Monitoring DNA Damage and Repair in Peripheral Blood Mononuclear Cells of Lung Cancer Radiotherapy Patients


 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
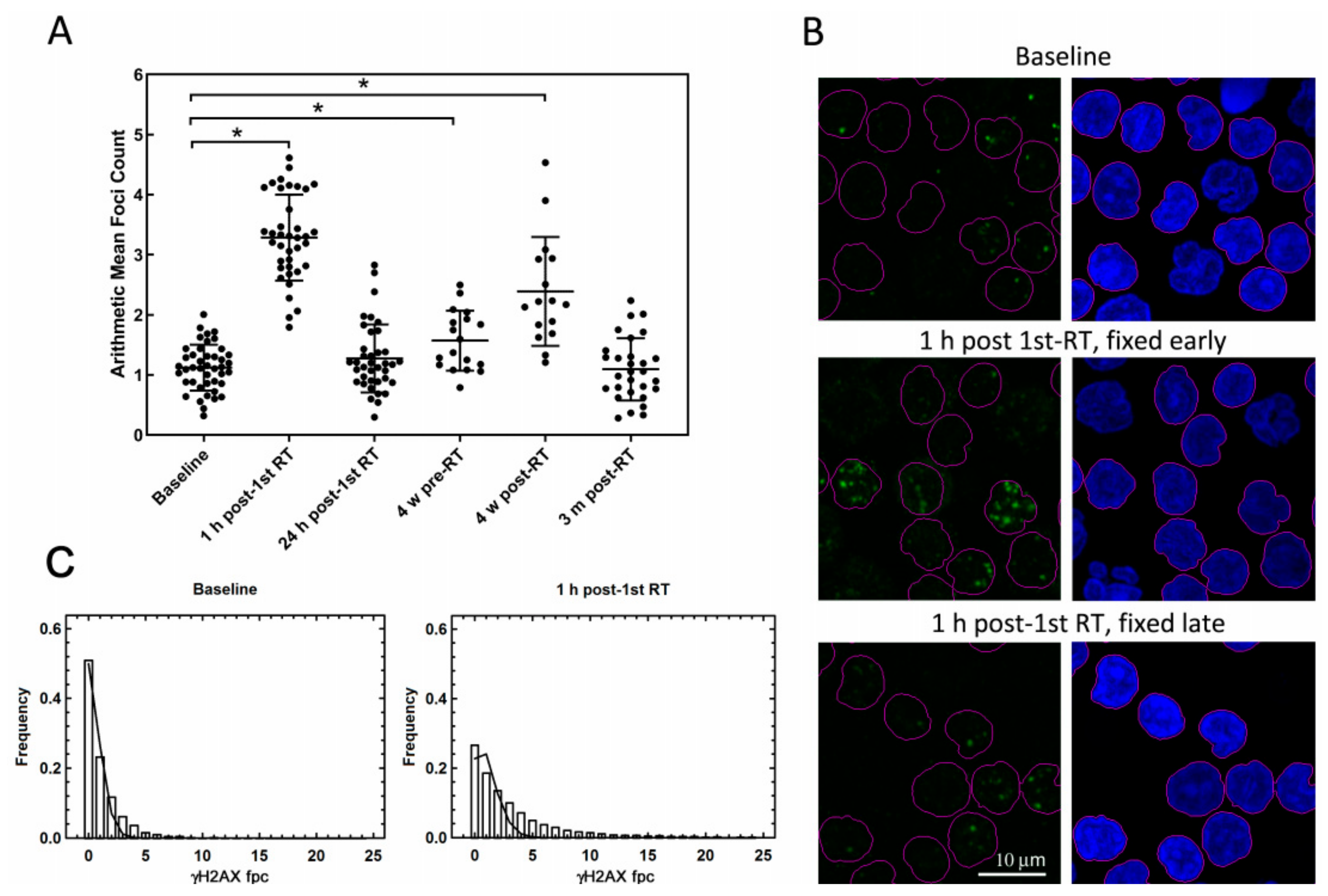
2.1. In Vivo Study: γ-H2AX Foci in PBMC that Were Not Exposed to Ex Vivo Irradiation
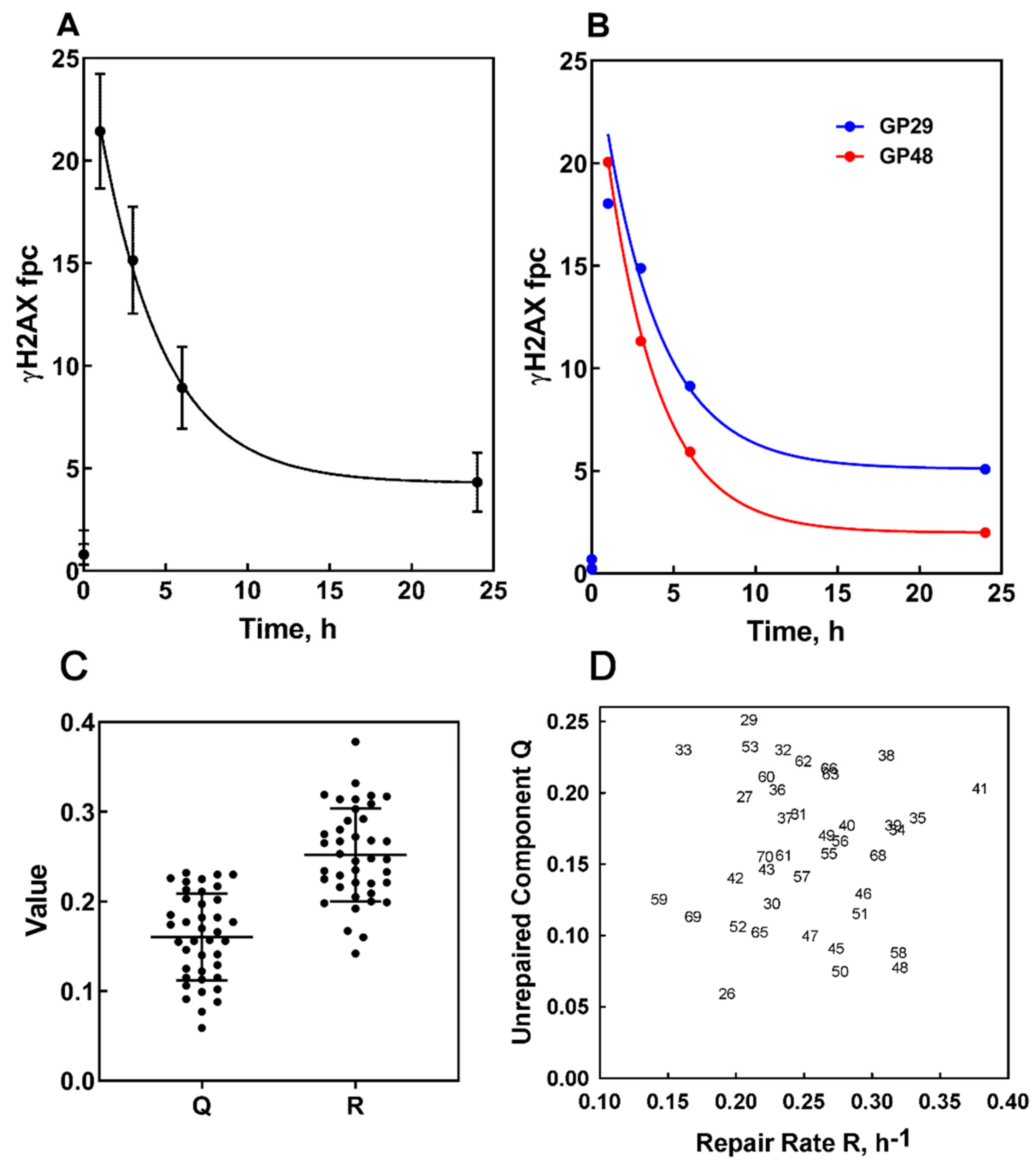
2.2. Ex Vivo Study: Kinetics of γ-H2AX Foci in Baseline PBMC that Were Exposed to Ex Vivo Irradiation
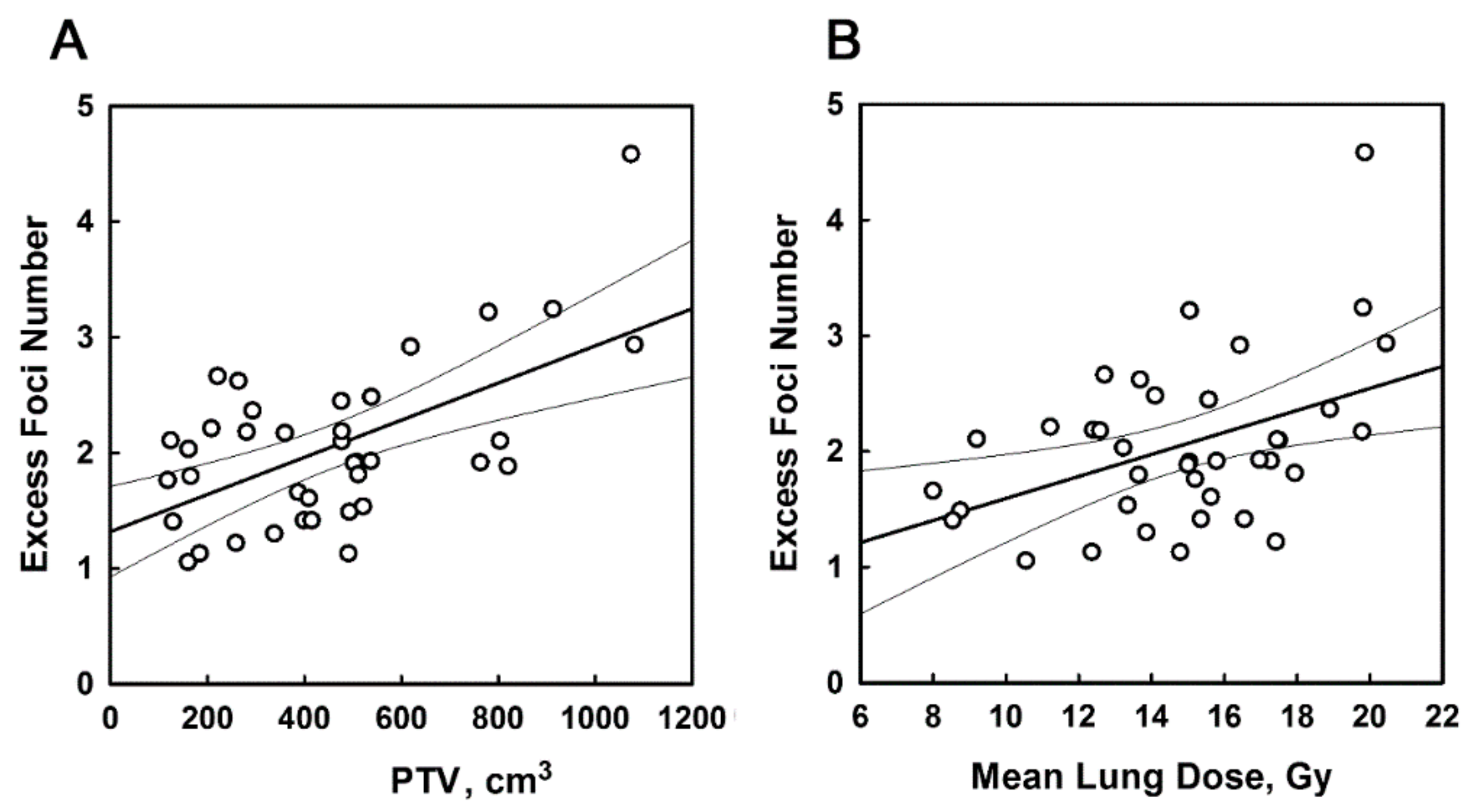
2.3. Correlation Studies with Treatment Conditions; PBMC that Were not Exposed to Ex Vivo Irradiation
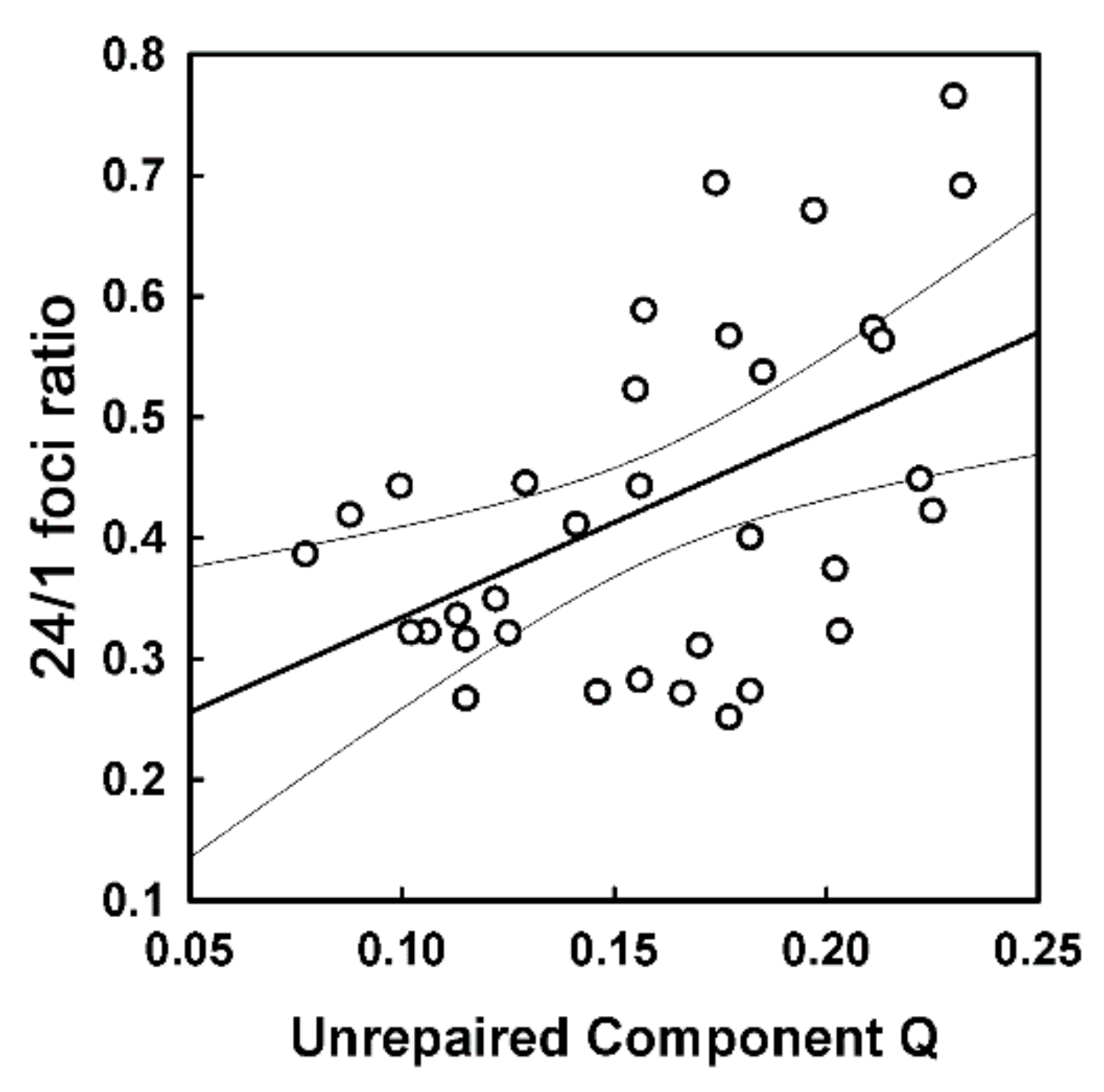
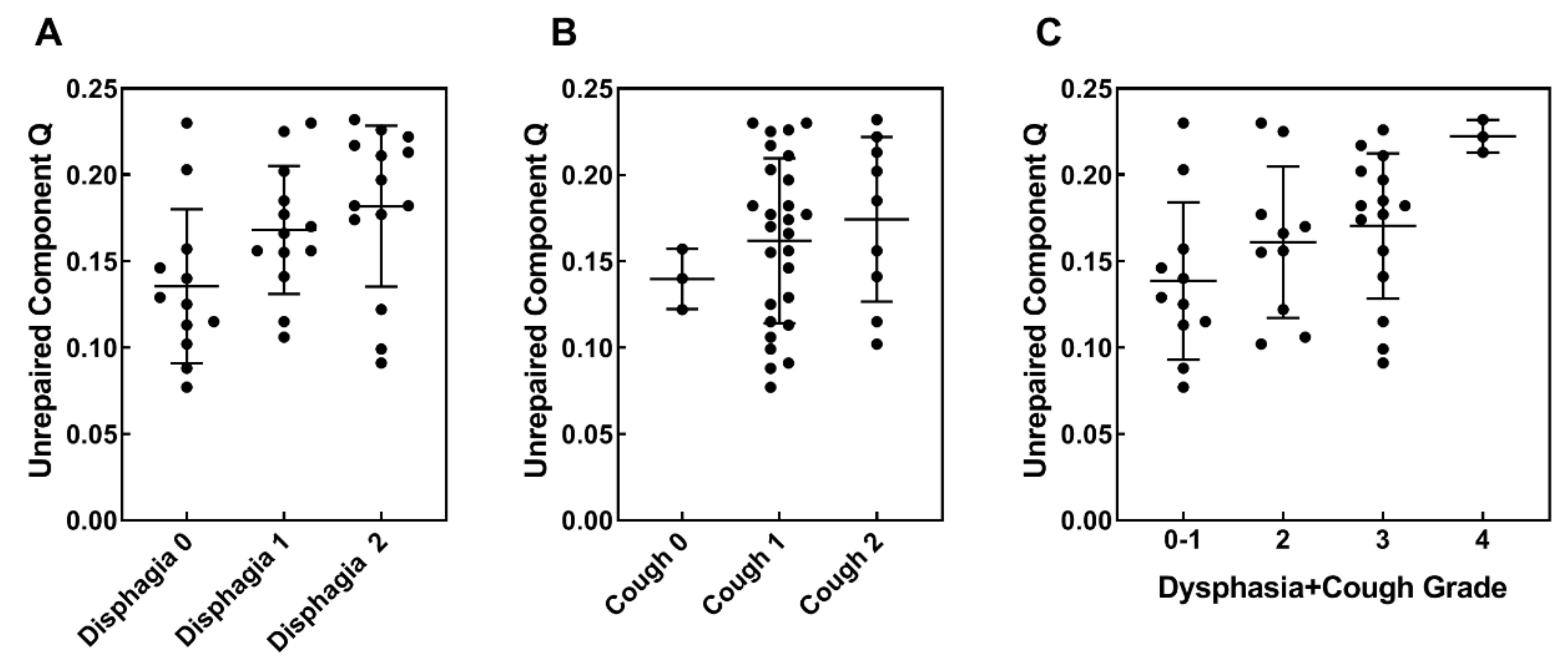
2.4. Correlation Studies with Treatment Outcomes; Baseline PBMC that Were Exposed to Ex Vivo Irradiation
3. Discussion
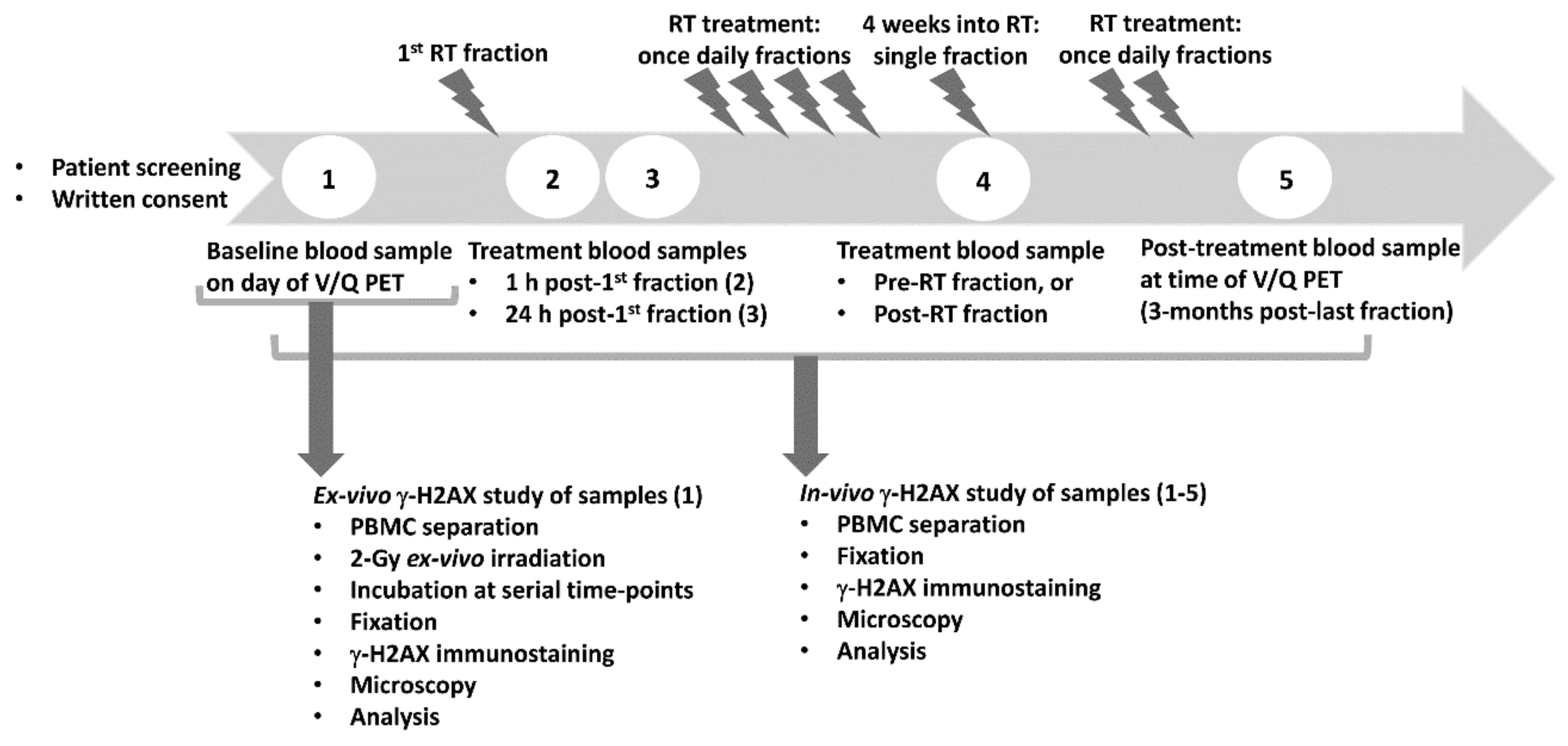
4. Materials and Methods
4.1. Patient Recruitment
4.2. Blood Collection and Processing
4.3. Immunostaining, Microscopy and Image Analysis
4.4. Data Analysis
4.4.1. Distributions of Foci Numbers
4.4.2. Analysis of Foci Kinetics
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Batumalai, V.; Wong, K.; Shafiq, J.; Hanna, T.P.; Gabriel, G.; Heberle, J.; Koprivic, I.; Kaadan, N.; King, O.; Tran, T.; et al. Estimating the cost of radiotherapy for 5-year local control and overall survival benefit. Radiother. Oncol. 2019, 136, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Travis, L.B. The epidemiology of second primary cancers. Cancer Epidemiol. Prev. Biomark. 2006, 15, 2020–2026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Travis, L.B.; Demark-Wahnefried, W.; Allan, J.M.; Wood, M.E.; Ng, A.K. Aetiology, genetics and prevention of secondary neoplasms in adult cancer survivors. Nat. Rev. Clin. Oncol. 2013, 10, 289–301. [Google Scholar] [CrossRef] [PubMed]
- Bradley, J.D.; Hu, C.; Komaki, R.R.; Masters, G.A.; Blumenschein, G.R.; Schild, S.E.; Bogart, J.A.; Forster, K.M.; Magliocco, A.M.; Kavadi, V.S.; et al. Long-Term Results of NRG Oncology RTOG 0617: Standard-Versus High-Dose Chemoradiotherapy With or Without Cetuximab for Unresectable Stage III Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2020, 38, 706–714. [Google Scholar] [CrossRef]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Kurata, T.; Chiappori, A.; Lee, K.H.; de Wit, M.; et al. Overall Survival with Durvalumab after Chemoradiotherapy in Stage III NSCLC. N. Engl. J. Med. 2018, 379, 2342–2350. [Google Scholar] [CrossRef]
- Palma, D.A.; Senan, S.; Tsujino, K.; Barriger, R.B.; Rengan, R.; Moreno, M.; Bradley, J.D.; Kim, T.H.; Ramella, S.; Marks, L.B.; et al. Predicting radiation pneumonitis after chemoradiation therapy for lung cancer: An international individual patient data meta-analysis. Int. J. Radiat. Oncol. Biol. Phys. 2013, 85, 444–450. [Google Scholar] [CrossRef] [Green Version]
- Barnett, G.C.; West, C.M.; Dunning, A.M.; Elliott, R.M.; Coles, C.E.; Pharoah, P.D.; Burnet, N.G. Normal tissue reactions to radiotherapy: Towards tailoring treatment dose by genotype. Nat. Rev. Cancer 2009, 9, 134–142. [Google Scholar] [CrossRef] [Green Version]
- Siva, S.; Callahan, J.; Kron, T.; Martin, O.A.; MacManus, M.P.; Ball, D.L.; Hicks, R.J.; Hofman, M.S. A prospective observational study of Gallium-68 ventilation and perfusion PET/CT during and after radiotherapy in patients with non-small cell lung cancer. BMC Cancer 2014, 14, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Martin, O.A.; Martin, R.F. Cancer Radiotherapy: Understanding the Price of Tumor Eradication. Front. Cell Dev. Biol. 2020, 8, 261. [Google Scholar] [CrossRef]
- Martin, O.A.; Yin, X.; Forrester, H.B.; Sprung, C.N.; Martin, R.F. Potential strategies to ameliorate risk of radiotherapy-induced second malignant neoplasms. Semin. Cancer Biol. 2016, 37, 65–76. [Google Scholar] [CrossRef]
- Sprung, C.N.; Forrester, H.B.; Siva, S.; Martin, O.A. Immunological markers that predict radiation toxicity. Cancer Lett. 2015, 368, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Bonner, W.M.; Redon, C.E.; Dickey, J.S.; Nakamura, A.J.; Sedelnikova, O.A.; Solier, S.; Pommier, Y. GammaH2AX and cancer. Nat. Rev. Cancer 2008, 8, 957–967. [Google Scholar] [CrossRef] [PubMed]
- Ivashkevich, A.; Redon, C.E.; Nakamura, A.J.; Martin, R.F.; Martin, O.A. Use of the gamma-H2AX assay to monitor DNA damage and repair in translational cancer research. Cancer Lett. 2012, 327, 123–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siva, S.; Lobachevsky, P.; MacManus, M.P.; Kron, T.; Moller, A.; Lobb, R.J.; Ventura, J.; Best, N.; Smith, J.; Ball, D.; et al. Radiotherapy for Non-Small Cell Lung Cancer Induces DNA Damage Response in Both Irradiated and Out-of-field Normal Tissues. Clin. Cancer Res. 2016, 22, 4817–4826. [Google Scholar] [CrossRef] [Green Version]
- Lobachevsky, P.; Leong, T.; Daly, P.; Smith, J.; Best, N.; Tomaszewski, J.; Thompson, E.R.; Li, N.; Campbell, I.G.; Martin, R.F.; et al. Compromized DNA repair as a basis for identification of cancer radiotherapy patients with extreme radiosensitivity. Cancer Lett. 2016, 383, 212–219. [Google Scholar] [CrossRef] [Green Version]
- Herschtal, A.; Martin, R.F.; Leong, T.; Lobachevsky, P.; Martin, O.A. A Bayesian Approach for Prediction of Patient Radiosensitivity. Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, 627–634. [Google Scholar] [CrossRef]
- Denoyer, D.; Lobachevsky, P.; Jackson, P.; Thompson, M.; Martin, O.A.; Hicks, R.J. Analysis of 177Lu-DOTA-octreotate therapy-induced DNA damage in peripheral blood lymphocytes of patients with neuroendocrine tumors. J. Nucl. Med. 2015, 56, 505–511. [Google Scholar] [CrossRef] [Green Version]
- Bussink, J.; Span, P.N. gamma-H2AX foci in peripheral blood lymphocytes to quantify radiation-induced DNA damage after 177Lu-DOTA-octreotate peptide receptor radionuclide therapy. J. Nucl. Med. 2015, 56, 501–502. [Google Scholar] [CrossRef] [Green Version]
- Balasubramaniam, S.; Redon, C.E.; Peer, C.J.; Bryla, C.; Lee, M.J.; Trepel, J.B.; Tomita, Y.; Rajan, A.; Giaccone, G.; Bonner, W.M.; et al. Phase I trial of belinostat with cisplatin and etoposide in advanced solid tumors, with a focus on neuroendocrine and small cell cancers of the lung. Anticancer. Drugs 2018, 29, 457–465. [Google Scholar] [CrossRef]
- Wang, L.H.; Pfister, T.D.; Parchment, R.E.; Kummar, S.; Rubinstein, L.; Evrard, Y.A.; Gutierrez, M.E.; Murgo, A.J.; Tomaszewski, J.E.; Doroshow, J.H.; et al. Monitoring drug-induced gammaH2AX as a pharmacodynamic biomarker in individual circulating tumor cells. Clin. Cancer Res. 2010, 16, 1073–1084. [Google Scholar] [CrossRef] [Green Version]
- Palmer, J.D.; Zaorsky, N.G.; Witek, M.; Lu, B. Molecular markers to predict clinical outcome and radiation induced toxicity in lung cancer. J. Thorac. Dis. 2014, 6, 387–398. [Google Scholar] [PubMed]
- Gomolka, M.; Blyth, B.; Bourguignon, M.; Badie, C.; Schmitz, A.; Talbot, C.; Hoeschen, C.; Salomaa, S. Potential screening assays for individual radiation sensitivity and susceptibility and their current validation state. Int. J. Radiat. Biol. 2020, 96, 280–296. [Google Scholar] [CrossRef] [PubMed]
- Siva, S.; MacManus, M.; Kron, T.; Best, N.; Smith, J.; Lobachevsky, P.; Ball, D.; Martin, O. A pattern of early radiation-induced inflammatory cytokine expression is associated with lung toxicity in patients with non-small cell lung cancer. PLoS ONE 2014, 9, e109560. [Google Scholar] [CrossRef]
- Adams, G.; Martin, O.A.; Roos, D.E.; Lobachevsky, P.N.; Potter, A.E.; Zacest, A.C.; Bezak, E.; Bonner, W.M.; Martin, R.F.; Leong, T. Enhanced intrinsic radiosensitivity after treatment with stereotactic radiosurgery for an acoustic neuroma. Radiother. Oncol. 2012, 103, 410–414. [Google Scholar] [CrossRef] [PubMed]
- Yin, X.; Mason, J.; Lobachevsky, P.N.; Munforte, L.; Selbie, L.; Ball, D.L.; Martin, R.F.; Leong, T.; Siva, S.; Martin, O.A. Radiation Therapy Modulates DNA Repair Efficiency in Peripheral Blood Mononuclear Cells of Patients With Non-Small Cell Lung Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2019, 103, 521–531. [Google Scholar] [CrossRef]
- Fleckenstein, J.; Kuhne, M.; Seegmuller, K.; Derschang, S.; Melchior, P.; Graber, S.; Fricke, A.; Rübe, C.E.; Rübe, C. The impact of individual in vivo repair of DNA double-strand breaks on oral mucositis in adjuvant radiotherapy of head-and-neck cancer. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 1465–1472. [Google Scholar] [CrossRef]
- Goutham, H.V.; Mumbrekar, K.D.; Vadhiraja, B.M.; Fernandes, D.J.; Sharan, K.; Kanive-Parashiva, G.K.; Kapaettu, S.; Sadashiva, S.R. DNA double-strand break analysis by gamma-H2AX foci: A useful method for determining the overreactors to radiation-induced acute reactions among head-and-neck cancer patients. Int. J. Radiat. Oncol. Biol. Phys. 2012, 84, e607–e612. [Google Scholar] [CrossRef]
- Li, P.; Du, C.R.; Xu, W.C.; Shi, Z.L.; Zhang, Q.; Li, Z.B.; Fu, S. Correlation of dynamic changes in gamma-H2AX expression in peripheral blood lymphocytes from head and neck cancer patients with radiation-induced oral mucositis. Radiat. Oncol. 2013, 8, 155. [Google Scholar] [CrossRef] [Green Version]
- Finnon, P.; Kabacik, S.; MacKay, A.; Raffy, C.; A’Hern, R.; Owen, R.; Badie, C.; Yarnold, J.; Bouffler, S. Correlation of in vitro lymphocyte radiosensitivity and gene expression with late normal tissue reactions following curative radiotherapy for breast cancer. Radiother. Oncol. 2012, 105, 329–336. [Google Scholar] [CrossRef]
- Greve, B.; Bolling, T.; Amler, S.; Rossler, U.; Gomolka, M.; Mayer, C. Evaluation of different biomarkers to predict individual radiosensitivity in an inter-laboratory comparison—Lessons for future studies. PLoS ONE 2012, 7, e47185. [Google Scholar] [CrossRef]
- Markova, E.; Somsedikova, A.; Vasilyev, S.; Pobijakova, M.; Lackova, A.; Lukacko, P.; Popanda, O.; Dreffke, K.; Rickinger, A.; Fritz, E. DNA repair foci and late apoptosis/necrosis in peripheral blood lymphocytes of breast cancer patients undergoing radiotherapy. Int. J. Radiat. Biol. 2015, 91, 934–945. [Google Scholar] [CrossRef]
- Bryant, J.; Shields, L.; Hynes, C.; Howe, O.; McCleanc, B.; Lynga, F. DNA Damage and Cytokine Production in Non-Target Irradiated Lymphocytes. Radiat. Res. 2019, 191, 545–555. [Google Scholar] [CrossRef] [PubMed]
- Rodemann, H.P.; Blaese, M.A. Responses of normal cells to ionizing radiation. Semin. Radiat. Oncol. 2007, 17, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Brush, J.; Lipnick, S.L.; Phillips, T.; Sitko, J.; McDonald, J.T.; McBride, W.H. Molecular mechanisms of late normal tissue injury. Semin. Radiat. Oncol. 2007, 17, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Schuster, B.; Ellmann, A.; Mayo, T.; Auer, J.; Haas, M.; Hecht, M.; Fietkau, R.; Distel, L.V. Rate of individuals with clearly increased radiosensitivity rise with age both in healthy individuals and in cancer patients. BMC Geriatr. 2018, 18, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Ivashkevich, A.N.; Martin, O.A.; Smith, A.J.; Redon, C.E.; Bonner, W.M.; Martin, R.F.; Lobachevsky, P.N. gammaH2AX foci as a measure of DNA damage: A computational approach to automatic analysis. Mutat. Res. 2011, 711, 49–60. [Google Scholar] [CrossRef] [Green Version]
- Jakl, L.; Lobachevsky, P.; Vokalova, L.; Durdik, M.; Markova, E.; Belyaev, I. Validation of JCountPro software for efficient assessment of ionizing radiation-induced foci in human lymphocytes. Int. J. Radiat. Biol. 2016, 92, 766–773. [Google Scholar] [CrossRef]
- Vogin, G.; Bastogne, T.; Bodgi, L.; Gillet-Daubin, J.; Canet, A.; Pereira, S.; Foray, N. The Phosphorylated ATM Immunofluorescence Assay: A High-performance Radiosensitivity Assay to Predict Postradiation Therapy Overreactions. Int. J. Radiat. Oncol. Biol. Phys. 2018, 101, 690–693. [Google Scholar] [CrossRef] [Green Version]
- Fhoghlu, M.N.; Barrett, S. A Review of Radiation-Induced Lymphocyte Apoptosis as a Predictor of Late Toxicity After Breast Radiotherapy. J. Med. Imaging Radiat. Sci. 2019, 50, 337–344. [Google Scholar] [CrossRef]
- Beaton, L.A.; Ferrarotto, C.; Marro, L.; Samiee, S.; Malone, S.; Grimes, S.; Malone, K.; Wilkins, R.C. Chromosome damage and cell proliferation rates in in vitro irradiated whole blood as markers of late radiation toxicity after radiation therapy to the prostate. Int. J. Radiat. Oncol. Biol. Phys. 2013, 85, 1346–1352. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time Points of Blood Collection | Baseline | 1 H Post First RT | 24 H Post First RT | 4 Weeks † (Sample Pre-RT) | 4 Weeks † (Sample Post-RT) | 3 Months Post-Final RT |
|---|---|---|---|---|---|---|
| Mean Value, fpc | 1.11 | 3.24 | 1.26 | 1.57 | 2.39 | 1.09 |
| Standard Deviation | 0.37 | 0.68 | 0.57 | 0.50 | 0.91 | 0.52 |
| Number of samples | 43 | 38 | 38 | 18 | 16 | 29 |
| p-value 1 relative to baseline | <0.0001 * | 0.130 | 0.0089 * | <0.0001 * | 0.688 |
| Parameter | PTV | MLD | Combined PTV and MLD | |||
|---|---|---|---|---|---|---|
| Correlation Coefficient | p-Value | Correlation Coefficient | p-Value | Correlation Coefficient | p-Value | |
| Average per cell number of induced foci | 0.235 | 0.155 | 0.234 | 0.158 | ||
| Fraction of affected cells | 0.417 | 0.010 | 0.274 | 0.0955 | ||
| Average per cell number of excess foci | 0.586 | 0.00011 | 0.437 | 0.00060 | 0.601 | <0.0001 |
| MLD | 0.597 | <0.0001 | ||||
| Tumour Response/Toxicity | Grade | N | Q-Values | R-Values | ||||
|---|---|---|---|---|---|---|---|---|
| Average | SD | p-Value | Average | SD | p-Value | |||
| Tumour response | CMR 1 | 12 | 0.155 | 0.048 | 0.246 | 0.048 | ||
| PMR 2 | 10 | 0.159 | 0.049 | 0.827 | 0.251 | 0.061 | 0.821 | |
| PMD 3 | 7 | 0.167 | 0.048 | 0.600 | 0.277 | 0.039 | 0.146 | |
| Dyspnoea | 0 | 7 | 0.161 | 0.044 | 0.226 | 0.050 | ||
| 1 | 18 | 0.175 | 0.043 | 0.488 | 0.265 | 0.048 | 0.110 | |
| 2 | 14 | 0.149 | 0.050 | 0.586 | 0.252 | 0.055 | 0.299 | |
| Cough | 0 | 3 | 0.140 | 0.018 | 0.230 | 0.035 | ||
| 1 | 27 | 0.162 | 0.048 | 0.155 | 0.256 | 0.058 | 0.327 | |
| 2 | 9 | 0.174 | 0.048 | 0.098 | 0.253 | 0.036 | 0.383 | |
| Pneumonitis | 0 | 20 | 0.168 | 0.042 | 0.267 | 0.055 | ||
| 1 | 7 | 0.140 | 0.039 | 0.135 | 0.227 | 0.051 | 0.109 | |
| 2 | 12 | 0.168 | 0.056 | 0.998 | 0.247 | 0.041 | 0.265 | |
| Dermatitis | 0 | 9 | 0.170 | 0.044 | 0.210 | 0.032 | ||
| 1 | 22 | 0.162 | 0.047 | 0.661 | 0.270 | 0.049 | 0.001 | |
| 2 | 9 | 0.141 | 0.071 | 0.314 | 0.228 | 0.098 | 0.630 | |
| Fatigue | 0 | 4 | 0.171 | 0.046 | 0.224 | 0.057 | ||
| 1 | 27 | 0.156 | 0.047 | 0.589 | 0.268 | 0.046 | 0.218 | |
| 2 | 7 | 0.189 | 0.042 | 0.551 | 0.229 | 0.040 | 0.878 | |
| Nausea | 0 | 30 | 0.157 | 0.048 | 0.249 | 0.053 | ||
| 1 | 7 | 0.186 | 0.040 | 0.131 | 0.269 | 0.046 | 0.348 | |
| 2 | 2 | 0.166 | 0.016 | 0.587 | 0.267 | 0.066 | 0.768 | |
| Dysphagia | 0 | 12 | 0.135 | 0.045 | 0.253 | 0.069 | ||
| 1 | 13 | 0.168 | 0.037 | 0.061 | 0.244 | 0.044 | 0.690 | |
| 2 | 14 | 0.182 | 0.047 | 0.016 | 0.263 | 0.042 | 0.697 | |
| Cough + dysphagia | 0-1 | 11 | 0.138 | 0.046 | 0.257 | 0.072 | ||
| 2 | 10 | 0.161 | 0.044 | 0.264 | 0.227 | 0.038 | 0.251 | |
| 3 | 15 | 0.170 | 0.042 | 0.083 | 0.239 | 0.098 | 0.583 | |
| 4 | 3 | 0.222 | 0.010 | 0.00011 | 0.242 | 0.030 | 0.598 | |
| Patient ID | Age | Gender | Pathology | Stage | PTV (cm3) | MLD | RT/CRT | 4 Weeks Beforeore or After RT | PET Response | Dyspnoea Grade | Cough Grade | Pneumonitis Grade | Dermatitis Grade | Fatigue Grade | Nausea Grade | Dysphagia Grade |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| GP26 | 59 | M | SCC | N/A | 11.69 | N/A | 1 | 1 | 0 | 0 | 0 | 0 | 0 | |||
| GP27 | 67 | M | NSCLC | T2N2M0 | 360 | 19.79 | CRT: ca/pa | Before | CMR | 0 | 1 | 0 | 2 | 1 | 1 | 2 |
| GP28 | 69 | M | AC | T2N2M0 | 453 | 15.73 | CRT: ca/pa | N/A | 0 | 1 | 0 | 0 | 0 | 0 | 2 | |
| GP29 | 49 | M | AC | T4N0M0 | 387 | 8.00 | CRT: cis/et | Before | N/A | 1 | 1 | 0 | 0 | 2 | 0 | 1 |
| GP30 | 48 | F | AC | T3N3M0 | 493 | 8.75 | CRT: cis/et | After | PMR | 0 | 0 | 1 | 2 | 1 | 0 | 2 |
| GP31 | 63 | M | SCC | T3N2M1b | 1081 | 20.45 | CRT: ca/pa | After | PMD | 1 | 2 | 2 | 1 | 0 | 0 | 1 |
| GP32 | 64 | M | SCC | T1aN1M1b | 184 | 14.79 | CRT: ca/pa | After | PMR | 1 | 1 | 2 | 2 | 1 | 0 | 0 |
| GP33 | 69 | M | AC | 251 | 12.29 | N/A | 0 | 1 | 0 | 0 | 0 | 0 | 1 | |||
| GP34 | 60 | M | AC | T2N2M1b | 491 | 12.36 | CRT: ca/pa | Before | N/A | 1 | 1 | 0 | 2 | 1 | 1 | 3 |
| GP35 | 70 | F | SCC | T4N0M0 | 1074 | 19.86 | CRT: cis/et | Before | PMD | 1 | 1 | 0 | 1 | 1 | 0 | 2 |
| GP36 | 75 | F | AC | T2aN3M0 | 521 | 13.34 | CRT: ca/pal | Before | PMR | 1 | 2 | 2 | 1 | 1 | 0 | 1 |
| GP37 | 78 | M | AC | T2bN2M0 | 763 | 15.79 | CRT: ca/pa | Before | CMR | 1 | 1 | 2 | 2 | 2 | 0 | 2 |
| GP38 | 68 | F | AC | T3N2M1b | 508 | 17.28 | CRT: cis/et | After | N/A | 1 | 1 | 0 | 1 | 1 | 1 | 2 |
| GP39 | 75 | M | NSCLC | T2bN3M0 | 913 | 19.81 | CRT: ca/pa | Before | N/A | 0 | 1 | 0 | 3 | 1 | 2 | 3 |
| GP40 | 70 | M | AC | T3N0M0 | 409 | 15.63 | RT | Before | N/A | 3 | 1 | 0 | 1 | 2 | 0 | 1 |
| GP41 | 72 | M | NSCLC | T1N2M0 | 399 | 16.55 | CRT: ca/pa | Before | PMR | 1 | 1 | 0 | 1 | 1 | 0 | 0 |
| GP42 | 64 | F | AC | N/A | 17.39 | N/A | 1 | 1 | 0 | 0 | 0 | 0 | 0 | |||
| GP43 | 67 | M | SCC | T4N1M0 | 780 | 15.05 | N/A | 1 | 1 | 0 | 0 | 1 | 0 | 0 | ||
| GP44 | 62 | M | NSCLC | T1N2M0 | 415 | 15.36 | CRT: ca/pa | Before | CMR | 1 | 1 | 1 | 3 | 2 | 1 | 2 |
| GP45 | 74 | F | AC | T1bN3M0 | 718 | 17.10 | CRT: ca/pa | Before | N/A | 1 | 1 | 0 | 1 | 1 | 0 | 2 |
| GP46 | 74 | F | AC | T2N3M0 | 477 | 17.50 | CRT: cis/et | Before | PMR | 3 | 1 | 0 | 1 | 0 | 0 | 0 |
| GP47 | 68 | M | SCC | rT0N2M0 | 160 | 10.55 | CRT: ca/pa | After | PMR | 1 | 1 | 2 | 1 | 1 | 0 | 2 |
| GP48 | 63 | F | AC | T1N2M0 | 259 | 17.42 | RT | After | CMR | 2 | 1 | 2 | 2 | 1 | 0 | 0 |
| GP49 | 74 | M | SCC | T2aN0M0 | 129 | 8.54 | RT | Before | PMD | 2 | 1 | 0 | 1 | 2 | 0 | 1 |
| GP50 | 78 | F | NSCLC | T1N2M0 | 161 | 13.23 | CRT: ca/pa | Before | CMR | 1 | 2 | 2 | 1 | 1 | 1 | 1 |
| GP51 | 82 | M | AC | T1cM0M0 | 124 | 9.20 | RT | After | PMD | 2 | 1 | 0 | 1 | 1 | 0 | 0 |
| GP52 | 48 | M | AC | T3N2M0 | 338 | 13.86 | CRT: cis/et | After | CMR | 3 | 1 | 1 | 2 | 1 | 0 | 1 |
| GP53 | 67 | M | SCC | T1N0M0 | 118 | 15.20 | CRT: cis/et | Before | CMR | 2 | 2 | 2 | 1 | 2 | 0 | 2 |
| GP54 | 68 | F | AC | T1bN2M0 | 264 | 13.69 | CRT: ca/pa | After | PMR | 0 | 1 | 1 | 1 | 2 | 0 | 2 |
| GP55 | 82 | M | SCC | T2aN2M0 | 165 | 13.65 | CRT: ca | After | CMR | 0 | 0 | 0 | 1 | 1 | 1 | 0 |
| GP56 | 48 | M | AC | T3N2M0 | 502 | 15.04 | CRT: ca/pa | After | PMR | 1 | 1 | 0 | 1 | 1 | 0 | 1 |
| GP57 | 68 | M | AC | T3N0M0 | 221 | 12.71 | CRT: ca/pa | Before | CMR | 1 | 2 | 2 | 0 | 1 | 0 | 1 |
| GP58 | 68 | M | AC | T2aN2M0 | 537 | 16.97 | CRT: ca/pa | Before | PMD | 2 | 1 | 0 | 1 | 1 | 0 | 0 |
| GP59 | 71 | F | SCC | T4N0M0 | 208 | 11.22 | CRT: ca/pa | Before | PMR | 2 | 1 | 1 | 1 | 3 | 0 | 0 |
| GP60 | 35 | M | AC | T2bN2M1b | 538 | 14.10 | CRT: cis/et | Before | PMD | 1 | 1 | 0 | 1 | 1 | 1 | 2 |
| GP61 | 67 | M | NSCLC | T3N2M0 | 804 | 17.45 | CRT: ca/pa | After | CMR | 2 | 1 | 1 | 0 | 1 | 0 | 1 |
| GP62 | 80 | F | AC | T1N2M0 | 293 | 18.90 | CRT: ca/pa | After | CMR | 2 | 2 | 2 | 0 | 2 | 1 | 2 |
| GP63 | 63 | F | SCC | T3N2M0 | 619 | 16.43 | CRT: ca/pa | PMR | 1 | 2 | 1 | 1 | 1 | 0 | 2 | |
| GP64 | 84 | F | SCC | T4N0M0 | 91 | 5.90 | RT | After | CMR | 1 | 1 | 0 | 0 | 2 | 0 | 2 |
| GP65 | 72 | M | AC | T3N2M0 | 476 | 15.57 | CRT: ca/pa | Before | PMR | 0 | 2 | 1 | 1 | 1 | 0 | 0 |
| GP66 | 71 | M | NSCLC | T4N0M0 | 477 | 12.40 | CRT: ca/pa | After | PMR | 1 | 2 | 1 | 1 | 1 | 0 | 2 |
| GP67 | 68 | F | AC | T1aN1M0 | 267 | 14.45 | RT | Before | PMD | 2 | 1 | 2 | 1 | 1 | 0 | 2 |
| GP68 | 80 | M | SCC | T2BN2M0 | 281 | 12.59 | CRT: ca/pa | After | CMR | 2 | 2 | 1 | 1 | 1 | 0 | 1 |
| GP69 | 71 | M | SCC | T2N2M0 | 511 | 17.94 | CRT: ca/pa | After | CMR | 2 | 1 | 2 | 0 | 2 | 0 | 0 |
| GP70 | 64 | M | AC | T4N2M1b | 820 | 15.00 | CRT: ca/pa | After | N/A | 1 | 1 | 0 | 0 | 1 | 2 | 1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lobachevsky, P.N.; Bucknell, N.W.; Mason, J.; Russo, D.; Yin, X.; Selbie, L.; Ball, D.L.; Kron, T.; Hofman, M.; Siva, S.; et al. Monitoring DNA Damage and Repair in Peripheral Blood Mononuclear Cells of Lung Cancer Radiotherapy Patients. Cancers 2020, 12, 2517. https://doi.org/10.3390/cancers12092517
Lobachevsky PN, Bucknell NW, Mason J, Russo D, Yin X, Selbie L, Ball DL, Kron T, Hofman M, Siva S, et al. Monitoring DNA Damage and Repair in Peripheral Blood Mononuclear Cells of Lung Cancer Radiotherapy Patients. Cancers. 2020; 12(9):2517. https://doi.org/10.3390/cancers12092517
Chicago/Turabian StyleLobachevsky, Pavel N., Nicholas W. Bucknell, Joel Mason, Diane Russo, Xiaoyu Yin, Lisa Selbie, David L. Ball, Tomas Kron, Michael Hofman, Shankar Siva, and et al. 2020. "Monitoring DNA Damage and Repair in Peripheral Blood Mononuclear Cells of Lung Cancer Radiotherapy Patients" Cancers 12, no. 9: 2517. https://doi.org/10.3390/cancers12092517