Obesity as a Risk Factor for Prostate Cancer Mortality: A Systematic Review and Dose-Response Meta-Analysis of 280,199 Patients

 , , , ,
, , , , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
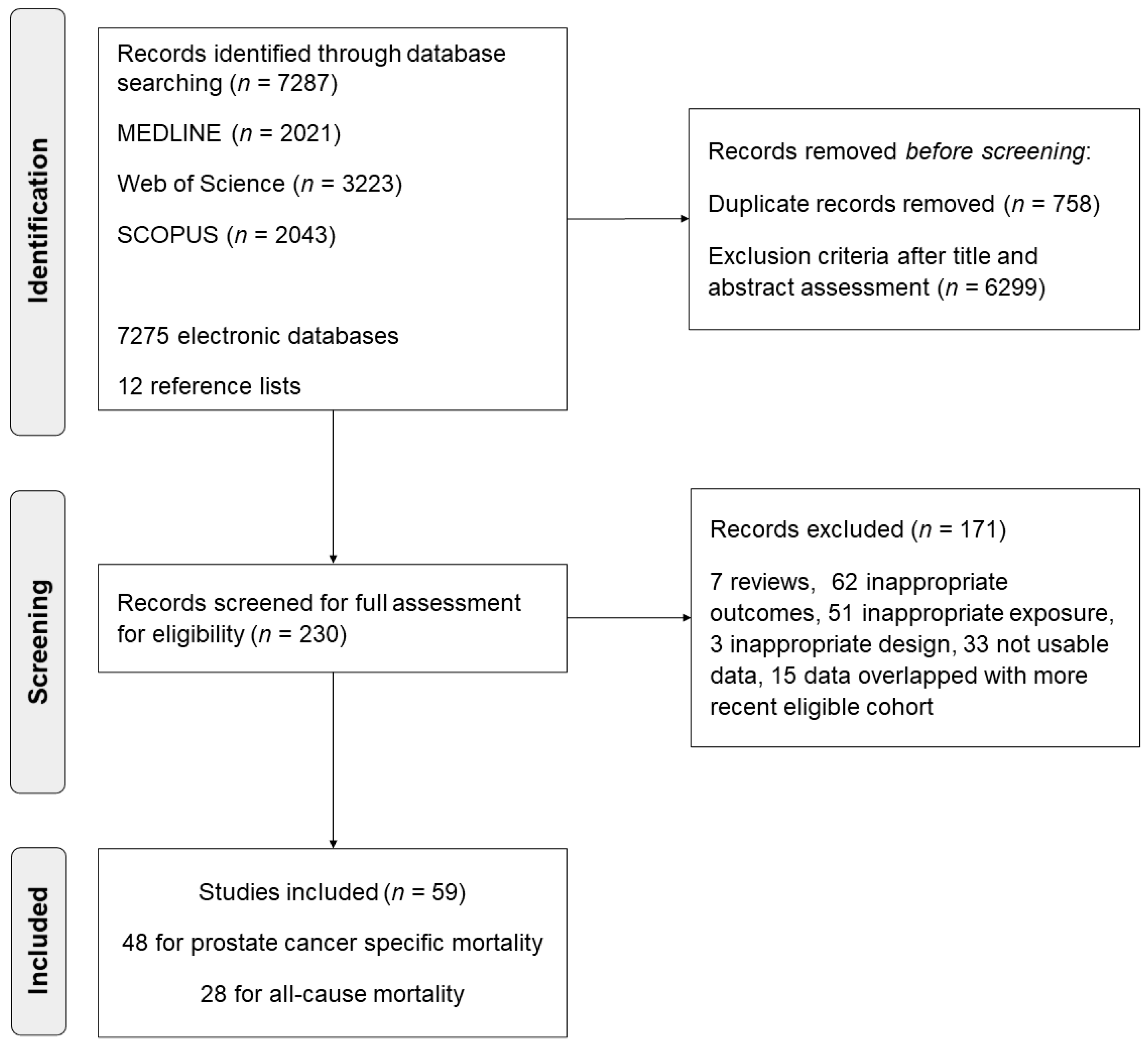
2.1. Search Strategy and Study Selection Criteria
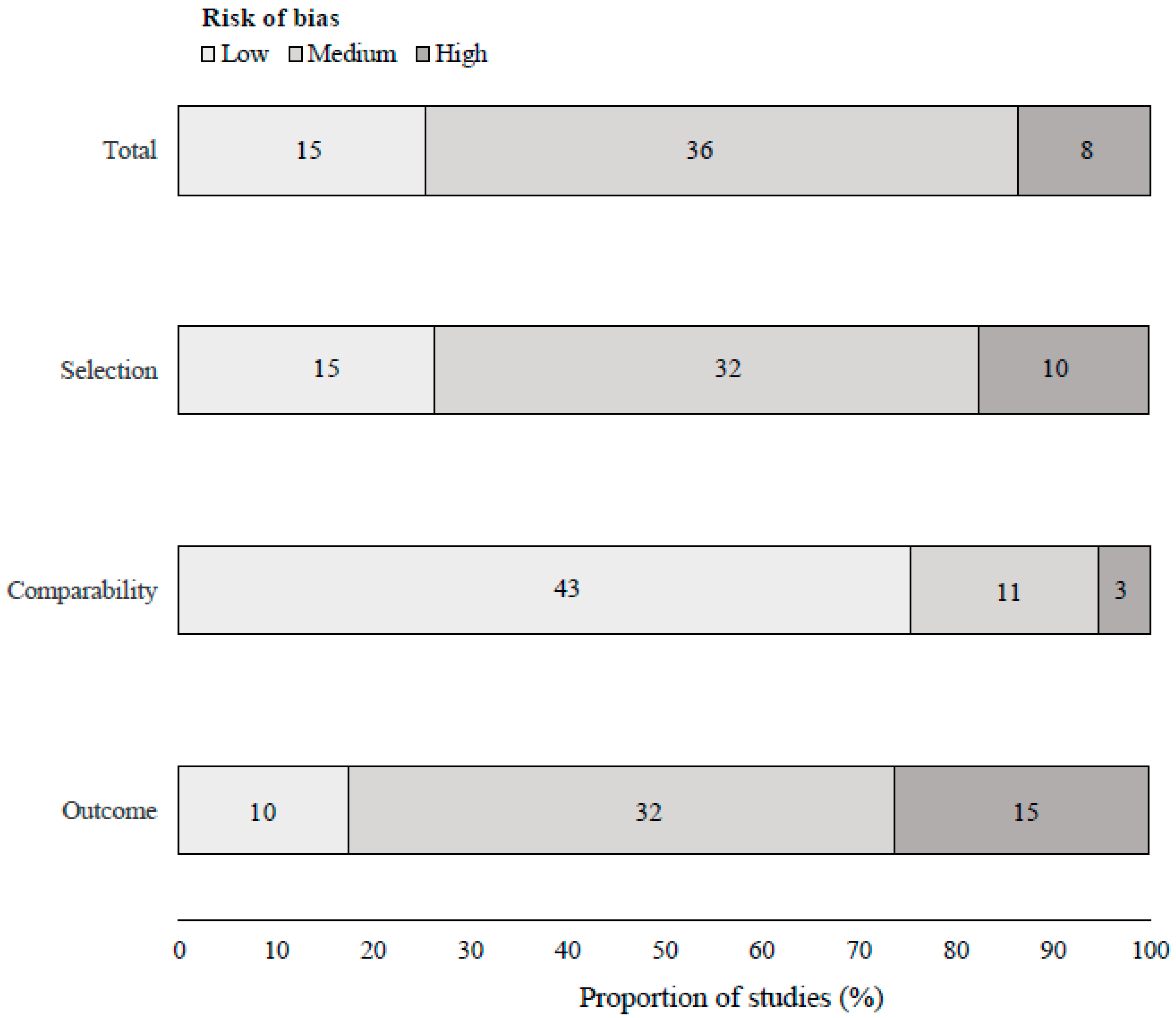
2.2. Data Extraction and Quality Assessment
2.3. Exposure and Outcomes
2.4. Data Synthesis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Fillon, M. Rates of advanced prostate cancer continue to increase. CA Cancer J. Clin. 2020, 70, 427–429. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 16 July 2021).
- Panuganti, K.K.; Nguyen, M.; Kshirsagar, R.K. Obesity. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Schatten, H. Brief Overview of Prostate Cancer Statistics, Grading, Diagnosis and Treatment Strategies. Adv. Exp. Med. Biol. 2018, 1095, 1–14. [Google Scholar] [PubMed]
- Genkinger, J.M.; Wu, K.; Wang, M.; Albanes, D.; Black, A.; van den Brandt, P.A.; Burke, K.A.; Cook, M.B.; Gapstur, S.M.; Giles, G.G.; et al. Measures of body fatness and height in early and mid-to-late adulthood and prostate cancer: Risk and mortality in The Pooling Project of Prospective Studies of Diet and Cancer. Ann. Oncol. 2020, 31, 103–114. [Google Scholar] [CrossRef] [Green Version]
- Jochems, S.H.J.; Stattin, P.; Häggström, C.; Järvholm, B.; Orho-Melander, M.; Wood, A.M.; Stocks, T. Height, body mass index and prostate cancer risk and mortality by way of detection and cancer risk category. Int. J. Cancer. 2020, 147, 3328–3338. [Google Scholar] [CrossRef] [PubMed]
- Jackson, M.D.; Tulloch-Reid, M.K.; McCaw-Binns, A.M.; Aiken, W.; Ferguson, T.S.; Bennett, N.R.; Harrison, L.; Badaloo, A.; McGrowder, D.; Grindley, A.; et al. Central adiposity at diagnosis may reduce prostate cancer-specific mortality in African-Caribbean men with prostate cancer: 10-year follow-up of participants in a case-control study. Cancer Causes Control. 2020, 31, 651–662. [Google Scholar] [CrossRef] [PubMed]
- Zhong, S.; Yan, X.; Wu, Y.; Zhang, X.; Chen, L.; Tang, J.; Zhao, J. Body mass index and mortality in prostate cancer patients: A dose-response meta-analysis. Prostate Cancer Prostatic Dis. 2016, 19, 122–131. [Google Scholar] [CrossRef]
- Zhang, X.; Zhou, G.; Sun, B.; Zhao, G.; Liu, D.; Sun, J.; Liu, C.; Guo, H. Impact of obesity upon prostate cancer-associated mortality: A meta-analysis of 17 cohort studies. Oncol. Lett. 2015, 9, 1307–1312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, Y.; Ma, J. Body mass index, prostate cancer-specific mortality, and biochemical recurrence: A systematic review and meta-analysis. Cancer Prev. Res. 2011, 4, 486–501. [Google Scholar] [CrossRef] [Green Version]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [Green Version]
- Bluethmann, S.M.; Wang, M.; Wasserman, E.; Chen, C.; Zaorsky, N.G.; Hohl, R.J.; McDonald, A.C. Prostate cancer in Pennsylvania: The role of older age at diagnosis, aggressiveness, and environmental risk factors on treatment and mortality using data from the Pennsylvania Cancer Registry. Cancer Med. 2020, 9, 3623–3633. [Google Scholar] [CrossRef]
- Crump, C.; Stattin, P.; Brooks, J.D.; Stocks, T.; Sundquist, J.; Sieh, W.; Sundquist, K. Early-Life Cardiorespiratory Fitness and Long-term Risk of Prostate Cancer. Cancer Epidemiol. Biomarkers Prev. 2020, 29, 2187–2194. [Google Scholar] [CrossRef]
- Vidal, A.C.; Oyekunle, T.; Howard, L.E.; De Hoedt, A.M.; Kane, C.J.; Terris, M.K.; Cooperberg, M.R.; Amling, C.L.; Klaassen, Z.; Freedland, S.J.; et al. Obesity, race, and long-term prostate cancer outcomes. Cancer 2020, 126, 3733–3741. [Google Scholar] [CrossRef]
- Troeschel, A.N.; Hartman, T.J.; Jacobs, E.J.; Stevens, V.L.; Gansler, T.; Flanders, W.D.; McCullough, L.E.; Wang, Y. Postdiagnosis Body Mass Index, Weight Change, and Mortality From Prostate Cancer, Cardiovascular Disease, and All Causes Among Survivors of Nonmetastatic Prostate Cancer. J. Clin. Oncol. 2020, 38, 2018–2027. [Google Scholar] [CrossRef]
- Langlais, C.S.; Cowan, J.E.; Neuhaus, J.; Kenfield, S.A.; Van Blarigan, E.L.; Broering, J.M.; Cooperberg, M.R.; Carroll, P.; Chan, J.M. Obesity at Diagnosis and Prostate Cancer Prognosis and Recurrence Risk Following Primary Treatment by Radical Prostatectomy. Cancer Epidemiol. Biomarkers Prev. 2019, 28, 1917–1925. [Google Scholar] [CrossRef] [Green Version]
- Darcey, E.; Pereira, G.; Salter, A.; Fritschi, L.; Leavy, J.; Ambrosini, G.L.; Boyle, T. The Impact of Lifestyle-related Factors on Survival After a Prostate Cancer Diagnosis. Eur. Urol. 2019, 75, 884–885. [Google Scholar] [CrossRef]
- Wade, K.H.; Carslake, D.; Tynelius, P.; Davey Smith, G.; Martin, R.M. Variation of all-cause and cause-specific mortality with body mass index in one million Swedish parent-son pairs: An instrumental variable analysis. PLoS Med. 2019, 16, e1002868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farris, M.S.; Courneya, K.S.; Kopciuk, K.A.; McGregor, S.E.; Friedenreich, C.M. Anthropometric measurements and survival after a prostate cancer diagnosis. Br. J. Cancer 2018, 118, 607–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, M.B.; Yang, T.; Hu, J.M.; Zhu, W.H.; Jiang, H.W.; Ding, Q. Prognostic factors in Chinese patients with prostate cancer receiving primary androgen deprivation therapy: Validation of Japan Cancer of the Prostate Risk Assessment (J-CAPRA) score and impacts of pre-existing obesity and diabetes mellitus. Int. J. Clin. Oncol. 2018, 23, 591–598. [Google Scholar] [CrossRef] [PubMed]
- Perez-Cornago, A.; Appleby, P.N.; Pischon, T.; Tsilidis, K.K.; Tjønneland, A.; Olsen, A.; Overvad, K.; Kaaks, R.; Kühn, T.; Boeing, H.; et al. Tall height and obesity are associated with an increased risk of aggressive prostate cancer: Results from the EPIC cohort study. BMC Med. 2017, 15, 115. [Google Scholar] [CrossRef] [PubMed]
- Dickerman, B.A.; Ahearn, T.U.; Giovannucci, E.; Stampfer, M.J.; Nguyen, P.L.; Mucci, L.A.; Wilson, K.M. Weight change, obesity and risk of prostate cancer progression among men with clinically localized prostate cancer. Int. J. Cancer 2017, 141, 933–944. [Google Scholar] [CrossRef]
- Kelly, S.P.; Graubard, B.I.; Andreotti, G.; Younes, N.; Cleary, S.D.; Cook, M.B. Prediagnostic Body Mass Index Trajectories in Relation to Prostate Cancer Incidence and Mortality in the PLCO Cancer Screening Trial. J. Natl. Cancer Inst. 2016, 109, djw225. [Google Scholar] [CrossRef] [Green Version]
- Hill, A.B. The environment and disease: Association or causation? Proc. R. Soc. Med. 1965, 58, 295–300. [Google Scholar] [CrossRef] [Green Version]
- Rivera-Izquierdo, M.; Jiménez-Moleón, J.J. Is Obesity A Prognostic Factor for Prostate Cancer? A Systematic Review and Meta-Analysis of Analytic Studies. PROSPERO: International Prospective Register of Systematic Reviews 2020: CRD42020214600. Available online: http://www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42020214600 (accessed on 19 July 2021).
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 17 July 2021).
- World Health Organization. Body Mass Index. Available online: https://www.who.int/data/gho/data/themes/theme-details/GHO/body-mass-index-(bmi) (accessed on 17 July 2021).
- Riley, R.D.; Moons, K.G.M.; Snell, K.I.E.; Ensor, J.; Hooft, L.; Altman, D.G.; Hayden, J.; Collins, G.S.; Debray, T.P.A. A guide to systematic review and meta-analysis of prognostic factor studies. BMJ 2019, 364, k4597. [Google Scholar] [CrossRef] [Green Version]
- Riley, R.D.; Higgins, J.P.; Deeks, J.J. Interpretation of random effects metaanalyses. BMJ 2011, 342, d549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenland, S.; Longnecker, M.P. Methods for trend estimation from summarized dose-response data, with applications to meta-analysis. Am. J. Epidemiol. 1992, 135, 1301–1309. [Google Scholar] [CrossRef]
- Centre for Evidence-Based Medicine. Levels of Evidence. Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence (accessed on 17 July 2021).
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Polesel, J.; Gini, A.; Dal Maso, L.; Stocco, C.; Birri, S.; Taborelli, M.; Serraino, D.; Zucchetto, A. The impact of diabetes and other metabolic disorders on prostate cancer prognosis. J. Diabetes Complicat. 2016, 30, 591–596. [Google Scholar] [CrossRef]
- Cushen, S.J.; Power, D.G.; Murphy, K.P.; McDermott, R.; Griffin, B.T.; Lim, M.; Daly, L.; MacEneaney, P.; O’ Sullivan, K.; Prado, C.M.; et al. Impact of body composition parameters on clinical outcomes in patients with metastatic castrate-resistant prostate cancer treated with docetaxel. Clin. Nutr. ESPEN 2016, 13, e39–e45. [Google Scholar] [CrossRef]
- Fowke, J.H.; McLerran, D.F.; Gupta, P.C.; He, J.; Shu, X.O.; Ramadas, K.; Tsugane, S.; Inoue, M.; Tamakoshi, A.; Koh, W.P.; et al. Associations of body mass index, smoking, and alcohol consumption with prostate cancer mortality in the Asia Cohort Consortium. Am. J. Epidemiol. 2015, 182, 381–389. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.S.; Murphy, C.T.; Ruth, K.; Zaorsky, N.G.; Smaldone, M.C.; Sobczak, M.L.; Kutikov, A.; Viterbo, R.; Horwitz, E.M. Impact of obesity on outcomes after definitive dose-escalated intensity-modulated radiotherapy for localized prostate cancer. Cancer 2015, 121, 3010–3017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cantarutti, A.; Bonn, S.E.; Adami, H.O.; Grönberg, H.; Bellocco, R.; Bälter, K. Body mass index and mortality in men with prostate cancer. Prostate 2015, 75, 1129–1136. [Google Scholar] [CrossRef] [PubMed]
- Taghizadeh, N.; Boezen, H.M.; Schouten, J.P.; Schröder, C.P.; Elisabeth de Vries, E.G.; Vonk, J.M. BMI and lifetime changes in BMI and cancer mortality risk. PLoS ONE 2015, 10, e0125261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohammed, A.A.; El-Tanni, H.; Ghanem, H.M.; Farooq, M.U.; El Saify, A.M.; Al-Zahrani, A.S.; El-Shentenawy, A.; El-Khatib, H.M. Impact of body mass index on clinico-pathological parameters and outcome in patients with metastatic prostate cancer. J. Egypt. Natl. Canc. Inst. 2015, 27, 155–159. [Google Scholar] [CrossRef] [Green Version]
- Møller, H.; Roswall, N.; Van Hemelrijck, M.; Larsen, S.B.; Cuzick, J.; Holmberg, L.; Overvad, K.; Tjønneland, A. Prostate cancer incidence, clinical stage and survival in relation to obesity: A prospective cohort study in Denmark. Int. J. Cancer. 2015, 136, 1940–1947. [Google Scholar] [CrossRef] [Green Version]
- Bonn, S.E.; Wiklund, F.; Sjölander, A.; Szulkin, R.; Stattin, P.; Holmberg, E.; Grönberg, H.; Bälter, K. Body mass index and weight change in men with prostate cancer: Progression and mortality. Cancer Causes Control 2014, 25, 933–943. [Google Scholar] [CrossRef]
- Chalfin, H.J.; Lee, S.B.; Jeong, B.C.; Freedland, S.J.; Alai, H.; Feng, Z.; Trock, B.J.; Partin, A.W.; Humphreys, E.; Walsh, P.C.; et al. Obesity and long-term survival after radical prostatectomy. J. Urol. 2014, 192, 1100–1104. [Google Scholar] [CrossRef]
- Haque, R.; Van Den Eeden, S.K.; Wallner, L.P.; Richert-Boe, K.; Kallakury, B.; Wang, R.; Weinmann, S. Association of body mass index and prostate cancer mortality. Obes. Res. Clin. Pract. 2014, 8, e374–e381. [Google Scholar] [CrossRef] [Green Version]
- Froehner, M.; Kellner, A.E.; Koch, R.; Baretton, G.B.; Hakenberg, O.W.; Wirth, M.P. A combined index to classify prognostic comorbidity in candidates for radical prostatectomy. BMC Urol. 2014, 14, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gravis, G.; Boher, J.M.; Fizazi, K.; Joly, F.; Priou, F.; Marino, P.; Latorzeff, I.; Delva, R.; Krakowski, I.; Laguerre, B.; et al. Prognostic Factors for Survival in Noncastrate Metastatic Prostate Cancer: Validation of the Glass Model and Development of a Novel Simplified Prognostic Model. Eur. Urol. 2015, 68, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Tendulkar, R.D.; Hunter, G.K.; Reddy, C.A.; Stephans, K.L.; Ciezki, J.P.; Abdel-Wahab, M.; Stephenson, A.J.; Klein, E.A.; Mahadevan, A.; Kupelian, P.A.; et al. Causes of mortality after dose-escalated radiation therapy and androgen deprivation for high-risk prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, 94–99. [Google Scholar] [CrossRef]
- Bassett, J.K.; Severi, G.; Baglietto, L.; MacInnis, R.J.; Hoang, H.N.; Hopper, J.L.; English, D.R.; Giles, G.G. Weight change and prostate cancer incidence and mortality. Int. J. Cancer 2012, 131, 1711–1719. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, G.G.; Skinner, H.G. A prospective study of total and ionized serum calcium and time to fatal prostate cancer. Cancer Epidemiol. Biomark. Prev. 2012, 21, 1768–1773. [Google Scholar] [CrossRef] [Green Version]
- Park, J.M.; Nam, J.S.; Na, W.; Oh, J.J.; Lee, S.; Hong, S.K.; Byun, S.S.; Lee, S.E. Prognostic value of body mass index in korean patients with castration-resistant prostate cancer. Korean J. Urol. 2012, 53, 761–765. [Google Scholar] [CrossRef]
- Häggström, C.; Stocks, T.; Ulmert, D.; Bjørge, T.; Ulmer, H.; Hallmans, G.; Manjer, J.; Engeland, A.; Nagel, G.; Almqvist, M.; et al. Prospective study on metabolic factors and risk of prostate cancer. Cancer 2012, 118, 6199–6206. [Google Scholar] [CrossRef]
- Discacciati, A.; Orsini, N.; Andersson, S.O.; Andrén, O.; Johansson, J.E.; Wolk, A. Body mass index in early and middle-late adulthood and risk of localised, advanced and fatal prostate cancer: A population-based prospective study. Br. J. Cancer 2011, 105, 1061–1068. [Google Scholar] [CrossRef]
- Dehal, A.; Garrett, T.; Tedders, S.H.; Arroyo, C.; Afriyie-Gyawu, E.; Zhang, J. Body mass index and death rate of colorectal cancer among a national cohort of U.S. adults. Nutr. Cancer 2011, 63, 1218–1225. [Google Scholar]
- Geinitz, H.; Thamm, R.; Mueller, T.; Jess, K.; Zimmermann, F.B.; Molls, M.; Nieder, C. Impact of body mass index on outcomes after conformal radiotherapy in patients with prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 16–22. [Google Scholar] [CrossRef]
- Van Roermund, J.G.; Hinnen, K.A.; Battermann, J.J.; Witjes, J.A.; Bosch, J.L.; Kiemeney, L.A.; van Vulpen, M. Body mass index is not a prognostic marker for prostate-specific antigen failure and survival in Dutch men treated with brachytherapy. BJU Int. 2010, 105, 42–48. [Google Scholar] [CrossRef]
- Han, M.; Trock, B.J.; Partin, A.W.; Humphreys, E.B.; Bivalacqua, T.J.; Guzzo, T.J.; Walsh, P.C. The impact of preoperative erectile dysfunction on survival after radical prostatectomy. BJU Int. 2010, 106, 1612–1617. [Google Scholar] [CrossRef] [Green Version]
- Burton, A.; Martin, R.; Galobardes, B.; Davey Smith, G.; Jeffreys, M. Young adulthood body mass index and risk of cancer in later adulthood: Historical cohort study. Cancer Causes Control. 2010, 21, 2069–2077. [Google Scholar] [CrossRef]
- Martin, R.M.; Vatten, L.; Gunnell, D.; Romundstad, P.; Nilsen, T.I. Components of the metabolic syndrome and risk of prostate cancer: The HUNT 2 cohort, Norway. Cancer Causes Control. 2009, 20, 1181–1192. [Google Scholar] [CrossRef] [PubMed]
- Pfitzenmaier, J.; Pritsch, M.; Haferkamp, A.; Jakobi, H.; Fritsch, F.; Gilfrich, C.; Djakovic, N.; Buse, S.; Pahernik, S.; Hohenfellner, M. Is the body mass index a predictor of adverse outcome in prostate cancer after radical prostatectomy in a mid-European study population? BJU Int. 2009, 103, 877–882. [Google Scholar] [CrossRef]
- Davies, B.J.; Smaldone, M.C.; Sadetsky, N.; Dall’era, M.; Carroll, P.R. The impact of obesity on overall and cancer specific survival in men with prostate cancer. J. Urol. 2009, 182, 112–117. [Google Scholar] [CrossRef]
- Armstrong, A.J.; Halabi, S.; de Wit, R.; Tannock, I.F.; Eisenberger, M. The relationship of body mass index and serum testosterone with disease outcomes in men with castration-resistant metastatic prostate cancer. Prostate Cancer Prostatic Dis. 2009, 12, 88–93. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.; Li, H.; Giovannucci, E.; Mucci, L.; Qiu, W.; Nguyen, P.L.; Gaziano, J.M.; Pollak, M.; Stampfer, M.J. Prediagnostic body-mass index, plasma C-peptide concentration, and prostate cancer-specific mortality in men with prostate cancer: A long-term survival analysis. Lancet Oncol. 2008, 9, 1039–1047. [Google Scholar] [CrossRef] [Green Version]
- Merrick, G.S.; Galbreath, R.W.; Butler, W.M.; Wallner, K.E.; Allen, Z.A.; Adamovich, E. Obesity is not predictive of overall survival following permanent prostate brachytherapy. Am. J. Clin. Oncol. 2007, 30, 588–596. [Google Scholar] [CrossRef]
- Efstathiou, J.A.; Bae, K.; Shipley, W.U.; Hanks, G.E.; Pilepich, M.V.; Sandler, H.M.; Smith, M.R. Obesity and mortality in men with locally advanced prostate cancer: Analysis of RTOG 85-31. Cancer 2007, 110, 2691–2699. [Google Scholar] [CrossRef] [PubMed]
- Gong, Z.; Agalliu, I.; Lin, D.W.; Stanford, J.L.; Kristal, A.R. Obesity is associated with increased risks of prostate cancer metastasis and death after initial cancer diagnosis in middle-aged men. Cancer 2007, 109, 1192–1202. [Google Scholar] [CrossRef]
- Montgomery, R.B.; Goldman, B.; Tangen, C.M.; Hussain, M.; Petrylak, D.P.; Page, S.; Klein, E.A.; Crawford, E.D.; Southwest Oncology Group. Association of body mass index with response and survival in men with metastatic prostate cancer: Southwest Oncology Group trials 8894 and 9916. J. Urol. 2007, 178, 1946–1951. [Google Scholar] [CrossRef] [PubMed]
- Wright, M.E.; Chang, S.C.; Schatzkin, A.; Albanes, D.; Kipnis, V.; Mouw, T.; Hurwitz, P.; Hollenbeck, A.; Leitzmann, M.F. Prospective study of adiposity and weight change in relation to prostate cancer incidence and mortality. Cancer 2007, 109, 675–684. [Google Scholar] [CrossRef] [PubMed]
- Asia Pacific Cohort Studies Collaboration; Huxley, R.; Ansary-Mohaddam, A.; Huxley, R.; Barzi, F.; Lam, T.H.; Jamrozik, K.; Ohkubo, T.; Fang, X.; Sun, H.J. The impact of modifiable risk factors on mortality from prostate cancer in populations of the Asia-Pacific region. Asian Pac. J. Cancer Prev. 2007, 8, 199–205. [Google Scholar]
- Halabi, S.; Ou, S.S.; Vogelzang, N.J.; Small, E.J. Inverse correlation between body mass index and clinical outcomes in men with advanced castration-recurrent prostate cancer. Cancer 2007, 110, 1478–1484. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, S.A.; Inman, B.A.; Sengupta, S.; Slezak, J.M.; Bergstralh, E.J.; Leibovich, B.C.; Zincke, H.; Blute, M.L. Obesity and survival after radical prostatectomy: A 10-year prospective cohort study. Cancer 2006, 107, 521–529. [Google Scholar] [CrossRef]
- Park, S.M.; Lim, M.K.; Shin, S.A.; Yun, Y.H. Impact of prediagnosis smoking, alcohol, obesity, and insulin resistance on survival in male cancer patients: National Health Insurance Corporation Study. J. Clin. Oncol. 2006, 24, 5017–5024. [Google Scholar] [CrossRef]
- Eichholzer, M.; Bernasconi, F.; Jordan, P.; Stähelin, H.B. Body mass index and the risk of male cancer mortality of various sites: 17-year follow-up of the Basel cohort study. Swiss Med. Wkly. 2005, 135, 27–33. [Google Scholar]
- Rodriguez, C.; Patel, A.V.; Calle, E.E.; Jacobs, E.J.; Chao, A.; Thun, M.J. Body mass index, height, and prostate cancer mortality in two large cohorts of adult men in the United States. Cancer Epidemiol. Biomark. Prev. 2001, 10, 345–353. [Google Scholar]
- Gapstur, S.M.; Gann, P.H.; Colangelo, L.A.; Barron-Simpson, R.; Kopp, P.; Dyer, A.; Liu, K. Postload plasma glucose concentration and 27-year prostate cancer mortality (United States). Cancer Causes Control. 2001, 12, 763–772. [Google Scholar] [CrossRef]
- Andersson, S.O.; Wolk, A.; Bergström, R.; Adami, H.O.; Engholm, G.; Englund, A.; Nyrén, O. Body size and prostate cancer: A 20-year follow-up study among 135006 Swedish construction workers. J. Natl. Cancer Inst. 1997, 89, 385–389. [Google Scholar] [CrossRef] [Green Version]
- Huedo-Medina, T.B.; Sánchez-Meca, J.; Marín-Martínez, F.; Botella, J. Assessing heterogeneity in meta-analysis: Q statistic or I2 index? Psychol. Methods 2006, 11, 193–206. [Google Scholar] [CrossRef] [Green Version]
- Khan, K.S.; Ball, E.; Fox, C.E.; Meads, C. Systematic reviews to evaluate causation: An overview of methods and application. Evid. Based Med. 2012, 17, 137–141. [Google Scholar] [CrossRef] [PubMed]
- Gerdtsson, A.; Poon, J.B.; Thorek, D.L.; Mucci, L.A.; Evans, M.J.; Scardino, P.; Abrahamsson, P.A.; Nilsson, P.; Manjer, J.; Bjartell, A.; et al. Anthropometric Measures at Multiple Times Throughout Life and Prostate Cancer Diagnosis, Metastasis, and Death. Eur. Urol. 2015, 68, 1076–1082. [Google Scholar] [CrossRef] [Green Version]
- Chamberlain, C.; Romundstad, P.; Vatten, L.; Gunnell, D.; Martin, R.M. The association of weight gain during adulthood with prostate cancer incidence and survival: A population-based cohort. Int. J. Cancer 2011, 129, 1199–1206. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, P.L.; Ma, J.; Chavarro, J.E.; Freedman, M.L.; Lis, R.; Fedele, G.; Fiore, C.; Qiu, W.; Fiorentino, M.; Finn, S.; et al. Fatty acid synthase polymorphisms, tumor expression, body mass index, prostate cancer risk, and survival. J. Clin. Oncol. 2010, 28, 3958–3964. [Google Scholar] [CrossRef] [Green Version]
- Arcidiacono, B.; Iiritano, S.; Nocera, A.; Possidente, K.; Nevolo, M.T.; Ventura, V.; Foti, D.; Chiefari, E.; Brunetti, A. Insulin resistance and cancer risk: An overview of the pathogenetic mechanisms. Exp. Diabetes Res. 2012, 2012, 789174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santoni, M.; Cimadamore, A.; Massari, F.; Piva, F.; Aurilio, G.; Martignetti, A.; Scarpelli, M.; Di Nunno, V.; Gatto, L.; Battelli, N.; et al. Key Role of Obesity in Genitourinary Tumors with Emphasis on Urothelial and Prostate Cancers. Cancers 2019, 11, 1225. [Google Scholar] [CrossRef] [Green Version]
- Petrelli, F.; Cortellini, A.; Indini, A.; Tomasello, G.; Ghidini, M.; Nigro, O.; Salati, M.; Dottorini, L.; Iaculli, A.; Varricchio, A.; et al. Association of Obesity With Survival Outcomes in Patients With Cancer: A Systematic Review and Meta-analysis. JAMA Netw. Open 2021, 4, e213520. [Google Scholar] [CrossRef] [PubMed]
- Annett, S.; Moore, G.; Robson, T. Obesity and Cancer Metastasis: Molecular and Translational Perspectives. Cancers 2020, 12, 3798. [Google Scholar] [CrossRef]
- World Cancer Research Fund. American Institute for Cancer Research. Body Fatness and Weight Gain. Available online: https://www.wcrf.org/dietandcancer/exposures/body-fatness (accessed on 17 August 2021).
- Freedland, S.J.; Howard, L.; Allen, J.; Smith, J.; Stout, J.; Aronson, W.; Inman, B.A.; Armstrong, A.J.; George, D.; Westman, E.; et al. A lifestyle intervention of weight loss via a low-carbohydrate diet plus walking to reduce metabolic disturbances caused by androgen deprivation therapy among prostate cancer patients: Carbohydrate and prostate study 1 (CAPS1) randomized controlled trial. Prostate Cancer Prostatic Dis. 2019, 22, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Schenk, J.M.; Neuhouser, M.L.; Beatty, S.J.; VanDoren, M.; Lin, D.W.; Porter, M.; Gore, J.L.; Gulati, R.; Plymate, S.R.; Wright, J.L. Randomized trial evaluating the role of weight loss in overweight and obese men with early stage prostate Cancer on active surveillance: Rationale and design of the Prostate Cancer Active Lifestyle Study (PALS). Contemp. Clin. Trials 2019, 81, 34–39. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subgroup | Prostate Cancer Specific Mortality | All-Cause Mortality | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Obesity (BMI ≥ 30) Compared with Normal Weight (BMI < 25) | BMI Continuous Per 5 kg/m2 | Obesity (BMI > 30) Compared with Normal Weight (BMI < 25) | BMI Continuous Per 5 kg/m2 | |||||||||
| N | HR (95% CI) | I2 | N | HR (95% CI) | I2 | N | HR (95% CI) | I2 | N | HR (95% CI) | I2 | |
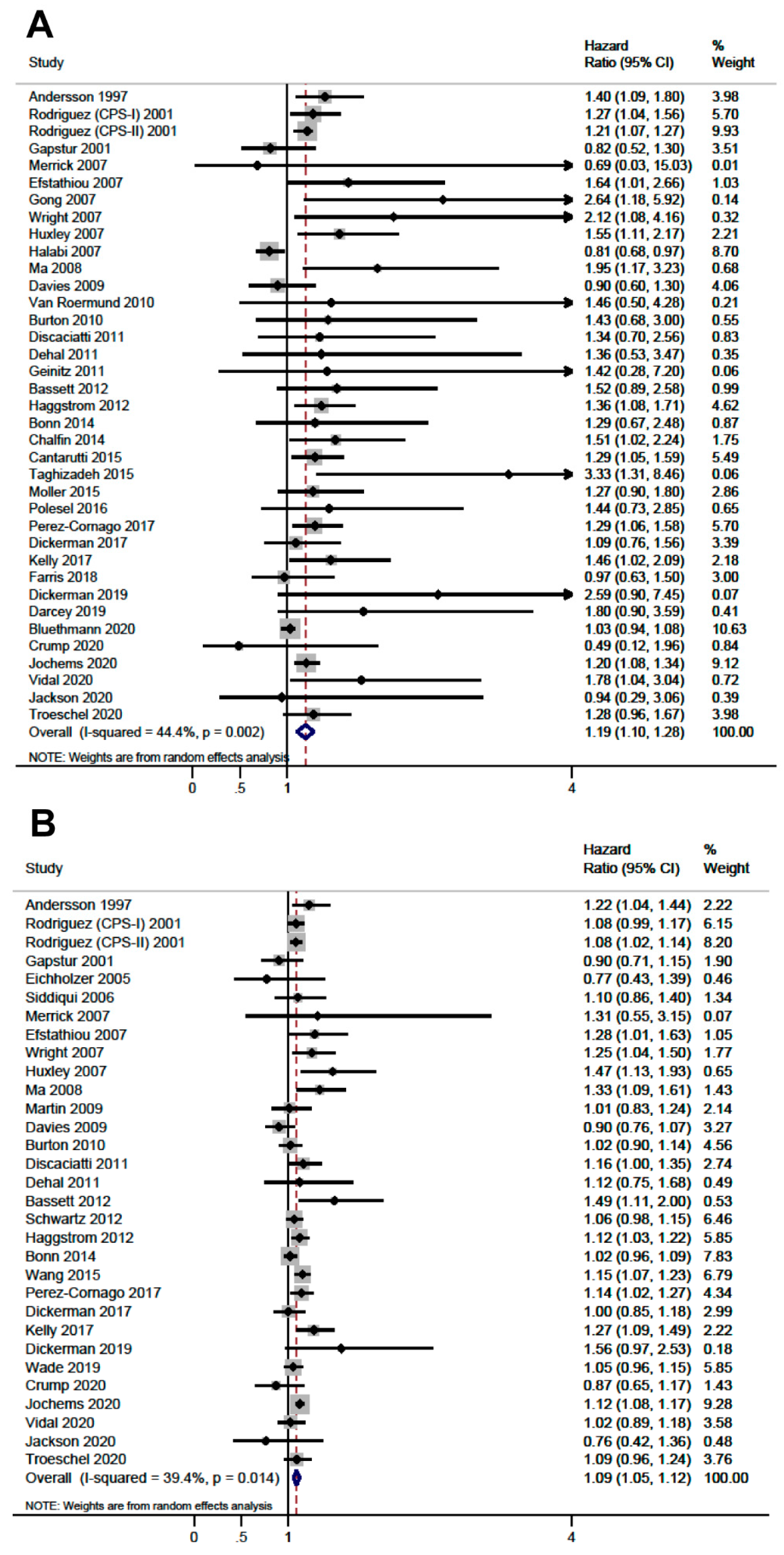
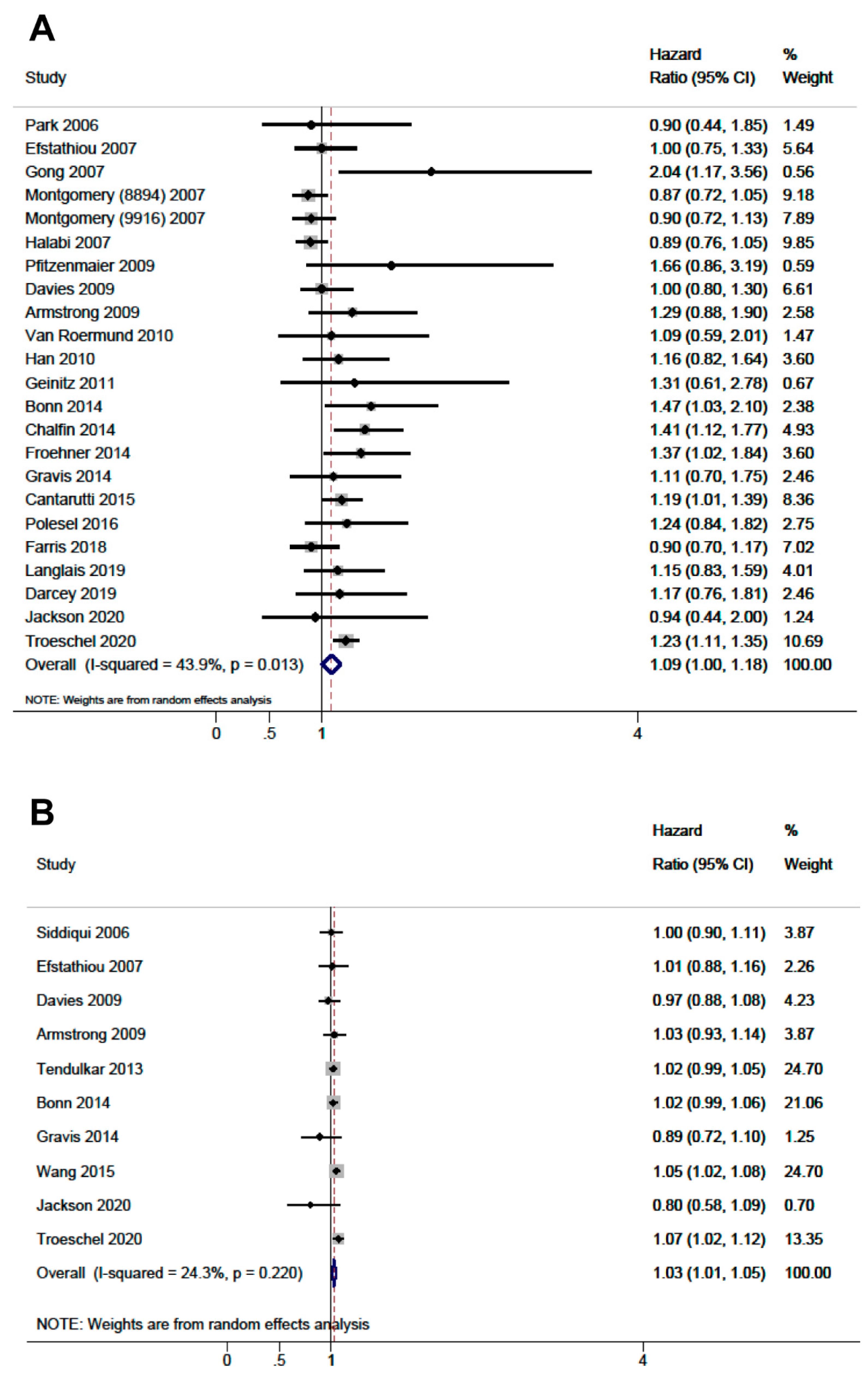
| All Studies (Total) | 37 | 1.19 (1.10–1.28) | 44.3 | 31 | 1.09 (1.05–1.12) | 44.3 | 23 | 1.09 (1.00–1.18) | 43.9 | 10 | 1.03 (1.01–1.05) | 24.3 |
| Population | ||||||||||||
| Population-Based Incident PC | 22 | 1.24 (1.18–1.31) | 0.0 | 18 | 1.10 (1.07–1.14) | 31.3 | 6 | 1.10 (0.92–1.28) | 25.5 | 0 | - | - |
| Industry Workers Incident PC | 2 | 1.12 (0.55–1.68) | 78.5 | 3 | 1.01 (0.74–1.27) | 65.9 | 0 | - | - | 0 | - | - |
| Radical Prostatectomy | 2 | 1.58 (1.06–2.10) | 0.0 | 2 | 1.04 (0.91–1.17) | 0.0 | 5 | 1.29 (1.11–1.48) | 0.0 | 1 | 1.00 (0.89–1.11) | - |
| Localized PC | 8 | 1.04 (0.97–1.10) | 0.0 | 6 | 1.05 (0.97–1.12) | 55.3 | 5 | 1.20 (1.09–1.30) | 0.0 | 4 | 1.04 (1.01–1.07) | 39.3 |
| Advanced PC | 2 | 1.12 (0.33–1.91) | 73.3 | 1 | 1.28 (0.97–1.59) | - | 6 | 0.91 (0.83–1.00) | 0.0 | 4 | 1.02 (0.99–1.05) | 0.0 |
| African-Caribbean Ancestry | 1 | 0.94 (0.44–2.33) | - | 1 | 0.76 (0.29–1.23) | - | 1 | 0.94 (0.16–1.72) | - | 1 | 0.80 (0.55–1.05) | - |
| Country | ||||||||||||
| USA | 17 | 1.13 (1.00–1.28) | 61.6 | 15 | 1.09 (1.04–1.14) | 36.8 | 12 | 1.05 (0.93–1.17) | 63.8 | 7 | 1.04 (1.02–1.05) | 0.0 |
| European Nordic Countries | 9 | 1.22 (1.12–1.32) | 0.0 | 9 | 1.08 (1.01–1.14) | 45.5 | 2 | 1.22 (1.04–1.40) | 0.0 | 1 | 1.02 (0.98–1.05) | - |
| European Central Countries | 7 | 1.33 (1.14–1.53) | 0.0 | 4 | 1.09 (1.01–1.17) | 25.2 | 6 | 1.26 (1.02–1.50) | 0.0 | 1 | 0.89 (0.70–1.08) | - |
| Other | 4 | 1.51 (1.11–1.92) | 0.0 | 3 | 1.25 (0.80–1.70) | 68.9 | 3 | 1.04 (0.67–1.41) | 0.0 | 1 | 0.80 (0.55–1.05) | - |
| Country status | ||||||||||||
| Developed Countries | 35 | 1.18 (1.10–1.27) | 45.2 | 29 | 1.09 (1.05–1.12) | 36.6 | 22 | 1.09 (1.00–1.19) | 46.3 | 9 | 1.03 (1.01–1.05) | 8.4 |
| Developing Countries | 2 | 1.47 (0.98–1.97) | 0.0 | 2 | 1.13 (0.43–1.82) | 80.3 | 1 | 0.94 (0.44–2.00) | - | 1 | 0.80 (0.55–1.05) | - |
| Exposure Measurement 1 | ||||||||||||
| Prediagnosis BMI | 22 | 1.23 (1.17–1.30) | 0.0 | 21 | 1.09 (1.06–1.13) | 35.0 | 19 | 1.08 (0.98–1.18) | 47.4 | 0 | - | - |
| Postdiagnosis BMI | 15 | 1.10 (0.96–1.23) | 42.8 | 10 | 1.07 (1.00–1.14) | 48.5 | 4 | 1.20 (1.03–1.37) | 0.0 | 10 | 1.03 (1.01–1.05) | 24.3 |
| Quality of the Evidence 2 | ||||||||||||
| Level 2 (Prospective Cohort) | 26 | 1.19 (1.10–1.28) | 34.4 | 26 | 1.09 (1.05−1.13) | 35.1 | 12 | 1.04 (0.92−1.16) | 50.3 | 6 | 1.02 (0.98−1.07) | 20.5 |
| Level 3 | 11 | 1.27 (0.99−1.55) | 57.5 | 5 | 1.08 (0.99−1.17) | 61.5 | 11 | 1.17 (1.02−1.32) | 40.0 | 4 | 1.03 (1.00−1.06) | 46.2 |
| Risk of Bias | ||||||||||||
| NOS: 8−9 | 9 | 1.24 (1.14−1.35) | 0.0 | 12 | 1.11 (1.07−1.15) | 26.6 | 2 | 1.46 (1.01−1.91) | 7.3 | 1 | 1.05 (1.02−1.08) | - |
| NOS: 6−7 | 27 | 1.17 (1.07−1.27) | 49.2 | 18 | 1.07 (1.02−1.12) | 41.6 | 16 | 1.10 (1.01−1.20) | 36.9 | 6 | 1.02 (0.98−1.06) | 34.2 |
| NOS <6 | 1 | 0.69 (0.03−15.03) | - | 1 | 1.31 (0.55−3.15) | - | 5 | 0.90 (0.80−1.07) | 10.3 | 3 | 1.02 (0.99−1.05) | 0.0 |
| Design | ||||||||||||
| Cohort | 36 | 1.19 (1.11–1.28) | 45.9 | 30 | 1.09 (1.05–1.12) | 39.1 | 22 | 1.09 (1.00–1.18) | 43.9 | 9 | 1.03 (1.01–1.05) | 8.4 |
| Case-Control | 1 | 0.94 (0.44–2.33) | - | 1 | 0.79 (0.29–1.23) | - | 1 | 0.94 (0.16–1.72) | - | 1 | 0.80 (0.55–1.05) | - |
| Stage | ||||||||||||
| Adjustment for Stage | 13 | 1.11 (0.95–1.27) | 44.0 | 8 | 1.08 (1.01–1.16) | 52.1 | 14 | 1.08 (0.95–1.21) | 55.6 | 5 | 1.04 (1.01–1.07) | 39.8 |
| Not Adjustment for Stage | 24 | 1.22 (1.16–1.29) | 0.0 | 23 | 1.09 (1.05–1.13) | 35.8 | 9 | 1.12 (1.00–1.23) | 10.0 | 5 | 1.01 (0.99–1.04) | 0.0 |
| Year of Publication | ||||||||||||
| <2016 | 24 | 1.19 (1.10–1.28) | 50.1 | 21 | 1.09 (1.05–1.12) | 39.4 | 6 | 1.13 (0.99–1.27) | 22.1 | 2 | 0.97 (0.71–1.22) | 75.9 |
| ≥2016 | 13 | 1.15 (1.04–1.26) | 28.9 | 10 | 1.08 (1.03–1.14) | 35.4 | 17 | 1.08 (0.97–1.19) | 42.4 | 8 | 1.03 (1.01–1.04) | 0.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rivera-Izquierdo, M.; Pérez de Rojas, J.; Martínez-Ruiz, V.; Pérez-Gómez, B.; Sánchez, M.-J.; Khan, K.S.; Jiménez-Moleón, J.J. Obesity as a Risk Factor for Prostate Cancer Mortality: A Systematic Review and Dose-Response Meta-Analysis of 280,199 Patients. Cancers 2021, 13, 4169. https://doi.org/10.3390/cancers13164169
Rivera-Izquierdo M, Pérez de Rojas J, Martínez-Ruiz V, Pérez-Gómez B, Sánchez M-J, Khan KS, Jiménez-Moleón JJ. Obesity as a Risk Factor for Prostate Cancer Mortality: A Systematic Review and Dose-Response Meta-Analysis of 280,199 Patients. Cancers. 2021; 13(16):4169. https://doi.org/10.3390/cancers13164169
Chicago/Turabian StyleRivera-Izquierdo, Mario, Javier Pérez de Rojas, Virginia Martínez-Ruiz, Beatriz Pérez-Gómez, María-José Sánchez, Khalid Saeed Khan, and José Juan Jiménez-Moleón. 2021. "Obesity as a Risk Factor for Prostate Cancer Mortality: A Systematic Review and Dose-Response Meta-Analysis of 280,199 Patients" Cancers 13, no. 16: 4169. https://doi.org/10.3390/cancers13164169