
Reference Values to Assess Hemodilution and Warn of Potential False-Negative Minimal Residual Disease Results in Myeloma

 , , , ,
, , , ,  , , ,
, , ,  , and
on behalf of the PETHEMA/GEM Cooperative Group and EuroFlow
, and
on behalf of the PETHEMA/GEM Cooperative Group and EuroFlow
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Treatment
2.2. Sample Collection
2.3. Assessment of MRD and Other BM Cell Types
2.4. Statistical Analyses
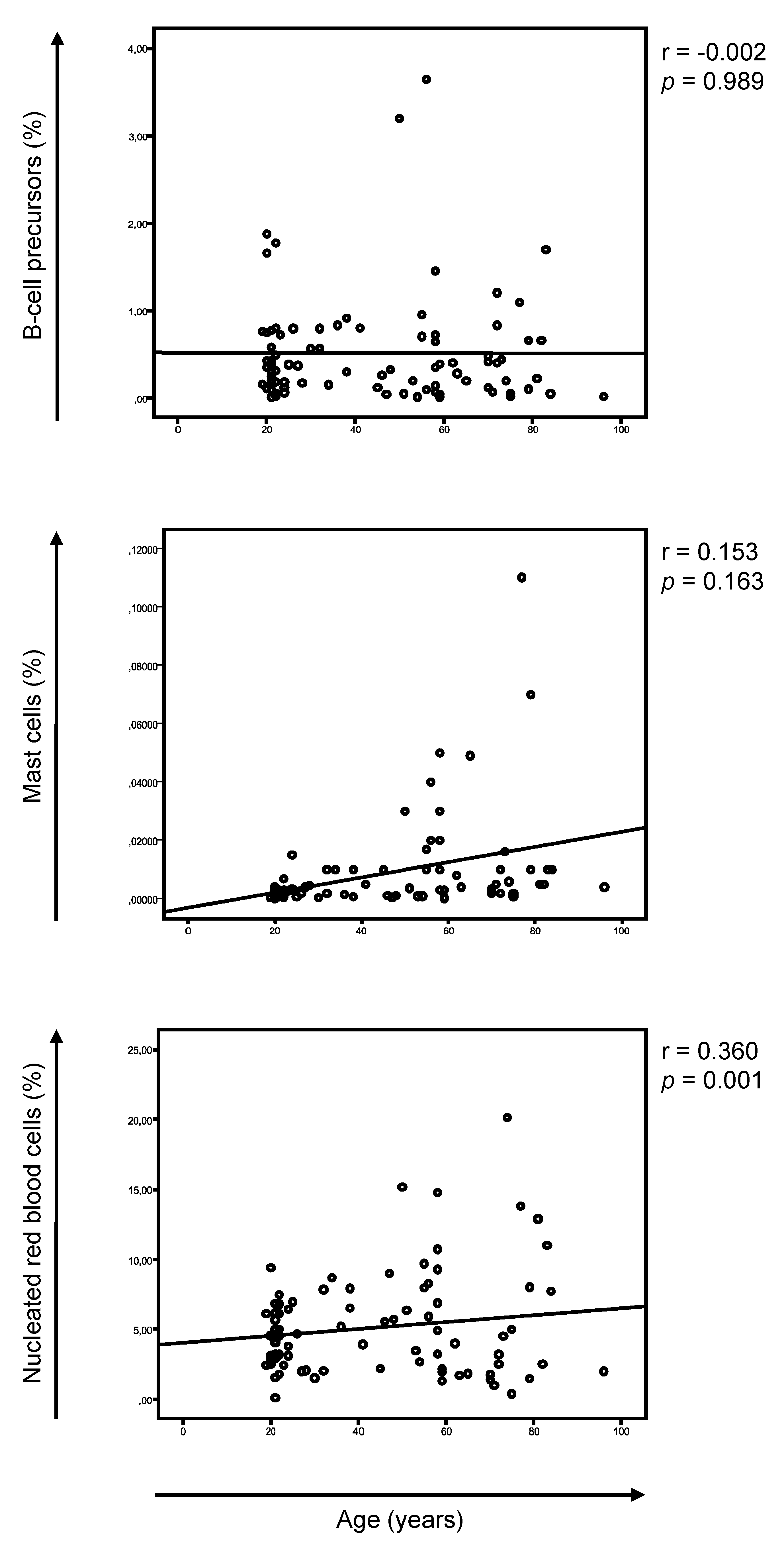
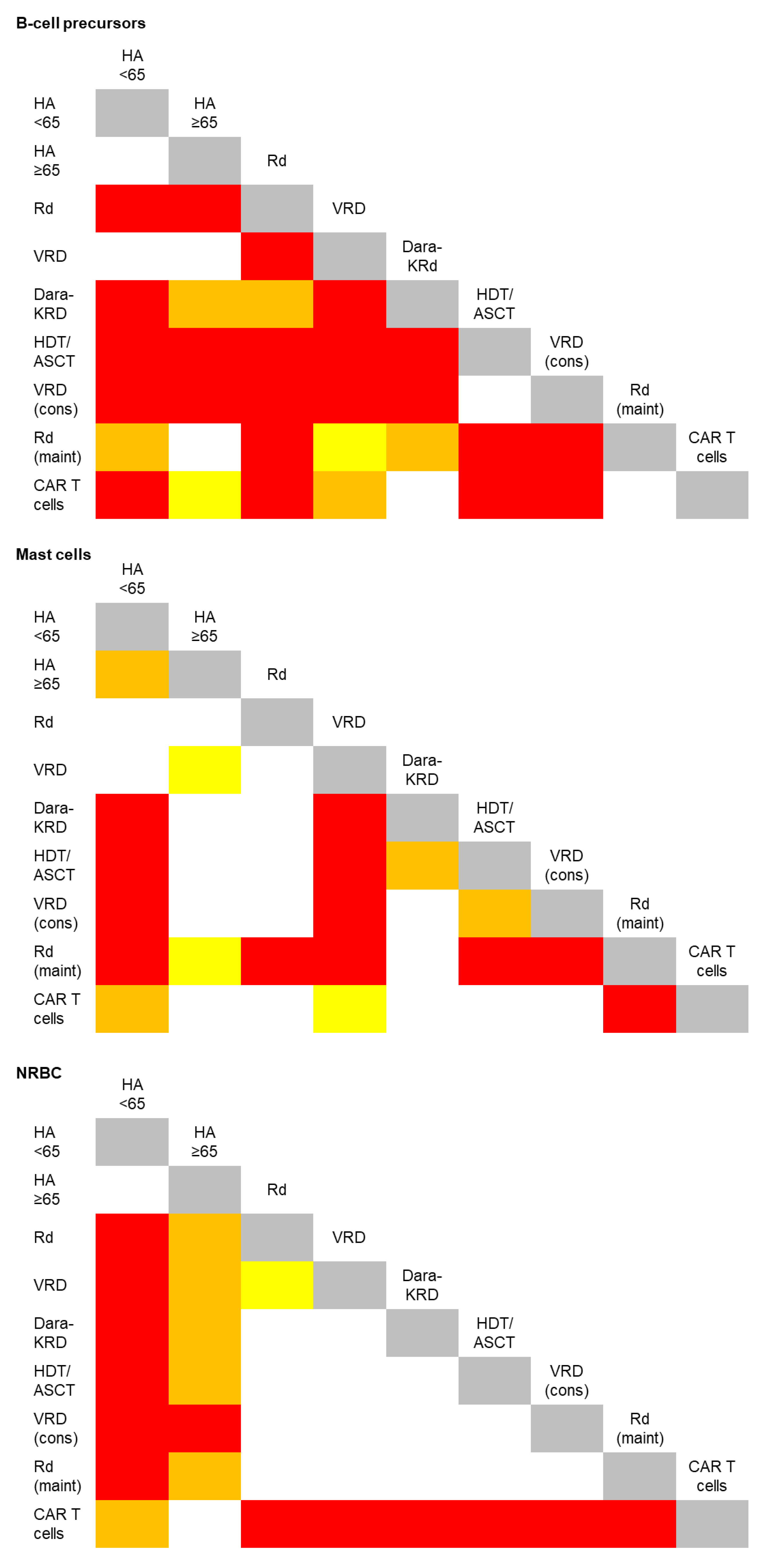
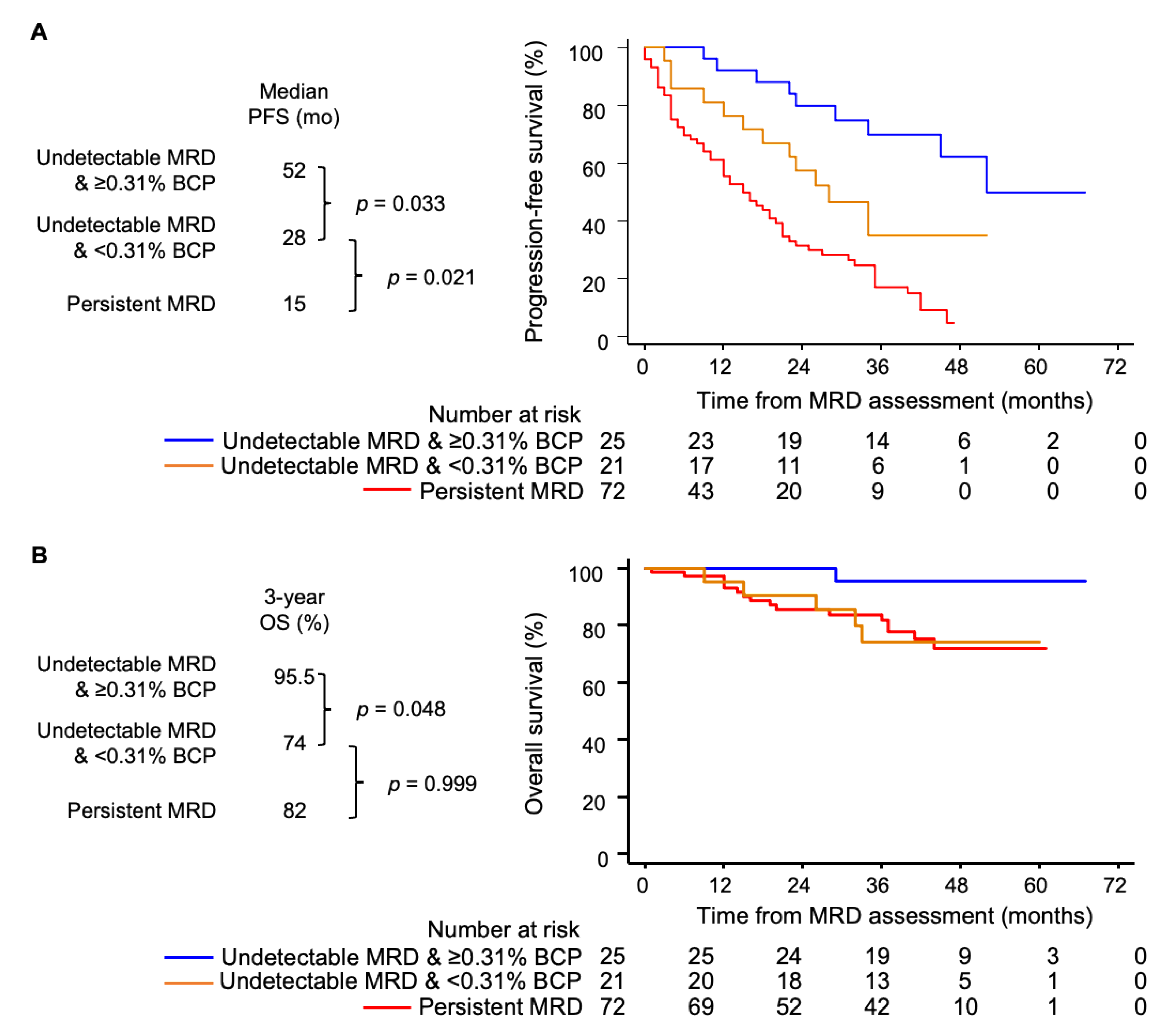
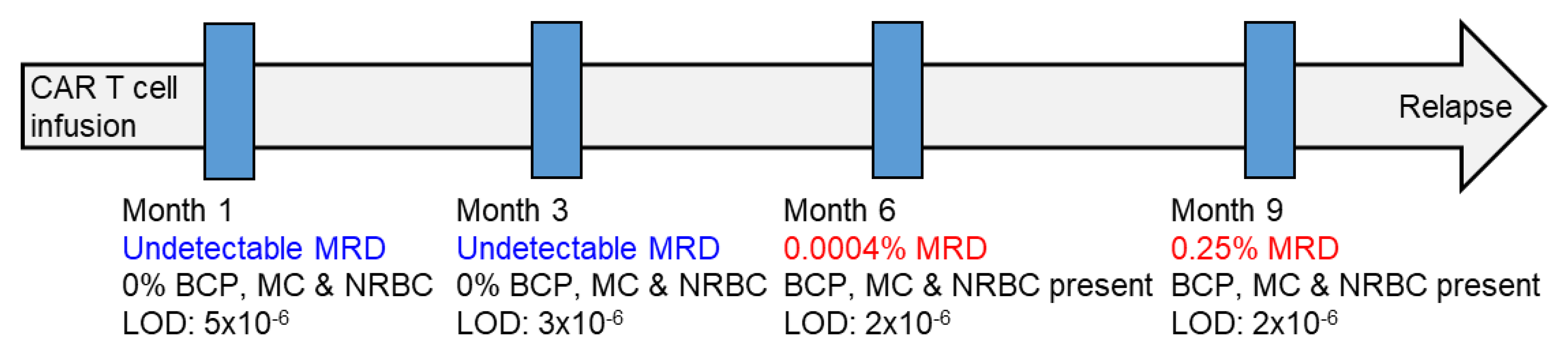
3. Results and Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Oliva, S.; D’Agostino, M.; Boccadoro, M.; Larocca, A. Clinical Applications and Future Directions of Minimal Residual Disease Testing in Multiple Myeloma. Front. Oncol. 2020, 10, 1. [Google Scholar] [CrossRef] [PubMed]
- Burgos, L.; Puig, N.; Cedena, M.T.; Mateos, M.V.; Lahuerta, J.J.; Paiva, B.; San-Miguel, J.F. Measurable residual disease in multiple myeloma: Ready for clinical practice? J. Hematol. Oncol. 2020, 13, 82. [Google Scholar] [CrossRef]
- Costa, L.J.; Derman, B.A.; Bal, S.; Sidana, S.; Chhabra, S.; Silbermann, R.; Ye, J.C.; Cook, G.; Cornell, R.F.; Holstein, S.A.; et al. International harmonization in performing and reporting minimal residual disease assessment in multiple myeloma trials. Leukemia 2021, 35, 18–30. [Google Scholar] [CrossRef] [PubMed]
- Moreau, P.; Attal, M.; Hulin, C.; Arnulf, B.; Belhadj, K.; Benboubker, L.; Béné, M.C.; Broijl, A.; Caillon, H.; Caillot, D.; et al. Bortezomib, thalidomide, and dexamethasone with or without daratumumab before and after autologous stem-cell transplantation for newly diagnosed multiple myeloma (CASSIOPEIA): A randomised, open-label, phase 3 study. Lancet 2019, 394, 29–38. [Google Scholar] [CrossRef]
- Mateos, M.-V.; Dimopoulos, M.A.; Cavo, M.; Suzuki, K.; Jakubowiak, A.; Knop, S.; Doyen, C.; Lucio, P.; Nagy, Z.; Kaplan, P.; et al. Daratumumab plus Bortezomib, Melphalan, and Prednisone for Untreated Myeloma. N. Engl. J. Med. 2018, 378, 518–528. [Google Scholar] [CrossRef]
- Facon, T.; Lee, J.H.; Moreau, P.; Niesvizky, R.; Dimopoulos, M.; Hajek, R.; Pour, L.; Jurczyszyn, A.; Qiu, L.; Klippel, Z.; et al. Carfilzomib or bortezomib with melphalan-prednisone for transplant-ineligible patients with newly diagnosed multiple myeloma. Blood 2019, 133, 1953–1963. [Google Scholar] [CrossRef] [PubMed]
- Munshi, N.C.; Avet-Loiseau, H.; Anderson, K.C.; Neri, P.; Paiva, B.; Samur, M.; Dimopoulos, M.; Kulakova, M.; Lam, A.; Hashim, M.; et al. A large meta-analysis establishes the role of MRD negativity in long-term survival outcomes in patients with multiple myeloma. Blood Adv. 2020, 4, 5988–5999. [Google Scholar] [CrossRef]
- Facon, T.; Kumar, S.; Plesner, T.; Orlowski, R.Z.; Moreau, P.; Bahlis, N.; Basu, S.; Nahi, H.; Hulin, C.; Quach, H.; et al. Daratumumab plus Lenalidomide and Dexamethasone for Untreated Myeloma. N. Engl. J. Med. 2019, 380, 2104–2115. [Google Scholar] [CrossRef] [PubMed]
- Dimopoulos, M.A.; Oriol, A.; Nahi, H.; San-Miguel, J.; Bahlis, N.J.; Usmani, S.Z.; Rabin, N.; Orlowski, R.Z.; Komarnicki, M.; Suzuki, K.; et al. Daratumumab, Lenalidomide, and Dexamethasone for Multiple Myeloma. N. Engl. J. Med. 2016, 375, 1319–1331. [Google Scholar] [CrossRef] [Green Version]
- Attal, M.; Lauwers-Cances, V.; Hulin, C.; Leleu, X.; Caillot, D.; Escoffre, M.; Arnulf, B.; Macro, M.; Belhadj, K.; Garderet, L.; et al. Lenalidomide, Bortezomib, and Dexamethasone with Transplantation for Myeloma. N. Engl. J. Med. 2017, 376, 1311–1320. [Google Scholar] [CrossRef]
- Sanoja-Flores, L.; Flores-Montero, J.; Puig, N.; Contreras-Sanfeliciano, T.; Pontes, R.; Corral-Mateos, A.; García-Sánchez, O.; Díez-Campelo, M.; de Magalhães, R.J.P.; García-Martín, L.; et al. Blood monitoring of circulating tumor plasma cells by next generation flow in multiple myeloma after therapy. Blood 2019, 134, 2218–2222. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Lopez, J.; Wong, S.W.; Shah, N.; Bahri, N.; Zhou, K.; Sheng, Y.; Huang, C.Y.; Martin, T.; Wolf, J. Clinical value of measurable residual disease testing for assessing depth, duration, and direction of response in multiple myeloma. Blood Adv. 2020, 4, 3295–3301. [Google Scholar] [CrossRef]
- Perrot, A.; Lauwers-Cances, V.; Corre, J.; Robillard, N.; Hulin, C.; Chretien, M.L.; Dejoie, T.; Maheo, S.; Stoppa, A.M.; Pegourie, B.; et al. Minimal residual disease negativity using deep sequencing is a major prognostic factor in multiple myeloma. Blood 2018, 132, 2456–2464. [Google Scholar] [CrossRef] [Green Version]
- Paiva, B.; Puig, N.; Cedena, M.T.; Rosiñol, L.; Cordón, L.; Vidriales, M.B.; Burgos, L.; Flores-Montero, J.; Sanoja-Flores, L.; Lopez-Anglada, L.; et al. Measurable residual disease by next-generation flow cytometry in multiple myeloma. J. Clin. Oncol. 2020, 38, 784–792. [Google Scholar] [CrossRef]
- Terpos, E.; Kostopoulos, I.V.; Kastritis, E.; Ntanasis-Stathopoulos, I.; Migkou, M.; Rousakis, P.; Argyriou, A.T.; Kanellias, N.; Fotiou, D.; Eleutherakis-Papaiakovou, E.; et al. Impact of Minimal Residual Disease Detection by Next-Generation Flow Cytometry in Multiple Myeloma Patients with Sustained Complete Remission after Frontline Therapyfile:///Users/noemipuig/Documents/CALIDAD DE LAS MUESTRAS/for CANCERS/Martinez-Lopez Blood. HemaSphere 2019, 3, e300. [Google Scholar] [CrossRef] [PubMed]
- Moreau, P.; Attal, M.; Caillot, D.; Macro, M.; Karlin, L.; Garderet, L.; Facon, T.; Benboubker, L.; Escoffre-Barbe, M.; Stoppa, A.M.; et al. Prospective Evaluation of Magnetic Resonance Imaging and [18F] Fluorodeoxyglucose Positron Emission Tomography-Computed Tomography at Diagnosis and Before Maintenance Therapy in Symptomatic PatientsWith Multiple Myeloma Included in the IFM/DFCI 2009 Trial. J. Clin. Oncol. 2017, 35, 2911–2918. [Google Scholar] [CrossRef]
- Rasche, L.; Alapat, D.; Kumar, M.; Gershner, G.; McDonald, J.E.; Wardell, C.P.; Choudhury, S.R.; van Hemert, R.L.; Epstein, J.; Williams, A.F. Combination of flow cytometry and functional imaging for monitoring of residual disease in myeloma. Leukemia 2019, 33, 1713–1722. [Google Scholar] [CrossRef] [PubMed]
- Rosiñol, L.; Oriol, A.; Rios, R.; Sureda, A.; Blanchard, M.J.; Hernández, M.T.; Martínez-Martínez, R.; Moraleda, J.M.; Jarque, I.; Bargay, J.; et al. Bortezomib, lenalidomide, and dexamethasone as induction therapy prior to autologous transplant in multiple myeloma. Blood 2019, 134, 1337–1345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puig, N.; Hernández, M.T.; Rosiñol, L.; González, E.; de Arriba, F.; Oriol, A.; González-Calle, V.; Escalante, F.; de la Rubia, J.; Gironella, M.; et al. Lenalidomide and dexamethasone with or without clarithromycin in patients with multiple myeloma ineligible for autologous transplant: A randomized trial. Blood Cancer J. 2021, 11, 101. [Google Scholar] [CrossRef] [PubMed]
- Flores-Montero, J.; Sanoja-Flores, L.; Paiva, B.; Puig, N.; García-Sánchez, O.; Böttcher, S.; Van Der Velden, V.H.J.; Pérez-Morán, J.J.; Vidriales, M.B.; García-Sanz, R.; et al. Next Generation Flow for highly sensitive and standardized detection of minimal residual disease in multiple myeloma. Leukemia 2017, 31, 2094–2103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paiva, B.; Cedena, M.T.; Puig, N.; Arana, P.; Vidriales, M.B.; Cordon, L.; Flores-Montero, J.; Gutierrez, N.C.; Martín-Ramos, M.L.; Martinez-Lopez, J.; et al. Minimal residual disease monitoring and immune profiling in multiple myeloma in elderly patients. Blood 2016, 127, 3165–3174. [Google Scholar] [CrossRef]
- Mateos, M.-V.; Martinez-Lopez, J.; Hernandez, M.-T.; Ocio, E.-M.; Rosinol, L.; Martinez, R.; Teruel, A.-I.; Gutierrez, N.C.; Martin Ramos, M.-L.; Oriol, A.; et al. Sequential vs. alternating administration of VMP and Rd in elderly patients with newly diagnosed MM. Blood 2016, 127, 420–425. [Google Scholar] [CrossRef] [Green Version]
- Sanoja-Flores, L.; Flores-Montero, J.; Garcés, J.J.; Paiva, B.; Puig, N.; García-Mateo, A.; García-Sánchez, O.; Corral-Mateos, A.; Burgos, L.; Blanco, E.; et al. Next generation flow for minimally-invasive blood characterization of MGUS and multiple myeloma at diagnosis based on circulating tumor plasma cells (CTPC). Blood Cancer J. 2018, 8, 117. [Google Scholar] [CrossRef] [Green Version]
- Arana, P.; Paiva, B.; Cedena, M.T.; Puig, N.; Cordon, L.; Vidriales, M.B.; Gutierrez, N.C.; Chiodi, F.; Burgos, L.; Anglada, L.L.; et al. Prognostic value of antigen expression in multiple myeloma: A PETHEMA/GEM study on 1265 patients enrolled in four consecutive clinical trials. Leukemia 2018, 32, 971–978. [Google Scholar] [CrossRef] [PubMed]
- Puig, N.; Paiva, B.; Lasa, M.; Burgos, L.; Perez, J.J.; Merino, J.; Moreno, C.; Vidriales, M.B.; Toboso, D.G.; Cedena, M.T.; et al. Flow cytometry for fast screening and automated risk assessment in systemic light-chain amyloidosis. Leukemia 2019, 33, 1256–1267. [Google Scholar] [CrossRef] [PubMed]
- Gulla, A.; Anderson, K.C. Multiple myeloma: The (r) evolution of current therapy and a glance into the future. Haematologica 2020, 105, 2358–2367. [Google Scholar] [CrossRef]
- Van De Donk, N.W.C.J.; Richardson, P.G.; Malavasi, F. CD38 antibodies in multiple myeloma: Back to the future. Blood 2018, 131, 13–29. [Google Scholar] [CrossRef] [PubMed]
- Quach, H.; Ritchie, D.; Stewart, A.K.; Neeson, P.; Harrison, S.; Smyth, M.J.; Prince, H.M. Mechanism of action of immunomodulatory drugs (IMiDS) in multiple myeloma. Leukemia 2010, 24, 22–32. [Google Scholar] [CrossRef] [Green Version]
- Minnie, S.A.; Hill, G.R. Immunotherapy of multiple myeloma. J. Clin. Investig. 2020, 130, 1565–1575. [Google Scholar] [CrossRef]
- Raje, N.; Berdeja, J.; Lin, Y.; Siegel, D.; Jagannath, S.; Madduri, D.; Liedtke, M.; Rosenblatt, J.; Maus, M.V.; Turka, A.; et al. Anti-BCMA CAR T-Cell Therapy bb2121 in Relapsed or Refractory Multiple Myeloma. N. Engl. J. Med. 2019, 380, 1726–1737. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Healthy Adults | Multiple Myeloma | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Induction | Intensification | Maintenance | Salvage | |||||||
| <65 (N = 65) | ≥65 (N = 20) | Rd (N = 63) | VRD (N = 300) | Dara-KRd (N = 34) | HDT/ASCT (N = 364) | VRD (N = 350) | Rd (N = 232) | CAR T (N = 61) | ||
| B-cell precursors | Q25 | 0.14 | 0.08 | 0 | 0.03 | 0 | 0.92 | 0.63 | 0.02 | 0.02 |
| Median (range) | 0.35 (0.01–3.64) | 0.31 (0.02–0.66) | 0.01 (0–0.90) | 0.31 (0–10.0) | 0.05 (0–3.1) | 2.0 (0–14.5) | 1.8 (0–19.6) | 0.13 (0–10.7) | 0.12 (0–5.75) | |
| Q75 | 0.73 | 0.66 | 0.04 | 1.0 | 0.2 | 3.8 | 4.0 | 0.74 | 0.33 | |
| Mast cells | Q25 | 0.001 | 0.003 | 0 | 0.001 | 0.004 | 0.002 | 0.003 | 0.007 | 0.002 |
| Median (range) | 0.002 (0.0002–0.05) | 0.005 (0.001–0.11) | 0.0095 (0–0.14) | 0.004 (0–0.93) | 0.01 (0–0.4) | 0.006 (0–0.11) | 0.01 (0–0.26) | 0.01 (0–0.76) | 0.007 (0–0.17) | |
| Q75 | 0.007 | 0.01 | 0.03 | 0.01 | 0.04 | 0.01 | 0.02 | 0.06 | 0.01 | |
| Nucleated red blood cells | Q25 | 2.7 | 1.7 | 4.0 | 4.4 | 6.0 | 4.5 | 5.0 | 3.5 | 1.8 |
| Median (range) | 4.6 (0.1–15.2) | 2.50 (0.4–20.1) | 11.0 (0–39.0) | 7.3 (0–43.0) | 7.3 (1.8–26.4) | 8.2 (0–53.9) | 8.2 (0–53.9) | 7.5 (0–52) | 2.5 (0–28.4) | |
| Q75 | 6.8 | 7.9 | 19.3 | 12.6 | 10.8 | 13.0 | 13.8 | 12.6 | 4.5 | |
| N = 118 | MRD Status | |||
|---|---|---|---|---|
| Positive (N = 72) | Negative (N = 46) | |||
| B-cell precursors | Q25 | 0.13 | 0.18 | 0.09 |
| Median (range) | 0.42 (0–7.7) | 0.48 (0–7.7) | 0.33 (0–4.6) | |
| Q75 | 1.46 | 1.36 | 1.51 | |
| Mast cells | Q25 | 0.01 | 0.01 | 0.005 |
| Median (range) | 0.02 (0–0.55) | 0.02 (0–5.5) | 0.015 (0–0.33) | |
| Q75 | 0.07 | 0.07 | 0.07 | |
| Nucleated red blood cells | Q25 | 9.56 | 10.7 | 8.74 |
| Median (range) | 17.4 (0–50.9) | 16.0 (1.4–50.9) | 17.6 (0–45) | |
| Q75 | 26.7 | 25.2 | 28.1 | |
| Healthy Adults | Multiple Myeloma | p-Value | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Induction | Intensification | Maintenance | Salvage | |||||||
| <65 (N = 65) | ≥65 (N = 20) | Rd (N = 63) | VRD (N = 300) | Dara-KRd (N = 34) | HDT/ASCT (N = 364) | VRD (N = 350) | Rd (N = 232) | CAR T (N = 61) | ||
| BCP | 0 (0%) | 0 (0%) | 27 (45%) | 32 (11%) | 9 (26.5%) | 11 (3%) | 10 (3%) | 31 (14%) | 10 (17%) | <0.001 |
| MC | 0 (0%) | 0 (0%) | 16 (27%) | 48 (16%) | 1 (3%) | 32 (9%) | 27 (8%) | 28 (12%) | 9 (15.5%) | <0.001 |
| NRBC | 0 (0%) | 0 (0%) | 3 (5%) | 2 (0.7%) | 0 (0%) | 8 (2%) | 6 (2%) | 5 (2%) | 7 (12%) | <0.001 |
| One of three | 0 (0%) | 0 (0%) | 24 (12%) | 59 (20%) | 8 (23.5%) | 31 (8.5%) | 24 (7%) | 42 (19%) | 8 (14%) | <0.001 |
| Two of three | 0 (0%) | 0 (0%) | 11 (18%) | 10 (3%) | 1 (3%) | 1 (0.3%) | 2 (0.6%) | 8 (4%) | 3 (5%) | |
| All three | 0 (0%) | 0 (0%) | 0 (0%) | 1 (0.3%) | 0 (0%) | 6 (2%) | 5 (1.4%) | 2 (1%) | 4 (7%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Puig, N.; Flores-Montero, J.; Burgos, L.; Cedena, M.-T.; Cordón, L.; Pérez, J.-J.; Sanoja-Flores, L.; Manrique, I.; Rodríguez-Otero, P.; Rosiñol, L.; et al. Reference Values to Assess Hemodilution and Warn of Potential False-Negative Minimal Residual Disease Results in Myeloma. Cancers 2021, 13, 4924. https://doi.org/10.3390/cancers13194924
Puig N, Flores-Montero J, Burgos L, Cedena M-T, Cordón L, Pérez J-J, Sanoja-Flores L, Manrique I, Rodríguez-Otero P, Rosiñol L, et al. Reference Values to Assess Hemodilution and Warn of Potential False-Negative Minimal Residual Disease Results in Myeloma. Cancers. 2021; 13(19):4924. https://doi.org/10.3390/cancers13194924
Chicago/Turabian StylePuig, Noemí, Juan Flores-Montero, Leire Burgos, María-Teresa Cedena, Lourdes Cordón, José-Juan Pérez, Luzalba Sanoja-Flores, Irene Manrique, Paula Rodríguez-Otero, Laura Rosiñol, and et al. 2021. "Reference Values to Assess Hemodilution and Warn of Potential False-Negative Minimal Residual Disease Results in Myeloma" Cancers 13, no. 19: 4924. https://doi.org/10.3390/cancers13194924