
Shorter Leukocyte Telomere Length Is Associated with Worse Survival of Patients with Bladder Cancer and Renal Cell Carcinoma

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Blood Samples and Clinical Data
2.2. DNA Extraction
2.3. Determination of RTL by Quantitative Polymerase Chain Reaction (qPCR)
2.4. Statistical Analysis
3. Results
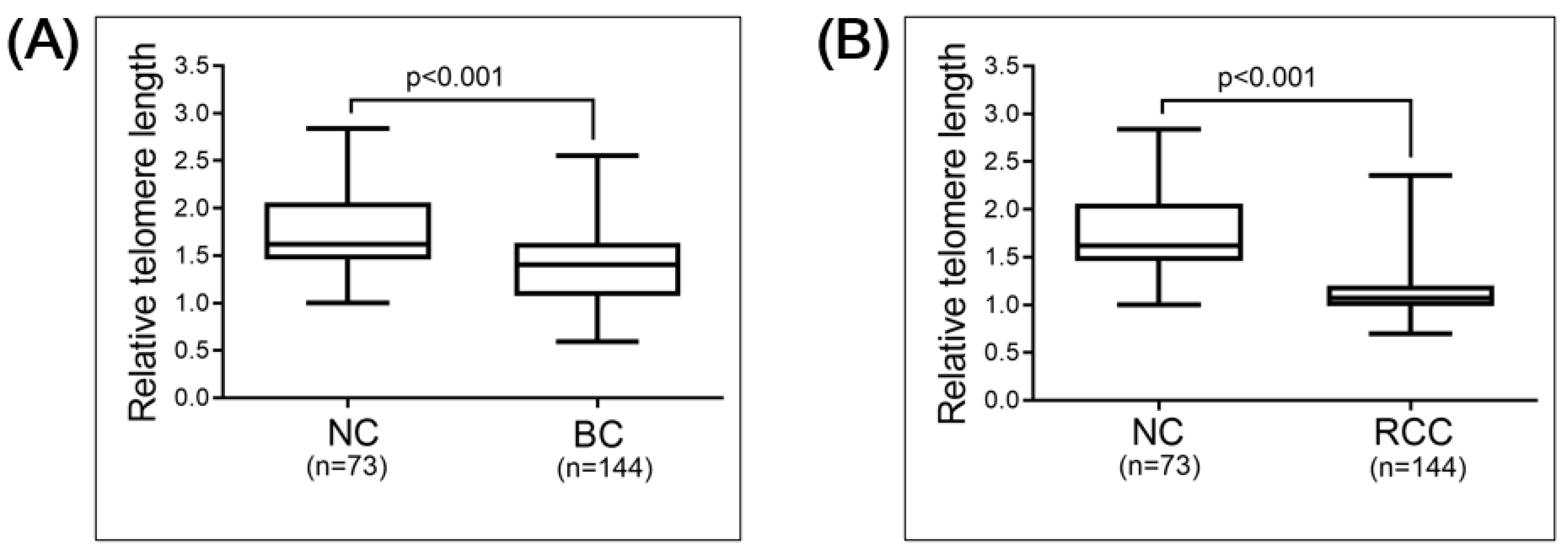
3.1. Basic Charactersristics of the Study Population and Group Comparison
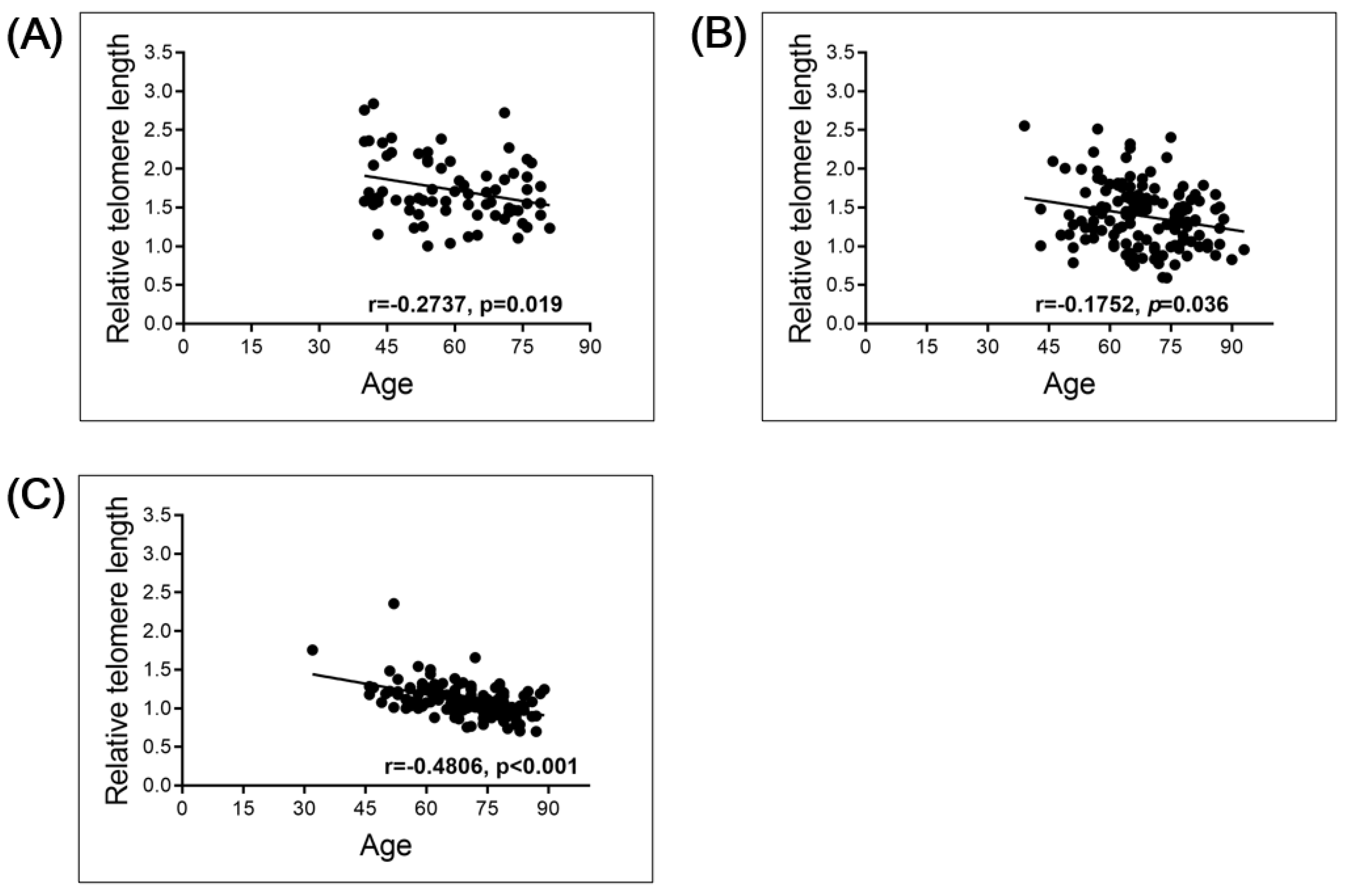
3.2. Correlation between RTL and Clinical Parameters in Cancer Patients
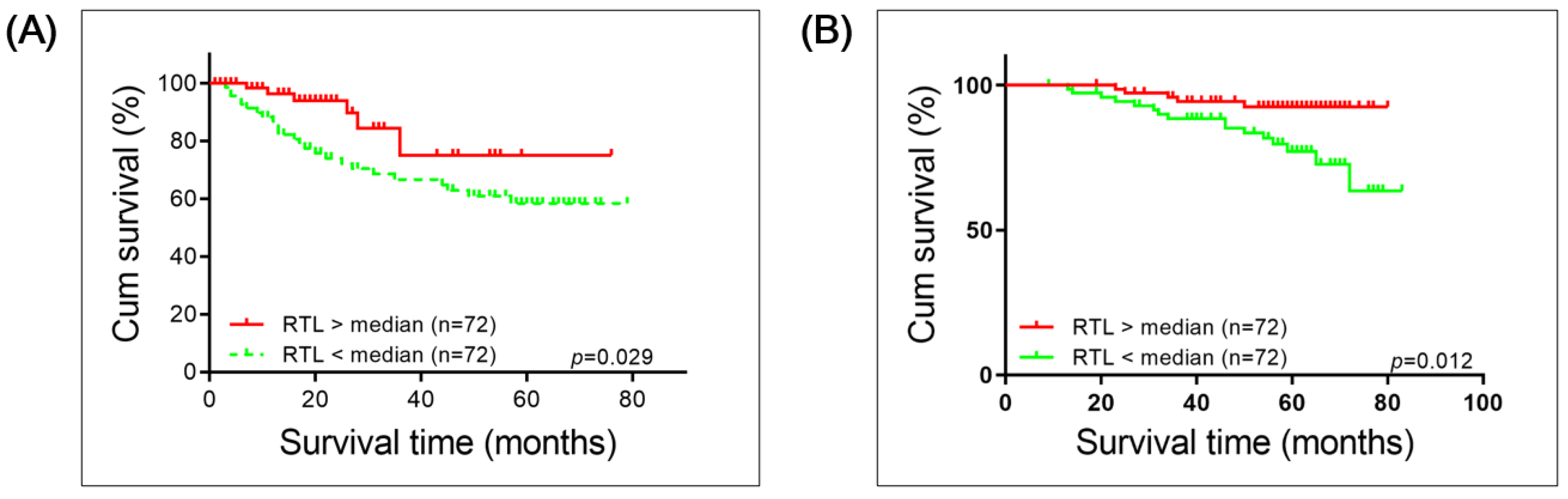
3.3. Correlation between PBL RTL and Overall Survival (OS) in Patients with BC and RCC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ljungberg, B.; Campbell, S.C.; Choi, H.Y.; Jacqmin, D.; Lee, J.E.; Weikert, S.; Kiemeney, L.A. The epidemiology of renal cell carcinoma. Eur. Urol. 2011, 60, 615–621. [Google Scholar] [CrossRef] [PubMed]
- Burger, M.; Catto, J.W.F.; Dalbagni, G.; Grossman, H.B.; Herr, H.; Karakiewicz, P.; Kassouf, W.; Kiemeney, L.A.; La Vecchia, C.; Shariat, S. Epidemiology and risk factors of urothelial bladder cancer. Eur. Urol. 2013, 63, 234–241. [Google Scholar] [CrossRef]
- Guzzo, T.J.; Magheli, A.; Bivalacqua, T.J.; Nielsen, M.E.; Attenello, F.J.; Schoenberg, M.P.; Gonzalgo, M.L. Pathological upstaging during radical cystectomy is associated with worse recurrence-free survival in patients with bacillus Calmette-Guerin-refractory bladder cancer. Urology 2009, 74, 1276–1280. [Google Scholar] [CrossRef] [PubMed]
- Stein, J.P.; Lieskovsky, G.; Cote, R.; Groshen, S.; Feng, A.-C.; Boyd, S.; Skinner, E.; Bochner, B.; Thangathurai, D.; Mikhail, M. Radical cystectomy in the treatment of invasive bladder cancer: Long-term results in 1,054 patients. J. Clin. Oncol. 2001, 19, 666–675. [Google Scholar] [CrossRef]
- Abdollah, F.; Gandaglia, G.; Thuret, R.; Schmitges, J.; Tian, Z.; Jeldres, C.; Passoni, N.M.; Briganti, A.; Shariat, S.F.; Perrotte, P. Incidence, survival and mortality rates of stage-specific bladder cancer in United States: A trend analysis. Cancer Epidemiol. 2013, 37, 219–225. [Google Scholar] [CrossRef]
- Meskawi, M.; Sun, M.; Trinh, Q.-D.; Bianchi, M.; Hansen, J.; Tian, Z.; Rink, M.; Ismail, S.; Shariat, S.F.; Montorsi, F. A review of integrated staging systems for renal cell carcinoma. Eur. Urol. 2012, 62, 303–314. [Google Scholar] [CrossRef]
- Wezel, F.; Vallo, S.; Roghmann, F. Do we have biomarkers to predict response to neoadjuvant and adjuvant chemotherapy and immunotherapy in bladder cancer? Transl. Androl. Urol. 2017, 6, 1067–1080. [Google Scholar] [CrossRef]
- Hedegaard, J.; Lamy, P.; Nordentoft, I.; Algaba, F.; Høyer, S.; Ulhøi, B.P.; Vang, S.; Reinert, T.; Hermann, G.G.; Mogensen, K.; et al. Comprehensive Transcriptional Analysis of Early-Stage Urothelial Carcinoma. Cancer Cell 2016, 30, 27–32. [Google Scholar] [CrossRef] [Green Version]
- Hussain, S.A.; Palmer, D.H.; Syn, W.K.; Sacco, J.J.; Greensmith, R.M.D.; Elmetwali, T.; Aachi, V.; Lloyd, B.H.; Jithesh, P.V.; Arrand, J.; et al. Gene expression profiling in bladder cancer identifies potential therapeutic targets. Int. J. Oncol. 2017, 50, 1147–1159. [Google Scholar] [CrossRef] [Green Version]
- Pietzak, E.J.; Bagrodia, A.; Cha, E.K.; Drill, E.N.; Iyer, G.; Isharwal, S.; Ostrovnaya, I.; Baez, P.; Li, Q.; Berger, M.F.; et al. Next-generation Sequencing of Nonmuscle Invasive Bladder Cancer Reveals Potential Biomarkers and Rational Therapeutic Targets. Eur. Urol. 2017, 72, 952–959. [Google Scholar] [CrossRef]
- Robertson, A.G.; Kim, J.; Al-Ahmadie, H.; Bellmunt, J.; Guo, G.; Cherniack, A.D.; Hinoue, T.; Laird, P.W.; Hoadley, K.A.; Akbani, R.; et al. Comprehensive Molecular Characterization of Muscle-Invasive Bladder Cancer. Cell 2017, 171, 540–556.e25. [Google Scholar] [CrossRef] [Green Version]
- Kandoth, C.; McLellan, M.D.; Vandin, F.; Ye, K.; Niu, B.; Lu, C.; Xie, M.; Zhang, Q.; McMichael, J.F.; Wyczalkowski, M.A.; et al. Mutational landscape and significance across 12 major cancer types. Nature 2013, 502, 333–339. [Google Scholar] [CrossRef] [Green Version]
- Cairns, P.; Shaw, M.E.; Knowles, M.A. Initiation of bladder cancer may involve deletion of a tumour-suppressor gene on chromosome 9. Oncogene 1993, 8, 1083–1085. [Google Scholar]
- van Oers, J.M.; Adam, C.; Denzinger, S.; Stoehr, R.; Bertz, S.; Zaak, D.; Stief, C.; Hofstaedter, F.; Zwarthoff, E.C.; van der Kwast, T.H.; et al. Chromosome 9 deletions are more frequent than FGFR3 mutations in flat urothelial hyperplasias of the bladder. Int. J. Cancer 2006, 119, 1212–1215. [Google Scholar] [CrossRef] [PubMed]
- Brunelli, M.; Eccher, A.; Gobbo, S.; Ficarra, V.; Novara, G.; Cossu-Rocca, P.; Bonetti, F.; Menestrina, F.; Cheng, L.; Eble, J.N.; et al. Loss of chromosome 9p is an independent prognostic factor in patients with clear cell renal cell carcinoma. Mod. Pathol. 2008, 21, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Di Nunno, V.; Mollica, V.; Brunelli, M.; Gatto, L.; Schiavina, R.; Fiorentino, M.; Santoni, M.; Montironi, R.; Calio, A.; Eccher, A.; et al. A Meta-Analysis Evaluating Clinical Outcomes of Patients with Renal Cell Carcinoma Harboring Chromosome 9P Loss. Mol. Diagn. Ther. 2019, 23, 569–577. [Google Scholar] [CrossRef]
- Rhodes, D.; Fairall, L.; Simonsson, T.; Chapman, L. Telomere architecture. EMBO Rep. 2002, 3, 1139–1145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, L.; Li, S.; Stohr, B.A. The role of telomere biology in cancer. Annu. Rev. Pathol. 2013, 8, 49–78. [Google Scholar] [CrossRef] [Green Version]
- Harley, C.B.; Futcher, A.B.; Greider, C.W. Telomeres shorten during ageing of human fibroblasts. Nature 1990, 345, 458–460. [Google Scholar] [CrossRef]
- De Lange, T.; Shiue, L.; Myers, R.M.; Cox, D.R.; Naylor, S.L.; Killery, A.M.; Varmus, H.E. Structure and variability of human chromosome ends. Mol. Cell. Biol. 1990, 10, 518–527. [Google Scholar] [CrossRef] [Green Version]
- Levy, M.Z.; Allsopp, R.C.; Futcher, A.B.; Greider, C.W.; Harley, C.B. Telomere end-replication problem and cell aging. J. Mol. Biol. 1992, 225, 951–960. [Google Scholar] [CrossRef]
- Ritz, J.M.; Kühle, O.; Riethdorf, S.; Sipos, B.; Deppert, W.; Englert, C.; Günes, C. A novel transgenic mouse model reveals humanlike regulation of an 8-kbp human TERT gene promoter fragment in normal and tumor tissues. Cancer Res. 2005, 65, 1187–1196. [Google Scholar] [CrossRef] [Green Version]
- Kim, N.W.; Piatyszek, M.A.; Prowse, K.R.; Harley, C.B.; West, M.D.; Ho, P.L.; Coviello, G.M.; Wright, W.E.; Weinrich, S.L.; Shay, J.W. Specific association of human telomerase activity with immortal cells and cancer. Science 1994, 266, 2011–2015. [Google Scholar] [CrossRef]
- Günes, C.; Wezel, F.; Southgate, J.; Bolenz, C. Implications of TERT promoter mutations and telomerase activity in urothelial carcinogenesis. Nat. Rev. Urol. 2018, 15, 386–393. [Google Scholar] [CrossRef] [Green Version]
- Grabowski, P.; Hultdin, M.; Karlsson, K.; Tobin, G.; Aleskog, A.; Thunberg, U.; Laurell, A.; Sundström, C.; Rosenquist, R.; Roos, G. Telomere length as a prognostic parameter in chronic lymphocytic leukemia with special reference to VH gene mutation status. Blood 2005, 105, 4807–4812. [Google Scholar] [CrossRef] [Green Version]
- Nagpal, N.; Agarwal, S. Telomerase RNA processing: Implications for human health and disease. Stem Cells 2020, 38, 1532–1543. [Google Scholar] [CrossRef] [PubMed]
- Mehle, C.; Piatyszek, M.A.; Ljungberg, B.; Shay, J.W.; Roos, G. Telomerase activity in human renal cell carcinoma. Oncogene 1996, 13, 161–166. [Google Scholar] [PubMed]
- Sugimura, K.; Yoshida, N.; Hisatomi, H.; Nakatani, T.; Ikemoto, S. Telomerase activity in human renal cell carcinoma. BJU Int. 1999, 83, 693–697. [Google Scholar] [CrossRef]
- Kanaya, T.; Kyo, S.; Takakura, M.; Ito, H.; Namiki, M.; Inoue, M. hTERT is a critical determinant of telomerase activity in renal-cell carcinoma. Int. J. Cancer 1998, 78, 539–543. [Google Scholar] [CrossRef]
- Vinagre, J.; Almeida, A.; Pópulo, H.; Batista, R.; Lyra, J.; Pinto, V.; Coelho, R.; Celestino, R.; Prazeres, H.; Lima, L.; et al. Frequency of TERT promoter mutations in human cancers. Nat. Commun. 2013, 4, 2815. [Google Scholar] [CrossRef] [Green Version]
- Allory, Y.; Beukers, W.; Sagrera, A.; Flández, M.; Marqués, M.; Márquez, M.; van der Keur, K.A.; Dyrskjot, L.; Lurkin, I.; Vermeij, M.; et al. Telomerase reverse transcriptase promoter mutations in bladder cancer: High frequency across stages, detection in urine, and lack of association with outcome. Eur. Urol. 2014, 65, 360–366. [Google Scholar] [CrossRef] [Green Version]
- Kumar, M.; Lechel, A.; Güneş, Ç. Telomerase: The devil inside. Genes 2016, 7, 43. [Google Scholar] [CrossRef] [Green Version]
- Weise, J.M.; Günes, C. Telomeres and telomerase. A survey about methods and recent advances in cancer diagnostic and therapy. Histol. Histopathol. 2006, 21, 1249–1261. [Google Scholar] [CrossRef]
- Artandi, S.E.; Chang, S.; Lee, S.L.; Alson, S.; Gottlieb, G.J.; Chin, L.; DePinho, R.A. Telomere dysfunction promotes non-reciprocal translocations and epithelial cancers in mice. Nature 2000, 406, 641–645. [Google Scholar] [CrossRef] [PubMed]
- Chin, L.; Artandi, S.E.; Shen, Q.; Tam, A.; Lee, S.L.; Gottlieb, G.J.; Greider, C.W.; DePinho, R.A. p53 deficiency rescues the adverse effects of telomere loss and cooperates with telomere dysfunction to accelerate carcinogenesis. Cell 1999, 97, 527–538. [Google Scholar] [CrossRef] [Green Version]
- Roake, C.M.; Artandi, S.E. Telomere-lengthening mechanism revealed. Nature 2016, 539, 35–36. [Google Scholar] [CrossRef] [Green Version]
- Allsopp, R.C.; Chang, E.; Kashefi-Aazam, M.; Rogaev, E.I.; Piatyszek, M.A.; Shay, J.W.; Harley, C.B. Telomere shortening is associated with cell division in vitro and in vivo. Exp. Cell Res. 1995, 220, 194–200. [Google Scholar] [CrossRef]
- Harley, C.B. Telomere loss: Mitotic clock or genetic time bomb? Mutat. Res. 1991, 256, 271–282. [Google Scholar] [CrossRef]
- Lindsey, J.; McGill, N.I.; Lindsey, L.A.; Green, D.K.; Cooke, H.J. In vivo loss of telomeric repeats with age in humans. Mutat. Res. 1991, 256, 45–48. [Google Scholar] [CrossRef]
- Shin, J.S.; Hong, A.; Solomon, M.J.; Lee, C.S. The role of telomeres and telomerase in the pathology of human cancer and aging. Pathology 2006, 38, 103–113. [Google Scholar] [CrossRef]
- Alter, B.P.; Giri, N.; Savage, S.A.; Rosenberg, P.S. Cancer in dyskeratosis congenita. Blood 2009, 113, 6549–6557. [Google Scholar] [CrossRef] [Green Version]
- Hartmann, D.; Srivastava, U.; Thaler, M.; Kleinhans, K.N.; N’kontchou, G.; Scheffold, A.; Bauer, K.; Kratzer, R.F.; Kloos, N.; Katz, S.F.; et al. Telomerase gene mutations are associated with cirrhosis formation. Hepatology 2011, 53, 1608–1617. [Google Scholar] [CrossRef] [Green Version]
- Savage, S.A.; Alter, B.P. Dyskeratosis congenita. Hematol. Oncol. Clin. N. Am. 2009, 23, 215–231. [Google Scholar] [CrossRef]
- Vulliamy, T.J.; Dokal, I. Dyskeratosis congenita: The diverse clinical presentation of mutations in the telomerase complex. Biochimie 2008, 90, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Walne, A.J.; Dokal, I. Dyskeratosis Congenita: A historical perspective. Mech. Ageing Dev. 2008, 129, 48–59. [Google Scholar] [CrossRef]
- Meeker, A.K.; Hicks, J.L.; Iacobuzio-Donahue, C.A.; Montgomery, E.A.; Westra, W.H.; Chan, T.Y.; Ronnett, B.M.; De Marzo, A.M. Telomere length abnormalities occur early in the initiation of epithelial carcinogenesis. Clin. Cancer Res. 2004, 10, 3317–3326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morton, M.J.; Zhang, S.; Lopez-Beltran, A.; MacLennan, G.T.; Eble, J.N.; Montironi, R.; Sung, M.T.; Tan, P.H.; Zheng, S.; Zhou, H.; et al. Telomere shortening and chromosomal abnormalities in intestinal metaplasia of the urinary bladder. Clin. Cancer Res. 2007, 13, 6232–6236. [Google Scholar] [CrossRef] [Green Version]
- Pal, D.; Sharma, U.; Khajuria, R.; Singh, S.K.; Kakkar, N.; Prasad, R. Augmented telomerase activity, reduced telomere length and the presence of alternative lengthening of telomere in renal cell carcinoma: Plausible predictive and diagnostic markers. Gene 2015, 562, 145–151. [Google Scholar] [CrossRef]
- Fiedler, W.; Dahse, R.; Schlichter, A.; Junker, K.; Kosmehl, H.; Ernst, G.; Schubert, J.; Claussen, U. Telomerase activity and telomere length in different areas of renal cell carcinoma. Int. J. Oncol. 1996, 9, 1227–1232. [Google Scholar] [CrossRef]
- Dahse, R.; Fiedler, W.; Junker, K.; Schlichter, A.; Schubert, J.; Claussen, U. Telomerase activity and telomere lengths: Alterations in renal cell carcinomas. Kidney Int. 1999, 56, 1289–1290. [Google Scholar] [CrossRef] [Green Version]
- Wentzensen, I.M.; Mirabello, L.; Pfeiffer, R.M.; Savage, S.A. The association of telomere length and cancer: A meta-analysis. Cancer Epidemiol. Biomarkers Prev. 2011, 20, 1238–1250. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Zhao, Q.; Zhu, W.; Liu, T.; Xie, S.-H.; Zhong, L.-X.; Cai, Y.-Y.; Li, X.-N.; Liang, M.; Chen, W. The association of telomere length in peripheral blood cells with cancer risk: A systematic review and meta-analysis of prospective studies. Cancer Epidemiol. Prev. Biomark. 2017, 26, 1381–1390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, J.; Zhu, X.; Xie, C.; Dai, N.; Gu, Y.; Zhu, M.; Wang, C.; Gao, Y.; Pan, F.; Ren, C.; et al. Telomere length, genetic variants and gastric cancer risk in a Chinese population. Carcinogenesis 2015, 36, 963–970. [Google Scholar] [CrossRef] [Green Version]
- Machiela, M.J.; Hsiung, C.A.; Shu, X.O.; Seow, W.J.; Wang, Z.; Matsuo, K.; Hong, Y.C.; Seow, A.; Wu, C.; Hosgood, H.D., 3rd; et al. G enetic variants associated with longer telomere length are associated with increased lung cancer risk among never-smoking women in Asia: A report from the female lung cancer consortium in Asia. Int. J. Cancer 2015, 137, 311–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rode, L.; Nordestgaard, B.G.; Bojesen, S.E. Peripheral blood leukocyte telomere length and mortality among 64 637 individuals from the general population. J. Natl. Cancer Inst. 2015, 107, djv074. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collaboration, T.M.R.; Haycock, P.C.; Burgess, S.; Nounu, A.; Zheng, J.; Okoli, G.N.; Bowden, J.; Wade, K.H.; Timpson, N.J.; Evans, D.M.; et al. Association between telomere length and risk of cancer and non-neoplastic diseases: A Mendelian randomization study. JAMA Oncol. 2017, 3, 636–651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Svenson, U.; Nordfjäll, K.; Stegmayr, B.; Manjer, J.; Nilsson, P.; Tavelin, B.; Henriksson, R.; Lenner, P.; Roos, G. Breast cancer survival is associated with telomere length in peripheral blood cells. Cancer Res. 2008, 68, 3618–3623. [Google Scholar] [CrossRef] [Green Version]
- Svenson, U.; Ljungberg, B.; Roos, G. Telomere length in peripheral blood predicts survival in clear cell renal cell carcinoma. Cancer Res. 2009, 69, 2896–2901. [Google Scholar] [CrossRef] [Green Version]
- Svenson, U.; Roos, G.; Wikström, P. Long leukocyte telomere length in prostate cancer patients at diagnosis is associated with poor metastasis-free and cancer-specific survival. Tumor Biol 2017, 39, 1010428317692236. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.Q.; An, J.Z.; Liu, J.; Yang, Y.F.; Zhang, H.X.; Zhao, B.Y.; Li, J.B.; Yang, H.S.; Chen, Z.N.; Xing, J.L. Leukocyte telomere length predicts overall survival in hepatocellular carcinoma treated with transarterial chemoembolization. Carcinogenesis 2012, 33, 1040–1045. [Google Scholar] [CrossRef]
- Russo, A.; Modica, F.; Guarrera, S.; Fiorito, G.; Pardini, B.; Viberti, C.; Allione, A.; Critelli, R.; Bosio, A.; Casetta, G.; et al. Shorter leukocyte telomere length is independently associated with poor survival in patients with bladder cancer. Cancer Epidemiol Biomarkers Prev. 2014, 23, 2439–2446. [Google Scholar] [CrossRef] [Green Version]
- Qu, F.; Li, R.; He, X.; Li, Q.; Xie, S.; Gong, L.; Ji, G.; Lu, J.; Bao, G. Short telomere length in peripheral blood leukocyte predicts poor prognosis and indicates an immunosuppressive phenotype in gastric cancer patients. Mol. Oncol. 2015, 9, 727–739. [Google Scholar] [CrossRef]
- Jia, H.; Wang, Z. Telomere length as a prognostic factor for overall survival in colorectal cancer patients. Cell. Physiol. Biochem. 2016, 38, 122–128. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Qu, F.; He, X.; Bao, G.; Liu, X.; Wan, S.; Xing, J. Short leukocyte telomere length predicts poor prognosis and indicates altered immune functions in colorectal cancer patients. Ann. Oncol. 2014, 25, 869–876. [Google Scholar] [CrossRef]
- Shanta, K.; Nakayama, K.; Ishikawa, M.; Ishibashi, T.; Yamashita, H.; Sato, S.; Sasamori, H.; Sawada, K.; Kurose, S.; Mahmud, H.M.; et al. Prognostic Value of Peripheral Blood Lymphocyte Telomere Length in Gynecologic Malignant Tumors. Cancers 2020, 12, 1469. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Wang, Y.; Kota, K.K.; Kallakury, B.; Mikhail, N.N.; Sayed, D.; Mokhtar, A.; Maximous, D.; Yassin, E.H.; Gouda, I.; et al. Strong association between long and heterogeneous telomere length in blood lymphocytes and bladder cancer risk in Egyptian. Carcinogenesis 2015, 36, 1284–1290. [Google Scholar] [CrossRef] [Green Version]
- McGrath, M.; Wong, J.Y.; Michaud, D.; Hunter, D.J.; De Vivo, I. Telomere length, cigarette smoking, and bladder cancer risk in men and women. Cancer Epidemiol Biomarkers Prev. 2007, 16, 815–819. [Google Scholar] [CrossRef] [Green Version]
- Shao, L.; Wood, C.G.; Zhang, D.; Tannir, N.M.; Matin, S.; Dinney, C.P.; Wu, X. Telomere dysfunction in peripheral lymphocytes as a potential predisposition factor for renal cancer. J. Urol. 2007, 178, 1492–1496. [Google Scholar] [CrossRef]
- Machiela, M.J.; Hofmann, J.N.; Carreras-Torres, R.; Brown, K.M.; Johansson, M.; Wang, Z.; Foll, M.; Li, P.; Rothman, N.; Savage, S.A.; et al. Genetic Variants Related to Longer Telomere Length are Associated with Increased Risk of Renal Cell Carcinoma. Eur. Urol. 2017, 72, 747–754. [Google Scholar] [CrossRef]
- Callahan, C.L.; Schwartz, K.; Ruterbusch, J.J.; Shuch, B.; Graubard, B.I.; Lan, Q.; Cawthon, R.; Baccarelli, A.A.; Chow, W.H.; Rothman, N.; et al. Leukocyte telomere length and renal cell carcinoma survival in two studies. Br. J. Cancer 2017, 117, 752–755. [Google Scholar] [CrossRef]
- O’Callaghan, N.J.; Fenech, M. A quantitative PCR method for measuring absolute telomere length. Biol. Proced. Online 2011, 13, 3. [Google Scholar] [CrossRef] [Green Version]
- Cawthon, R.M. Telomere measurement by quantitative PCR. Nucleic Acids Res. 2002, 30, e47. [Google Scholar] [CrossRef]
- Meena, J.K.; Cerutti, A.; Beichler, C.; Morita, Y.; Bruhn, C.; Kumar, M.; Kraus, J.M.; Speicher, M.R.; Wang, Z.Q.; Kestler, H.A.; et al. Telomerase abrogates aneuploidy-induced telomere replication stress, senescence and cell depletion. EMBO J. 2015, 34, 1371–1384. [Google Scholar] [CrossRef] [Green Version]
- Ma, H.; Zhou, Z.; Wei, S.; Liu, Z.; Pooley, K.A.; Dunning, A.M.; Svenson, U.; Roos, G.; Hosgood, H.D., 3rd; Shen, M.; et al. Shortened telomere length is associated with increased risk of cancer: A meta-analysis. PLoS ONE 2011, 6, e20466. [Google Scholar] [CrossRef]
- Gao, Y.; Wei, Y.; Zhou, X.; Huang, S.; Zhao, H.; Zeng, P. Assessing the Relationship Between Leukocyte Telomere Length and Cancer Risk/Mortality in UK Biobank and TCGA Datasets With the Genetic Risk Score and Mendelian Randomization Approaches. Front. Genet. 2020, 11, 583106. [Google Scholar] [CrossRef]
- Xu, Y.; Xu, J.; Chancoco, H.; Huang, M.; Torres, K.E.; Gu, J. Long Leukocyte Telomere Length Is Associated with Increased Risks of Soft Tissue Sarcoma: A Mendelian Randomization Study. Cancers 2020, 12, 594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luu, H.N.; Qi, M.; Wang, R.; Adams-Haduch, J.; Miljkovic, I.; Opresko, P.L.; Jin, A.; Koh, W.P.; Yuan, J.M. Association Between Leukocyte Telomere Length and Colorectal Cancer Risk in the Singapore Chinese Health Study. Clin. Transl. Gastroenterol. 2019, 10, 1–9. [Google Scholar] [CrossRef]
- Luu, H.N.; Huang, J.Y.; Wang, R.; Adams-Haduch, J.; Jin, A.; Koh, W.P.; Yuan, J.M. Association between leukocyte telomere length and the risk of pancreatic cancer: Findings from a prospective study. PLoS ONE 2019, 14, e0221697. [Google Scholar] [CrossRef] [Green Version]
- Samavat, H.; Xun, X.; Jin, A.; Wang, R.; Koh, W.P.; Yuan, J.M. Association between prediagnostic leukocyte telomere length and breast cancer risk: The Singapore Chinese Health Study. Breast Cancer Res. 2019, 21, 50. [Google Scholar] [CrossRef]
- Samavat, H.; Luu, H.N.; Beckman, K.B.; Jin, A.; Wang, R.; Koh, W.P.; Yuan, J.M. Leukocyte telomere length, cancer incidence and all-cause mortality among Chinese adults: Singapore Chinese Health Study. Int. J. Cancer 2021, 148, 352–362. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Koh, W.P.; Jin, A.; Wang, R.; Yuan, J.M. Telomere length and risk of developing gastric adenocarcinoma: The Singapore Chinese Health Study. Gastric Cancer 2018, 21, 598–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weischer, M.; Nordestgaard, B.G.; Cawthon, R.M.; Freiberg, J.J.; Tybjaerg-Hansen, A.; Bojesen, S.E. Short telomere length, cancer survival, and cancer risk in 47102 individuals. J. Natl. Cancer Inst. 2013, 105, 459–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, M.; Tsai, C.W.; Chang, W.S.; Xu, J.; Xu, Y.; Bau, D.T.; Gu, J. Prognostic value of leukocyte telomere length in renal cell carcinoma patients. Am. J. Cancer Res. 2020, 10, 3428–3439. [Google Scholar]
- Morais, M.; Dias, F.; Teixeira, A.L.; Medeiros, R. Telomere Length in Renal Cell Carcinoma: The Jekyll and Hyde Biomarker of Ageing of the Kidney. Cancer Manag. Res. 2020, 12, 1669–1679. [Google Scholar] [CrossRef] [Green Version]
- Benitez-Buelga, C.; Sanchez-Barroso, L.; Gallardo, M.; Apellániz-Ruiz, M.; Inglada-Perez, L.; Yanowski, K.; Carrillo, J.; Garcia-Estevez, L.; Calvo, I.; Perona, R. Impact of chemotherapy on telomere length in sporadic and familial breast cancer patients. Breast Cancer Res. Treat. 2015, 149, 385–394. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.J.; Nam, C.E.; Cho, S.H.; Park, K.S.; Chung, I.J.; Kim, H.J. Telomere length shortening in non-Hodgkin’s lymphoma patients undergoing chemotherapy. Ann. Hematol. 2003, 82, 492–495. [Google Scholar] [CrossRef]
- Szyper-Kravitz, M.; Uziel, O.; Shapiro, H.; Radnay, J.; Katz, T.; Rowe, J.M.; Lishner, M.; Lahav, M. Granulocyte colony-stimulating factor administration upregulates telomerase activity in CD34+ haematopoietic cells and may prevent telomere attrition after chemotherapy. Br. J. Haematol. 2003, 120, 329–336. [Google Scholar] [CrossRef]
- Unryn, B.M.; Hao, D.; Glück, S.; Riabowol, K.T. Acceleration of telomere loss by chemotherapy is greater in older patients with locally advanced head and neck cancer. Clin. Cancer Res. 2006, 12, 6345–6350. [Google Scholar] [CrossRef] [Green Version]
- Effros, R.B. Telomere/telomerase dynamics within the human immune system: Effect of chronic infection and stress. Exp. Gerontol. 2011, 46, 135–140. [Google Scholar] [CrossRef] [Green Version]
- Epel, E.S.; Blackburn, E.H.; Lin, J.; Dhabhar, F.S.; Adler, N.E.; Morrow, J.D.; Cawthon, R.M. Accelerated telomere shortening in response to life stress. Proc. Natl. Acad. Sci. USA 2004, 101, 17312–17315. [Google Scholar] [CrossRef] [Green Version]
- Valdes, A.M.; Andrew, T.; Gardner, J.P.; Kimura, M.; Oelsner, E.; Cherkas, L.F.; Aviv, A.; Spector, T.D. Obesity, cigarette smoking, and telomere length in women. Lancet 2005, 366, 662–664. [Google Scholar] [CrossRef]
- Cherkas, L.F.; Aviv, A.; Valdes, A.M.; Hunkin, J.L.; Gardner, J.P.; Surdulescu, G.L.; Kimura, M.; Spector, T.D. The effects of social status on biological aging as measured by white-blood-cell telomere length. Aging Cell 2006, 5, 361–365. [Google Scholar] [CrossRef] [PubMed]
- Freedman, N.D.; Silverman, D.T.; Hollenbeck, A.R.; Schatzkin, A.; Abnet, C.C. Association between smoking and risk of bladder cancer among men and women. JAMA 2011, 306, 737–745. [Google Scholar] [CrossRef]
- Hunt, J.D.; van der Hel, O.L.; McMillan, G.P.; Boffetta, P.; Brennan, P. Renal cell carcinoma in relation to cigarette smoking: Meta-analysis of 24 studies. Int. J. Cancer 2005, 114, 101–108. [Google Scholar] [CrossRef]
- Frenck, R.W., Jr.; Blackburn, E.H.; Shannon, K.M. The rate of telomere sequence loss in human leukocytes varies with age. Proc. Natl. Acad. Sci. USA 1998, 95, 5607–5610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slagboom, P.E.; Droog, S.; Boomsma, D.I. Genetic determination of telomere size in humans: A twin study of three age groups. Am. J. Hum. Genet. 1994, 55, 876–882. [Google Scholar]
- Bischoff, C.; Graakjaer, J.; Petersen, H.C.; Jeune, B.; Bohr, V.A.; Koelvraa, S.; Christensen, K. Telomere length among the elderly and oldest-old. Twin Res. Hum. Genet. 2005, 8, 425–432. [Google Scholar] [CrossRef]
- Li, H.; Xu, D.; Li, J.; Berndt, M.C.; Liu, J.P. Transforming growth factor beta suppresses human telomerase reverse transcriptase (hTERT) by Smad3 interactions with c-Myc and the hTERT gene. J. Biol. Chem. 2006, 281, 25588–25600. [Google Scholar] [CrossRef] [Green Version]
- Brazvan, B.; Farahzadi, R.; Mohammadi, S.M.; Saheb, S.M.; Shanehbandi, D.; Schmied, L.; Rad, J.S.; Darabi, M.; Charoudeh, H.N. Key Immune Cell Cytokines Affects the Telomere Activity of Cord Blood Cells In vitro. Adv. Pharm. Bull. 2016, 6, 153–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robles-Espinoza, C.D.; Harland, M.; Ramsay, A.J.; Aoude, L.G.; Quesada, V.; Ding, Z.; Pooley, K.A.; Pritchard, A.L.; Tiffen, J.C.; Petljak, M.; et al. POT1 loss-of-function variants predispose to familial melanoma. Nat. Genet. 2014, 46, 478–481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, J.; Yang, X.R.; Ballew, B.; Rotunno, M.; Calista, D.; Fargnoli, M.C.; Ghiorzo, P.; de Paillerets, B.B.; Nagore, E.; Avril, M.F.; et al. Rare missense variants in POT1 predispose to familial cutaneous malignant melanoma. Nat. Genet. 2014, 46, 482–486. [Google Scholar] [CrossRef] [PubMed]
- Gunes, C.; Avila, A.I.; Rudolph, K.L. Telomeres in cancer. Differentiation 2017, 99, 41–50. [Google Scholar] [CrossRef]
- Bojesen, S.E.; Pooley, K.A.; Johnatty, S.E.; Beesley, J.; Michailidou, K.; Tyrer, J.P.; Edwards, S.L.; Pickett, H.A.; Shen, H.C.; Smart, C.E.; et al. Multiple independent variants at the TERT locus are associated with telomere length and risks of breast and ovarian cancer. Nat. Genet. 2013, 45, 371–384. [Google Scholar] [CrossRef] [PubMed]
- Killedar, A.; Stutz, M.D.; Sobinoff, A.P.; Tomlinson, C.G.; Bryan, T.M.; Beesley, J.; Chenevix-Trench, G.; Reddel, R.R.; Pickett, H.A. A Common Cancer Risk-Associated Allele in the hTERT Locus Encodes a Dominant Negative Inhibitor of Telomerase. PLoS Genet. 2015, 11, e1005286. [Google Scholar] [CrossRef] [PubMed]
- Svenson, U.; Gronlund, E.; Soderstrom, I.; Sitaram, R.T.; Ljungberg, B.; Roos, G. Telomere length in relation to immunological parameters in patients with renal cell carcinoma. PLoS ONE 2013, 8, e55543. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Control Copulation | ||||
| N | Long RTL | Short RTL | p-Value | |
| Cohorts | 73 (100%) | 36 (49.32%) | 37 (50.68%) | |
| Age, mean (SD) | 60 (12.61) | 58 (12.84) | 61 (12.31) | 0.019 a |
| Gender | ||||
| Male | 59 (80.82%) | 26 (44.07%) | 33 (55.93%) | |
| Female | 14 (19.18%) | 10 (71.43%) | 4 (28.57%) | 0.066 b |
| Smoking status | ||||
| No smoking | 53 (72.60%) | 27 (50.94%) | 26 (49.06%) | |
| Smoking | 20 (27.40%) | 9 (45%) | 11 (55%) | 0.651 b |
| Bladder Cancer | ||||
| N | Long RTL | Short RTL | p-Value | |
| Patients | 144 (100%) | 72 (50%) | 72 (50%) | |
| Age, mean (SD) | 68 (10.94) | 67 (10.08) | 69 (11.75) | 0.036 a |
| Gender | ||||
| Male | 116 (80.56%) | 57 (49.14%) | 59 (50.86%) | |
| Female | 28 (19.44%) | 15 (53.57%) | 13 (46.43%) | 0.674 b |
| Smoking status | ||||
| No smoking | 99 (68.75%) | 49 (49.49%) | 50 (50.51%) | |
| Smoking | 45 (31.25%) | 23 (51.11%) | 22 (48.89%) | 0.875 b |
| Grade | ||||
| NHG | 33 (22.92%) | 15 (45.45%) | 18 (54.55%) | |
| HG | 108 (75%) | 55 (50.93%) | 53 (49.07%) | 0.582 b |
| Muscle invasiveness | ||||
| NMIBC (Tis, Ta, T1) | 82 (56.94%) | 45 (54.88%) | 37 (45.12%) | |
| MIBC (T2, 3, 4) | 62 (43.06%) | 27 (43.55%) | 35 (56.45%) | 0.178 b |
| Metastasis | ||||
| No | 140 (97.22%) | 71 (50.71%) | 69 (49.29%) | |
| Yes | 4 (2.78%) | 1 (25%) | 3 (75%) | 0.612 c |
| Lymphovascular invasion (LVI) | ||||
| No | 120 (83.33%) | 64 (53.33%) | 56 (46.67%) | |
| Yes | 24 (16.67%) | 8 (33.33%) | 16 (66.67%) | 0.074 b |
| Renal Cell Carcinoma | ||||
| N (%) | Long RTL (%) | Short RTL (%) | p-Value | |
| Patients | 144 (100) | 72 (50%) | 72 (50%) | |
| Age, mean (SD) | 69 (10.72) | 65 (11.16) | 73 (8.33) | <0.001 a |
| Gender | ||||
| Male | 93 (65.28%) | 48 (51.61%) | 45 (48.39%) | |
| Female | 51 (35.42%) | 24 (47.06%) | 27 (52.94%) | 0.601 b |
| Smoking status | ||||
| No smoking | 122 (84.72%) | 61(50%) | 61 (50%) | |
| Smoking | 22 (15.28%) | 11 (50%) | 11 (50%) | 1.000 b |
| Grade | ||||
| grade 1, 2 | 92 (65.25%) | 48 (52.17%) | 44 (47.83%) | |
| grade 3 | 49 (34.75%) | 22 (44.90%) | 27 (55.10%) | 0.411 b |
| Stage | ||||
| T 1,2 | 100 (69.44%) | 51 (51%) | 49 (49%) | |
| T 3 | 44 (30.56%) | 21 (47.73%) | 23 (52.27%) | 0.717 b |
| Pathology types | ||||
| ccRCC | 120 (83.33%) | 54 (45%) | 66 (55%) | |
| Other types | 24 (16.67%) | 18 (75%) | 6 (25%) | 0.007 b |
| Bladder Cancer | |||||||
| Factors | Cases | Univariate Analysis | Multivariate Analysis | ||||
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | ||
| Age | |||||||
| ≤68 | 77 | 1.08 | 0.528–2.200 | 0.837 | NA | NA | NA |
| >68 | 67 | ||||||
| Gender | |||||||
| Male | 116 | 1.60 | 0.750–3.396 | 0.225 | NA | NA | NA |
| Female | 28 | ||||||
| Smoking status | |||||||
| No smoking | 99 | 0.86 | 0.396–1.873 | 0.707 | NA | NA | NA |
| Smoking | 45 | ||||||
| Grade | |||||||
| NHG | 33 | 1.52 | 0.581–3.980 | 0.393 | NA | NA | NA |
| HG | 108 | ||||||
| Muscle invasiveness | |||||||
| NMIBC | 82 | 5.01 | 2.054–12.215 | <0.001 | 4.036 | 1.528–10.658 | 0.005 |
| MIBC | 62 | ||||||
| Metastasis | |||||||
| No | 140 | 8.74 | 2.520–30.337 | 0.001 | 4.995 | 1.385–18.009 | 0.014 |
| Yes | 4 | ||||||
| Lymphovascular invasion | |||||||
| No | 120 | 3.31 | 1.583–6.912 | 0.001 | 1.499 | 0.671–3.351 | 0.324 |
| Yes | 24 | ||||||
| RTL | |||||||
| long | 72 | 2.65 | 1.071–6.562 | 0.035 | 2.613 | 1.049–6.510 | 0.039 |
| short | 72 | ||||||
| Renal Cell Carcinoma | |||||||
| Factors | Cases | Univariate Analysis | Multivariate Analysis | ||||
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | ||
| Age | |||||||
| ≤69 | 71 | 2.34 | 0.908–6.305 | 0.078 | 1.59 | 0.592–4.268 | 0.357 |
| >69 | 73 | ||||||
| Gender | |||||||
| Male | 93 | 0.69 | 0.269–1.794 | 0.451 | NA | NA | NA |
| Female | 51 | ||||||
| Smoking status | |||||||
| No smoking | 122 | 1.27 | 0.428–3.790 | 0.663 | NA | NA | NA |
| Smoking | 22 | ||||||
| Grade | |||||||
| Grade 1, 2 | 92 | 1.92 | 0.801–4.608 | 0.143 | NA | NA | NA |
| Grade 3 | 49 | ||||||
| Stage | |||||||
| T 1,2 | 100 | 2.80 | 1.188–6.590 | 0.019 | 2.809 | 1.192–6.623 | 0.018 |
| T 3 | 44 | ||||||
| Pathology types | |||||||
| ccRCC | 120 | 0.90 | 0.264–3.097 | 0.872 | NA | NA | NA |
| Other types | 24 | ||||||
| RTL | |||||||
| long | 72 | 3.36 | 1.231–9.183 | 0.018 | 2.913 | 1.021–8.310 | 0.046 |
| short | 72 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zheng, X.; Wezel, F.; Azoitei, A.; Meessen, S.; Wang, W.; Najjar, G.; Wang, X.; Kraus, J.M.; Kestler, H.A.; John, A.; et al. Shorter Leukocyte Telomere Length Is Associated with Worse Survival of Patients with Bladder Cancer and Renal Cell Carcinoma. Cancers 2021, 13, 3774. https://doi.org/10.3390/cancers13153774
Zheng X, Wezel F, Azoitei A, Meessen S, Wang W, Najjar G, Wang X, Kraus JM, Kestler HA, John A, et al. Shorter Leukocyte Telomere Length Is Associated with Worse Survival of Patients with Bladder Cancer and Renal Cell Carcinoma. Cancers. 2021; 13(15):3774. https://doi.org/10.3390/cancers13153774
Chicago/Turabian StyleZheng, Xi, Felix Wezel, Anca Azoitei, Sabine Meessen, Wenya Wang, Gregoire Najjar, Xue Wang, Johann M. Kraus, Hans A. Kestler, Axel John, and et al. 2021. "Shorter Leukocyte Telomere Length Is Associated with Worse Survival of Patients with Bladder Cancer and Renal Cell Carcinoma" Cancers 13, no. 15: 3774. https://doi.org/10.3390/cancers13153774