4. Discussion
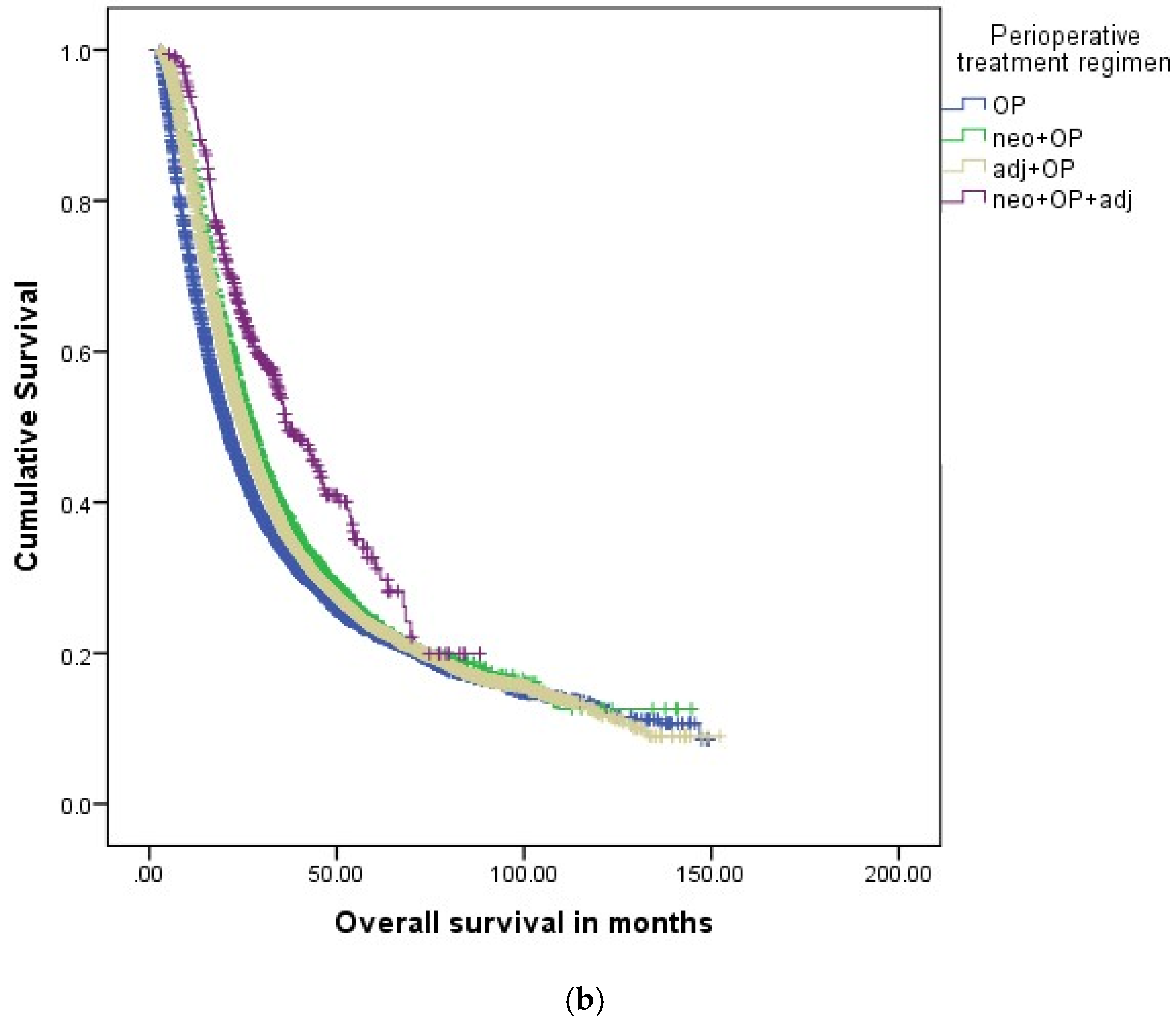
The cross-validation of perioperative therapy concepts and outcomes comparing the National Cancer Database (NCDB) and the German Cancer Registry Group of the Society of German Tumor Centers—Network for Care, Quality, and Research in Oncology, Berlin (GCRG/ADT) demonstrated that patient selection, and the use of multi-agent concepts in perioperative PDAC therapy remain widely consistent across the registries. Neoadjuvant therapy, when compared to upfront surgery, resulted in improved median overall survival for all clinical stages in both registries, while neoadjuvant radiochemotherapy (neoRCTX + OP) was not superior to neoadjuvant chemotherapy alone (neoCTX + OP). This is the first study to show that neoadjuvant therapy combined with adjuvant therapy (neo + OP + adj) was associated with improved overall survival rates when compared to neoadjuvant (neo + OP) or adjuvant therapy alone (OP + adj) in both stages IA-IIA and IIB-III PDAC after propensity score-based matching.
National cancer registries have been established over the past years to serve as a measure to assure quality control and to evaluate treatment effects and outcomes on a nationwide scale [
9,
13]. These registries provide major insights into current treatment practice for PDAC, among other cancer entities. Beyond evaluation of clinical practice standards, these registries provide platforms to validate treatment effects observed in clinical trials on “real-world” data with nationwide coverage [
9]. The large-scale set-up of national registries makes them ideal databases to address current controversies of perioperative therapy in PDAC to gain insights into treatment outcomes beyond the settings of clinical trials. While national registries are increasingly used to evaluate PDAC treatment effects on a national level [
13,
14,
15], very few international cross-validations of registry studies have been performed so far [
8,
16].
The German Cancer Registry Group of the Society of German Tumor Centers—Network for Care, Quality, and Research in Oncology, Berlin (GCRG/ADT) is a joint organization of the German Cancer Centers and combines the regional German cancer registries in the national German cancer registry covering all patients treated for any cancer entity in Germany [
17,
18]. The U.S.-American NCDB is sponsored by the American College of Surgeons and the Commission on Cancer and represents a clinical oncology database sourced from hospital registry data. The NCDB covers 70% of the newly diagnosed cancer cases in the United States [
19,
20]. These two registries cover the main part of the respective PDAC patient national caseloads and provide large-scale cohorts to compare perioperative treatment concepts and outcomes in patients with clinical stage IA-III PDAC. Patient selection for different perioperative treatment concepts was similar in both registries. Patients selected for neoadjuvant regimens were younger than those receiving adjuvant therapy or surgery alone in both registries. In the NCDB registry, patients receiving OP alone were more likely to have a higher co-morbidity index when compared to patients receiving perioperative treatment. This clinical practice reflects statements by both the U.S.-American National Comprehensive Cancer Network (NCCN) Guideline Pancreatic Adenocarcinoma and the German S3 guideline for the treatment of pancreatic cancer [
21,
22]. Both national guidelines recommend deescalating or avoiding perioperative therapy in elderly or multi-morbid PDAC patients if reasonable.
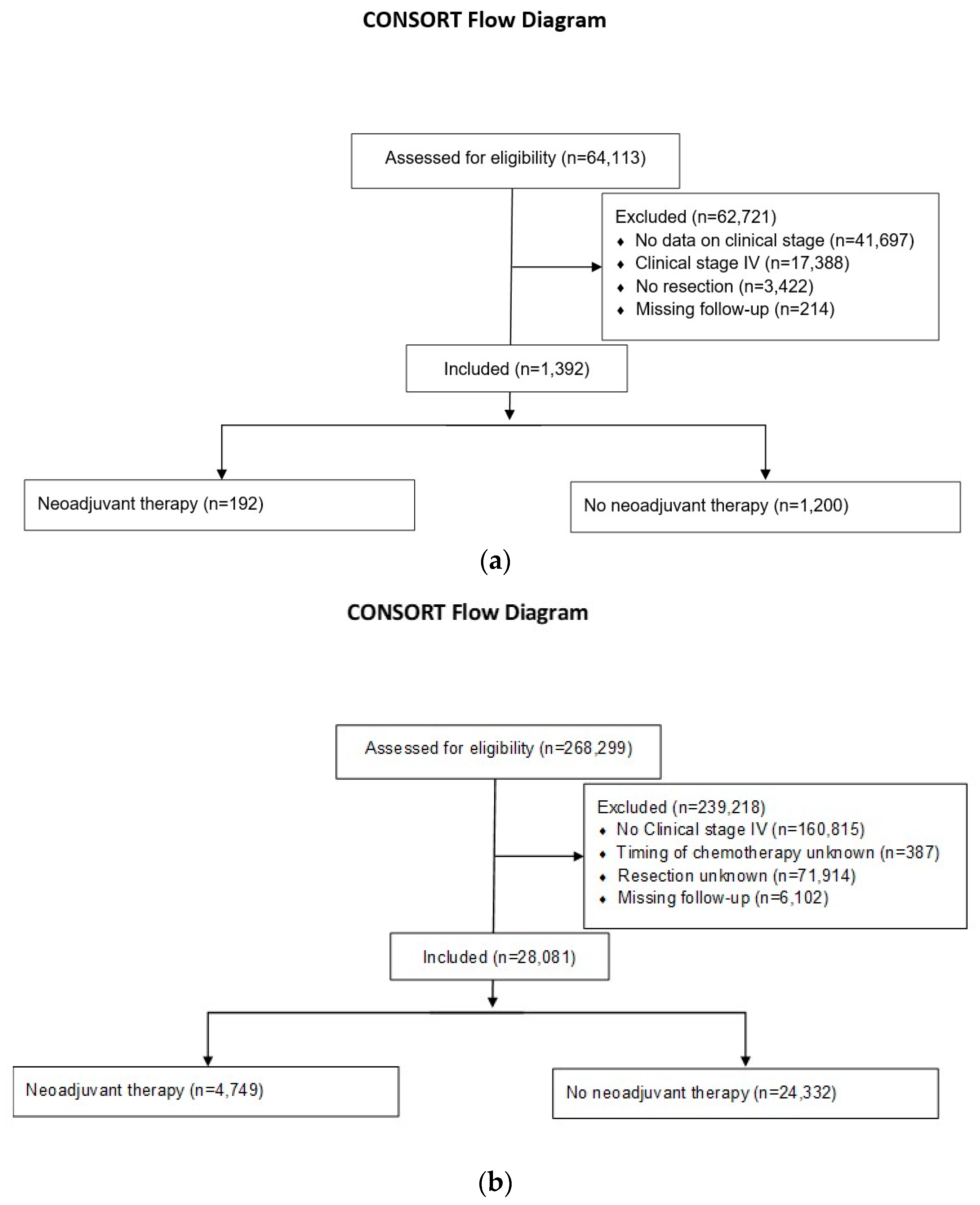
Neoadjuvant therapy was performed in 12% of the patients in NCDB as compared to 3% in the GCRG/ADT registry for stages IA-IIA, and 19% as compared to 10% for the stages IIB-III. Moreover, the total numbers of patients in the study with neo + OP or neo + OP + adj for stage IA-III are much lower for the GCRG/ADT registry (
n = 192) as compared to the NCDB (
n = 4749). This difference is most likely associated with divergent recommendations in national treatment guidelines. While neoadjuvant therapy was already recommended by the U.S.-American NCCN guideline for PDAC in 2014 in selected patients with borderline resectable PDAC, it is currently only considered an option in high-risk resectable PDAC patients and is encouraged in the context of clinical trials [
22,
23]. The German S3 guideline for the treatment of pancreatic cancer recommends more restricted use of neoadjuvant therapy [
21]. While neoadjuvant therapy may be considered in PDAC patients with locally advanced disease, it is not recommended in resectable patients outside of clinical trials. Thus, neoadjuvant therapy is not routinely performed in Germany, and total numbers of PDAC patients who underwent neoadjuvant therapy entered into the GCRG/ADT registry are lower when compared to the NCDB. Furthermore, adjuvant therapy is recommended for all stages by the German S3-guideline. Therefore, adjuvant therapy, in addition to neoadjuvant therapy, is relatively common in Germany as compared to the U.S. Despite these differences, the use of multi-agent chemotherapy remained similar in both registries. Chemotherapy agents used in perioperative concepts are not available from the NCDB and still incomplete for the GCRG/ADT registry. However, both registries provide data regarding the use of single- and multi-agent chemotherapy. Interestingly, the current study showed improved survival rates with neoadjuvant therapy as compared to adjuvant therapy. In the context of neoadjuvant therapy, multi-agent therapies were the most common strategy in both registries. These combination therapies involve gemcitabine and nab-paclitaxel or FOLFIRINOX, which proved superior to standard single-agent therapies [
20]. For adjuvant therapy, the majority of patients in both registries received single-agent therapy. The most common single-agent strategy for PDAC involves gemcitabine alone [
21]. Recent studies showed superior long-term outcomes for multi-agent therapies such as gemcitabine and nab-paclitaxel or FOLFIRINOX as compared to single-agent therapies such as gemcitabine alone [
7]. Therefore, the higher percentage of patients receiving single-agent therapies in the adjuvant as compared to the neoadjuvant setting might explain improved overall survival rates for patients with neoadjuvant as compared to adjuvant therapy.
In general, overall survival times were shorter for patients from the GCRG/ADT registry as compared to the NCDB; the most considerable difference is found in the group of patients with neoadjuvant and adjuvant therapy (21.3 months versus 35.4 months). There are several potential explanations for this discrepancy. First, the study period for the GCRG-ADT registry started in 2000, while it only started in 2004 for the NCDB. Therefore, it may be hypothesized that the GCRG-ADT registry includes more patients with currently outdated chemotherapy concepts. Furthermore, the first-line chemotherapy agents used in neoadjuvant and adjuvant settings differ in the United States and in Germany. While gemcitabine with or without capecitabine is still recommended by the German S3-guideline, the NCCN started recommending multi-agent therapies such as gemcitabine and nab-paclitaxel, and FOLFIRINOX that proved superior in terms of oncological outcomes [
21].
Neoadjuvant therapy has become an important part of PDAC perioperative therapy over the past years [
3,
5,
7,
20,
24]. The main rationale for neoadjuvant therapy in PDAC is to achieve a downstaging of tumors and to improve resectability [
24,
25,
26]. Our study demonstrated impressive downstaging of tumors in terms of T and N stage for patients undergoing neoadjuvant therapy across registries. Despite successful shrinkage of tumors, tumor burden was not eliminated by neoadjuvant therapy in the vast majority of patients. Recent consensus guidelines suggest focusing on the remaining tumor burden as an important parameter to determine the efficacy of neoadjuvant therapy [
27]. While growing evidence supports the benefits of neoadjuvant therapy, the ideal sequence and treatment regimen of perioperative therapy has yet to be determined [
7,
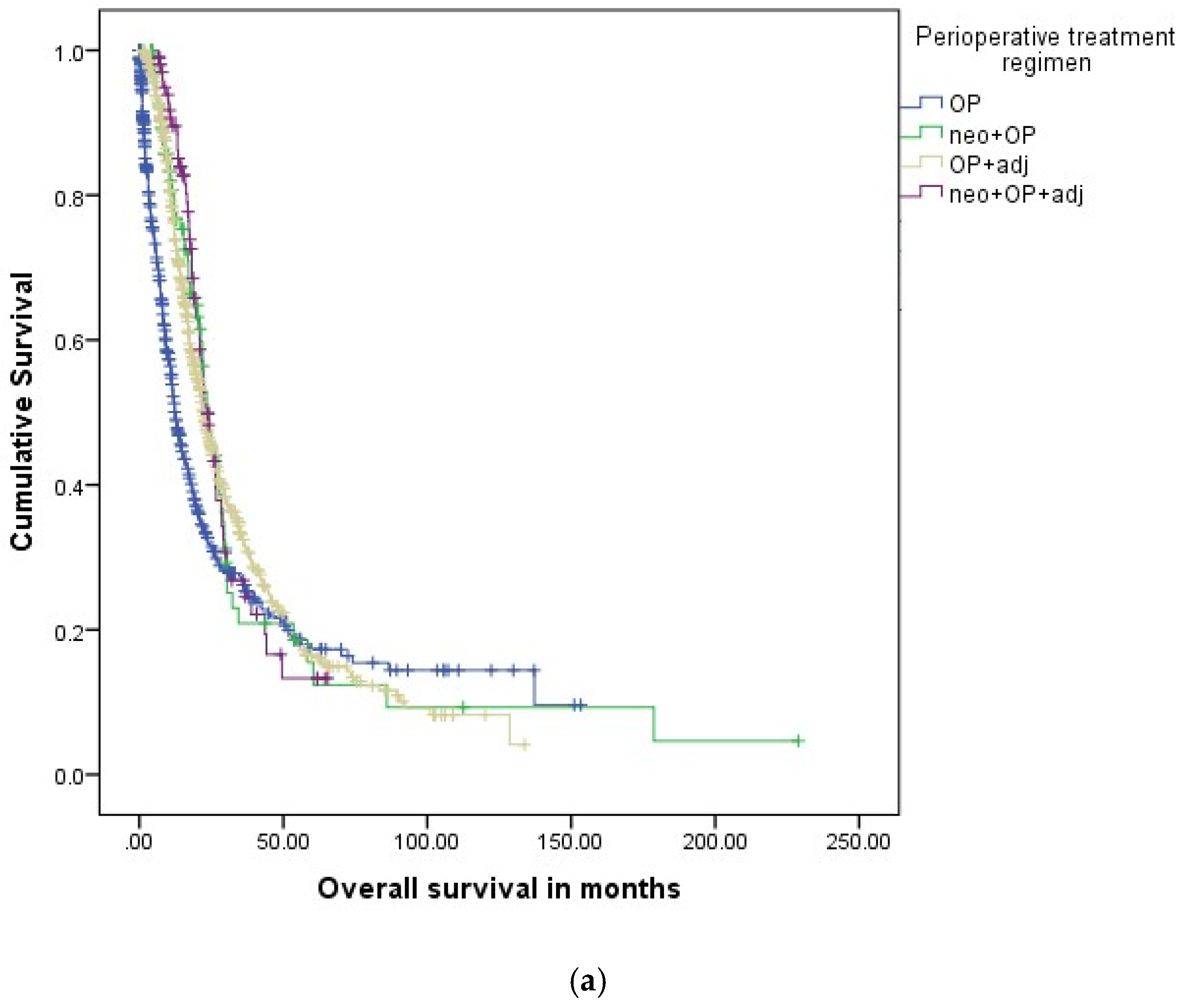
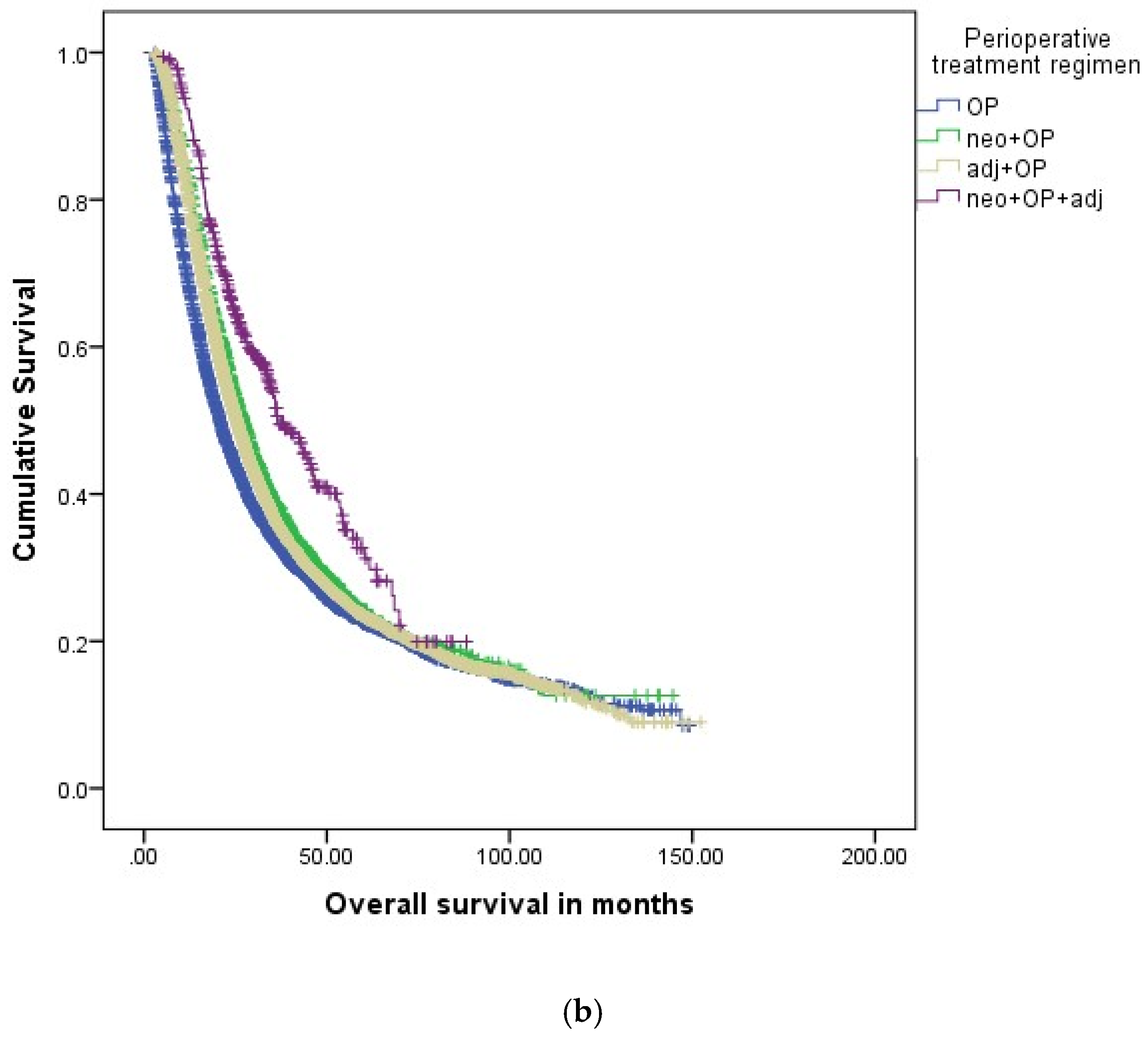
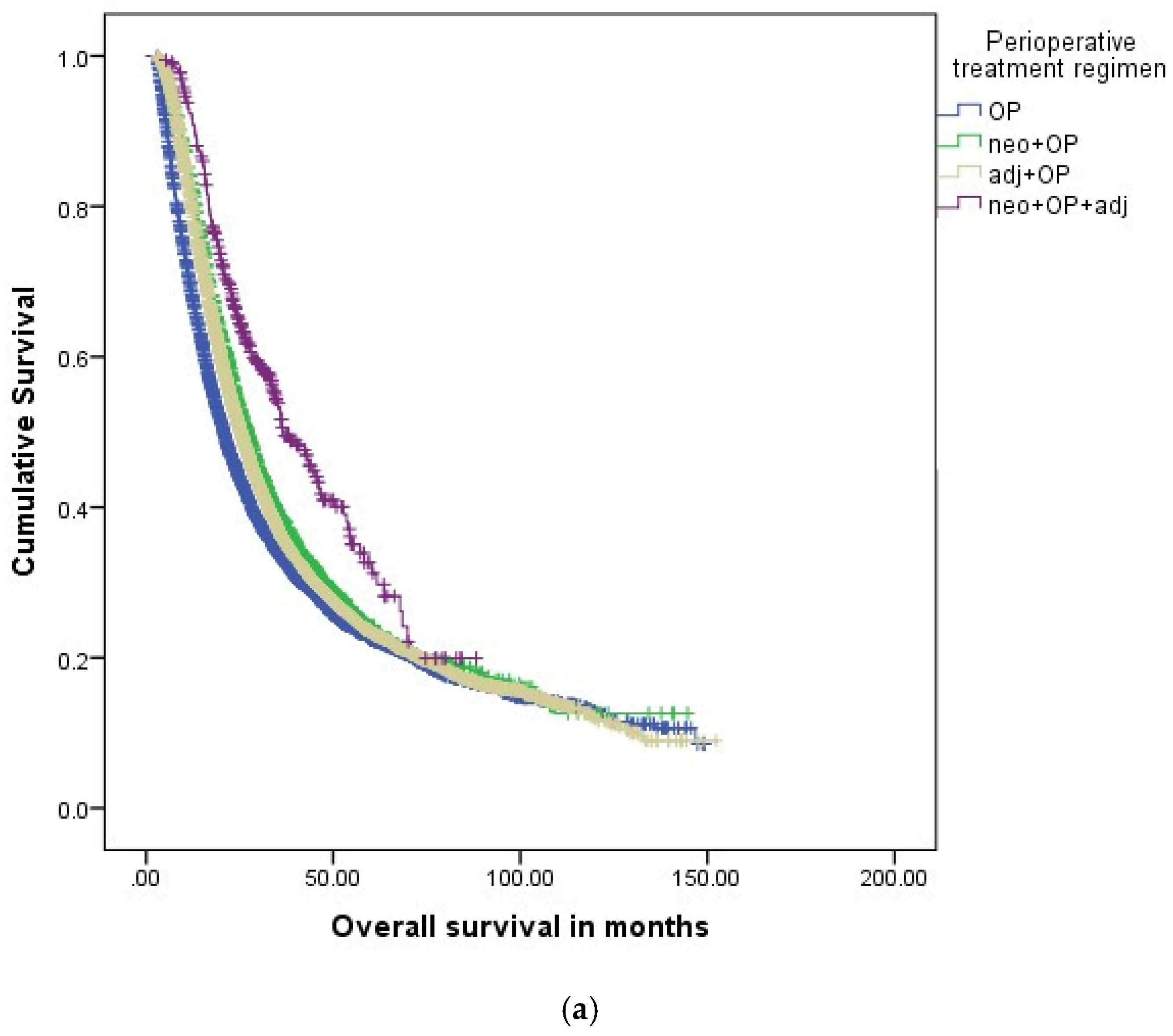
28]. It is unclear whether neoadjuvant therapy is superior to adjuvant therapy or if a combination of neoadjuvant and adjuvant therapy is more beneficial than each of these options alone. This study is the first to assess the sequence of perioperative therapy of stage IA-III PDAC patients. Neoadjuvant therapy was associated with prolonged overall survival as compared to adjuvant therapy for both clinical stage IA-IIA and IIB-III PDAC in the NCDB registry (27.1 m vs. 25.3 m and 25.8 m vs. 20.8 m, respectively). These results were not confirmed in the GCRG/ADT, and overall survival was similar for patients with neoadjuvant and adjuvant therapy across all stages. The combination of neoadjuvant and adjuvant therapy was associated with considerably higher overall survival rates than either perioperative treatment alone for clinical stage IA-IIA (36.6 m) and IIB-III (28.6 m). These results were confirmed in the GCRG/ADT registry showing prolonged overall survival rates for all patients and for patients with stage IIB-III but not stage IA-IIA. It may be speculated that the analysis was underpowered due to low absolute patient numbers in the groups of neoadjuvant therapy alone and even more so for combined neoadjuvant and adjuvant therapy. Very few other studies have addressed the issue of combining neoadjuvant and adjuvant therapy in PDAC. Watson et al. performed an analysis of clinical stage 0-II PDAC patients from the NCDB and found improved overall survival with neoadjuvant and adjuvant therapy as compared to neoadjuvant therapy alone [
28]. Drake et al. found that additional adjuvant therapy is particularly beneficial in patients with microscopically incomplete R1 resection [
29].
While neoadjuvant therapy was associated with prolonged overall survival, this study failed to demonstrate the benefit of neoadjuvant radiochemotherapy over neoadjuvant chemotherapy alone for both registries. Radiotherapy is often integrated into standard neoadjuvant concepts in the United States and is recommended by the current NCCN guideline [
22]. In Germany, however, the use of radiotherapy in the context of neoadjuvant or adjuvant therapy for PDAC is discouraged by the German S3 guideline for the treatment of pancreatic cancer [
21]. While there is evidence supporting neoadjuvant chemotherapy with and without radiochemotherapy, respectively, head-to-head comparisons of neoadjuvant radiochemotherapy versus neoadjuvant chemotherapy alone are rare [
7]. Trinh et al. assessed neoadjuvant chemotherapy alone versus neoadjuvant chemoradiation for resectable and borderline resectable PDAC and found no difference in overall survival [
30]. An analysis of the NCDB for the time period from 2004 to 2013 also failed to show a difference in overall survival for resected PDAC with neoadjuvant radiochemotherapy versus neoadjuvant chemotherapy alone [
25].
While perioperative therapy primarily consists of classical single- or multi-agent chemotherapy regimens, a growing body of evidence suggests that PDAC tumors are heterogeneous and more individualized approaches are warranted [
31,
32,
33,
34]. Multiple PDAC therapeutic targets have been identified, including mismatch repair deficiency, microsatellite instability, or BRCA mutations [
31,
32]. Immunotherapy might help to improve long-term outcomes in these and other patient subgroups [
27]. Future perioperative therapy should take molecular tumor characteristics into account and involve not only multi-agent chemotherapies but also combined immunotherapy.
This study has several limitations. Details about chemotherapy agents were not available from the NCDB and only partially available from the GCRG/ADT registry. Molecular marker profiles or mutational analyses could also not be derived from the registries. Therefore, detailed analysis of perioperative therapy regimens and distinct agents and individualized therapy could not be performed. A further limitation is a change in national treatment guidelines over the course of the study period, leading to the inclusion of patients with different perioperative therapy regimens and indications. The national registries are derived from population-based retrospective databases, and inaccuracy in data collection cannot be ruled out. Furthermore, patients with missing data had to be excluded introducing potential selection bias that is difficult to account for at the scale of this study. However, the national coverage of PDAC cases is about 70% for the NCDB and 100% for the GCRG/ADT registry. Therefore, these databases provide two of the largest national PDAC cohorts to study perioperative therapy on “real-world data”.


 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}