
Comparison of Post-Transplantation Lymphoproliferative Disorder Risk and Prognostic Factors between Kidney and Liver Transplant Recipients

 , , , , , , , , and
, , , , , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Statistical Analyses
3. Results
3.1. Clinical Characteristics
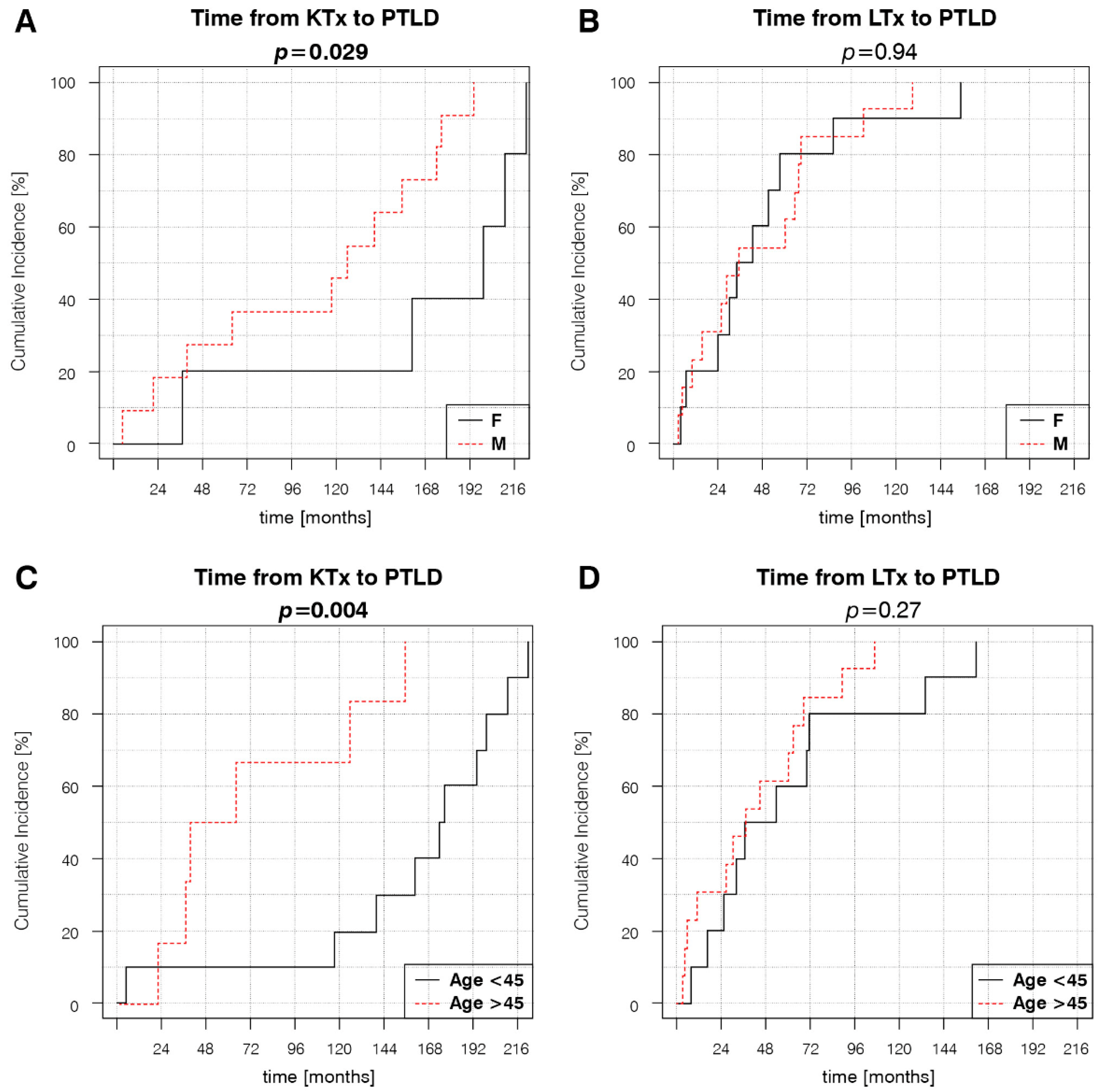
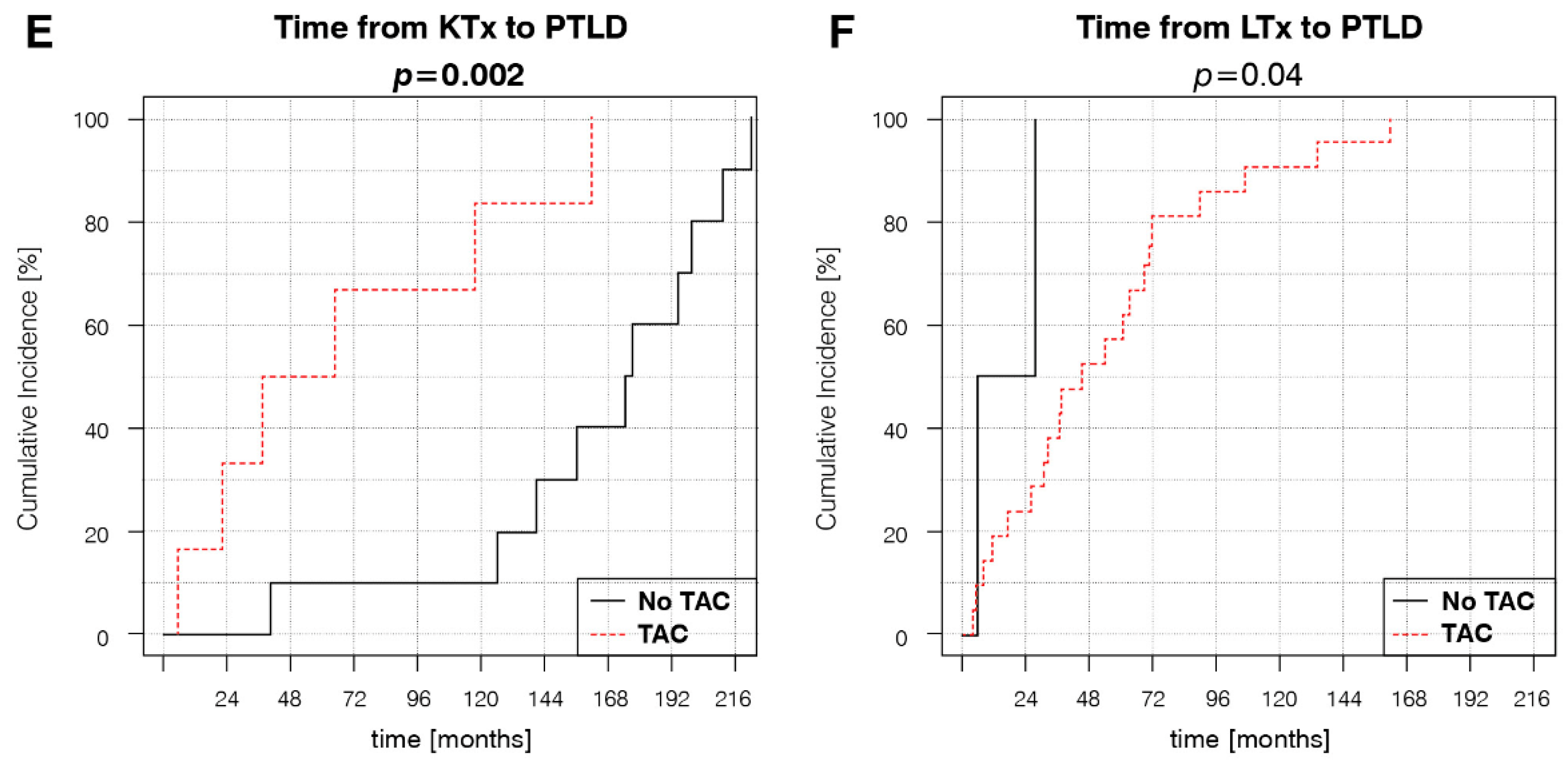
3.2. Factors Associated with PTLD Development
3.3. Treatment and Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Penn, I.; Hammond, W.; Brettschneider, L.; Starzl, T.E. Malignant lymphomas in transplantation patients. Transplant. Proc. 1969, 1, 106–112. [Google Scholar]
- Grulich, A.E.; Van Leeuwen, M.T.; Falster, M.O.; Vajdic, C.M. Incidence of cancers in people with HIV/AIDS compared with immunosuppressed transplant recipients: A meta-analysis. Lancet 2007, 370, 59–67. [Google Scholar] [CrossRef]
- Swerdlow, S.H.; Campo, E.; Pileri, S.A.; Harris, N.L.; Stein, H.; Siebert, R.; Advani, R.; Ghielmini, M.; Salles, G.A.; Zelenetz, A.D.; et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood 2016, 127, 2375–2390. [Google Scholar] [CrossRef] [Green Version]
- Mynarek, M.; Schober, T.; Behrends, U.; Maecker-Kolhoff, B. Posttransplant lymphoproliferative disease after pediatric solid organ transplantation. Clin. Dev. Immunol. 2013, 2013, 814973. [Google Scholar] [CrossRef]
- Luskin, M.R.; Heil, D.S.; Tan, K.S.; Choi, S.; Stadtmauer, E.A.; Schuster, S.J.; Porter, D.L.; Vonderheide, R.H.; Bagg, A.; Heitjan, D.F.; et al. The Impact of EBV Status on Characteristics and Outcomes of Posttransplantation Lymphoproliferative Disorder. Am. J. Transplant. 2015, 15, 2665–2673. [Google Scholar] [CrossRef]
- Al-Mansour, Z.; Nelson, B.P.; Evens, A.M. Post-transplant lymphoproliferative disease (PTLD): Risk factors, diagnosis, and current treatment strategies. Curr. Hematol. Malig. Rep. 2013, 8, 173–183. [Google Scholar] [CrossRef] [Green Version]
- Fang, Y.; Pinkney, K.A.; Lee, J.C.; Gindin, T.; Weiner, M.A.; Alobeid, B.; Bhagat, G. T-cell acute lymphoblastic leukaemia after liver transplantation: Post-transplant lymphoproliferative disorder or coincidental de novo leukaemia? Hematol. Oncol. 2013, 31, 49–53. [Google Scholar] [CrossRef]
- Le, J.; Durand, C.M.; Agha, I.; Brennan, D.C. Epstein-Barr virus and renal transplantation. Transplant. Rev. 2017, 31, 55–60. [Google Scholar] [CrossRef]
- Morton, M.; Coupes, B.; Roberts, S.A.; Klapper, P.E.; Byers, R.J.; Vallely, P.J.; Ryan, K.; Picton, M.L. Epidemiology of posttransplantation lymphoproliferative disorder in adult renal transplant recipients. Transplantation 2013, 95, 470–478. [Google Scholar] [CrossRef] [Green Version]
- Dharnidharka, V.R. Comprehensive review of post-organ transplant hematologic cancers. Am. J. Transplant. 2018, 18, 537–549. [Google Scholar] [CrossRef]
- Abu-Shanab, A.; Ged, Y.; Ullah, N.; Houlihan, D.; McCormick, A. Increased Incidence of Post-transplant Lymphoproliferative Disorder in Autoimmune Liver Disease: An Irish National Experience. J. Clin. Exp. Hepatol. 2018, 8, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Yu, F.; Huang, Y.; Wang, Y.; Yu, Z.; Li, X.; Dong, J. Very late onset post-transplant diffuse large B cell lymphoma in a liver transplant recipient with hepatitis B: A case report. Medicine 2018, 97, e13063. [Google Scholar] [CrossRef] [PubMed]
- Kinch, A.; Baecklund, E.; Backlin, C.; Ekman, T.; Molin, D.; Tufveson, G.; Fernberg, P.; Sundström, C.; Pauksens, K.; Enblad, G. A population-based study of 135 lymphomas after solid organ transplantation: The role of Epstein-Barr virus, hepatitis C and diffuse large B-cell lymphoma subtype in clinical presentation and survival. Acta Oncol. 2014, 53, 669–679. [Google Scholar] [CrossRef] [Green Version]
- Burra, P.; Buda, A.; Livi, U.; Rigotti, P.; Zanus, G.; Calabrese, F.; Caforio, A.; Menin, C.; Canova, D.; Farinati, F.; et al. Occurrence of post-transplant lymphoproliferative disorders among over thousand adult recipients: Any role for hepatitis C infection? Eur. J. Gastroenterol. Hepatol. 2006, 18, 1065–1070. [Google Scholar] [CrossRef] [PubMed]
- Mihaila, R.G. Hepatitis C virus-associated B cell non-Hodgkin’s lymphoma. World J. Gastroenterol. 2016, 22, 6214–6223. [Google Scholar] [CrossRef]
- Karuturi, M.; Shah, N.; Frank, D.; Fasan, O.; Reshef, R.; Ahya, V.N.; Bromberg, M.; Faust, T.; Goral, S.; Schuster, S.J.; et al. Plasmacytic post-transplant lymphoproliferative disorder: A case series of nine patients. Transpl. Int. 2013, 26, 616–622. [Google Scholar] [CrossRef]
- Bishnoi, R.; Bajwa, R.; Franke, A.J.; Skelton, W.P., 4th; Wang, Y.; Patel, N.M.; Slayton, W.B.; Zou, F.; Dang, N.H. Post-transplant lymphoproliferative disorder (PTLD): Single institutional experience of 141 patients. Exp. Hematol. Oncol. 2017, 6, 26. [Google Scholar] [CrossRef] [Green Version]
- Reshef, R.; Vardhanabhuti, S.; Luskin, M.R.; Heitjan, D.F.; Hadjiliadis, D.; Goral, S.; Krok, K.L.; Goldberg, L.R.; Porter, D.L.; Stadtmauer, E.A.; et al. Reduction of immunosuppression as initial therapy for posttransplantation lymphoproliferative disorder. Am. J. Transplant. 2011, 11, 336–347. [Google Scholar] [CrossRef]
- Yoon, S.O.; Yu, E.; Cho, Y.M.; Suh, C.; Kim, K.M.; Han, D.J.; Lee, S.G.; Huh, J. Post-transplant lymphoproliferative disorders: Clinicopathological analysis of 43 cases in a single center, 1990–2009. Clin. Transplant. 2012, 26, 67–73. [Google Scholar] [CrossRef]
- Martinez-Calle, N.; Alfonso, A.; Rifon, J.; Herrero, I.; Errasti, P.; Rábago, G.; Merino, J.; Panizo, Á.; Pardo, J.; Prósper, F.; et al. First-line use of rituximab correlates with increased overall survival in late post-transplant lymphoproliferative disorders: Retrospective, single-centre study. Eur. J. Haematol. 2017, 98, 38–43. [Google Scholar] [CrossRef]
- Montanari, F.; Radeski, D.; Seshan, V.; Alobeid, B.; Bhagat, G.; O’Connor, O.A. Recursive partitioning analysis of prognostic factors in post-transplant lymphoproliferative disorders (PTLD): A 120 case single institution series. Br. J. Haematol. 2015, 171, 491–500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dierickx, D.; Habermann, T.M. Post-Transplantation Lymphoproliferative Disorders in Adults. N. Engl. J. Med. 2018, 378, 549–562. [Google Scholar] [CrossRef] [PubMed]
- Lau, E.; Moyers, J.T.; Wang, B.C.; Jeong, I.S.D.; Lee, J.; Liu, L.; Kim, M.; Villicana, R.; Kim, B.; Mitchell, J.; et al. Analysis of Post-Transplant Lymphoproliferative Disorder (PTLD) Outcomes with Epstein-Barr Virus (EBV) Assessments-A Single Tertiary Referral Center Experience and Review of Literature. Cancers 2021, 13, 899. [Google Scholar] [CrossRef] [PubMed]
- Abbas, F.; El Kossi, M.; Shaheen, I.S.; Sharma, A.; Halawa, A. Post-transplantation lymphoproliferative disorders: Current concepts and future therapeutic approaches. World J. Transplant. 2020, 10, 29–46. [Google Scholar] [CrossRef] [PubMed]
- Quinlan, S.C.; Pfeiffer, R.M.; Morton, L.M.; Engels, E.A. Risk factors for early-onset and late-onset post-transplant lymphoproliferative disorder in kidney recipients in the United States. Am. J. Hematol. 2011, 86, 206–209. [Google Scholar] [CrossRef] [Green Version]
- Caillard, S.; Porcher, R.; Provot, F.; Dantal, J.; Choquet, S.; Durrbach, A.; Morelon, E.; Moal, V.; Janbon, B.; Alamartine, E.; et al. Post-transplantation lymphoproliferative disorder after kidney transplantation: Report of a nationwide French registry and the development of a new prognostic score. J. Clin. Oncol. 2013, 31, 1302–1309. [Google Scholar] [CrossRef]
- Fararjeh, F.A.; Mahmood, S.; Tachtatzis, P.; Yallop, D.; Devereux, S.; Patten, P.; Agrawal, K.; Suddle, A.; O’Grady, J.; Heaton, N.; et al. A retrospective analysis of post-transplant lymphoproliferative disorder following liver transplantation. Eur. J. Haematol. 2018, 100, 98–103. [Google Scholar] [CrossRef] [Green Version]
- Bishnoi, R.; Minish, J.; Franke, A.J.; Skelton, W.P., 4th; Shah, C.P.; Wang, Y.; Dang, N.H. Single-institution Retrospective Analysis of Prognostic Factors Influencing Very Late-onset Post-transplant Lymphoproliferative Disorder. Cureus 2020, 12, e6912. [Google Scholar] [CrossRef] [Green Version]
- Bustami, R.T.; Ojo, A.O.; Wolfe, R.A.; Merion, R.M.; Bennett, W.M.; McDiarmid, S.V.; Leichtman, A.B.; Held, P.J.; Port, F.K. Immunosuppression and the risk of post-transplant malignancy among cadaveric first kidney transplant recipients. Am. J. Transplant. 2004, 4, 87–93. [Google Scholar] [CrossRef]
- Francis, A.; Johnson, D.W.; Teixeira-Pinto, A.; Craig, J.C.; Wong, G. Incidence and predictors of post-transplant lymphoproliferative disease after kidney transplantation during adulthood and childhood: A registry study. Nephrol. Dial. Transplant. 2018, 33, 881–889. [Google Scholar] [CrossRef] [Green Version]
- Sampaio, M.S.; Cho, Y.W.; Shah, T.; Bunnapradist, S.; Hutchinson, I.V. Association of immunosuppressive maintenance regimens with posttransplant lymphoproliferative disorder in kidney transplant recipients. Transplantation 2012, 93, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Taylor, E.; Jones, M.; Hourigan, M.J.; Johnson, D.W.; Gill, D.S.; Isbel, N.; Hawley, C.M.; Marlton, P.; Gandhi, M.K.; Campbell, S.B.; et al. Cessation of immunosuppression during chemotherapy for post-transplant lymphoproliferative disorders in renal transplant patients. Nephrol. Dial. Transplant. 2015, 30, 1774–1779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mucha, K.; Foroncewicz, B.; Ziarkiewicz-Wróblewska, B.; Krawczyk, M.; Lerut, J.; Paczek, L. Post-transplant lymphoproliferative disorder in view of the new WHO classification: A more rational approach to a protean disease? Nephrol. Dial. Transplant. 2010, 25, 2089–2098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trappe, R.U.; Dierickx, D.; Zimmermann, H.; Morschhauser, F.; Mollee, P.; Zaucha, J.M.; Dreyling, M.H.; Dührsen, U.; Reinke, P.; Verhoef, G.; et al. Response to Rituximab Induction Is a Predictive Marker in B-Cell Post-Transplant Lymphoproliferative Disorder and Allows Successful Stratification into Rituximab or R-CHOP Consolidation in an International, Prospective, Multicenter Phase II Trial. J. Clin. Oncol. 2017, 35, 536–543. [Google Scholar] [CrossRef] [Green Version]
- Herreman, A.; Dierickx, D.; Morscio, J.; Camps, J.; Bittoun, E.; Verhoef, G.; De Wolf-Peeters, C.; Sagaert, X.; Tousseyn, T. Clinicopathological characteristics of posttransplant lymphoproliferative disorders of T-cell origin: Single-center series of nine cases and meta-analysis of 147 reported cases. Leuk. Lymphoma 2013, 54, 2190–2199. [Google Scholar] [CrossRef]
- Tsai, D.E.; Bagley, S.; Reshef, R.; Shaked, A.; Bloom, R.D.; Ahya, V.; Goldberg, L.; Chung, A.; Debonera, F.; Schuster, S.J.; et al. The changing face of adult posttransplant lymphoproliferative disorder: Changes in histology between 1999 and 2013. Am. J. Hematol. 2018, 93, 874–881. [Google Scholar] [CrossRef]
- Peters, A.C.; Akinwumi, M.S.; Cervera, C.; Mabilangan, C.; Ghosh, S.; Lai, R.; Iafolla, M.; Doucette, K.; Preiksaitis, J.K. The Changing Epidemiology of Posttransplant Lymphoproliferative Disorder in Adult Solid Organ Transplant Recipients Over 30 Years: A Single-center Experience. Transplantation 2018, 102, 1553–1562. [Google Scholar] [CrossRef]
- Gwon, J.G.; Kim, Y.H.; Han, D.J. Different causes of early and late-onset post transplant lymphoproliferative disorder in kidney transplantation patients after 2000. Asian J. Surg. 2019, 42, 551–556. [Google Scholar] [CrossRef]
- Ville, S.; Imbert-Marcille, B.M.; Coste-Burel, M.; Garandeau, C.; Meurette, A.; Cantarovitch, D.; Giral, M.; Hourmant, M.; Blancho, G.; Dantal, J. Impact of antiviral prophylaxis in adults Epstein-Barr Virus-seronegative kidney recipients on early and late post-transplantation lymphoproliferative disorder onset: A retrospective cohort study. Transpl. Int. 2018, 31, 484–494. [Google Scholar] [CrossRef] [Green Version]
- Roberts, T.K.; Chen, X.; Liao, J.J. Diagnostic and therapeutic challenges of EBV-positive mucocutaneous ulcer: A case report and systematic review of the literature. Exp. Hematol. Oncol. 2015, 5, 13. [Google Scholar] [CrossRef] [Green Version]
- Bieling, M.; Tischer, S.; Kalinke, U.; Blasczyk, R.; Buus, S.; Maecker-Kolhoff, B.; Eiz-Vesper, B. Personalized adoptive immunotherapy for patients with EBV-associated tumors and complications: Evaluation of novel naturally processed and presented EBV-derived T-cell epitopes. Oncotarget 2018, 9, 4737–4757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghobadi, A. Chimeric antigen receptor T cell therapy for non-Hodgkin lymphoma. Curr. Res. Transl. Med. 2018, 66, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Skorka, K.; Ostapinska, K.; Malesa, A.; Giannopoulos, K. The Application of CAR-T Cells in Haematological Malignancies. Arch. Immunol. Ther. Exp. 2020, 68, 34. [Google Scholar] [CrossRef] [PubMed]
- Prockop, S.; Doubrovina, E.; Suser, S.; Heller, G.; Barker, J.; Dahi, P.; Perales, M.A.; Papadopoulos, E.; Sauter, C.; Castro-Malaspina, H.; et al. Off-the-shelf EBV-specific T cell immunotherapy for rituximab-refractory EBV-associated lymphoma following transplant. J. Clin. Investig. 2019, 130, 733–747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schuster, S.J.; Svoboda, J.; Chong, E.A.; Nasta, S.D.; Mato, A.R.; Anak, Ö.; Brogdon, J.L.; Pruteanu-Malinici, I.; Bhoj, V.; Landsburg, D.; et al. Chimeric Antigen Receptor T Cells in Refractory B-Cell Lymphomas. N. Engl. J. Med. 2017, 377, 2545–2554. [Google Scholar] [CrossRef] [PubMed]
- Nakid-Cordero, C.; Baron, M.; Guihot, A.; Vieillard, V. Natural Killer Cells in Post-Transplant Lymphoproliferative Disorders. Cancers 2021, 13, 1836. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| LTRs | KTRs | ||
|---|---|---|---|
| Patient Characteristics | n (%) | p-Value | |
| Number of patients | 23 (100) | 16 (100) | |
| PTLD incidence rate (per 1000 patient-years) Mean age at Tx (years) [SD] | 2.1 | 0.8 | |
| 43.7 (12.0) | 36.3 (20.7) | 0.21 | |
| Males Females | 13 (56.5) | 11 (68.8) | 0.456 |
| 10 (43.5) | 5 (31.3) | 0.456 | |
| KT+LTRs Retransplantation | 1 (4.4) | 1 (6.3) | 1.0 |
| 1 (4.4) | 1 (6.3) | 1.0 | |
| IS Treatment | |||
| Induction | |||
| Anti-CD25 | 12 (52.2) | 3 (18.8) | 0.076 |
| ATG | 0 (0) | 1 (6.3) | 0.853 |
| Acute rejection | |||
| Total | 8 (34.8) | 5 (31.3) | 0.329 |
| 1 (4.4) no data | 2 (12.5) no data | ||
| GCS treated | 8 (34.8) | 5 (31.3) | 0.984 |
| ATG treated | 1 (4.4) | 0 (0) | 0.456 |
| Maintenance | |||
| Monotherapy | 4 (17.4) | 0 (0) | 0.052 |
| Double drug therapy | 12 (52.2) | 6 (37.5) | 0.381 |
| Triple drug therapy | 7 (30.4) | 10 (62.5) | 0.052 |
| GCS | 14 (60.9) | 13 (81.3) | 0.428 |
| CsA | 2 (8.7) | 8 (50) | 0.004 * |
| TAC | 21 (91.3) | 6 (37.5) | <0.001 * |
| AZA | 1 (4.4) | 5 (31.3) | 0.025 * |
| MMF | 11 (47.8) | 10 (62.5) | 0.255 |
| Viral Replication | LTRs | KTRs | p-Value |
| EBV DNA | 10 (43.2) | 10 (62.5) | 0.053 |
| 5 (21.7) no data | 5 (31.3) no data | ||
| CMV DNA | 0 (0) | 2 (12.5) | 0.093 |
| HBV DNA | 2 (8.7) | 1 (6.3) | 0.805 |
| HCV RNA | 5 (21.7) | 1 (6.3) | 0.201 |
| LTRs | KTRs | ||
|---|---|---|---|
| PTLD Characteristics | n (%) | p-Value | |
| Focal disease | 11 (47.8) | 8 (50) | 0.908 |
| Disseminated disease Early onset | 12 (52.2) | 8 (50) | 0.908 |
| 5 (21.7) | 1 (6.3) | 0.16 | |
| Late onset Post-mortem diagnosis | 18 (78.3) | 15 (93.8) | 0.16 |
| 3 (13) | 0 (0) | 0.083 | |
| WHO 2016 Type | |||
| Florid follicular hyperplasia | 1 (4.4) | 0 (0) | 0.434 |
| Infectious mononucleosis | 0 (0) | 1 (6.3) | 0.251 |
| Plasmacytic hyperplasia | 6 (26.1) | 1 (6.3) | 0.122 |
| Polymorphic | 4 (17.4) | 1 (6.3) | 0.324 |
| Monomorphic B-cell | 11 (47.8) | 9 (56.3) | 0.182 |
| -DLBCL | 9 (39.1) | 3 (18.8) | 0.168 |
| -HGBL | 1 (4.4) | 1 (6.3) | 0.805 |
| -Lymphomatoid granulomatosis | 0 (0) | 2 (12.5) | 0.164 |
| -Plasmacytic myeloma | 0 (0) | 1 (6.3) | 0.333 |
| -MCL | 0 (0) | 1 (6.3) | 0.333 |
| -Other | 1 (4.4) | 1 (6.3) | 0.805 |
| Monomorphic T-cell | 1 (4.4) | 3 (18.8) | 0.167 |
| Classic Hodgkin lymphoma | 0 (0) | 1 (6.3) | 0.853 |
| SOT—Univariate | KTR—Univariate | LTR—Univariate | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | HR | 95% CI | p-Value | Variable | HR | 95% CI | p-Value | Variable | HR | 95% CI | p-Value |
| Male sex | 1.49 | (0.74–3.02) | 0.269 | Male sex | 4.86 | (1.03–22.81) | 0.045 * | Male sex | 1.03 | (0.44–2.44) | 0.939 |
| Age at Tx > 45 years | 1.03 | (1.01–1.05) | 0.006 * | Age at Tx > 45 years | 1.04 | (1.00–1.07) | 0.044 * | Age at Tx > 45 years | 1.02 | (0.98–1.05) | 0.357 |
| Retransplantation | 0.96 | (0.29–3.2) | 0.95 | Retransplantation | 2.46 | (0.29–21.12) | 0.412 | Retransplantation | 0.46 | (0.1–2.04) | 0.306 |
| Monotherapy | 2.18 | (0.81–5.84) | 0.12 | Monotherapy | NA | NA | NA | Monotherapy | 1.11 | (0.41–3.06) | 0.835 |
| Double drug therapy | 0.88 | (0.46–1.67) | 0.69 | Double drug therapy | 0.56 | (0.19–1.61) | 0.282 | Double drug therapy | 1.18 | (0.51–2.75) | 0.695 |
| Triple drug therapy | 0.97 | (0.51–1.86) | 0.934 | Triple drug therapy | 1.79 | (0.62–5.14) | 0.282 | Triple drug therapy | 0.91 | (0.35–2.36) | 0.851 |
| GCS | 0.87 | (0.43–1.78) | 0.703 | GCS | 0.68 | (0.18–2.59) | 0.574 | GCS | 1.66 | (0.7–3.94) | 0.247 |
| CsA | 0.44 | (0.20–0.95) | 0.036 * | CsA | 0.59 | (0.21–1.64) | 0.31 | CsA | 4.55 | (0.91–22.8) | 0.065 |
| TAC | 5.09 | (2.00–12.95) | <0.001 * | TAC | 6.25 | (1.68–23.21) | 0.006 * | TAC | 0.22 | (0.04–1.1) | 0.065 |
| AZA | 0.68 | (0.28–1.64) | 0.385 | AZA | 1.28 | (0.42–3.95) | 0.664 | AZA | 0.58 | (0.08–4.39) | 0.596 |
| MMF | 0.78 | (0.41–1.5) | 0.463 | MMF | 1.04 | (0.36–3.05) | 0.936 | MMF | 0.68 | (0.28–1.64) | 0.399 |
| ATG induction | 0.33 | (0.04–2.52) | 0.288 | ATG induction | 0.48 | (0.06–3.8) | 0.488 | ATG induction | NA | NA | NA |
| Anti-CD25 induction | 1.35 | (0.69–2.64) | 0.376 | Anti-CD25 induction | 0.74 | (0.2–2.67) | 0.645 | Anti-CD25 induction | 1.07 | (0.44–2.6) | 0.884 |
| AR treated with GCS | 0.75 | (0.37–1.51) | 0.413 | AR treated with GCS | 0.61 | (0.18–2.01) | 0.413 | AR treated with GCS | 0.72 | (0.3–1.76) | 0.476 |
| AR treated with ATG | 1.38 | (0.18–10.37) | 0.753 | AR treated with ATG | NA | NA | NA | AR treated with ATG | 0.9 | (0.12–6.93) | 0.922 |
| EBV DNA | 0.72 | (0.31–1.68) | 0.447 | EBV DNA | 0.7 | (0.08–6.03) | 0.744 | EBV DNA | 1.66 | (0.62–4.43) | 0.314 |
| CMV DNA | 0.6 | (0.14–2.51) | 0.482 | CMV DNA | 1.26 | (0.27–5.87) | 0.767 | CMV DNA | NA | NA | NA |
| HBV DNA | 0.86 | (0.26–2.83) | 0.802 | HBV DNA | 0.61 | (0.08–4.78) | 0.638 | HBV DNA | 1.32 | (0.3–5.85) | 0.718 |
| HCV RNA | 1.08 | (0.45–2.61) | 0.861 | HCV RNA | 0.48 | (0.06–3.8) | 0.488 | HCV RNA | 0.96 | (0.35–2.65) | 0.942 |
| SOT—Multivariate | KTR—Multivariate | LTR—Multivariate | |||||||||
| Variable | HR | 95% CI | p-Value | Variable | HR | 95% CI | p-Value | Variable | HR | 95% CI | p-Value |
| LTx | 1.75 | (0.63–4.83) | 0.281 | Male sex | 7.87 | (1.25–49.26) | 0.027 * | Male sex | 0.872 | (0.36–2.13) | 0.746 |
| Age at Tx > 45 years | 3.16 | (1.4–7.1) | 0.005 * | Age at Tx > 45 years | 5.21 | (1.04–26.25) | 0.045 * | Age at Tx > 45 years | 1.61 | (0.62–4.21) | 0.332 |
| TAC | 5.85 | (0.89–38.24) | 0.065 | TAC | 18.57 | (2.79–123.87) | 0.003 * | TAC | 0.24 | (0.04–1.35) | 0.107 |
| CsA | 1.91 | (0.39–9.31) | 0.423 |
| LTRs | KTRs | ||
|---|---|---|---|
| PTLD Treatment | n (%) | p-Value | |
| RIS RAPA | 22 (95.7) | 14 (87.5) | 0.37 |
| 9 (39.1) | 3 (18.8) | 0.186 | |
| EVR Anti-CD20 | 0 (0) | 1 (6.3) | 0.251 |
| 6 (26.1) | 4 (25) | 0.955 | |
| Chemotherapy -R-CHOP | 14 (60.9) | 11 (68.8) | 0.631 |
| 7 (30.4) | 2 (12.5) | 0.204 | |
| -CHOP | 4 (17.4) | 2 (12.5) | 0.698 |
| -Other | 3 (13) | 7 (43.8) | 0.02 * |
| Surgery | 8 (34.8) | 5 (31.3) | 0.834 |
| Radiotherapy | 0 (0) | 2 (12.5) | 0.093 |
| LTRs | KTRs | ||
|---|---|---|---|
| Outcomes | n (%) | p-Value | |
| CR | 12 (52.2) | 3 (18.8) | 0.039 * |
| Mean CR duration (months) (SD) Mean survival (months) (SD) | 73.7 (56.1) | 89.7 (61.7) | 0.711 |
| 56.1 (53.4) | 37.3 (51.9) | 0.28 | |
| Total deaths PTLD related deaths | 9 (39.1) | 6 (37.5) | 0.933 |
| 5 (21.7) | 4 (25) | 0.83 | |
| Alive | 12 (52.2) | 9 (56.3) | 0.817 |
| Lost to follow up | 2 (8.7) | 1 (6.3) | 0.805 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mucha, K.; Staros, R.; Foroncewicz, B.; Ziarkiewicz-Wróblewska, B.; Kosieradzki, M.; Nazarewski, S.; Naumnik, B.; Raszeja-Wyszomirska, J.; Zieniewicz, K.; Pączek, L. Comparison of Post-Transplantation Lymphoproliferative Disorder Risk and Prognostic Factors between Kidney and Liver Transplant Recipients. Cancers 2022, 14, 1953. https://doi.org/10.3390/cancers14081953
Mucha K, Staros R, Foroncewicz B, Ziarkiewicz-Wróblewska B, Kosieradzki M, Nazarewski S, Naumnik B, Raszeja-Wyszomirska J, Zieniewicz K, Pączek L. Comparison of Post-Transplantation Lymphoproliferative Disorder Risk and Prognostic Factors between Kidney and Liver Transplant Recipients. Cancers. 2022; 14(8):1953. https://doi.org/10.3390/cancers14081953
Chicago/Turabian StyleMucha, Krzysztof, Rafał Staros, Bartosz Foroncewicz, Bogna Ziarkiewicz-Wróblewska, Maciej Kosieradzki, Sławomir Nazarewski, Beata Naumnik, Joanna Raszeja-Wyszomirska, Krzysztof Zieniewicz, and Leszek Pączek. 2022. "Comparison of Post-Transplantation Lymphoproliferative Disorder Risk and Prognostic Factors between Kidney and Liver Transplant Recipients" Cancers 14, no. 8: 1953. https://doi.org/10.3390/cancers14081953