
Training Simulators for Gastrointestinal Endoscopy: Current and Future Perspectives

 , , ,
, , ,  ,
,  and
and 
Abstract
:Simple Summary
Abstract
1. Introduction
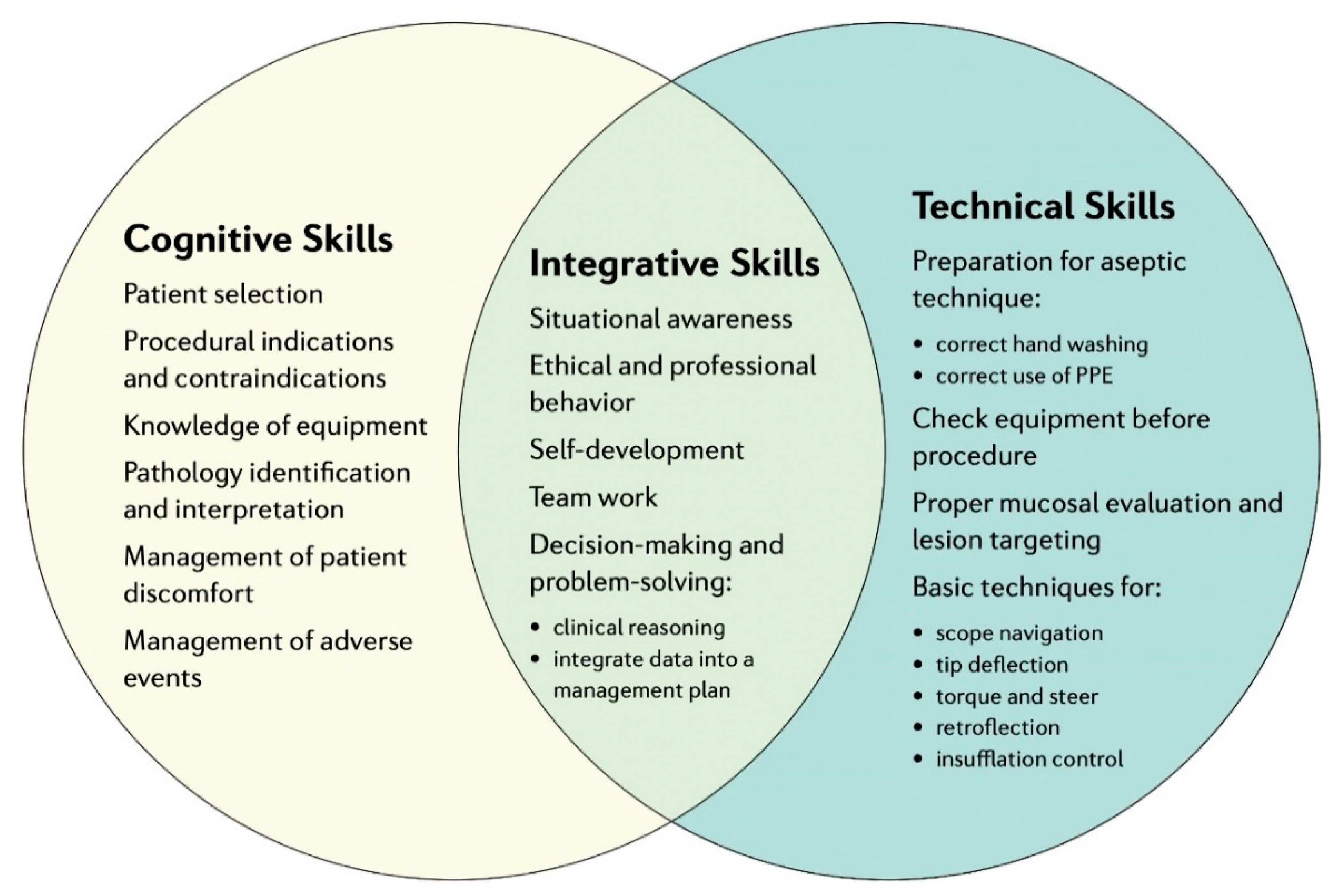
2. Fundamentals of Training in GI Endoscopy
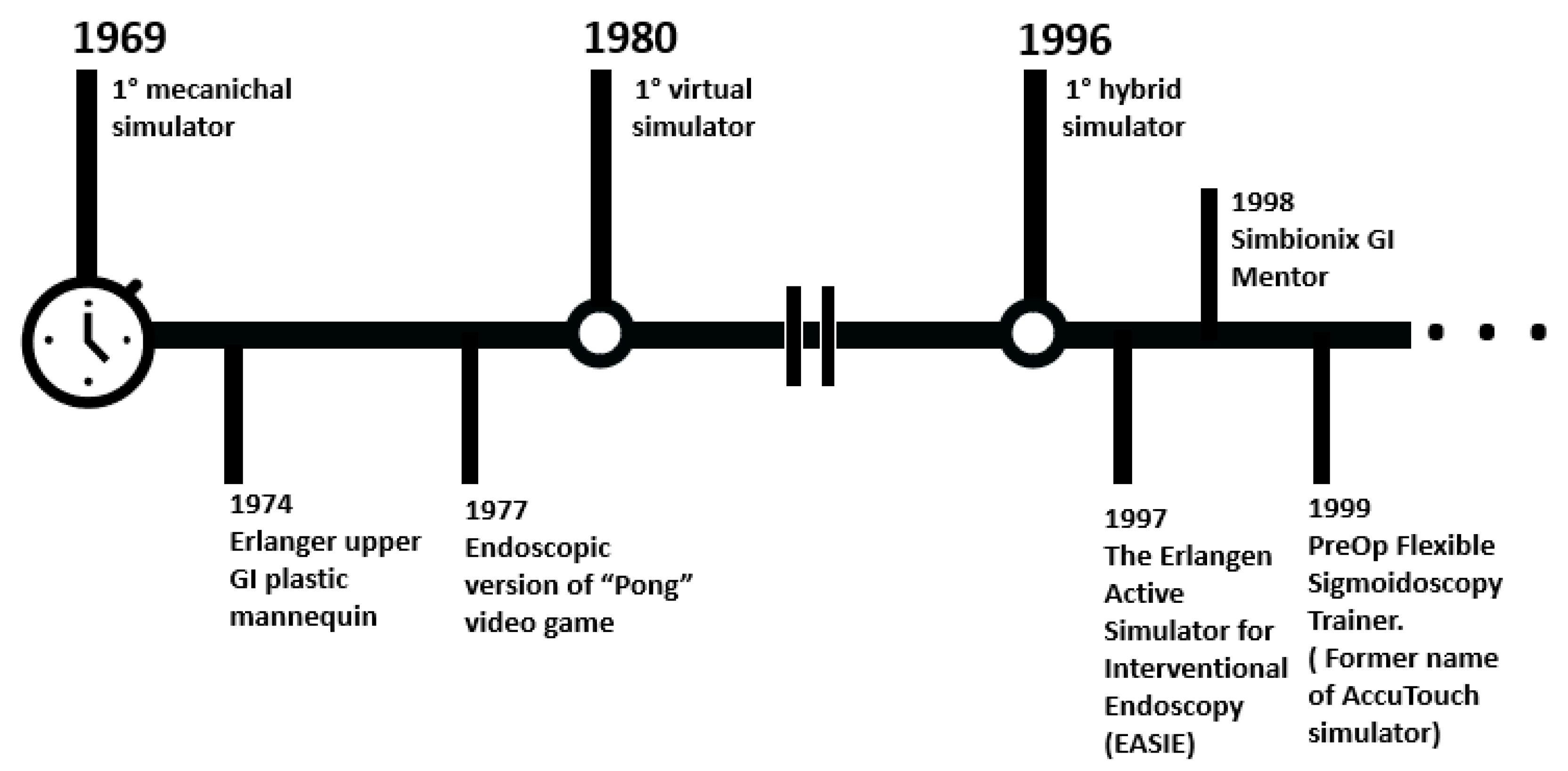
3. Conventional/Standard Simulators for Training
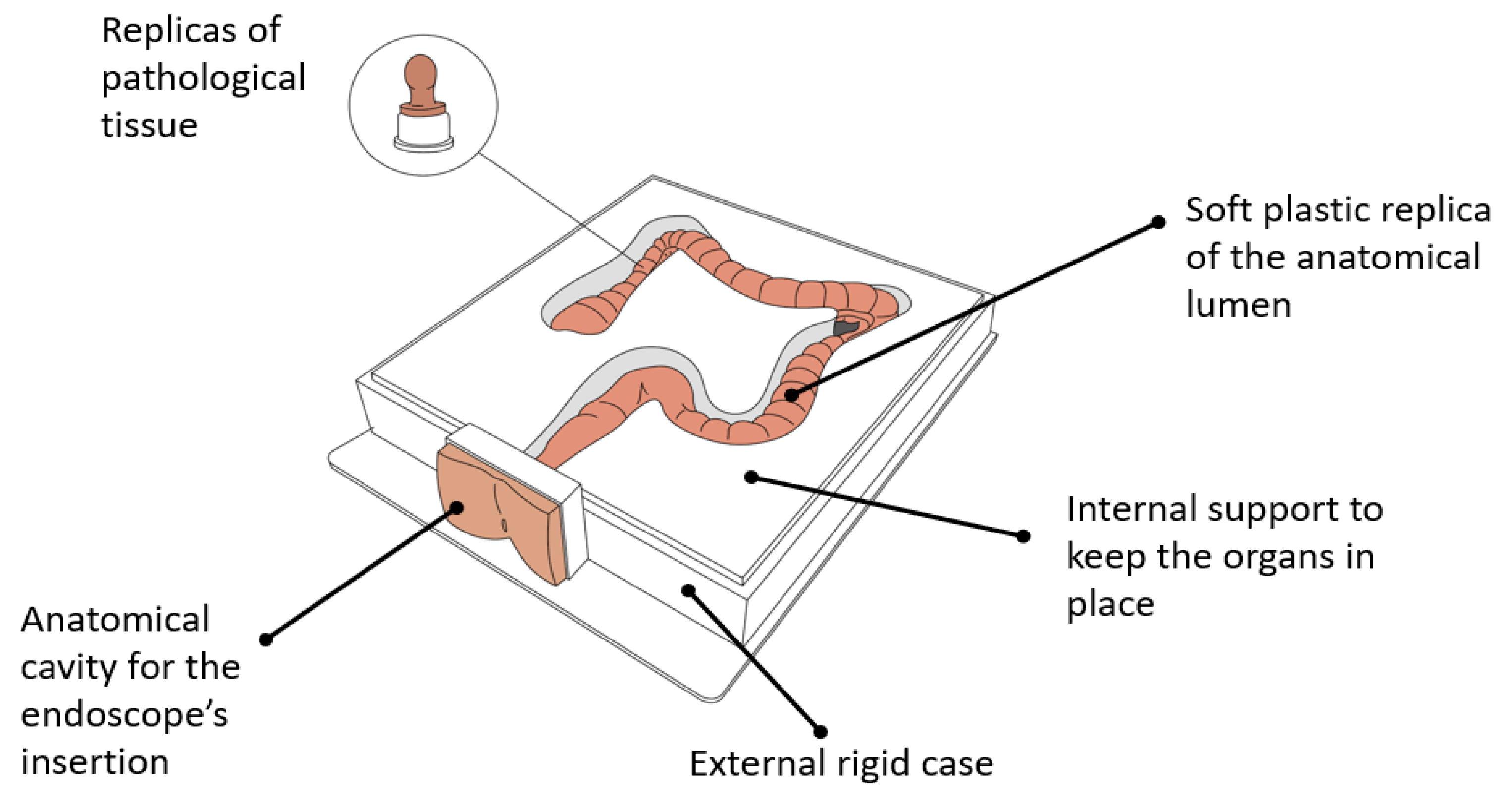
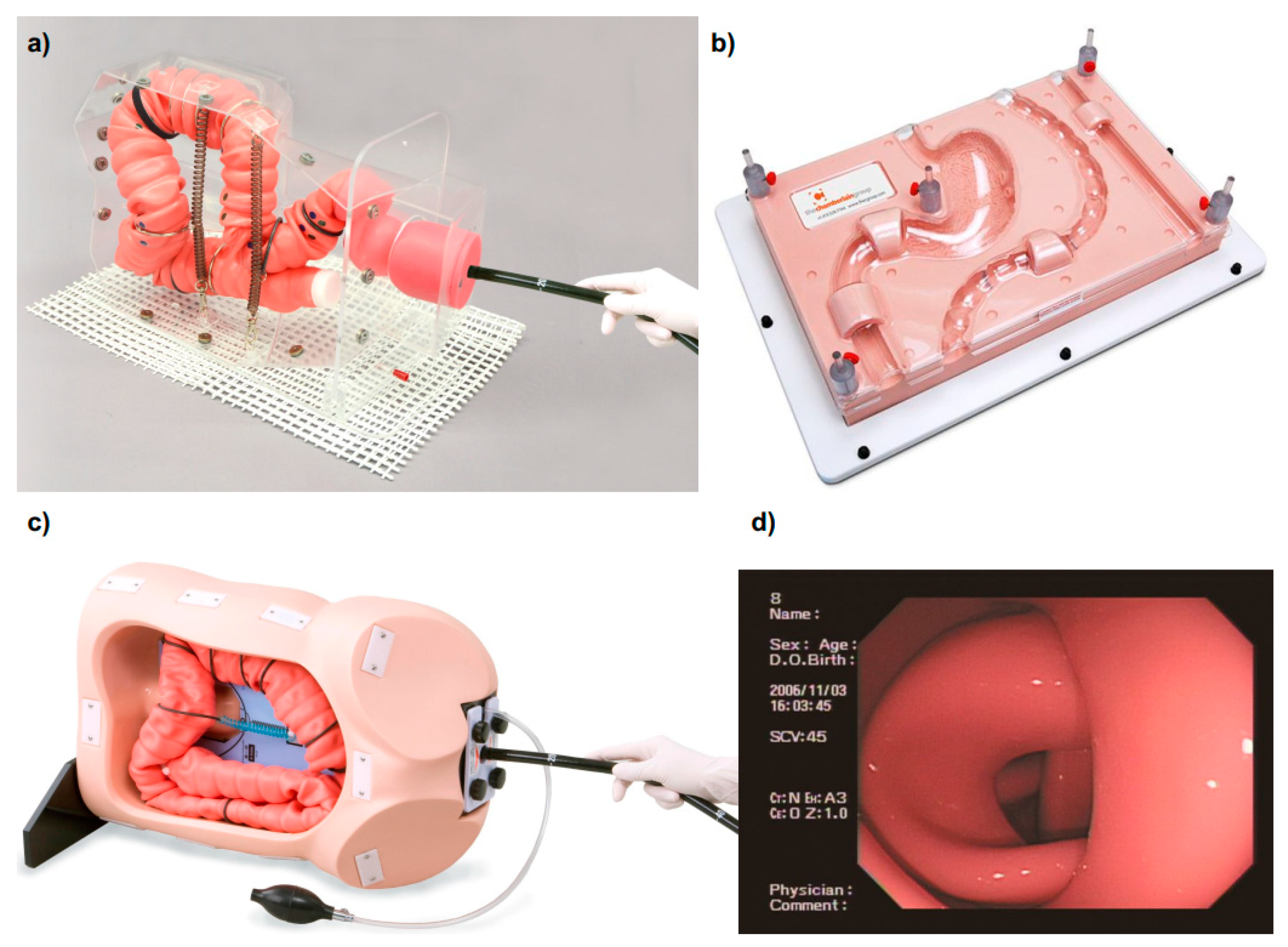
3.1. Mechanical Simulators for GI Endoscopy
- a replica of the anatomical lumen (i.e., esophagus, stomach, small intestine, colon) resembling the living organ in terms of visual appearance and tactile texture, made with soft plastic (e.g., silicone rubbers);
- an external rigid case containing the phantom, endowed with one or multiple cavities, allowing the insertion of the endoscope (i.e., replicas of mouth, anal sphincter, nose);
- rigid or semi-flexible internal support for keeping the organs in place, in some cases allowing the partial deformation/movement of the lumen during the procedure;
- optional adds-on replicas of pathologic tissue (e.g., polyps) to be attached to the main organ, allowing one to practice multiple tasks (e.g., clipping, stenting, biopsy, polypectomy).
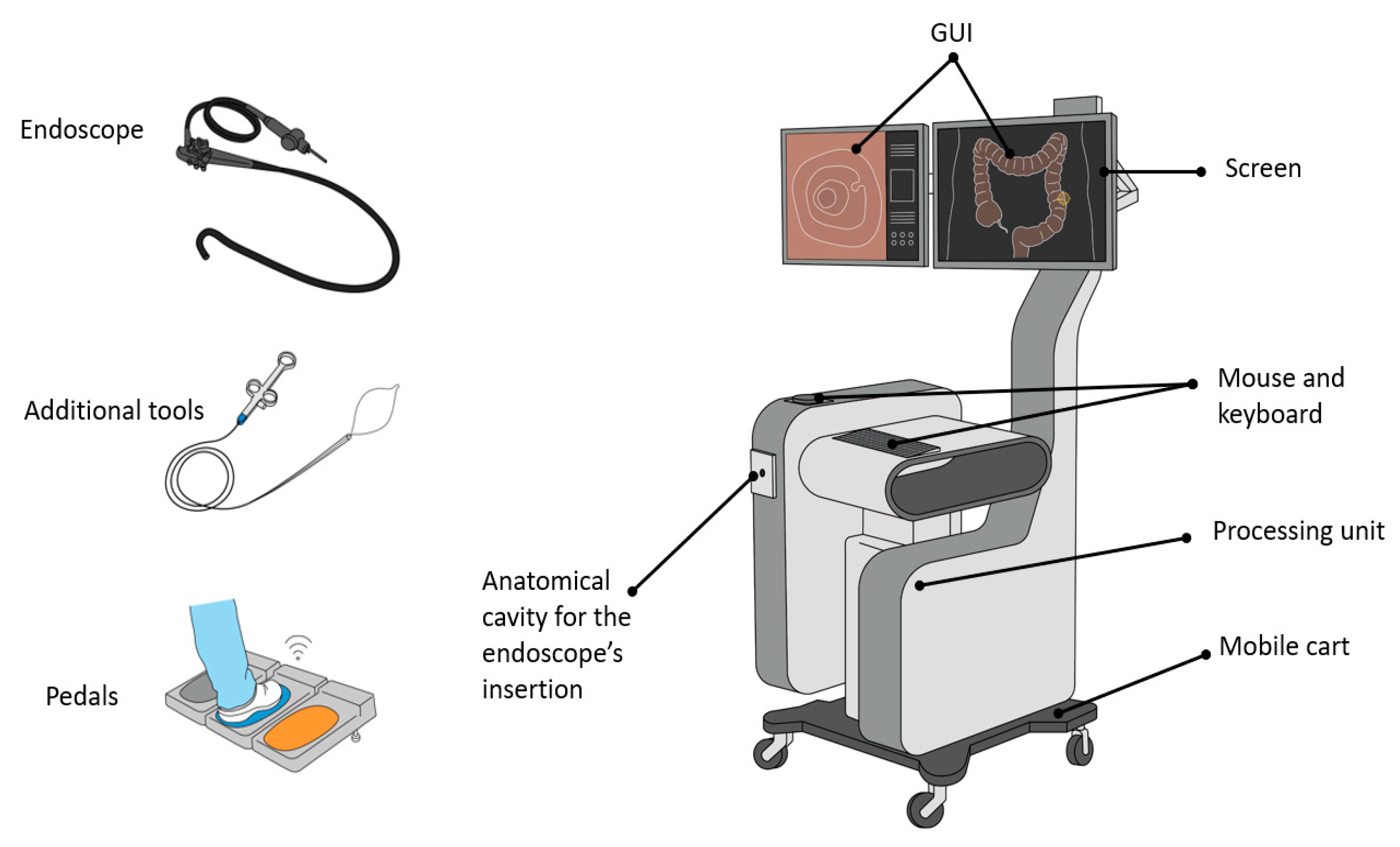
3.2. Computerized Simulators for GI Endoscopy
- a mobile cart platform including one or two screens, a keyboard or/and a touchpad, a box with one or two anatomical plates (i.e., holes) for inserting the endoscope, and a processing unit;
- a set of scope heads and tubes for upper and lower GI tract endoscopy with identical appearance and functionalities of those used in the clinical practice;
- a collection of tools to insert in the endoscope operative channels (e.g., forceps, electrodes for coagulation); and
- optional pedals for extra functionalities.
- a graphical user interface (GUI) showing the simulated endoscopic environment together with all the additional information and aids regarding the procedure;
- biomechanical simulation of the organs, allowing one to reproduce the expansion and the collapse of the lumen under insufflation or, in the case of a colonoscopy, looping formation;
- haptic feedback mimicking the tactile sensation normally felt by the endoscopists while navigating the endoscope throughout a lumen;
- a repository of real patient cases simulating diverse pathologies and anatomies with different level of difficulty both for upper and lower GI tracts;
- indications for performance metrics both real-time and as a summary at the end of each procedure;
- didactic modules providing online aids to the user such as step by step instructions on how to perform the procedure or a 3D map of the scope inside the lumen.
3.3. Animal Models
3.3.1. In-Vivo Animal Models
3.3.2. Ex-Vivo Animal Models
4. GI Endoscopy Simulators in Research
5. Validation of GI Simulators
6. Experts’ Commentary and Lesson Learned
6.1. Clinically Oriented
6.2. Technologically Oriented
7. Conclusions and Future Perspectives
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| GI | Gastrointestinal |
| ASGE | American Society for Gastrointestinal Endoscopy |
| ERCP | Endoscopic Retrograde Cholangio-Pancreatography |
| EGD | Esophagastroduodenoscopy |
| EUS | Endoscopic Ultrasonography |
| EMR | Endoscopic Mucosal Resection |
| ESD | Endoscopic Submucosal Dissection |
| AI | Artificial Intelligence |
| FGE | Fundamentals of GI Endoscopy |
| VR | Virtual Reality |
| AR | Augmented Reality |
| SAGES | Society of American Gastrointestinal and Endoscopic Surgeons |
| PIVI | Preservation and Incorporation of Valuable endoscopic Innovations |
| POEM | Per Oral Endoscopic Myotomy |
| NOTES | Natural Orifice Transluminal Endoscopic Surgery |
References
- Hd, M. A New System for Teaching Proctosigmoidoscopic Morphology. Am. J. Gastroenterol. 1969, 52, 65–69. [Google Scholar]
- Cohen, J.; Bosworth, B.P.; Chak, A.; Dunkin, B.J.; Early, D.S.; Gerson, L.B.; Hawes, R.H.; Haycock, A.V.; Hochberger, J.H.; Hwang, J.H.; et al. Preservation and Incorporation of Valuable Endoscopic Innovations (PIVI) on the Use of Endoscopy Simulators for Training and Assessing Skill. Gastrointest. Endosc. 2012, 76, 471–475. [Google Scholar] [CrossRef] [PubMed]
- Adler, D.G.; Bakis, G.; Coyle, W.J.; Degregorio, B.; Dua, K.S.; Lee, L.S.; McHenry, L.; Pais, S.A.; Rajan, E.; Sedlack, R.E.; et al. Principles of Training in GI Endoscopy. Gastrointest. Endosc. 2012, 75, 231–235. [Google Scholar] [CrossRef]
- Sedlack, R.E. The State of Simulation in Endoscopy Education: Continuing to Advance toward Our Goals. Gastroenterology 2013, 144, 9–12. [Google Scholar] [CrossRef] [PubMed]
- Bini, E.J.; Firoozi, B.; Choung, R.J.; Ali, E.M.; Osman, M.; Weinshel, E.H. Systematic Evaluation of Complications Related to Endoscopy in a Training Setting: A Prospective 30-Day Outcomes Study. Gastrointest. Endosc. 2003, 57, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Khan, R.; Plahouras, J.; Johnston, B.C.; Scaffidi, M.A.; Grover, S.C.; Walsh, C.M. Virtual Reality Simulation Training for Health Professions Trainees in Gastrointestinal Endoscopy. Cochrane Database Syst. Rev. 2018, 2018. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.C.; Rex, D.K. Endoscopist Can Be More Powerful than Age and Male Gender in Predicting Adenoma Detection at Colonoscopy. Am. J. Gastroenterol. 2007, 102, 856–861. [Google Scholar] [CrossRef] [PubMed]
- Barclay, R.L.; Vicari, J.J.; Doughty, A.S.; Johanson, J.F.; Greenlaw, R.L. Colonoscopic Withdrawal Times and Adenoma Detection during Screening Colonoscopy. N. Engl. J. Med. 2006, 355, 2533–2541. [Google Scholar] [CrossRef] [Green Version]
- Siau, K.; Hawkes, N.D.; Dunckley, P. Training in Endoscopy. Curr. Treat. Options Gastroenterol. 2018, 16, 345–361. [Google Scholar] [CrossRef]
- Ekkelenkamp, V.E.; Koch, A.D.; De Man, R.A.; Kuipers, E.J. Training and Competence Assessment in GI Endoscopy: A Systematic Review. Gut 2016, 65, 607–615. [Google Scholar] [CrossRef]
- Ward, S.T.; Mohammed, M.A.; Walt, R.; Valori, R.; Ismail, T.; Dunckley, P. An Analysis of the Learning Curve to Achieve Competency at Colonoscopy Using the JETS Database. Gut 2014, 63, 1746–1754. [Google Scholar] [CrossRef] [Green Version]
- Ward, S.T.; Hancox, A.; Mohammed, M.A.; Ismail, T.; Griffiths, E.A.; Valori, R.; Dunckley, P. The Learning Curve to Achieve Satisfactory Completion Rates in Upper GI Endoscopy: An Analysis of a National Training Database. Gut 2017, 66, 1022–1030. [Google Scholar] [CrossRef]
- Hazey, J.W.; Marks, J.M.; Mellinger, J.D.; Trus, T.L.; Chand, B.; Delaney, C.P.; Dunkin, B.J.; Fanelli, R.D.; Fried, G.M.; Martinez, J.M.; et al. Why Fundamentals of Endoscopic Surgery (FES)? Surg. Endosc. 2014, 28, 701–703. [Google Scholar] [CrossRef] [Green Version]
- Sedlack, R.E.; Shami, V.M.; Adler, D.G.; Coyle, W.J.; Degregorio, B.; Dua, K.S.; Dimaio, C.J.; Lee, L.S.; McHenry, L.; Pais, S.A.; et al. Colonoscopy Core Curriculum. Gastrointest. Endosc. 2012, 76, 482–490. [Google Scholar] [CrossRef] [PubMed]
- Walsh, C.M. In-Training Gastrointestinal Endoscopy Competency Assessment Tools: Types of Tools, Validation and Impact. In Best Practice and Research: Clinical Gastroenterology; Bailliere Tindall Ltd.: Kent, UK, 1 June 2016; pp. 357–374. [Google Scholar] [CrossRef]
- Azzam, N.; Khamis, N.; Almadi, M.; Batwa, F.; Alsohaibani, F.; Aljebreen, A.; Alharbi, A.; Alaska, Y.; Alameel, T.; Irving, P.; et al. Development and Validation of Metric-Based-Training to Proficiency Simulation Curriculum for Upper Gastrointestinal Endoscopy Using a Novel Assessment Checklist. Saudi J. Gastroenterol. 2020, 26, 179–187. [Google Scholar] [CrossRef]
- Waschke, K.A.; Anderson, J.; Valori, R.M.; MacIntosh, D.G.; Kolars, J.C.; DiSario, J.A.; Faigel, D.O.; Petersen, B.T.; Cohen, J. ASGE Principles of Endoscopic Training. Gastrointest. Endosc. 2019, 90, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Triantafyllou, K. Virtual Reality Simulators for Gastrointestinal Endoscopy Training. World J. Gastrointest. Endosc. 2014, 6, 6–12. [Google Scholar] [CrossRef]
- Gerson, L.B.; Van Dam, J. Technology Review: The Use of Simulators for Training in GI Endoscopy. Gastrointest. Endosc. 2004, 60, 992–1001. [Google Scholar] [CrossRef]
- Classen, M.; Ruppin, H. Practical Endoscopy Training Using a New Gastrointestinal Phantom. Endoscopy 1974, 6, 127–131. [Google Scholar] [CrossRef]
- EMS Trainer (#2068). The Chamberlain Group. Available online: https://www.thecgroup.com/product/ems-trainer-2068/ (accessed on 7 September 2020).
- Koken Co., Ltd. Available online: https://www.kokenmpc.co.jp/english/index.html (accessed on 7 September 2020).
- KYOTO KAGAKU. Available online: https://www.kyotokagaku.com/en/ (accessed on 7 September 2020).
- Upper GI Trainer (#2002). The Chamberlain Group. Available online: https://www.thecgroup.com/product/upper-gi-trainer-2002/ (accessed on 10 March 2021).
- Biliary Endoscopy Trainer (#2061). The Chamberlain Group. Available online: https://www.thecgroup.com/product/biliary-endoscopy-trainer-2061/ (accessed on 10 March 2021).
- Colonoscopy Trainer (#2003). The Chamberlain Group. Available online: https://www.thecgroup.com/product/colonoscopy-trainer-2003/ (accessed on 10 March 2021).
- Colon Endoscopy Trainer (#2041). The Chamberlain Group. Available online: https://www.thecgroup.com/product/colon-endoscopy-trainer-2041/ (accessed on 10 March 2021).
- Colon Endoscopy Trainer with Flat Polyps (#2201). The Chamberlain Group. Available online: https://www.thecgroup.com/product/colon-endoscopy-trainer-with-flat-polyps-2201/ (accessed on 10 March 2021).
- Colon Endoscopy Trainer with Raised Polyps (#2204). The Chamberlain Group. Available online: https://www.thecgroup.com/product/colon-endoscopy-trainer-with-raised-polyps-2204/ (accessed on 10 March 2021).
- Colonoscope Training Simulator. KYOTO KAGAKU. Available online: http://www.kyotokagaku.com/en/products_data/m40/ (accessed on 10 March 2021).
- 3D Colonoscope Training Simulator NKS. KYOTO KAGAKU. Available online: https://www.kyotokagaku.com/en/products_data/mw24/ (accessed on 10 March 2021).
- Colonoscopy (Lower GI Endoscopy) Simulator Type II LM-107: KOKEN CO.,LTD. Available online: https://www.kokenmpc.co.jp/english/products/life_simulation_models/medical_education/lm-107/index.html (accessed on 10 March 2021).
- EGD (EsophagoGastroDuodenoscopy) Simulator LM-103: KOKEN CO.,LTD. Available online: https://www.kokenmpc.co.jp/english/products/life_simulation_models/medical_education/lm-103/index.html (accessed on 10 March 2021).
- Noar, M.D. Robotics Interactive Endoscopy Simulation of ERCP/Sphincterotomy and EGD. In Endoscopy; Endoscopy: Thieme, Stuttgart, Germany, 1992; Volume 24, pp. 539–541. [Google Scholar] [CrossRef]
- Williams, C.B.; Baillie, J.; Gillies, D.F.; Borislow, D.; Cotton, P.B. Teaching Gastrointestinal Endoscopy by Computer Simulation: A Prototype for Colonoscopy and ERCP. Gastrointest. Endosc. 1990, 36, 49–54. [Google Scholar] [CrossRef]
- GI Mentor. Simbionix. Available online: https://simbionix.com/simulators/gi-mentor/ (accessed on 7 August 2020).
- EndoVR Endoscopy Training Simulator. CAE Healthcare. Available online: https://caehealthcare.com/surgical-simulation/endovr/ (accessed on 7 August 2020).
- EndoSim VR laparoscopic. EndoSim®. Surgical Science. Available online: https://surgicalscience.com/systems/endosim/?gclid=CjwKCAjw97P5BRBQEiwAGflV6YvrWL9WGSHmdOvKUTidTGsVugPUBzQ5Ov6DmXxl7E0RQKb_2Iq6XRoCnlMQAvD_BwE (accessed on 7 August 2020).
- MedVision. Available online: https://www.medvisiongroup.com/endovision.html (accessed on 7 August 2020).
- ENDO-X-MEDICAL-X-PDF Catalogs. Technical Documentation. Available online: https://pdf.medicalexpo.com/pdf/medical-x/endo-x/112986-160332.html (accessed on 10 March 2021).
- Simulators for Healthcare Training. Medical-X. Available online: https://medical-x.com/ (accessed on 10 March 2021).
- Haycock, A.; Koch, A.D.; Familiari, P.; van Delft, F.; Dekker, E.; Petruzziello, L.; Haringsma, J.; Thomas-Gibson, S. Training and Transfer of Colonoscopy Skills: A Multinational, Randomized, Blinded, Controlled Trial of Simulator versus Bedside Training. Gastrointest. Endosc. 2010, 71, 298–307. [Google Scholar] [CrossRef] [PubMed]
- GI Mentor Platforms. Simbionix. Available online: https://simbionix.com/simulators/gi-mentor/gi-mentor/ (accessed on 10 March 2021).
- Falkenstein, D.B.; Abrams, R.M.; Kessler, R.E.; Jones, B.; Johnson, G.; Zimmon, D.S. Endoscopic Retrograde Cholangiopancreatography in the Dog: A Model for Training and Research. Gastrointest. Endosc. 1974, 21, 25–26. [Google Scholar] [CrossRef]
- Matthes, K. Simulator Training in Endoscopic Hemostasis. Gastrointest. Endosc. Clin. North Am. 2006, 16, 511–527. [Google Scholar] [CrossRef]
- Hochberger, J.; Matthes, K.; Maiss, J.; Koebnick, C.; Hahn, E.G.; Cohen, J. Training with the CompactEASIE Biologic Endoscopy Simulator Significantly Improves Hemostatic Technical Skill of Gastroenterology Fellows: A Randomized Controlled Comparison with Clinical Endoscopy Training Alone. Gastrointest. Endosc. 2005, 61, 204–215. [Google Scholar] [CrossRef]
- Bhutani, M.S.; Hoffman, B.J.; Hawes, R.H. A Swine Model for Teaching Endoscopic Ultrasound (EUS) Imaging and Intervention under EUS Guidance. Endoscopy 1998, 30, 605–609. [Google Scholar] [CrossRef] [PubMed]
- Bhutani, M.S.; Aveyard, M.; Stills, H.F. Improved Model for Teaching Interventional EUS. Gastrointest. Endosc. 2000, 52, 400–403. [Google Scholar] [CrossRef]
- Bhutani, M.S.; Wong, R.F.; Hoffman, B.J. Training Facilities in Gastrointestinal Endoscopy: An Animal Model as an Aid to Learning Endoscopic Ultrasound. Endoscopy 2006, 38, 932–934. [Google Scholar] [CrossRef]
- Barthet, M.; Gasmil, M.; Boustiere, C.; Giovannini, M.; Grimaud, J.C.; Berdah, S. EUS Training in a Live Pig Model: Does It Improve Echo Endoscope Hands-on and Trainee Competence? Endoscopy 2007, 39, 535–539. [Google Scholar] [CrossRef]
- Gholson, C.F.; Provenza, J.M.; Doyle, J.T.; Bacon, B.R. Endoscopic Retrograde Sphincterotomy in Swine. Dig. Dis. Sci. 1991, 36, 1406–1409. [Google Scholar] [CrossRef]
- Gholson, C.F.; Mark Provenza, J.; Silver, R.C.; Bacon, B.R. Endoscopic Retrograde Cholangiography in the Swine: A New Model for Endoscopic Training and Hepatobiliary Research. Gastrointest. Endosc. 1990, 36, 600–603. [Google Scholar] [CrossRef]
- Parra-Blanco, A.; Arnau, M.R.; Nicolás-Pérez, D.; Gimeno-García, A.Z.; González, N.; Díaz-Acosta, J.A.; Jiménez, A.; Quintero, E. Endoscopic Submucosal Dissection Training with Pig Models in a Western Country. World J. Gastroenterol. 2010, 16, 2895–2900. [Google Scholar] [CrossRef]
- Vázquez-Sequeiros, E.; De Miquel, D.B.; Olcina, J.R.F.; Martín, J.A.G.; García, M.; Lucas, D.J.; Garrido, E.; González, C.; Blanco, A.P.; Arnau, M.R.; et al. Training Model for Teaching Endoscopic Submucosal Dissection of Gastric Tumors. Rev. Española Enferm. Dig. 2009, 101, 546–552. [Google Scholar] [CrossRef] [Green Version]
- Berr, F.; Ponchon, T.; Neureiter, D.; Kiesslich, T.; Haringsma, J.; Kaehler, G.F.; Schmoll, F.; Messmann, H.; Yahagi, N.; Oyama, T. Experimental Endoscopic Submucosal Dissection Training in a Porcine Model: Learning Experience of Skilled Western Endoscopists. Dig. Endosc. 2011, 23, 281–289. [Google Scholar] [CrossRef]
- Tanimoto, M.A.; Torres-Villalobos, G.; Fujita, R.; Santillan-Doherty, P.; Albores-Saavedra, J.; Gutierrez, G.; Martin-del-Campo, L.A.; Bravo-Reyna, C.; Villanueva, O.; Villalobos, J.J.; et al. Endoscopic Submucosal Dissection in Dogs in a World Gastroenterology Organisation Training Center. World J. Gastroenterol. 2010, 16, 1759–1764. [Google Scholar] [CrossRef]
- Tanaka, S.; Morita, Y.; Fujita, T.; Wakahara, C.; Ikeda, A.; Toyonaga, T.; Azuma, T. Ex Vivo Pig Training Model for Esophageal Endosopic Submucosal Dissection (ESD) for Endoscopists with Experience in Gastric ESD. Surg. Endosc. 2012, 26, 1579–1586. [Google Scholar] [CrossRef]
- Balekuduru, A.B.; Dutta, A.K.; Subbaraj, S.B. Endoscopy on a Human Cadaver: A Feasibility Study as a Training Tool. J. Dig. Endosc. 2018, 09, 103–108. [Google Scholar] [CrossRef] [Green Version]
- Mondragón, O.H.; Martínez, D.R.; Bautista, A.M.; Castañeda, M.A.; Blanco-Velasco, G.; Valencia, J.B. The Per Oral Endoscopic Myotomy (POEM) Technique: How Many Preclinical Procedures Are Needed to Master It? Endosc. Int. Open 2015, 03, E559–E565. [Google Scholar] [CrossRef] [Green Version]
- Perretta, S.; Dallemagne, B.; Marescaux, J. STEPS to POEM: Introduction of a New Technique at the IRCAD. Surg. Innov. 2012, 19, 216–220. [Google Scholar] [CrossRef]
- Telem, D.A.; Meireles, O.R.; Gee, D.W.; Sylla, P.; Brugge, W.R.; Rattner, D.W. Mo2074 Training for Per-Oral Endoscopic Myotomy (POEM): Cadavers or Swine? Gastroenterology 2012, 142, S-1088. [Google Scholar] [CrossRef]
- Porzionato, A.; Polese, L.; Lezoche, E.; Macchi, V.; Lezoche, G.; Da Dalt, G.; Stecco, C.; Norberto, L.; Merigliano, S.; De Caro, R. On the Suitability of Thiel Cadavers for Natural Orifice Transluminal Endoscopic Surgery (NOTES): Surgical Training, Feasibility Studies, and Anatomical Education. Surg. Endosc. 2015, 29, 737–746. [Google Scholar] [CrossRef] [PubMed]
- Noar, M.D. An Established Porcine Model for Animate Training in Diagnostic and Therapeutic ERCP. In Endoscopy; Georg Thieme: Stuttgart, Germany, 1995; Volume 27, pp. 77–80. [Google Scholar] [CrossRef]
- Siegel, J.H.; Korsten, M.A. ERCP in a Nonhuman Primate. Gastrointest. Endosc. 1989, 35, 557–559. [Google Scholar] [CrossRef]
- Fischer, J.; Zinner, D. Introduction to Special Issue: Frontiers in Baboon Research. J. Human Evol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Parra-Blanco, A.; González, N.; González, R.; Ortiz-Fernández-Sordo, J.; Ordieres, C. Animal Models for Endoscopic Training: Do We Really Need Them? Endoscopy 2013, 45, 478–484. [Google Scholar] [CrossRef] [PubMed]
- OIE. World Organisation for Animal Health. Available online: https://www.oie.int/ (accessed on 1 February 2021).
- Terrestrial Animal Health Code. OIE, 28th ed.; World Organisation for Animal Health: Paris, France, 2019. [Google Scholar]
- Directive 2010/63/eu of the European Parliament and of the Council of 22 September 2010 on the Protection of Animals Used for Scientific Purposes; in Official Journal of the European Union 2010; Publications Office of the European Union: Luxemburg, 22 September 2010; Volume 53. [CrossRef]
- Project Evaluation and Retrospective Assessment Directive 2010/63/eu on Protection of Animals Used for Scientific Purposes. Caring for Animals Aiming for Better Science; Publications Office of the European Union: Luxemburg, 2010.
- Clark, J.M. The 3Rs in Research: A Contemporary Approach to Replacement, Reduction and Refinement. Br. J. Nutr. 2018, 120 (Suppl. 1), S1–S7. [Google Scholar] [CrossRef]
- Erlangen Surgery and Endoscopy Training. Available online: http://www.endo-trainer.de/endotrainer/english/trainingszentrum.php (accessed on 28 September 2020).
- Hochberger, J.; Neumann, M.; Hohenberger, W.; Hahn, E. EASIE-Erlangen Education Simulation Model for Interventional Endoscopy--a New Bio-Training Model for Surgical Endoscopy. Biomed. Tech. Biomed. Eng. 1997, 42, 334. [Google Scholar] [CrossRef]
- Hochberger, J.; Neumann, M.; Hohenberger, W.; Gastroenterol, E.H.-Z. Neuer Endoskopie-Trainer Für Die Therapeutische Flexible Endoskopie. Z Gastroenterol 1997, 35, 722–723. [Google Scholar]
- Maiss, J.; Hildebrand, V.; Bayer, J.; Heute, E.H.-E. Mini-EASIE: Ein Neues, Auf Die Belange Der Interventionellen Endoskopie Reduziertes Trainingsmodell. Endosk. Heute 1999, 12, 53. [Google Scholar]
- Gastrointestinal Endoscopy Specimen Models and Simulators. EndoSim Evidence-Based Simulation. Available online: https://endosim.com/gastroenterology (accessed on 28 September 2020).
- Medicalinnovations. Speciality Medical Device Manufacturer and Commercialization Contractor Medical InnovationsTM Intl Inc. Available online: https://www.medicalinnovations.com/#products (accessed on 28 September 2020).
- Endoscopy Training Models. DeLegge Medical Design. Available online: https://www.deleggemedicaldesign.com/endoscopy-models (accessed on 28 September 2020).
- Ahn, J.Y.; Lee, J.S.; Lee, G.H.; Lee, J.W.; Na, H.K.; Jung, K.W.; Lee, J.H.; Kim, D.H.; Choi, K.D.; Song, H.J.; et al. The Efficacy of a Newly Designed, Easy-to-Manufacture Training Simulator for Endoscopic Biopsy of the Stomach. Gut Liver 2016, 10, 764–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, N.; Kunac, A.; Johnsen, E.; Gallina, G.; Merchant, A.M. Design and Validation of a Cost-Effective Physical Endoscopic Simulator for Fundamentals of Endoscopic Surgery Training. Surg. Endosc. 2016, 30, 4871–4879. [Google Scholar] [CrossRef] [PubMed]
- Walczak, D.A.; Grajek, M.; Walczak, P.A.; Tuliszka-Gołowkin, M.; Massopust, R.; Pawełczak, D.; Pasieka, Z.; Krakowczyk, Ł.; Maciejewski, A. The First Homemade Colonoscopy Trainer. Z. Gastroenterol. 2017, 55, 1004–1008. [Google Scholar] [CrossRef]
- Lee, S.; Ahn, J.Y.; Han, M.; Lee, G.H.; Na, H.K.; Jung, K.W.; Lee, J.H.; Kim, D.H.; Choi, K.D.; Song, H.J.; et al. Efficacy of a Three-Dimensional-Printed Training Simulator for Endoscopic Biopsy in the Stomach. Gut Liver 2018, 12, 149–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- 3D Slicer. Available online: https://www.slicer.org/ (accessed on 17 October 2020).
- Autodesk Meshmixer. Available online: https://www.meshmixer.com/ (accessed on 17 October 2020).
- Fujii, M.; Onoyama, T.; Ikebuchi, Y.; Uehara, K.; Koga, A.; Ueki, M.; Isomoto, H. A Novel Humanoid-Robot Simulator for Colonoscopy. Endoscopy 2020. [Google Scholar] [CrossRef]
- Kühl, C.; Dumont, G. Coloscopy Simulation: Towards Endoscopes Improve. Comput. Methods Biomech. Biomed. Eng. 2005, 8, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Yi, S.Y.; Woo, H.S.; Ahn, W.J.; Kwon, J.Y.; Lee, D.Y. New Colonoscopy Simulator with Improved Haptic Fidelity. Adv. Robot. 2006, 20, 349–365. [Google Scholar] [CrossRef]
- De Visser, H.; Passenger, J.; Conlan, D.; Russ, C.; Hellier, D.; Cheng, M.; Acosta, O.; Ourselin, S.; Salvado, O. Developing a Next Generation Colonoscopy Simulator. Int. J. Image Graph. 2010, 10, 203–217. [Google Scholar] [CrossRef]
- Chakravarthy, S.; Balakuntala, M.V.S.; Rao, A.M.; Thakur, R.K.; Ananthasuresh, G.K. Development of an Integrated Haptic System for Simulating Upper Gastrointestinal Endoscopy. Mechatronics 2018, 115–131. [Google Scholar] [CrossRef]
- Cheng, W.-B.; Di, Y.Y.; Zhang, E.M.; Moser, M.A.J.; Kanagaratnam, S.; Korman, L.Y.; Sarvazyan, N.; Zhang, W.J. Modeling and in Vitro Experimental Validation for Kinetics of the Colonoscope in Colonoscopy. Ann. Biomed. Eng. 2013, 41, 1084–1093. [Google Scholar] [CrossRef] [Green Version]
- Welch, C.R.; Reid, J.D. Looping Formation During Colonoscopy A Simulation. In Proceedings of the 14th International LS-Dyna Users Conference, Dearborn, MI, USA, 8–10 June 2014; pp. 1–12. [Google Scholar]
- Zupanc, C.M.; Wallis, G.M.; Hill, A.; Burgess-Limerick, R.; Riek, S.; Plooy, A.M.; Horswill, M.S.; Watson, M.O.; De Visser, H.; Conlan, D.; et al. Assessing Colonoscopic Inspection Skill Using a Virtual Withdrawal Simulation: A Preliminary Validation of Performance Metrics. BMC Med. Educ. 2017, 17, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riek, S.; Hill, A.; Plooy, A.M.; Horswill, M.S.; Cresp, A.S.G.; Marinovic, W.; Christofidis, M.J.; Burgess-Limerick, R.; Wallis, G.M.; Watson, M.O.; et al. A Novel Training Device for Tip Control in Colonoscopy: Preliminary Validation and Efficacy as a Training Tool. Surg. Endosc. 2017, 31, 5364–5371. [Google Scholar] [CrossRef] [Green Version]
- van der Wiel, S.; Koch, A.; Bruno, M. Face and Construct Validity of a Novel Mechanical ERCP Simulator. Endosc. Int. Open 2018, 6, E758–E765. [Google Scholar] [CrossRef] [Green Version]
- Walsh, C.M.; Cohen, J.; Woods, K.L.; Wang, K.K.; Andersen, D.K.; Anderson, M.A.; Dunkin, B.J.; Edmundowicz, S.A.; Faigel, D.O.; Law, J.K.; et al. ASGE EndoVators Summit: Simulators and the Future of Endoscopic Training. Gastrointest. Endosc. 2019, 90, 13–26. [Google Scholar] [CrossRef]
- Waschke, K.A. Will You Be My First Colonoscopy Patient? Planning Simulator Training for Novice Endoscopists. Gastrointest. Endosc. 2017, 890–891. [Google Scholar] [CrossRef] [Green Version]
- Goodman, A.J.; Melson, J.; Aslanian, H.R.; Bhutani, M.S.; Krishnan, K.; Lichtenstein, D.R.; Navaneethan, U.; Pannala, R.; Parsi, M.A.; Schulman, A.R.; et al. Endoscopic Simulators. Gastrointest. Endosc. 2019, 90, 1–12. [Google Scholar] [CrossRef]
- Singh, S.; Sedlack, R.E.; Cook, D.A. Effects of Simulation-Based Training in Gastrointestinal Endoscopy: A Systematic Review and Meta-Analysis. Clin. Gastroenterol. Hepatol. 2014, 1611–1623.e4. [Google Scholar] [CrossRef] [PubMed]
- Bittner, J.G., IV; Mellinger, J.D.; Imam, T.; Schade, R.R.; MacFadyen, B.V. Face and Construct Validity of a Computer-Based Virtual Reality Simulator for ERCP. Gastrointest. Endosc. 2010, 71, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Sedlack, R.E. Validation of Computer Simulation Training for Esophagogastroduodenoscopy: Pilot Study. J. Gastroenterol. Hepatol. 2007, 22, 1214–1219. [Google Scholar] [CrossRef]
- Childers, C.P.; Maggard-Gibbons, M. Understanding Costs of Care in the Operating Room. JAMA Surg. 2018, 153. [Google Scholar] [CrossRef] [PubMed]
- Asche, C.V.; Kim, M.; Brown, A.; Golden, A.; Laack, T.A.; Rosario, J.; Strother, C.; Totten, V.Y.; Okuda, Y. Communicating Value in Simulation: Cost-Benefit Analysis and Return on Investment. Acad. Emerg. Med. 2018, 25, 230–237. [Google Scholar] [CrossRef]
- Maloney, S.; Haines, T. Issues of Cost-Benefit and Cost-Effectiveness for Simulation in Health Professions Education. Adv. Simul. 2016, 1, 13. [Google Scholar] [CrossRef] [Green Version]
- Fletcher, J.D.; Wind, A.P. Cost Considerations in Using Simulations for Medical Training. Mil. Med. 2013, 37–46. [Google Scholar] [CrossRef] [Green Version]
- Faure, F.; Duriez, C.; Delingette, H.; Allard, J.; Gilles, B.; Marchesseau, S.; Talbot, H.; Courtecuisse, H.; Bousquet, G.; Peterlik, I.; et al. SOFA: A Multi-Model Framework for Interactive Physical Simulation in Soft Tissue Biomechanical Modeling for Computer Assisted Surgery Springer; Springer: Berlin/Heidelberg, Germany, 2012; Volume 11. [Google Scholar] [CrossRef] [Green Version]
- NVIDIA PhysX System Software. Available online: https://www.nvidia.com/en-us/drivers/physx/physx-9-19-0218-driver/ (accessed on 1 February 2021).
- Bullet Real-Time Physics Simulation. Home of Bullet and PyBullet: Physics Simulation for Games, Visual Effects, Robotics and Reinforcement Learning. Available online: https://pybullet.org/wordpress/ (accessed on 1 February 2021).
- OGRE—Open Source 3D Graphics Engine. Home of a Marvelous Rendering Engine. Available online: https://www.ogre3d.org/ (accessed on 1 February 2021).
- Unity Real-Time Development Platform. 3D, 2D VR & AR Engine. Available online: https://unity.com/ (accessed on 13 September 2020).
- Ho, C.N.; Schostek, S.; Kalanovic, D.S.M. Experimental Testbed for Measuring Forces during Gastrointestinal Endoscopy. Biomed. Tech. 2005, 50, 6. [Google Scholar]
- Verra, M.; Firrincieli, A.; Chiurazzi, M.; Mariani, A.; Lo Secco, G.; Forcignanò, E.; Koulaouzidis, A.; Menciassi, A.; Dario, P.; Ciuti, G.; et al. Robotic-Assisted Colonoscopy Platform with a Magnetically-Actuated Soft-Tethered Capsule. Cancers 2020, 12, 2485. [Google Scholar] [CrossRef]
- Crespo, J.; Carrillo, C.F.; Iruzubieta, P.; Hernández-Conde, M.; Rasines, L.; Jorquera, F.; Albillos, A.; Bañares, R.; Mora, P.; Vázquez, I.F.; et al. Massive Impact of Coronavirus Disease 2019 Pandemic on Gastroenterology and Hepatology Departments and Doctors in Spain. J. Gastroenterol. Hepatol. 2020. [Google Scholar] [CrossRef]
- Pawlak, K.M.; Kral, J.; Khan, R.; Amin, S.; Bilal, M.; Lui, R.N.; Sandhu, D.S.; Hashim, A.; Bollipo, S.; Charabaty, A.; et al. Impact of COVID-19 on Endoscopy Trainees: An International Survey. Gastrointest. Endosc. 2020, 92, 925–935. [Google Scholar] [CrossRef]
- Roemmele, C.; Manzeneder, J.; Messmann, H.; Ebigbo, A. Impact of the COVID-19 Outbreak on Endoscopy Training in a Tertiary Care Centre in Germany. Frontline Gastroenterol. 2020, 11, 454–457. [Google Scholar] [CrossRef] [PubMed]
- Siau, K.; Iacucci, M.; Dunckley, P.; Penman, I.; Pawlak, K.M.; Kral, J.; Khan, R.; Amin, S.; Bilal, M.; Lui, R.N.; et al. The Impact of COVID-19 on Gastrointestinal Endoscopy Training in the United Kingdom. Gastroenterology 2020, 1582–1585.e3. [Google Scholar] [CrossRef] [PubMed]
- Clough, J.; Fitzpatrick, M.; Harvey, P.; Morris, L. Shape of Training Review: An Impact Assessment for UK Gastroenterology Trainees. Frontline Gastroenterol. 2019, 10, 356–363. [Google Scholar] [CrossRef] [PubMed]
- Keswani, R.N.; Sethi, A.; Repici, A.; Messmann, H.; Chiu, P.W. How To Maximize Trainee Education During the Coronavirus Disease-2019 Pandemic: Perspectives From Around the World. Gastroenterology 2020, 159, 26–29. [Google Scholar] [CrossRef]
- Meara, J.G.; Leather, A.J.M.; Hagander, L.; Alkire, B.C.; Alonso, N.; Ameh, E.A.; Bickler, S.W.; Conteh, L.; Dare, A.J.; Davies, J.; et al. Global Surgery 2030: Evidence and Solutions for Achieving Health, Welfare, and Economic Development. Lancet 2015, 386, 569–624. [Google Scholar] [CrossRef]
- Dummer, T.J.B.; Cook, I.G. Health in China and India: A Cross-Country Comparison in a Context of Rapid Globalisation. Soc. Sci. Med. 2008, 67, 590–605. [Google Scholar] [CrossRef]
- Kopp, W. How Western Diet and Lifestyle Drive the Pandemic of Obesity and Civilization Diseases. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 2221–2236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mock, C.N.; Donkor, P.; Gawande, A.; Jamison, D.T.; Kruk, M.E.; Debas, H.T. Essential Surgery: Key Messages of This Volume. In Disease Control Priorities, Third Edition (Volume 1): Essential Surgery; The World Bank: Washington, DC, USA, 2015; Volume 18, pp. 1–18. [Google Scholar] [CrossRef]
- We Need a Moore’s Law for Medicine. MIT Technology Review. Available online: https://www.technologyreview.com/2013/09/03/15135/we-need-a-moores-law-for-medicine/ (accessed on 1 February 2021).
- Veneziano, D.; Ahmed, K.; Van Cleynenbreugel, B.; Gozen, A.; Palou, J.; Sarica, K.; Liatsikos, E.; Sanguedolce, F.; Honeck, P.; Alvarez-Maestro, M.; et al. Development Methodology of the Novel Endoscopic Stone Treatment Step 1 Training/Assessment Curriculum: An International Collaborative Work by European Association of Urology Sections. J. Endourol. 2017, 31, 934–941. [Google Scholar] [CrossRef]
- Veneziano, D.; Canova, A.; Arnolds, M.; Beatty, J.D.; Biyani, C.S.; Dehò, F.; Fiori, C.; Hellawell, G.O.; Langenhuijsen, J.F.; Pini, G.; et al. Performance Improvement (Pi) Score: An Algorithm to Score Pi Objectively during E-BLUS Hands-on Training Sessions. A European Association of Urology, Section of Uro-Technology (ESUT) Project. BJU Int. 2019, 123, 726–732. [Google Scholar] [CrossRef] [PubMed]
- Healey, P.; Samanta, J. When Does the “Learning Curve” of Innovative Interventions Become Questionable Practice? Eur. J. Vasc. Endovasc. Surg. 2008, 253–257. [Google Scholar] [CrossRef]
- Yule, S.; Flin, R.; Paterson-Brown, S.; Maran, N.; Rowley, D. Development of a Rating System for Surgeons’ Non-Technical Skills. Med. Educ. 2006, 40, 1098–1104. [Google Scholar] [CrossRef]
- Shih, J.J.; Krusienski, D.J.; Wolpaw, J.R. Brain-Computer Interfaces in Medicine. In Mayo Clinic Proceedings; Elsevier Ltd.: Amsterdam, The Netherlands, 2012; pp. 268–279. [Google Scholar] [CrossRef] [Green Version]
- Marlicz, W.; Ren, X.; Robertson, A.; Skonieczna-żydecka, K.; Łoniewski, I.; Dario, P.; Wang, S.; Plevris, J.N.; Koulaouzidis, A.; Ciuti, G. Frontiers of Robotic Gastroscopy: A Comprehensive Review of Robotic Gastroscopes and Technologies. Cancers 2020, 12, 2775. [Google Scholar] [CrossRef]
- Ciuti, G.; Skonieczna-Żydecka, K.; Marlicz, W.; Iacovacci, V.; Liu, H.; Stoyanov, D.; Arezzo, A.; Chiurazzi, M.; Toth, E.; Thorlacius, H.; et al. Frontiers of Robotic Colonoscopy: A Comprehensive Review of Robotic Colonoscopes and Technologies. J. Clin. Med. 2020, 9, 1648. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Simulators | Advantages | Disadvantages |
|---|---|---|
| Mechanical |
|
|
| Computerized |
|
|
| Ex-Vivo Model |
|
|
| In-Vivo Model |
|
|
| Type of Platform | Virtual Simulators | Mechanical Simulators | Ex-vivo Simulators | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Simulators | GI Mentor | CAE Endo VR | Endo-X | EndoSim | EndoVision | Endoscopic Trainer for the upper GI system Chamberlain Group | Biliary Endoscopy Trainer Chamberlain Group | Colonoscopy Trainer Chamberlain Group | EMS trainer Chamberlain Group | Colonoscope Training Simulator Kyoto Kagaku Co. | 3D Colonoscope Training Simulator NKS Kyoto Kagaku Co. | Colonoscopy Lower GI endoscopy simulator type II Koken Co. | EGD Simulator Koken Co. | EASIE-R4 EndoSim, | ColoEASIE-2 EndoSim, | Erlanger Endo-Trainer |
| Modules | ||||||||||||||||
| Upper GI endoscopy | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | x | x | ✓ | x | x | x | ✓ | ✓ | x | ✓ |
| Lower GI endoscopy | ✓ | ✓ | ✓ | ✓ | ✓ | x | x | ✓ | ✓ | ✓ | ✓ | ✓ | x | x | ✓ | ✓ |
| Non-anatomical environments | ✓ | x | x | x | ✓ | x | x | x | x | x | x | x | x | x | x | x |
| ERCP | ✓ | ✓ | x | ✓ | x | x | ✓ | x | x | x | x | x | ✓ | ✓ | x | ✓ |
| Flexible sigmoidoscopy | ✓ | ✓ | ✓ | x | x | x | x | x | x | x | x | x | x | x | ✓ | ✓ |
| EUS | ✓ | x | x | x | x | x | x | x | x | x | x | x | x | ✓ | x | ✓ |
| GI Bleeding | ✓ | ✓ | ✓ | x | ✓ | x | x | x | x | x | x | ✓ | ✓ | ✓ | ✓ | ✓ |
| EMR/ESD | ✓ | x | x | x | x | x | x | x | x | x | x | x | x | x | ✓ | ✓ |
| Polypectomy/Biopsy | ✓ | ✓ | ✓ | ✓ | ✓ | x | x | x | x | x | x | ✓ | ✓ | ✓ | ✓ | ✓ |
| Bronchoscopy | ✓ | ✓ | x | ✓ | ✓ | x | x | x | x | x | x | x | x | x | x | ✓ |
| Enteroscopy | x | x | x | x | x | x | x | x | x | x | x | ✓ | x | x | x | ✓ |
| Basic skills | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Key features | ||||||||||||||||
| Force feedback | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Intestinal looping | ✓ | x | x | ✓ | x | x | x | x | x | ✓ | ✓ | x | x | x | x | x |
| Multiple organs layout | ✓ | ✓ | ✓ | ✓ | ✓ | x | x | x | x | ✓ | ✓ | x | x | ✓ | x | ✓ |
| Replicas of polyps | ✓ | ✓ | ✓ | ✓ | ✓ | x | x | ✓ | ✓ | x | x | ✓ | ✓ | ✓ | ✓ | ✓ |
| Replicas of ulcers | ✓ | ✓ | ✓ | ✓ | ✓ | x | x | x | ✓ | x | x | x | ✓ | ✓ | ✓ | ✓ |
| Replicas of strictures | ✓ | ✓ | ✓ | ✓ | ✓ | x | ✓ | ✓ | ✓ | x | x | x | x | x | ✓ | ✓ |
| Suction/insufflation | ✓ | ✓ | ✓ | ✓ | ✓ | x | x | x | x | ✓ | ✓ | x | x | ✓ | ✓ | ✓ |
| Virtual patients’ cases | ✓ | ✓ | x | x | ✓ | x | x | x | x | x | x | x | x | x | x | x |
| Patient vitals measurements | ✓ | x | x | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Multiple body positions | ✓ | ✓ | ✓ | ✓ | ✓ | x | x | x | x | ✓ | ✓ | x | x | x | x | ✓ |
| Manual abdominal compression | n/a | n/a | n/a | n/a | n/a | x | x | x | x | ✓ | ✓ | x | x | x | x | x |
| Drugs management | ✓ | ✓ | ✓ | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Online tips | ✓ | ✓ | x | x | ✓ | x | x | x | x | x | x | x | x | x | x | x |
| 3D Map of the organ | ✓ | x | x | ✓ | ✓ | x | x | x | x | x | x | x | x | x | x | x |
| Recording the procedure | ✓ | x | x | ✓ | ✓ | x | x | x | x | x | x | x | x | x | x | x |
| Trainee feedback | ✓ | ✓ | ✓ | ✓ | ✓ | x | x | x | x | x | x | x | x | x | x | x |
| Issue to be Addressed | Possible Remarks in GI Endoscopic Training |
|---|---|
| Learning objectives | Hands-on practice of the most complex procedures in GI endoscopy, e.g., ESD, in the case no other simulation environments can correctly replicate the procedure. |
| Target group for the training activity | Advanced trainees (not beginners) |
| Purposes and needs of the procedures | Learn a specific endoscopic procedure, which cannot be practiced elsewhere (i.e., using other types of simulators) and that is too dangerous to perform on patients without previous experience. |
| The procedure is a single demonstration/trainee will directly participate | Trainees directly practice the procedure. |
| Justification of the in-vivo model respect to alternative models, by exploring other teaching methods highlighting the reasons of their unsuitability (e.g., comparing with experiments on human volunteers, video- and computer-based learning methods, and in vitro and ex-vivo studies) | Cases in which a realistic haptic feedback very close to the one experienced with human tissues and high visual rendering are paramount for correctly training the procedure. Therefore, even the most advanced simulators and ex-vivo models cannot replicate a scenario close enough to the real one. |
| When it is extremely important to practice, together with the technical procedure, drug administration, replicating all the conditions of the real clinical intervention: secretions, respiratory movements, and bleeding. However, advanced virtual and physical simulators now allow repetitive practice of the clinical tasks in highly realistic environments. | |
| Specify whether the procedure could be video recorded to avoid replicating the use of animals | Watching recorded procedures helps in learning the technique, although hands-on practice is preferred and usually paramount for acquiring technical skills. |
| Prior methodologies and approaches before applying in-vivo work | Watching recorded or live procedures performed by expert physicians. Test specific set of technical skills on simulators or ex-vivo models. |
| Reasons that avoid the learning objective to be fulfilled by observation of on-going research | Technical skills are hard to learn by only watching experts performing the specific tasks. Therefore, trainees usually need to acquire them directly on the field. |
| Justify the procedure in terms of severity if greater than mild | Before starting to simulate an endoscopic procedure, the animals are anesthetized and sacrificed at the end of the training. Although this protocol does not induce severe pain on the animals, refinement techniques should be always applied to minimize the suffering. |
| What feedback will be sought from the students on whether the educational objectives have been attained | Students will be able to perform the procedure on patients with a previous successful experience on animal models. However, similar experience can be gained by repetitive training the complex tasks on different types of simulators or ex-vivo models. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Finocchiaro, M.; Cortegoso Valdivia, P.; Hernansanz, A.; Marino, N.; Amram, D.; Casals, A.; Menciassi, A.; Marlicz, W.; Ciuti, G.; Koulaouzidis, A. Training Simulators for Gastrointestinal Endoscopy: Current and Future Perspectives. Cancers 2021, 13, 1427. https://doi.org/10.3390/cancers13061427
Finocchiaro M, Cortegoso Valdivia P, Hernansanz A, Marino N, Amram D, Casals A, Menciassi A, Marlicz W, Ciuti G, Koulaouzidis A. Training Simulators for Gastrointestinal Endoscopy: Current and Future Perspectives. Cancers. 2021; 13(6):1427. https://doi.org/10.3390/cancers13061427
Chicago/Turabian StyleFinocchiaro, Martina, Pablo Cortegoso Valdivia, Albert Hernansanz, Nicola Marino, Denise Amram, Alicia Casals, Arianna Menciassi, Wojciech Marlicz, Gastone Ciuti, and Anastasios Koulaouzidis. 2021. "Training Simulators for Gastrointestinal Endoscopy: Current and Future Perspectives" Cancers 13, no. 6: 1427. https://doi.org/10.3390/cancers13061427