
Prolonged Exposure to Oxaliplatin during HIPEC Improves Effectiveness in a Preclinical Micrometastasis Model

 , , , , , , ,
, , , , , , , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Samples
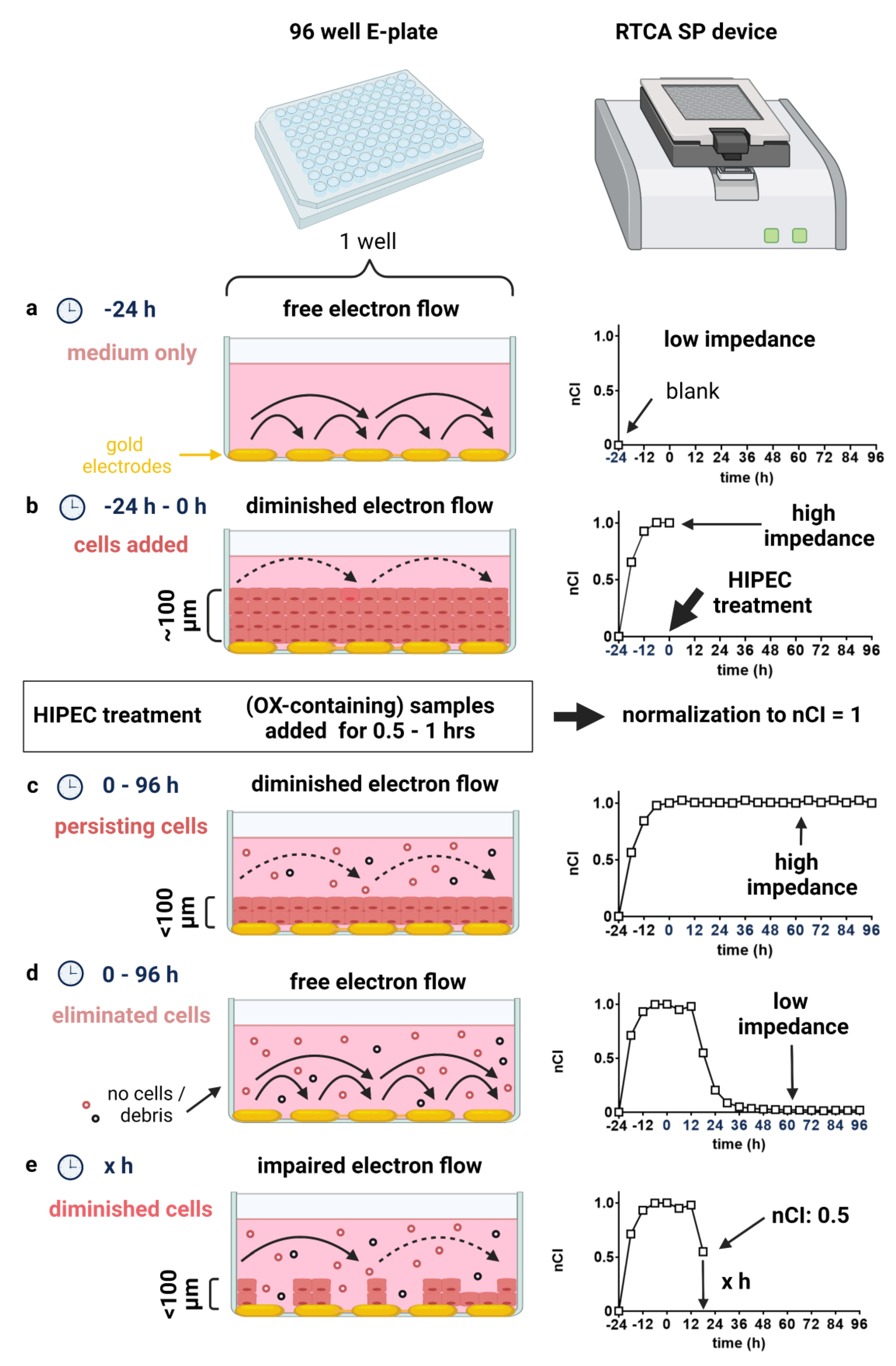
2.2. Impedance-Based Real-Time Cell Analysis (RTCA)
2.3. CellTiter-Blue® (CTB) Cell Viability Assay
2.4. Sulforhodamine B (SRB) Cytotoxicity Assay
2.5. Microscopy
2.6. Flow Cytometry
3. Results
3.1. Monitoring HIPEC Effects in a Micrometastasis Model in Real-Time by Impedance Assessment
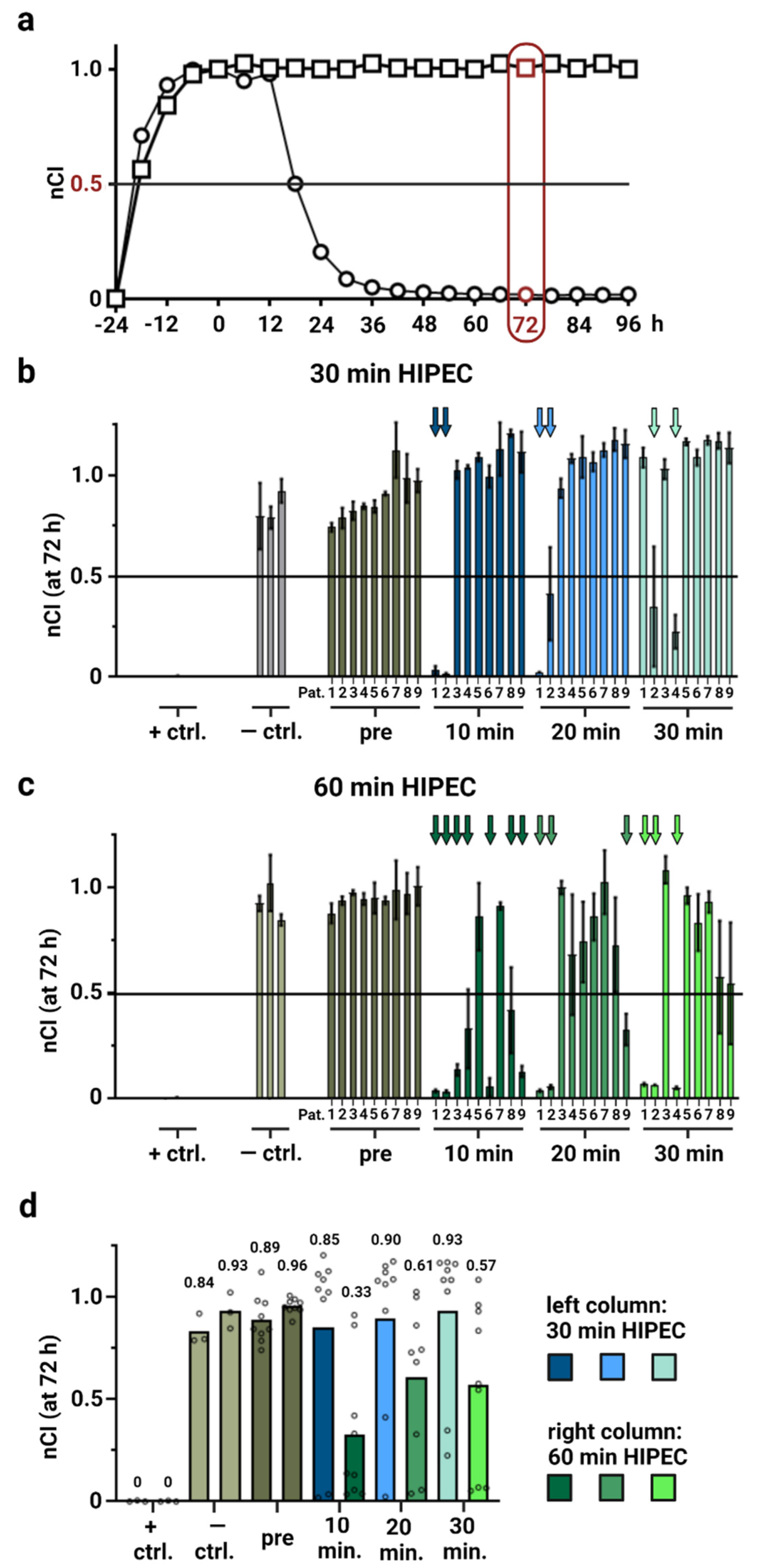
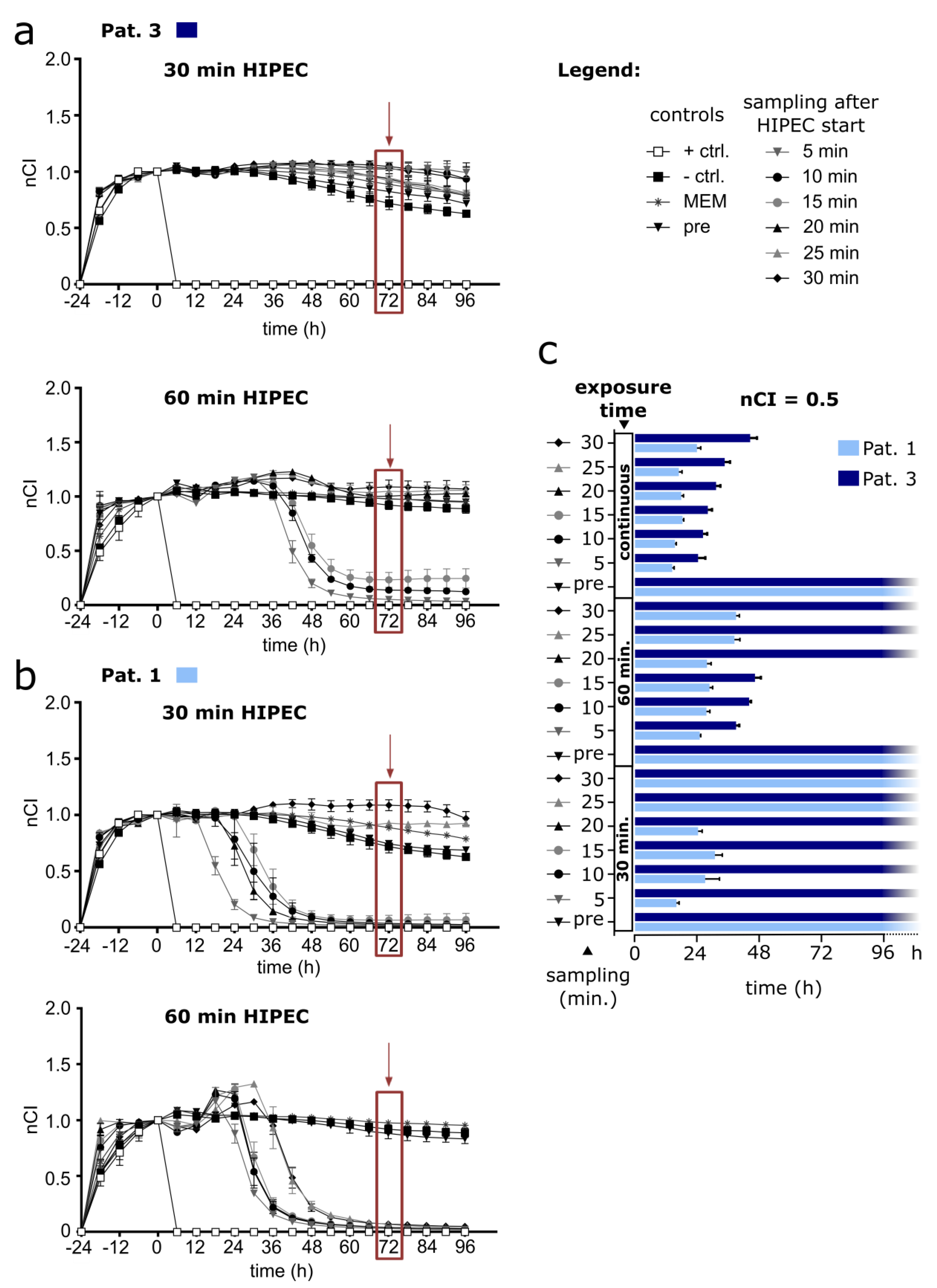
3.2. Modelling HIPEC with Patient Samples Displays Heterogeneous Effectivity (by RTCA Assay) in a Micrometastasis Model
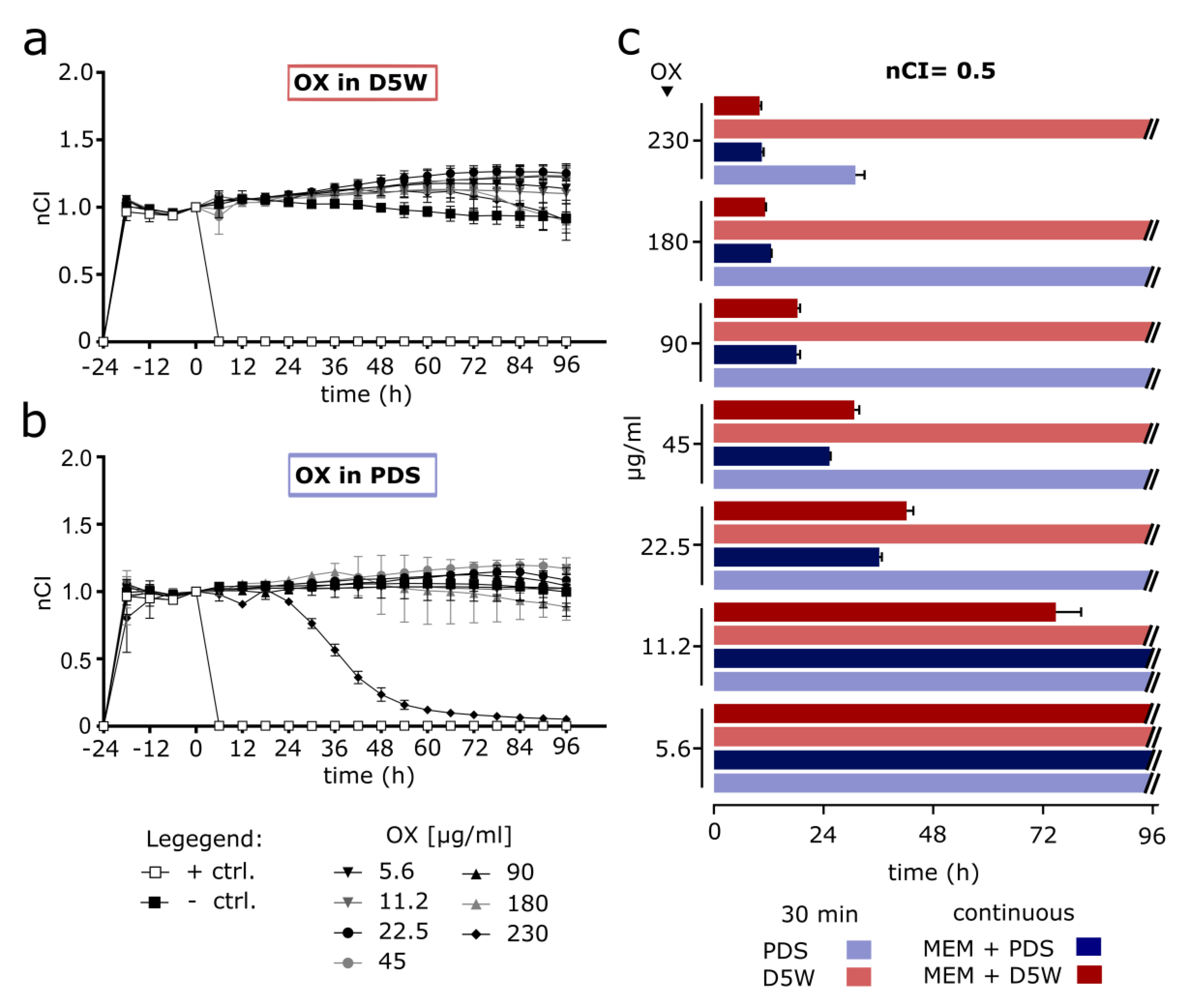
3.3. Short-Term HIPEC with OX-Containing Solutions Prepared According to Clinically Established Protocols Proves Ineffective in Modelled Micrometastases (RTCA Assay)
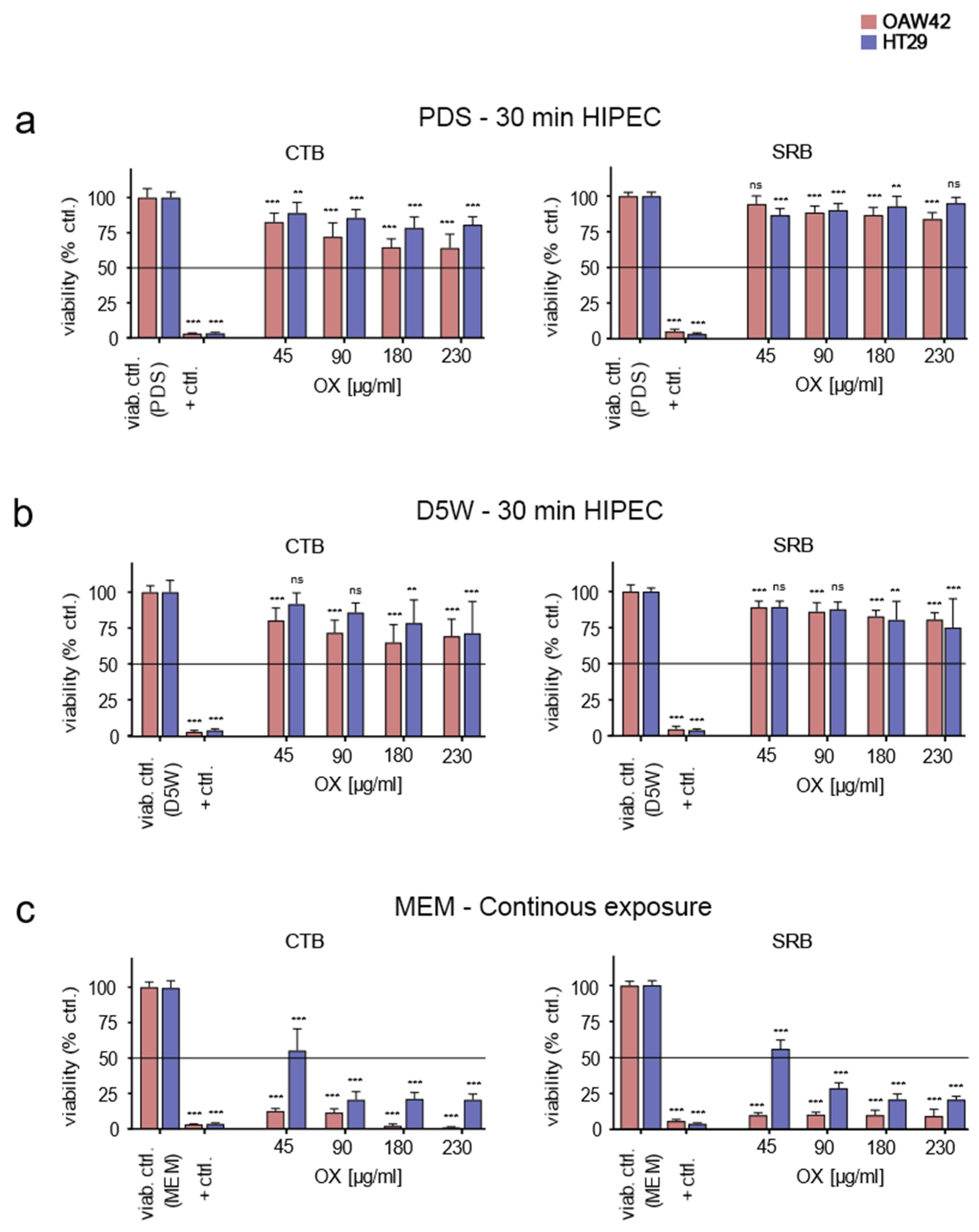
3.4. Confirming RTCA Results with Prepared OX-Containing Solutions by Classical End-Points Assays
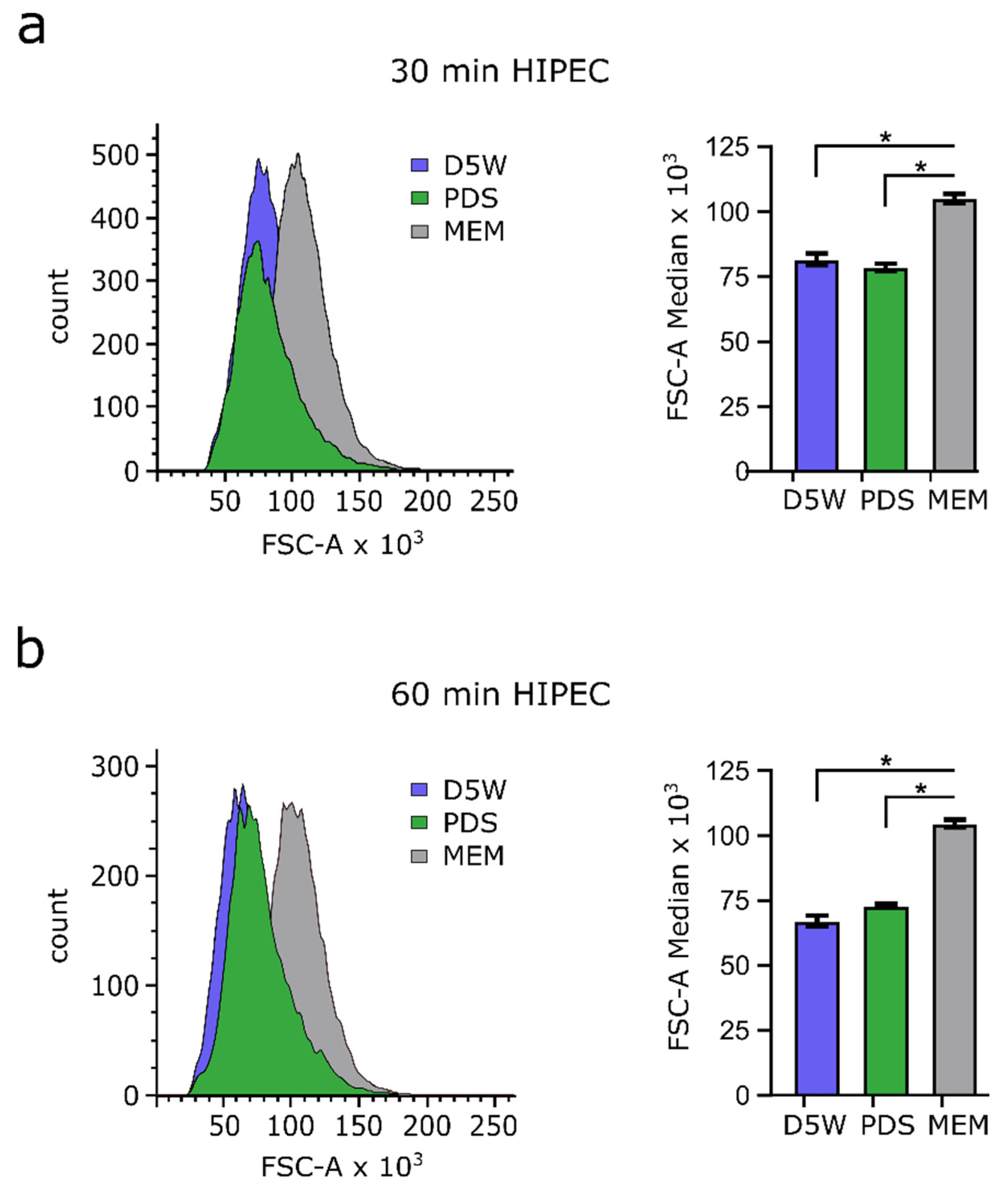
3.5. Drug Solvents Used for HIPEC Reduce Cell Size
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Verwaal, V.J.; Van Ruth, S.; De Bree, E.; Van Slooten, G.W.; Van Tinteren, H.; Boot, H.; Zoetmulder, F.A. Randomized Trial of Cytoreduction and Hyperthermic Intraperitoneal Chemotherapy Versus Systemic Chemotherapy and Palliative Surgery in Patients With Peritoneal Carcinomatosis of Colorectal Cancer. J. Clin. Oncol. 2003, 21, 3737–3743. [Google Scholar] [CrossRef] [PubMed]
- Helderman, R.F.C.P.A.; Löke, D.R.; Kok, H.P.; Oei, A.L.; Tanis, P.J.; Franken, N.A.P.K.; Crezee, J. Variation in Clinical Application of Hyperthermic Intraperitoneal Chemotherapy: A Review. Cancers 2019, 11, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacquet, P.; Sugarbaker, P.H. Peritoneal-plasma barrier. Cancer Treat. Res. 1996, 82, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Kusamura, S.; Barretta, F.; Yonemura, Y.; Sugarbaker, P.H.; Moran, B.J.; Levine, E.A.; Goere, D.; Baratti, D.; Nizri, E.; Morris, D.L.; et al. The Role of Hyperthermic Intraperitoneal Chemotherapy in Pseudomyxoma Peritonei After Cytoreductive Surgery. JAMA Surg. 2021, 156, e206363. [Google Scholar] [CrossRef]
- Lin, Y.-L.; Xu, D.-Z.; Li, X.-B.; Yan, F.-C.; Xu, H.-B.; Peng, Z.; Li, Y. Consensuses and controversies on pseudomyxoma peritonei: A review of the published consensus statements and guidelines. Orphanet J. Rare Dis. 2021, 16, 85. [Google Scholar] [CrossRef]
- Van Driel, W.J.; Koole, S.N.; Sikorska, K.; Van Leeuwen, J.H.S.; Schreuder, H.W.R.; Hermans, R.H.M.; De Hingh, I.H.J.T.; Van Der Velden, J.; Arts, H.J.; Massuger, L.F.A.G.; et al. Hyperthermic Intraperitoneal Chemotherapy in Ovarian Cancer. N. Engl. J. Med. 2018, 378, 230–240. [Google Scholar] [CrossRef]
- Yurttas, C.; Hoffmann, G.; Tolios, A.; Haen, S.P.; Schwab, M.; Königsrainer, I.; Königsrainer, A.; Beckert, S.; Löffler, M.W.; Yurttas, C.; et al. Systematic Review of Variations in Hyperthermic Intraperitoneal Chemotherapy (HIPEC) for Peritoneal Metastasis from Colorectal Cancer. J. Clin. Med. 2018, 7, 567. [Google Scholar] [CrossRef] [Green Version]
- Elias, D.; Bonnay, M.; Puizillou, J.M.; Antoun, S.; Demirdjian, S.; El Otmany, A.; Pignon, J.-P.; Drouard-Troalen, L.; Ouellet, J.F.; Ducreux, M. Heated intra-operative intraperitoneal oxaliplatin after complete resection of peritoneal carcinomatosis: Pharmacokinetics and tissue distribution. Ann. Oncol. 2002, 13, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Mehta, S.S.; Bhatt, A.; Glehen, O. Cytoreductive Surgery and Peritonectomy Procedures. Indian J. Surg. Oncol. 2016, 7, 139–151. [Google Scholar] [CrossRef] [Green Version]
- Kuijpers, A.; Hauptmann, M.; Aalbers, A.; Nienhuijs, S.; de Hingh, I.; Wiezer, M.; van Ramshorst, B.; van Ginkel, R.; Havenga, K.; Verwaal, V. Cytoreduction and hyperthermic intraperitoneal chemotherapy: The learning curve reassessed. Eur. J. Surg. Oncol. (EJSO) 2016, 42, 244–250. [Google Scholar] [CrossRef]
- Moradi, B.N.; Esquivel, J. Learning curve in cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. J. Surg. Oncol. 2009, 100, 293–296. [Google Scholar] [CrossRef] [PubMed]
- Morales-Soriano, R.; Esteve-Pérez, N.; Segura-Sampedro, J.J.; Cascales-Campos, P.; Barrios, P.; Alonso-Gómez, J.; García-Fadrique, A.; Arjona-Sánchez, A.; Arteaga-Martín, X.; Bretcha-Boix, P.; et al. Current practice in cytoreductive surgery and HIPEC for metastatic peritoneal disease: Spanish multicentric survey. Eur. J. Surg. Oncol. (EJSO) 2018, 44, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Quénet, F.; Elias, D.; Roca, L.; Goéré, D.; Ghouti, L.; Pocard, M.; Facy, O.; Arvieux, C.; Lorimier, G.; Pezet, D.; et al. Cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy versus cytoreductive surgery alone for colorectal peritoneal metastases (PRODIGE 7): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 256–266. [Google Scholar] [CrossRef]
- Ceelen, W. HIPEC with oxaliplatin for colorectal peritoneal metastasis: The end of the road? Eur. J. Surg. Oncol. (EJSO) 2018, 45, 400–402. [Google Scholar] [CrossRef]
- Königsrainer, A.; Rau, B. Cytoreductive Surgery (CRS) and Hyperthermic IntraPeritoneal Chemotherapy (HIPEC): Don’t throw the baby out with the bathwater. Pleura Peritoneum 2018, 3, 20180131. [Google Scholar] [CrossRef]
- Yurttas, C.; Fisher, O.M.; Cortés-Guiral, D.; Haen, S.P.; Königsrainer, I.; Königsrainer, A.; Beckert, S.; Liauw, W.; Löffler, M.W. Cytoreductive surgery and HIPEC in colorectal cancer—did we get hold of the wrong end of the stick? Mag. Eur. Med Oncol. 2020, 13, 434–439. [Google Scholar] [CrossRef]
- Ceelen, W.; Demuytere, J.; de Hingh, I. Hyperthermic Intraperitoneal Chemotherapy: A Critical Review. Cancers 2021, 13, 3114. [Google Scholar] [CrossRef]
- Löffler, M.W.; Schuster, H.; Zeck, A.; Quilitz, N.; Weinreich, J.; Tolios, A.; Haen, S.P.; Horvath, P.; Löb, S.; Rammensee, H.-G.; et al. Pharmacodynamics of Oxaliplatin-Derived Platinum Compounds During Hyperthermic Intraperitoneal Chemotherapy (HIPEC): An Emerging Aspect Supporting the Rational Design of Treatment Protocols. Ann. Surg. Oncol. 2017, 24, 1650–1657. [Google Scholar] [CrossRef]
- Limame, R.; Wouters, A.; Pauwels, B.; Fransen, E.; Peeters, M.; Lardon, F.; De Wever, O.; Pauwels, P. Comparative Analysis of Dynamic Cell Viability, Migration and Invasion Assessments by Novel Real-Time Technology and Classic Endpoint Assays. PLoS ONE 2012, 7, e46536. [Google Scholar] [CrossRef]
- Roberts, D.; Schick, J.; Conway, S.; Biade, S.; Laub, P.B.; Stevenson, J.P.; Hamilton, T.C.; O’Dwyer, P.J.; Johnson, S.W. Identification of genes associated with platinum drug sensitivity and resistance in human ovarian cancer cells. Br. J. Cancer 2005, 92, 1149–1158. [Google Scholar] [CrossRef] [Green Version]
- Ubink, I.; Bolhaqueiro, A.C.F.; Elias, S.G.; Raats, D.A.E.; Constantinides, A.; Peters, N.A.; Wassenaar, E.C.E.; De Hingh, I.H.J.T.; Rovers, K.P.; Van Grevenstein, W.M.U.; et al. Organoids from colorectal peritoneal metastases as a platform for improving hyperthermic intraperitoneal chemotherapy. Br. J. Surg. 2019, 106, 1404–1414. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, J.; Wilson, I.; Orton, T.; Pognan, F. Investigation of the Alamar Blue (resazurin) fluorescent dye for the assessment of mammalian cell cytotoxicity. Eur. J. Biochem. 2000, 267, 5421–5426. [Google Scholar] [CrossRef] [PubMed]
- Orellana, E.A.; Kasinski, A.L. Sulforhodamine B (SRB) Assay in Cell Culture to Investigate Cell Proliferation. Bio. Protocol. 2016, 6, e1984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-Maqueda, D.; Miralles, B.; Recio, I. HT29 Cell Line. In The Impact of Food Bioactives on Health: In Vitro and Ex Vivo Models; Verhoeckx, K., Cotter, P., Lopez-Exposito, I., Kleiveland, C., Lea, T., Mackie, A., Requena, T., Swiatecka, D., Wichers, H., Eds.; Springer: Cham, Switzerland; Heidelberg, Germany; New York, NY, USA; Dordrecht, The Netherlands; London, UK, 2015; pp. 113–124. ISBN 978-3-319-16104-4. [Google Scholar] [CrossRef]
- Shoemaker, R.H. The NCI60 human tumour cell line anticancer drug screen. Nat. Cancer 2006, 6, 813–823. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.K.; Osada, T.; Barry, W.T.; Yang, X.Y.; Freedman, J.A.; Tsamis, K.A.; Datto, M.; Clary, B.M.; Clay, T.; Morse, M.A.; et al. Characterization of an Oxaliplatin Sensitivity Predictor in a Preclinical Murine Model of Colorectal Cancer. Mol. Cancer Ther. 2012, 11, 1500–1509. [Google Scholar] [CrossRef] [Green Version]
- Lambert, L.A. Looking up: Recent advances in understanding and treating peritoneal carcinomatosis. CA: A Cancer J. Clin. 2015, 65, 283–298. [Google Scholar] [CrossRef]
- Klaver, C.E.L.; Wisselink, D.D.; Punt, C.J.A.; Snaebjornsson, P.; Crezee, J.; Aalbers, A.G.J.; Brandt, A.; Bremers, A.J.A.; Burger, J.W.A.; Fabry, H.F.J.; et al. Adjuvant hyperthermic intraperitoneal chemotherapy in patients with locally advanced colon cancer (COLOPEC): A multicentre, open-label, randomised trial. Lancet Gastroenterol. Hepatol. 2019, 4, 761–770. [Google Scholar] [CrossRef]
- Cashin, P.; Sugarbaker, P.H. Hyperthermic intraperitoneal chemotherapy (HIPEC) for colorectal and appendiceal peritoneal metastases: Lessons learned from PRODIGE 7. J. Gastrointest. Oncol. 2021, 12, S120–S128. [Google Scholar] [CrossRef]
- Rovers, K.P.; Kok, N.F.M.; Punt, C.J.A.; Tanis, P.J.; de Hingh, I.H.J.T. Limitations of the PRODIGE 7 trial. Lancet Oncol. 2021, 22, e174. [Google Scholar] [CrossRef]
- Nagourney, R.A.; Evans, S.; Tran, P.H.; Nagourney, A.J.; Sugarbaker, P.H. Colorectal cancer cells from patients treated with FOLFOX or CAPOX are resistant to oxaliplatin. Eur. J. Surg. Oncol. (EJSO) 2020, 47, 738–742. [Google Scholar] [CrossRef]
- Helderman, R.; Löke, D.; Tanis, P.; Tuynman, J.; Ceelen, W.; de Hingh, I.; van der Speeten, K.; Franken, N.; Oei, A.; Kok, H.; et al. Preclinical In Vivo-Models to Investigate HIPEC; Current Methodologies and Challenges. Cancers 2021, 13, 3430. [Google Scholar] [CrossRef] [PubMed]
- Dedrick, R.L. Theoretical and experimental bases of intraperitoneal chemotherapy. Semin. Oncol. 1985, 12, 1–6. [Google Scholar] [PubMed]
- Butcher, D.T.; Alliston, T.; Weaver, V.M. A tense situation: Forcing tumour progression. Nat. Cancer 2009, 9, 108–122. [Google Scholar] [CrossRef]
- Pestieau, S.R.; Belliveau, J.F.; Griffin, H.; Stuart, O.A.; Sugarbaker, P.H. Pharmacokinetics of intraperitoneal oxaliplatin: Experimental studies. J. Surg. Oncol. 2001, 76, 106–114. [Google Scholar] [CrossRef]
- Mehta, A.; Hoven, J.V.D.; Rosing, H.; Hillebrand, M.; Nuijen, B.; Huitema, A.; Beijnen, J.; Verwaal, V. Stability of oxaliplatin in chloride-containing carrier solutions used in hyperthermic intraperitoneal chemotherapy. Int. J. Pharm. 2015, 479, 23–27. [Google Scholar] [CrossRef]
- Forsythe, S.D.; Sasikumar, S.; Moaven, O.; Sivakumar, H.; Shen, P.; Levine, E.A.; Soker, S.; Skardal, A.; Votanopoulos, K.I. Personalized Identification of Optimal HIPEC Perfusion Protocol in Patient-Derived Tumor Organoid Platform. Ann. Surg. Oncol. 2020, 27, 4950–4960. [Google Scholar] [CrossRef]
- Helderman, R.F.; Löke, D.R.; Verhoeff, J.; Rodermond, H.M.; Van Bochove, G.G.; Boon, M.; Van Kesteren, S.; Vallejo, J.J.G.; Kok, H.P.; Tanis, P.J.; et al. The Temperature-Dependent Effectiveness of Platinum-Based Drugs Mitomycin-C and 5-FU during Hyperthermic Intraperitoneal Chemotherapy (HIPEC) in Colorectal Cancer Cell Lines. Cells 2020, 9, 1775. [Google Scholar] [CrossRef]
- Oei, A.L.; Vriend, L.E.M.; Crezee, J.; Franken, N.A.P.; Krawczyk, P.M. Effects of hyperthermia on DNA repair pathways: One treatment to inhibit them all. Radiat. Oncol. 2015, 10, 165. [Google Scholar] [CrossRef] [Green Version]
- Schaaf, L.; Schwab, M.; Ulmer, C.; Heine, S.; Mürdter, T.E.; Schmid, J.O.; Sauer, G.; Aulitzky, W.E.; Van Der Kuip, H. Hyperthermia Synergizes with Chemotherapy by Inhibiting PARP1-Dependent DNA Replication Arrest. Cancer Res. 2016, 76, 2868–2875. [Google Scholar] [CrossRef] [Green Version]
- Less, J.R.; Posner, M.C.; Boucher, Y.; Borochovitz, D.; Wolmark, N.; Jain, R.K. Interstitial hypertension in human breast and colorectal tumors. Cancer Res. 1992, 52, 6371–6374. [Google Scholar]
- Larroque, M.; Mounicou, S.; Sgarbura, O.; Arnaudguilhem, C.; Rebel, L.; Leaha, C.; Faye, P.-A.; Enjalbal, C.; Quénet, F.; Bouyssiere, B.; et al. Study of oxaliplatin penetration into ovaries of patients treated with hyperthermic intraperitoneal chemotherapy (HIPEC) for peritoneal metastases of colorectal and appendiceal origin using mass spectrometry imaging. Pleura Peritoneum 2021, 6, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Gremonprez, F.; Willaert, W.; Ceelen, W. Intraperitoneal chemotherapy (IPC) for peritoneal carcinomatosis: Review of animal models. J. Surg. Oncol. 2014, 109, 110–116. [Google Scholar] [CrossRef]
- Gremonprez, F.; Willaert, W.; Ceelen, W. Animal models of colorectal peritoneal metastasis. Pleura Peritoneum 2016, 1, 23–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceelen, W.P.; Pahlman, L.; Mahteme, H. Pharmacodynamic aspects of intraperitoneal cytotoxic therapy. Cancer Treat. Res. 2007, 134, 195–214. [Google Scholar] [CrossRef] [PubMed]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seyfried, N.; Yurttas, C.; Burkard, M.; Oswald, B.; Tolios, A.; Herster, F.; Kauer, J.; Jäger, T.; Königsrainer, I.; Thiel, K.; et al. Prolonged Exposure to Oxaliplatin during HIPEC Improves Effectiveness in a Preclinical Micrometastasis Model. Cancers 2022, 14, 1158. https://doi.org/10.3390/cancers14051158
Seyfried N, Yurttas C, Burkard M, Oswald B, Tolios A, Herster F, Kauer J, Jäger T, Königsrainer I, Thiel K, et al. Prolonged Exposure to Oxaliplatin during HIPEC Improves Effectiveness in a Preclinical Micrometastasis Model. Cancers. 2022; 14(5):1158. https://doi.org/10.3390/cancers14051158
Chicago/Turabian StyleSeyfried, Nick, Can Yurttas, Markus Burkard, Benedikt Oswald, Alexander Tolios, Franziska Herster, Joseph Kauer, Tarkan Jäger, Ingmar Königsrainer, Karolin Thiel, and et al. 2022. "Prolonged Exposure to Oxaliplatin during HIPEC Improves Effectiveness in a Preclinical Micrometastasis Model" Cancers 14, no. 5: 1158. https://doi.org/10.3390/cancers14051158