deletion polymorphism predicts survival in advanced non-small-cell lung cancer. J. Thorac. Oncol. 2014, 9, 1385–1392. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Wang, L.R.; Chen, J.; Lou, Y.; Zhang, G.B. First-line gemcitabine plus cisplatin in nonsmall cell lung cancer patients. Dis. Markers 2014, 2014, 960458. [Google Scholar] [CrossRef] [PubMed]
- Mai, T.; Takano, A.; Suzuki, H.; Hirose, T.; Mori, T.; Teramoto, K.; Kiyotani, K.; Nakamura, Y.; Daigo, Y. Quantitative analysis and clonal characterization of T-cell receptor β repertoires in patients with advanced non-small cell lung cancer treated with cancer vaccine. Oncol. Lett. 2017, 14, 283–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muinelo-Romay, L.; Vieito, M.; Abalo, A.; Nocelo, M.A.; Baron, F.; Anido, U.; Brozos, E.; Vazquez, F.; Aguin, S.; Abal, M.; et al. Evaluation of Circulating Tumor Cells and Related Events as Prognostic Factors and Surrogate Biomarkers in Advanced NSCLC Patients Receiving First-Line Systemic Treatment. Cancers (Basel) 2014, 6, 153–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nel, I.; Jehn, U.; Gauler, T.; Hoffmann, A.C. Individual profiling of circulating tumor cell composition in patients with non-small cell lung cancer receiving platinum based treatment. Transl. Lung Cancer Res. 2014, 3, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Nygaard, A.D.; Holdgaard, P.C.; Spindler, K.L.; Pallisgaard, N.; Jakobsen, A. The correlation between cell-free DNA and tumour burden was estimated by PET/CT in patients with advanced NSCLC. Br. J. Cancer 2014, 110, 363–368. [Google Scholar] [CrossRef] [Green Version]
- Ostheimer, C.; Gunther, S.; Bache, M.; Vordermark, D.; Multhoff, G. Dynamics of heat shock protein 70 serum levels as a predictor of clinical response in non-small-cell lung cancer and correlation with the hypoxia-related marker osteopontin. Front. Immunol. 2017, 8, 1305. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Hirsh, V.; Zhang, L.; de Marinis, F.; Yang, J.C.; Wakelee, H.A.; Seto, T.; Wu, Y.L.; Novello, S.; Juhasz, E.; et al. Monotherapy Administration of Sorafenib in Patients With Non-Small Cell Lung Cancer (MISSION) Trial: A Phase III, Multicenter, Placebo-Controlled Trial of Sorafenib in Patients with Relapsed or Refractory Predominantly Nonsquamous Non-Small-Cell Lung Cancer after 2 or 3 Previous Treatment Regimens. J. Thorac. Oncol. 2015, 10, 1745–1753. [Google Scholar] [CrossRef] [Green Version]
- Qi, Y.; Wang, W. Clinical significance of circulating tumor cells in squamous cell lung cancer patients. Cancer Biomark. 2017, 18, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Quoix, E.; Lena, H.; Losonczy, G.; Forget, F.; Chouaid, C.; Papai, Z.; Gervais, R.; Ottensmeier, C.; Szczesna, A.; Kazarnowicz, A.; et al. TG4010 immunotherapy and first-line chemotherapy for advanced non-small-cell lung cancer (TIME): Results from the phase 2b part of a randomised, double-blind, placebo-controlled, phase 2b/3 trial. Lancet Oncol. 2016, 17, 212–223. [Google Scholar] [CrossRef]
- Shi, W.L.; Li, J.; Bao, Q.L.; Wu, J.N.; Ge, L.P.; Zhu, L.R.; Wang, Y.; Zhu, W.F. Survivin mRNA expression in blood as a predictor of the response to EGFR-tyrosine kinase inhibitors and prognosis in patients with non-small cell lung cancer. Med. Oncol. 2014, 31, 893. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.; Yu, H.; Wang, H.; Zhao, X.; Zhao, X.; Wu, X.; Qiao, J.; Chang, J.; Wang, J. Exploratory cohort study and meta-analysis of BIM deletion polymorphism in patients with epidermal growth factor receptor-mutant nonsmall-cell lung cancer treated with epidermal growth factor receptor tyrosine kinase inhibitors. OncoTargets Ther. 2017, 10, 1955–1967. [Google Scholar] [CrossRef] [Green Version]
- Svaton, M.; Fiala, O.; Pesek, M.; Bruha, F.; Mukensnabl, P.; Racek, J.; Minarik, M.; Bortlicek, Z. Predictive and prognostic significance of sodium levels in patients with NSCLC treated by erlotinib. Anticancer Res. 2014, 34, 7461–7465. [Google Scholar]
- Tissot, C.; Toffart, A.C.; Villar, S.; Souquet, P.J.; Merle, P.; Moro-Sibilot, D.; Pérol, M.; Zavadil, J.; Brambilla, C.; Olivier, M.; et al. Circulating free DNA concentration is an independent prognostic biomarker in lung cancer. Eur. Respir. J. 2015, 46, 1773–1780. [Google Scholar] [CrossRef]
- Tu, C.; Zhu, Y.; Jiang, B.; He, W.; Jin, C. Correlation between circulating tumor cells EGFR expression and t cell subsets in advanced non-small cell lung cancer patients after tyrosine kinase inhibitor treatment. Neoplasma 2017, 64, 619–625. [Google Scholar] [CrossRef] [Green Version]
- Uchibori, K.; Satouchi, M.; Sueoka-Aragane, N.; Urata, Y.; Sato, A.; Imamura, F.; Inoue, T.; Tachihara, M.; Kobayashi, K.; Katakami, N.; et al. Phase II trial of gefitinib plus pemetrexed after relapse using first-line gefitinib in patients with non-small cell lung cancer harboring EGFR gene mutations. Lung Cancer 2018, 124, 65–70. [Google Scholar] [CrossRef]
- Wang, W.; Song, Z.; Zhang, Y. A Comparison of ddPCR and ARMS for detecting EGFR T790M status in ctDNA from advanced NSCLC patients with acquired EGFR-TKI resistance. Cancer Med. 2017, 6, 154–162. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Wei, Y.; Ma, X.; Ma, X.; Gong, P. Association between advanced NSCLC T790 M EGFR-TKI secondary resistance and prognosis: A observational study. Medicine 2018, 97, e11346. [Google Scholar] [CrossRef]
- Wang, Z.; Chen, R.; Wang, S.; Zhong, J.; Wu, M.; Zhao, J.; Duan, J.; Zhuo, M.; An, T.; Wang, Y.; et al. Quantification and dynamic monitoring of EGFR T790M in plasma cell-free DNA by digital PCR for prognosis of EGFR-TKI treatment in advanced NSCLC. PLoS ONE 2014, 9, e110780. [Google Scholar] [CrossRef]
- Winther-Larsen, A.; Demuth, C.; Fledelius, J.; Madsen, A.T.; Hjorthaug, K.; Meldgaard, P.; Sorensen, B.S. Correlation between circulating mutant DNA and metabolic tumour burden in advanced non-small cell lung cancer patients. Br. J. Cancer 2017, 117, 704–709. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.L.; Sequist, L.V.; Hu, C.P.; Feng, J.; Lu, S.; Huang, Y.; Li, W.; Hou, M.; Schuler, M.; Mok, T.; et al. EGFR mutation detection in circulating cell-free DNA of lung adenocarcinoma patients: Analysis of LUX-Lung 3 and 6. Br. J. Cancer 2017, 116, 175–185. [Google Scholar] [CrossRef] [Green Version]
- Yanagita, M.; Redig, A.J.; Paweletz, C.P.; Dahlberg, S.E.; O’Connell, A.; Feeney, N.; Taibi, M.; Boucher, D.; Oxnard, G.R.; Johnson, B.E.; et al. A Prospective Evaluation of Circulating Tumor Cells and Cell-Free DNA in EGFR-Mutant Non-Small Cell Lung Cancer Patients Treated with Erlotinib on a Phase II Trial. Clin. Cancer Res. 2016, 22, 6010–6020. [Google Scholar] [CrossRef] [Green Version]
- Yang, B.; Qin, A.; Zhang, K.; Ren, H.; Liu, S.; Liu, X.; Pan, X.; Yu, G. Circulating tumor cells predict prognosis following tyrosine kinase inhibitor treatment in EGFR-mutant non-small cell lung cancer patients. Oncol. Res. 2017, 25, 1601–1606. [Google Scholar] [CrossRef]
- Yang, B.; Zheng, D.; Zeng, U.; Qin, A.; Gao, J.; Yu, G. Circulating tumor cells predict prognosis following secondline AZD 9291 treatment in EGFR-T790M mutant non-small cell lung cancer patients. J. BUON. 2018, 23, 1077–1081. [Google Scholar]
- Yonesaka, K.; Hirotani, K.; von Pawel, J.; Dediu, M.; Chen, S.; Copigneaux, C.; Nakagawa, K. Circulating heregulin level is associated with the efficacy of patritumab combined with erlotinib in patients with non-small cell lung cancer. Lung Cancer 2017, 105, 1–6. [Google Scholar] [CrossRef]
- Zhang, Q.L.; Xing, X.Z.; Li, F.Y.; Xing, Y.J.; Li, J. Pretreatment Pokemon Level as a Predictor of Response to Cisplatin and Paclitaxel in Patients with Unresectable Non-Small Cell Lung Cancer. Oncol. Res. Treat. 2015, 38, 496–502. [Google Scholar] [CrossRef] [Green Version]
- Zhang, S.; He, L.; Dai, N.; Guan, W.; Shan, J.; Yang, X.; Zhong, Z.; Qing, Y.; Jin, F.; Chen, C.; et al. Serum APE1 as a predictive marker for platinum-based chemotherapy of non-small cell lung cancer patients. Oncotarget 2016, 7, 77482–77494. [Google Scholar] [CrossRef] [Green Version]
- Zhou, J.; Dong, F.; Cui, F.; Xu, R.; Tang, X. The role of circulating tumor cells in evaluation of prognosis and treatment response in advanced non-small-cell lung cancer. Cancer Chemother. Pharmacol. 2017, 79, 825–833. [Google Scholar] [CrossRef]
- Zhu, Y.J.; Zhang, H.B.; Liu, Y.H.; Zhang, F.L.; Zhu, Y.Z.; Li, Y.; Bai, J.P.; Liu, L.R.; Qu, Y.C.; Qu, X.; et al. Estimation of cell-free circulating EGFR mutation concentration predicts outcomes in NSCLC patients treated with EGFR-TKIs. Oncotarget 2017, 8, 13195–13205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akamatsu, H.; Koh, Y.; Okamoto, I.; Fujimoto, D.; Bessho, A.; Azuma, K.; Morita, S.; Yamamoto, N.; Nakagawa, K. Clinical significance of monitoring EGFR mutation in plasma using multiplexed digital PCR in EGFR mutated patients treated with afatinib (West Japan Oncology Group 8114LTR study). Lung Cancer 2019, 131, 128–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alama, A.; Coco, S.; Genova, C.; Rossi, G.; Fontana, V.; Tagliamento, M.; Giovanna Dal Bello, M.; Rosa, A.; Boccardo, S.; Rijavec, E.; et al. Prognostic Relevance of Circulating Tumor Cells and Circulating Cell-Free DNA Association in Metastatic Non-Small Cell Lung Cancer Treated with Nivolumab. J. Clin. Med. 2019, 8, 1011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bordi, P.; Del Re, M.; Minari, R.; Rofi, E.; Buti, S.; Restante, G.; Squadrilli, A.; Crucitta, S.; Casartelli, C.; Gnetti, L.; et al. From the beginning to resistance: Study of plasma monitoring and resistance mechanisms in a cohort of patients treated with osimertinib for advanced T790M-positive NSCLC. Lung Cancer 2019, 131, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Hojbjerg, J.A.; Ebert, E.B.F.; Clement, M.S.; Winther-Larsen, A.; Meldgaard, P.; Sorensen, B. Circulating miR-30b and miR-30c predict erlotinib response in EGFR-mutated non-small cell lung cancer patients. Lung Cancer 2019, 135, 92–96. [Google Scholar] [CrossRef] [Green Version]
- Kotsakis, A.; Kallergi, G.; Aggouraki, D.; Lyristi, Z.; Koinis, F.; Lagoudaki, E.; Koutsopoulos, A.; Georgoulias, V.; Vetsika, E.K. CD8(+) PD-1(+) T-cells and PD-L1(+) circulating tumor cells in chemotherapy-naive non-small cell lung cancer: Towards their clinical relevance? Ther. Adv. Med. Oncol. 2019, 11, 1758835919853193. [Google Scholar] [CrossRef]
- Navarro, A.; Molins, L.; Marrades, R.M.; Moises, J.; Vinolas, N.; Morales, S.; Canals, J.; Castellano, J.J.; Ramirez, J.; Monzo, M. Exosome Analysis in Tumor-Draining Pulmonary Vein Identifies NSCLC Patients with Higher Risk of Relapse after Curative Surgery. Cancers (Basel) 2019, 11, 249. [Google Scholar] [CrossRef] [Green Version]
- Passiglia, F.; Galvano, A.; Castiglia, M.; Incorvaia, L.; Calo, V.; Listi, A.; Mazzarisi, S.; Perez, A.; Gallina, G.; Rizzo, S.; et al. Monitoring blood biomarkers to predict nivolumab effectiveness in NSCLC patients. Ther. Adv. Med. Oncol. 2019, 11, 1758835919839928. [Google Scholar] [CrossRef] [Green Version]
- Tamminga, M.; De Wit, S.; Hiltermann, T.J.N.; Timens, W.; Schuuring, E.; Terstappen, L.; Groen, H.J.M. Circulating tumor cells in advanced non-small cell lung cancer patients are associated with worse tumor response to checkpoint inhibitors. J. Immunother. Cancer 2019, 7, 173. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Duan, J.; Cai, S.; Han, M.; Dong, H.; Zhao, J.; Zhu, B.; Wang, S.; Zhuo, M.; Sun, J.; et al. Assessment of Blood Tumor Mutational Burden as a Potential Biomarker for Immunotherapy in Patients with Non-Small Cell Lung Cancer with Use of a Next-Generation Sequencing Cancer Gene Panel. JAMA Oncol. 2019, 5, 696–702. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Feng, Y.C.; Zhu, H.G.; Xiong, T.C.; Hou, Y.S.; Song, J.; Jiang, W.; Zhu, C.J. The peripheral blood neutrophil-to-lymphocyte ratio is a prognostic predictor for survival of EGFR-mutant nonsmall cell lung cancer patients treated with EGFR-TKIs. Medicine (United States) 2018, 97, 30. [Google Scholar] [CrossRef]
- Yang, Y.L.; Wang, W.; Xu, L.P. Predictive value of microRNA-10b expression in peripheral blood mononuclear cells in evaluating short-and long-term efficacy of chemotherapy for patients with advanced non-small-cell lung cancer. Neoplasma 2018, 65, 610–619. [Google Scholar] [CrossRef] [Green Version]
- Chae, Y.K.; Davis, A.A.; Agte, S.; Pan, A.; Simon, N.I.; Iams, W.T.; Cruz, M.R.; Tamragouri, K.; Rhee, K.; Mohindra, N.; et al. Clinical Implications of Circulating Tumor DNA Tumor Mutational Burden (ctDNA TMB) in Non-Small Cell Lung Cancer. Oncologist 2019, 24, 820–828. [Google Scholar] [CrossRef] [Green Version]
- Rao, S.; Beckman, R.A.; Riazi, S.; Yabar, C.S.; Boca, S.M.; Marshall, J.L.; Pishvaian, M.J.; Brody, J.R.; Madhavan, S. Quantification and expert evaluation of evidence for chemopredictive biomarkers to personalize cancer treatment. Oncotarget 2017, 8, 37923–37934. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Zhou, C. Comparison of cross-platform technologies for EGFR T790M testing in patients with non-small cell lung cancer. Oncotarget 2017, 8, 100801. [Google Scholar] [CrossRef] [Green Version]
- Kim, E.; Feldman, R.; Wistuba, I.I. Update on EGFR Mutational Testing and the Potential of Noninvasive Liquid Biopsy in Non–Small-cell Lung Cancer. Clin. Lung Cancer 2018, 19, 105–114. [Google Scholar] [CrossRef]
- Rolfo, C.; Mack, P.C.; Scagliotti, G.V.; Baas, P.; Barlesi, F.; Bivona, T.G.; Herbst, R.S.; Mok, T.S.; Peled, N.; Pirker, R.; et al. Liquid Biopsy for Advanced Non-Small Cell Lung Cancer (NSCLC): A Statement Paper from the IASLC. J. Thorac. Oncol. 2018, 13, 1248–1268. [Google Scholar] [CrossRef] [Green Version]
- Network, N.C.C. Non-Small Cell Lung Cancer (Version 3.2020). Available online: Nccn.org (accessed on 17 April 2020).
- Midha, A.; Dearden, S.; McCormack, R. EGFR mutation incidence in non-small-cell lung cancer of adenocarcinoma histology: A systematic review and global map by ethnicity (mutMapII). Am. J. Cancer Res. 2015, 5, 2892–2911. [Google Scholar]
- Zhang, Y.-L.; Yuan, J.-Q.; Wang, K.-F.; Fu, X.-H.; Han, X.-R.; Threapleton, D.; Yang, Z.-Y.; Mao, C.; Tang, J.-L. The prevalence of EGFR mutation in patients with non-small cell lung cancer: A systematic review and meta-analysis. Oncotarget 2016, 7, 78985–78993. [Google Scholar] [CrossRef] [Green Version]
- Yuan, M.; Huang, L.-L.; Chen, J.-H.; Wu, J.; Xu, Q. The emerging treatment landscape of targeted therapy in non-small-cell lung cancer. Signal Transduct. Target. Ther. 2019, 4, 61. [Google Scholar] [CrossRef] [Green Version]
- Bernabé, R.; Hickson, N.; Wallace, A.; Blackhall, F.H. What do we need to make circulating tumour DNA (ctDNA) a routine diagnostic test in lung cancer? Eur. J. Cancer 2017, 81, 66–73. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1st Author | Publication Year | Evaluated Biomarker(s) | Analysis Method | Reference Number |
|---|---|---|---|---|
| Alegre et al. | 2016 | L858R, del E746-A750 | PCR | [14] |
| Arriola et al. | 2018 | EGFR | PCR | [15] |
| Balgkouranidou et al. | 2014 | BRMS1 | PCR | [16] |
| Chai et al. | 2016 | Exon 19 deletion, L858R, L861Q, T790M, exon 20 insertions | cSMART | [17] |
| Chen et al. | 2017 | Gene panel | NGS | [18] |
| Chen et al. | 2016 | Gene panel | NGS | [19] |
| Cui et al. | 2017 | ALK | NGS | [20] |
| Douillard et al. | 2014 | EGFR | PCR | [21] |
| Duan et al. | 2015 | EGFR | PCR | [22] |
| Guibert et al. | 2018 | PD-L1 | Fluorescence | [23] |
| Guibert et al. | 2018 | EGFR, T790M | NGS & PCR | [24] |
| Guibert et al. | 2016 | KRAS | NGS & PCR | [25] |
| Guo et al. | 2016 | Gene panel | NGS | [26] |
| Han et al. | 2016 | EGFR, KRAS | PCR | [27] |
| He et al. | 2017 | L858R, exon 19 deletion, EGFR | PCR | [28] |
| Ilie et al. | 2018 | PD-L1 | Fluorescence | [29] |
| Ilie et al. | 2017 | MET | Fluorescence | [30] |
| Jenkins et al. | 2017 | T790M, L858R, exon 19 deletion | PCR | [31] |
| Kasahara et al. | 2017 | Exon 19 deletion, L858R | PCR | [32] |
| Krug et al. | 2018 | EGFR, T790M | NGS & PCR | [33] |
| Lam et al. | 2015 | EGFR | PCR | [34] |
| Lee et al. | 2016 | Exon 19 deletion, L858R | PCR | [35] |
| Li et al. | 2017 | Exon 19 deletion, L858R, gene panel | PCR | [36] |
| Li et al. | 2014 | EGFR | PCR | [37] |
| Liu et al. | 2018 | Gene panel, L858R, exon 19 deletion, KRAS, ALK | NGS | [38] |
| Ma | 2016 | EGFR, exon 19 deletion, L858R | PCR | [39] |
| Mayo-de-las-Casas et al. | 2017 | EGFR | PCR | [40] |
| Mok et al. | 2015 | EGFR, exon 19 deletion, L858R, G719X, L861Q | PCR | [41] |
| Muller et al. | 2017 | Gene panel | NGS | [42] |
| Nilsson et al. | 2016 | ALK | PCR | [43] |
| Oxnard et al. | 2016 | Exon 19 deletion, L858R, T790M | PCR | [44] |
| Que et al. | 2016 | EGFR | Chromatograpy | [45] |
| Reck et al. | 2016 | EGFR | PCR | [46] |
| Reckamp et al. | 2016 | T790M, L858R, exon 19 deletion | NGS | [47] |
| Sacher et al. | 2016 | Exon 19 deletion, L858R, T790M, KRAS | PCR | [48] |
| Schwaederle et al. | 2017 | Gene panel, EGFR | NGS | [49] |
| Shi et al. | 2018 | EGFR, exon 19 deletion, L858R | cSMART | [50] |
| Sim et al. | 2018 | EGFR | PCR | [51] |
| Sundaresan | 2016 | T790M | PCR | [52] |
| Sung et al. | 2017 | Exon 19 deletion, L858R | NGS | [53] |
| Tompson et al. | 2016 | Gene panel, EGFR | NGS | [54] |
| Thress et al. | 2015 | Exon 19 deletion, L858R, T790M | PCR | [55] |
| Uchida et al. | 2015 | L858R, EGFR, gene panel | NGS | [56] |
| Vazquez et al. | 2016 | EGFR | NGS | [57] |
| Wan et al. | 2017 | EGFR | PCR | [58] |
| Wang et al. | 2014 | EGFR | PCR | [59] |
| Wang et al. | 2016 | ALK | NGS | [60] |
| Watanabe et al. | 2016 | EGFR, exon 19 deletion | PCR | [61] |
| Wei et al. | 2018 | Gene panel, L858R, exon 19 deletion | EFIRM | [62] |
| Wei et al. | 2017 | Gene panel, L858R, exon 19 deletion | PCR | [63] |
| Wu et al. | 2018 | EGFR | PCR | [64] |
| Wu et al. | 2017 | Exon 19 deletion, L858R | PCR | [65] |
| Xu et al. | 2016 | Gene panel | NGS | [66] |
| Yang et al. | 2017 | BRAF, EGFR, exon 19 deletion, L858R, T790M | PCR | [67] |
| Yao et al. | 2017 | Gene panel | NGS | [68] |
| Yu et al. | 2019 | EGFR | PCR | [69] |
| Yu et al. | 2017 | Exon 19 deletion, L858R, T790M | PCR | [70] |
| Zhang et al. | 2018 | EGFR, L858R, exon 19 deletion | PCR | [71] |
| Zhang et al. | 2017 | L858R, exon 19 deletion | PCR | [72] |
| Zheng et al. | 2016 | T790M | PCR | [73] |
| Zhu et al. | 2015 | Exon 19 deletion, L858R | PCR | [74] |
| Zhu et al. | 2017 | Exon 19 deletion, L858R | PCR | [75] |
| Zhu et al. | 2017 | Exon 19 deletion, L858R | PCR | [76] |
| Chen et al. | 2019 | PD-L1 | Fluorescence | [77] |
| Ding et al. | 2019 | Exon 19 deletion, L858R, S768I, L861Q | PCR | [78] |
| Garcia et al. | 2019 | EGFR | NGS | [79] |
| He et al. | 2019 | ALK | Fluorescence | [80] |
| Li et al. | 2019 | ALK, KRAS, EGFR, MET, ERBB2, BRAF, ROS1, RET, T790M | NGS | [81] |
| O’kane et al. | 2019 | T790M | NGS | [82] |
| Park et al. | 2019 | ALK | PCR | [83] |
| Soria-Comes et al. | 2019 | EGFR | PCR | [84] |
| Usui et al. | 2019 | T790M | NGS | [85] |
| Wang et al. | 2019 | EGFR | NGS | [86] |
| Yang et al. | 2018 | T790M | PCR | [87] |
| Ye et al. | 2019 | KRAS | PCR | [88] |
| Zhang et al. | 2019 | EGFR | NGS | [89] |
| Zhang et al. | 2019 | Exon 19 deletion, L858R | PCR | [90] |
| Yoshida et al. | 2017 | Exon 19 deletion, L858R, T790M | PCR | [91] |
| 1st Author | Publication Year | Evaluated Biomarker(s) | Treatment | Reference Number |
|---|---|---|---|---|
| Arrieta et al. | 2014 | Ck18, Ck19, CEA | Chemotherapy | [92] |
| Azuma et al. | 2016 | c-MET | Erlotinib, Tivantinib | [93] |
| Chen et al. | 2016 | has-miR-98-5p, has-miR-302e, has-miR-495-3p, has-miR-613 | Radiotherapy | [94] |
| Costantini et al. | 2018 | sGranB | Nivolumab | [95] |
| Del Re et al. | 2017 | KRAS | Erlotinib, Gefitinib | [96] |
| Dowler Nygaard et al. | 2014 | cfDNA level, KRAS | Chemotherapy, bevacizumab | [97] |
| Fiala et al. | 2014 | NSE, TK | Erlotinib, Gefitinib | [98] |
| Fiala et al. | 2014 | CYFRA, CEA | Erlotinib | [99] |
| Fiala et al. | 2015 | CRP | Erlotinib | [100] |
| Haghgoo et al. | 2017 | TGF-aplha, soluble EGFR, amphiregulin | EGFR TKI | [101] |
| He et al. | 2017 | L858R, exon 19 deletion, T790M | Afatinib | [28] |
| Jiang et al. | 2017 | MMB | Chemotherapy | [102] |
| Jiang et al. | 2018 | CTC count | Afatinib, Erlotinib, Gefitinib, Icotinib | [103] |
| Juan et al. | 2014 | CTC count | Chemotherapy | [104] |
| Karachaliou et al. | 2015 | Exon 19 deletion, L858R | Erlotinib, chemotherapy | [105] |
| Lee et al. | 2014 | BIM | Chemotherapy | [106] |
| Li et al. | 2014 | EGFR | EGFR TKI | [37] |
| Li et al. | 2014 | RRM1, ERCC1, BRCA1 | Chemotherapy | [107] |
| Ma et al. | 2016 | EGFR | EGFR TKI | [39] |
| Mai et al. | 2017 | CD8/CD4 | Montanide ISA 51 | [108] |
| Mok et al. | 2015 | EGFR | Chemotherapy, Erlotinib | [41] |
| Muinelo-Romay et al. | 2014 | CTC count | Chemotherapy | [109] |
| Nel et al. | 2014 | CD133/pan-CK, N-cadherin | Chemotherapy | [110] |
| Nilsson et al. | 2016 | ALK | Crizotinib | [43] |
| Nygaard et al. | 2014 | cfDNA level | Chemotherapy | [111] |
| Ostheimer et al. | 2017 | OPN plasma level | Radiotherapy, Chemotherapy | [112] |
| Oxnard et al. | 2016 | T790M | Osimertinib | [44] |
| Paz-Ares et al. | 2015 | EGFR | Sorafenib | [113] |
| Qi et al. | 2017 | CTC count | Chemotherapy | [114] |
| Que et al. | 2016 | EGFR | EGFR TKI | [45] |
| Quoix et al. | 2016 | TrPAL | TG4010+chemotherapy, chemotherapy | [115] |
| Shi et al. | 2014 | survivin mRNA, EGFR | Gefitinib, Erlotinib | [116] |
| Sun et al. | 2017 | BIM | Gefitinib, Erlotinib | [117] |
| Svaton et al. | 2014 | Natrium level | Erlotinib | [118] |
| Tissot et al. | 2015 | cfDNA level | Chemotherapy | [119] |
| Tu et al. | 2017 | CD4/CD8, NK expression | EGFR TKI | [120] |
| Uchibori et al. | 2018 | Exon 19 deletion, L858R, T790M | Gefitinib+ chemotherapy | [121] |
| Wang et al. | 2017 | T790M | EGFR TKI, chemotherapy | [122] |
| Wang et al. | 2018 | T790M | EGFR TKI | [123] |
| Wang et al. | 2014 | T790M | Gefitinib, erlotinib | [124] |
| Winther-Larsen et al. | 2017 | cfDNA mutation | Erlotinib | [125] |
| Wu et al. | 2017 | EGFR | Chemotherapy, Afatinib | [126] |
| Yanagita et al. | 2016 | CTC count, cfDNA level | Erlotinib | [127] |
| Yang et al. | 2017 | CTC count | Gefitinib, Erlotinib | [128] |
| Yang et al. | 2018 | CTC count | AZD9291 | [129] |
| Yonesaka et al. | 2017 | Soluble HRG | Patritumab + Erlotinib | [130] |
| Zhang et al. | 2015 | Pokemon | Chemotherapy | [131] |
| Zhang et al. | 2016 | sAPE1 | Chemotherapy | [132] |
| Zhou et al. | 2017 | CTC count | Chemotherapy | [133] |
| Zhu et al. | 2017 | EGFR, L858R, exon 19 deletion | EGFR TKI | [134] |
| Akamatsu et al. | 2019 | EGFR | Afatinib | [135] |
| Alama et al. | 2019 | CTC count, cfDNA level | Nivolumab | [136] |
| Bordi et al. | 2019 | Mutation level, EGFR | Osimertinib | [137] |
| Hojbjerg et al. | 2019 | miR-30b, miR-30c- miR-211, miR-222 | Erlotinib | [138] |
| Kotsakis et al. | 2019 | CD4, T-cells, PD-1, PD-L1, B-cells, DC/monocytes | Chemotherapy | [139] |
| Navarro et al. | 2019 | Exosome seize | Surgery | [140] |
| O’Kane et al. | 2019 | EGFR, T790M | EGFR TKI | [82] |
| Park et al. | 2019 | ALK | Crizotinib | [83] |
| Passiglia et al. | 2019 | cfDNA level, neutrophil to lymphocyte ratio | Nivolumab | [141] |
| Tamminga et al. | 2019 | CTC count | Checkpoint inhibitors | [142] |
| Wang et al. | 2019 | TMB | Anti PD-(L)1 | [143] |
| Zhang et al. | 2018 | Lymphocyte to monocyte ratio, neutrophil to lymphocyte ratio | EGFR TKI | [144] |
| Yang et al. | 2018 | MiR-10b | Chemotherapy | [145] |
| Chea et al. | 2019 | TMB, MAF | Checkpoint inhibitors | [146] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Delft, F.; Koffijberg, H.; Retèl, V.; Heuvel, M.v.d.; IJzerman, M. The Validity and Predictive Value of Blood-Based Biomarkers in Prediction of Response in the Treatment of Metastatic Non-Small Cell Lung Cancer: A Systematic Review. Cancers 2020, 12, 1120. https://doi.org/10.3390/cancers12051120
van Delft F, Koffijberg H, Retèl V, Heuvel Mvd, IJzerman M. The Validity and Predictive Value of Blood-Based Biomarkers in Prediction of Response in the Treatment of Metastatic Non-Small Cell Lung Cancer: A Systematic Review. Cancers. 2020; 12(5):1120. https://doi.org/10.3390/cancers12051120
Chicago/Turabian Stylevan Delft, Frederik, Hendrik Koffijberg, Valesca Retèl, Michel van den Heuvel, and Maarten IJzerman. 2020. "The Validity and Predictive Value of Blood-Based Biomarkers in Prediction of Response in the Treatment of Metastatic Non-Small Cell Lung Cancer: A Systematic Review" Cancers 12, no. 5: 1120. https://doi.org/10.3390/cancers12051120