
Digital Holographic Microscopy for Label-Free Detection of Leukocyte Alternations Associated with Perioperative Inflammation after Cardiac Surgery

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
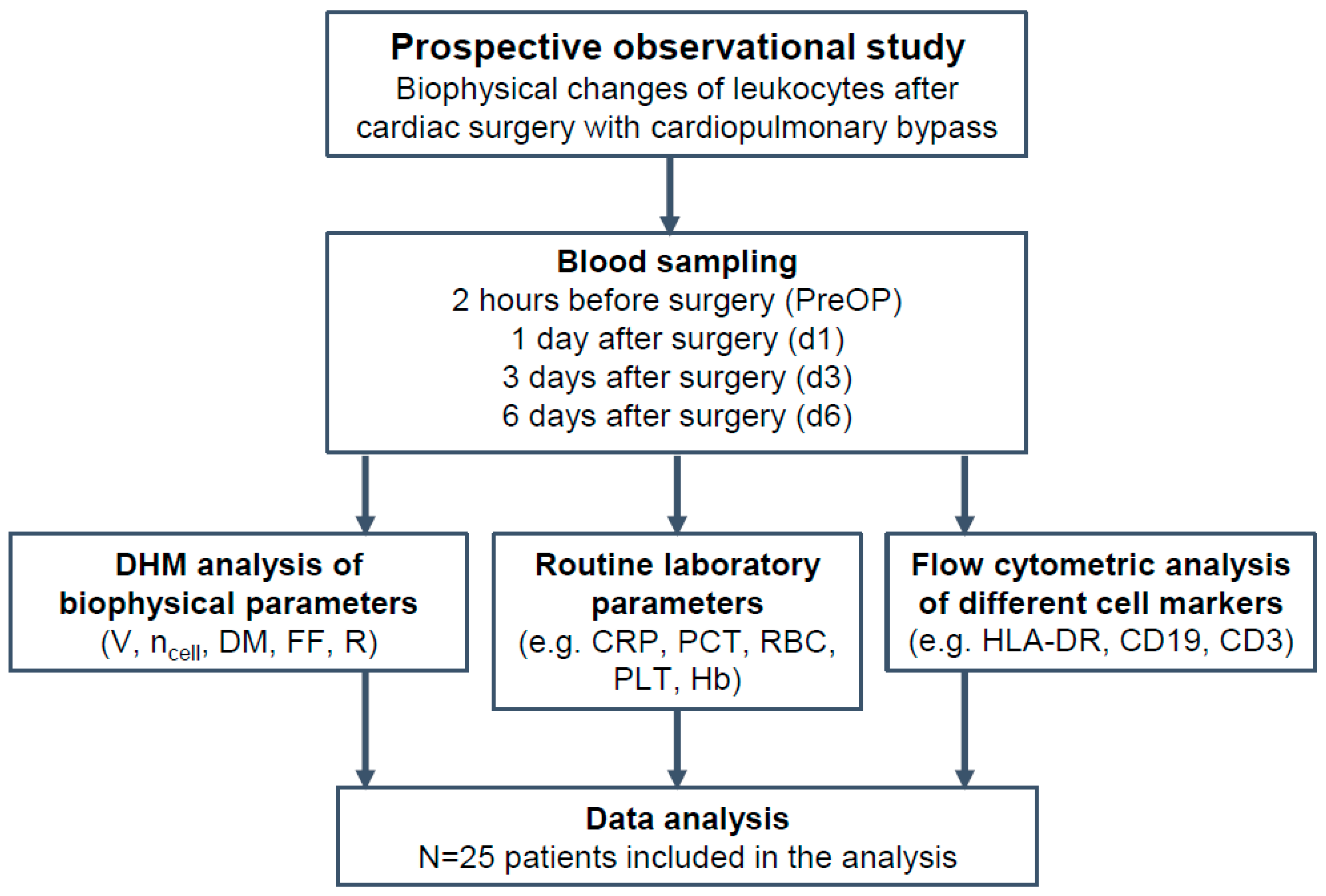
2.1. Study Design and Blood Collection
2.2. Isolation of Peripheral Blood Mononuclear Cells for DHM Analysis
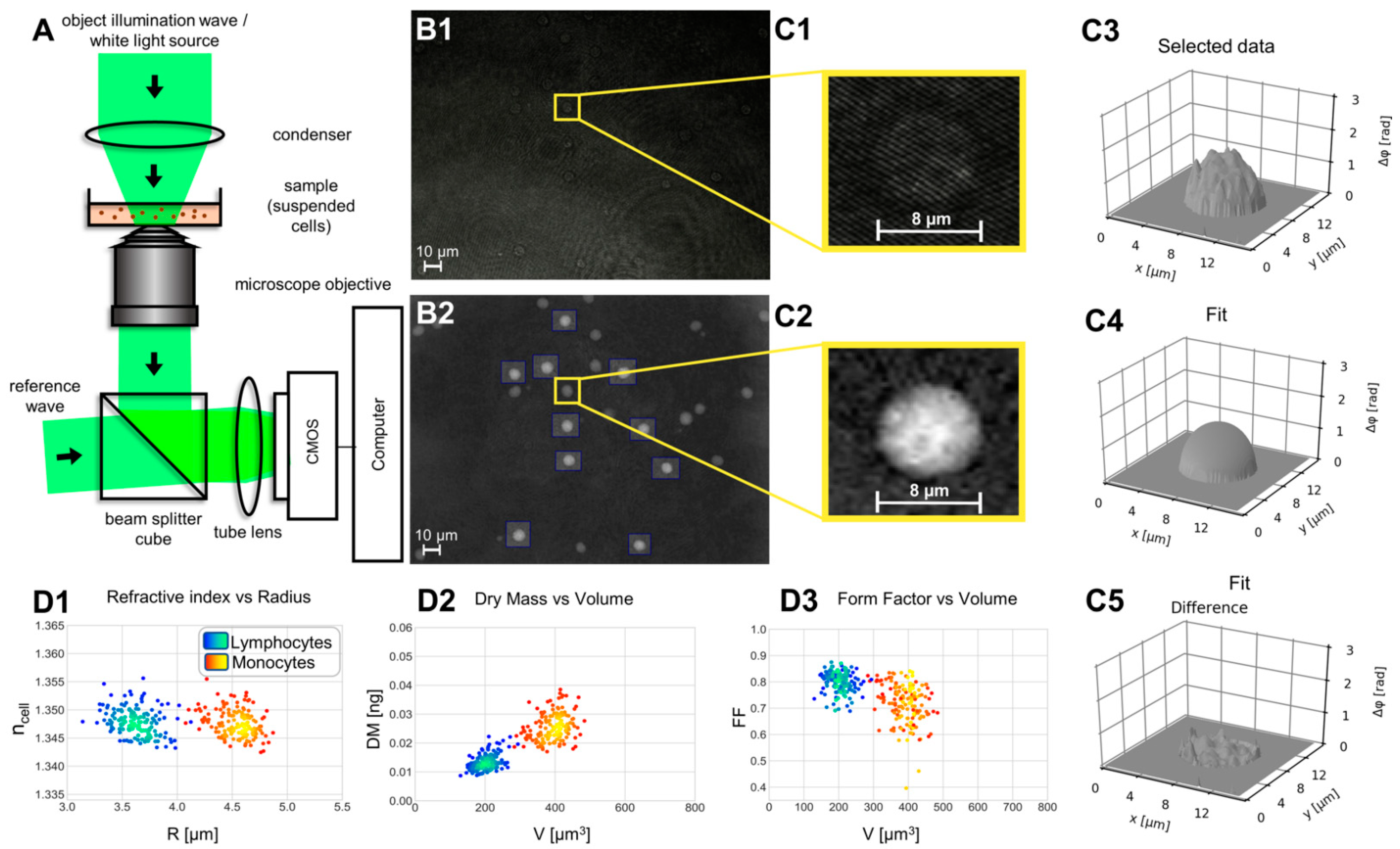
2.3. Quantitative Phase Imaging with Digital Holographic Microscopy
2.4. Evaluation of DHM QPI Images for Determination of Biophysical Parameters and Morphology Changes
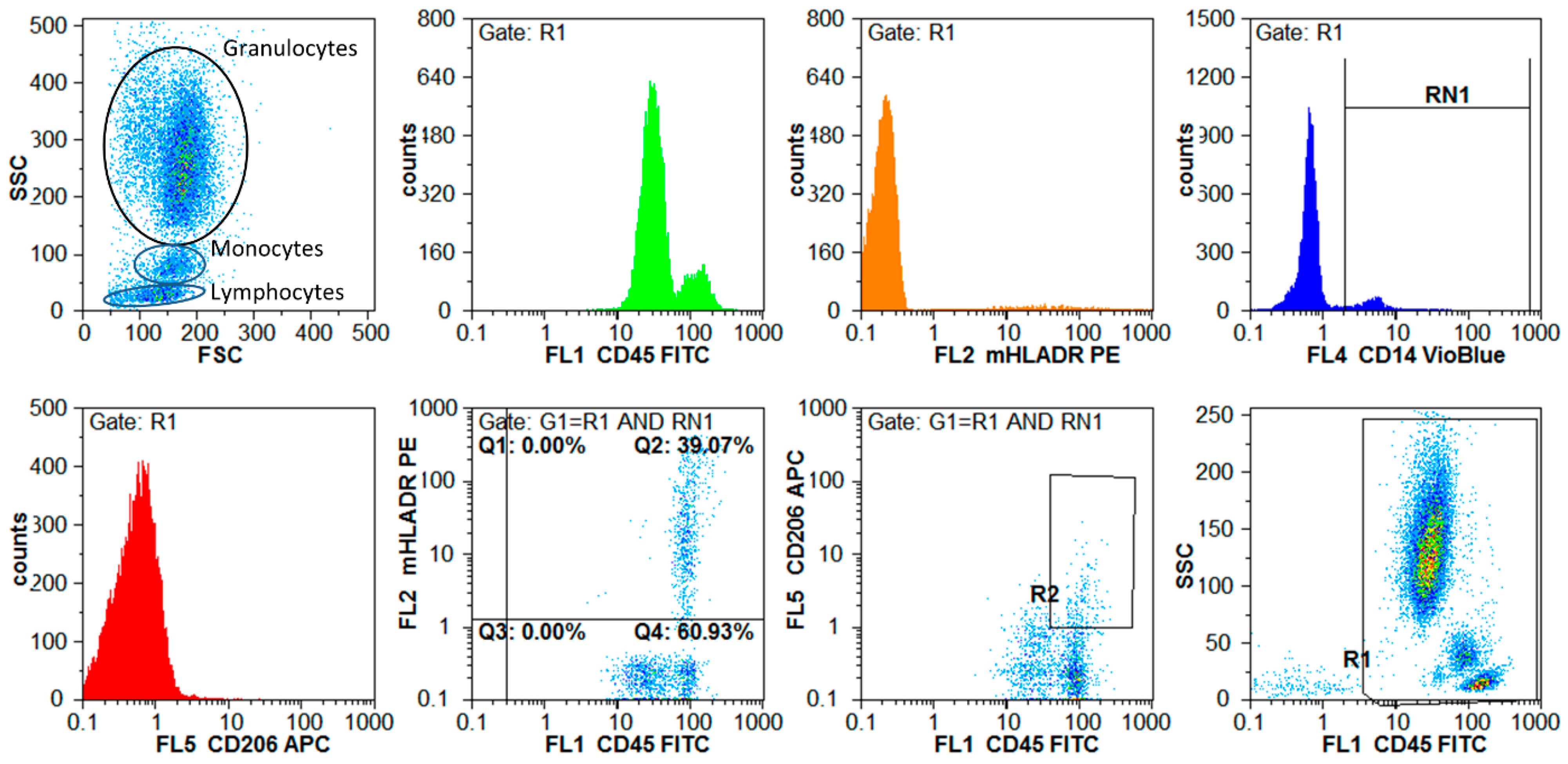
2.5. Flow Cytometric Analyses
2.6. Statistical Analyses and Outcome Measures
3. Results
3.1. The Selected Patient Cohort Had a Typical Spectrum of Features for Cardiac Surgery
3.2. Biophysical Parameters Allow Clear Cell Differentiation between Lymphocytes and Monocytes and Increase in Scattering Immediately after Surgery
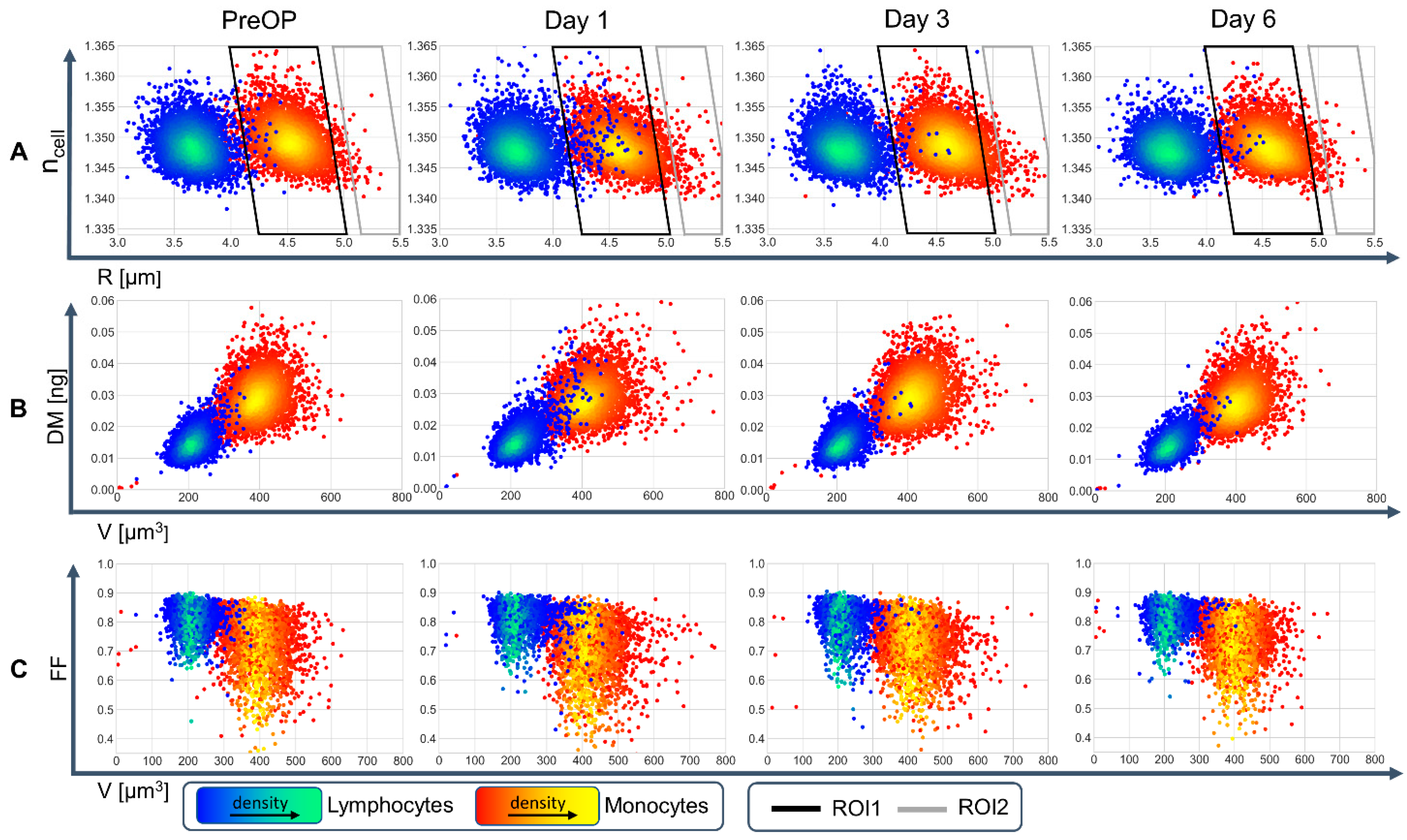
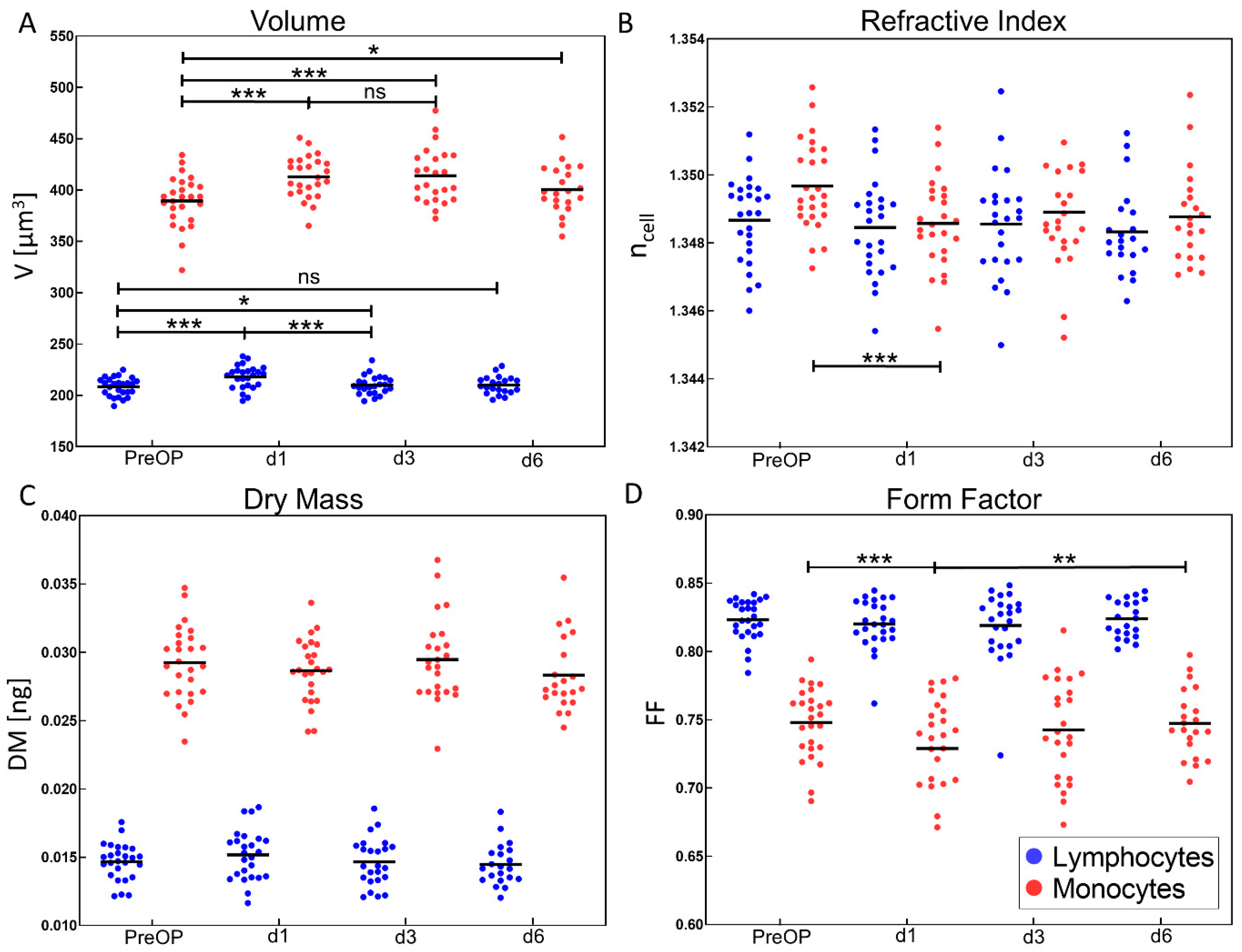
3.3. Cell Volume, Refractive Index and Form Factor Change Significantly during Perioperative Course
3.4. Synchronous Changes in Biophysical DHM Data, Flow Cytometric Markers, Routine Laboratory Parameters, and Drug Dosages Revealed by Bivariate Correlation
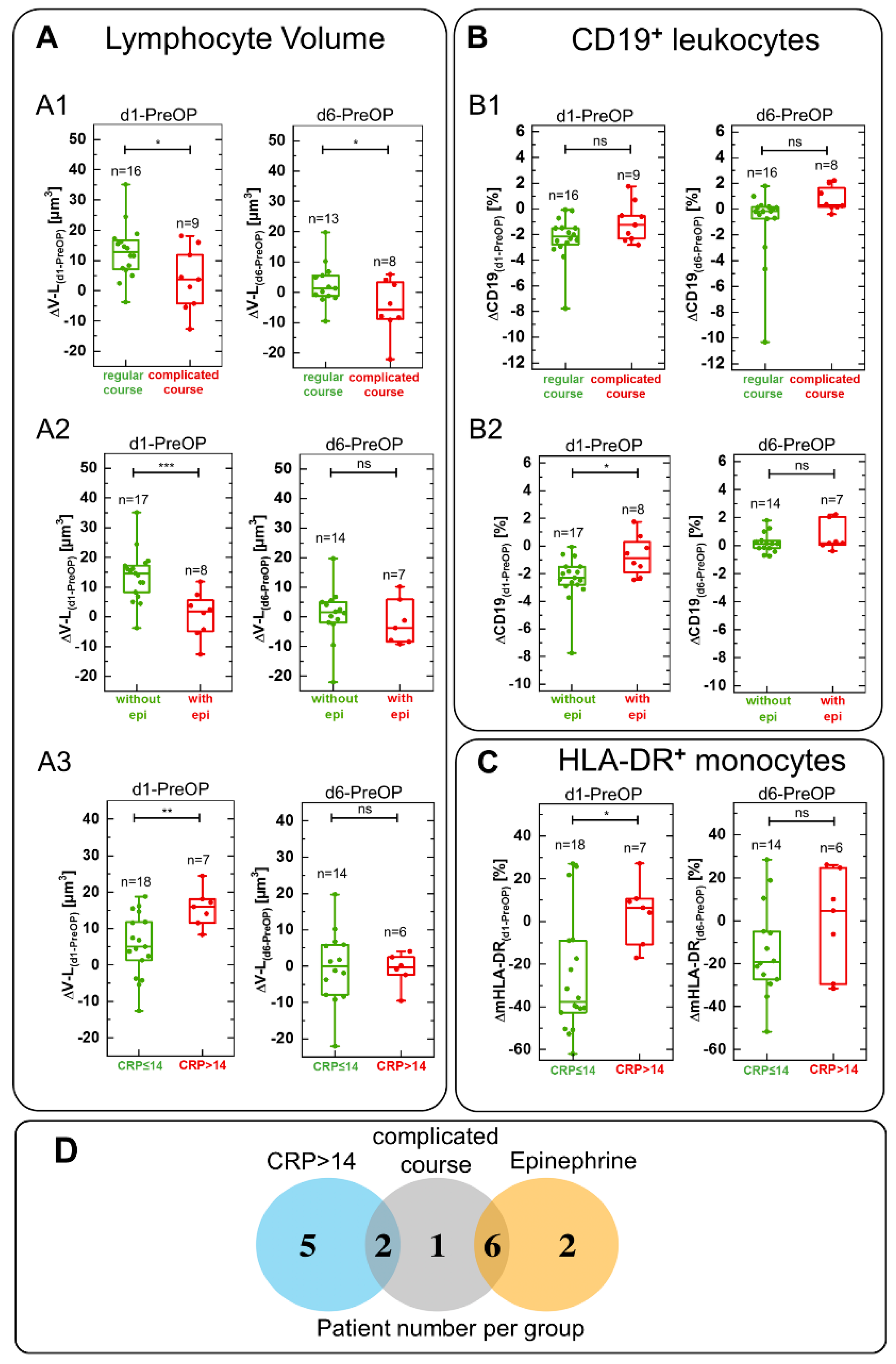
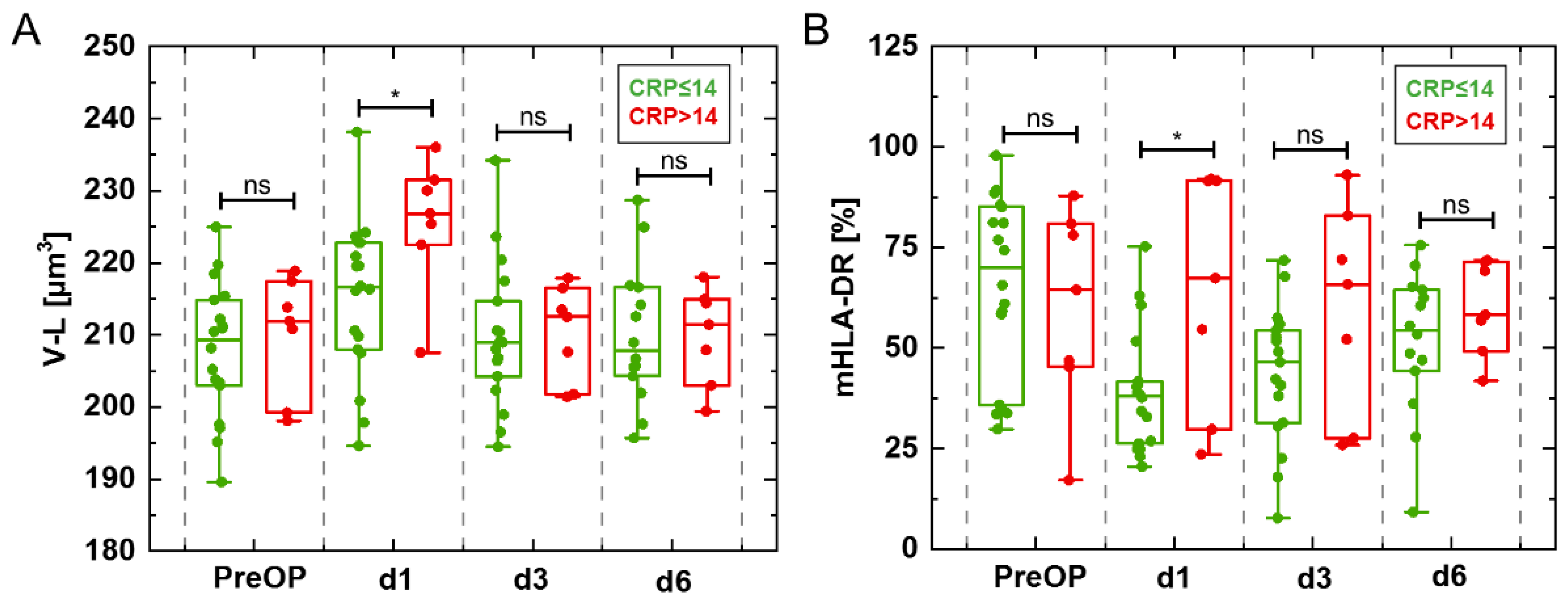
3.5. DHM Parameter Changes Correlated Significantly with Complicated Course, Epinephrine Treatment and Inflammation Marker CRP
4. Discussion
5. Conclusions and Future Perspectives
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abbasciano, R.G.; Lai, F.Y.; Roman, M.A.; Rizzello, A.; Pathak, S.; Ramzi, J.; Lucarelli, C.; Layton, G.R.; Kumar, T.; Wozniak, M.J.; et al. Activation of the Innate Immune Response and Organ Injury after Cardiac Surgery: A Systematic Review and Meta-Analysis of Randomised Trials and Analysis of Individual Patient Data from Randomised and Non-Randomised Studies. Br. J. Anaesth. 2021, 127, 365–375. [Google Scholar] [CrossRef] [PubMed]
- Warltier, D.C.; Laffey, J.G.; Boylan, J.F.; Cheng, D.C.H. The Systemic Inflammatory Response to Cardiac Surgery. Anesthesiology 2002, 97, 215–252. [Google Scholar] [CrossRef] [PubMed]
- Dieleman, J.M.; Peelen, L.M.; Coulson, T.G.; Tran, L.; Reid, C.M.; Smith, J.A.; Myles, P.S.; Pilcher, D. Age and Other Perioperative Risk Factors for Postoperative Systemic Inflammatory Response Syndrome after Cardiac Surgery. Br. J. Anaesth. 2017, 119, 637–644. [Google Scholar] [CrossRef] [Green Version]
- Becher, R.D.; Hoth, J.J.; Miller, P.R.; Meredith, J.W.; Chang, M.C. Systemic Inflammation Worsens Outcomes in Emergency Surgical Patients. J. Trauma Acute Care Surg. 2012, 72, 1140–1149. [Google Scholar] [CrossRef]
- Li, J.; Yang, L.; Wang, G.; Wang, Y.; Wang, C.; Shi, S. Severe Systemic Inflammatory Response Syndrome in Patients Following Total Aortic Arch Replacement with Deep Hypothermic Circulatory Arrest. J. Cardiothorac. Surg. 2019, 14, 217. [Google Scholar] [CrossRef] [PubMed]
- Lindman, B.R.; Goldstein, J.S.; Nassif, M.E.; Zajarias, A.; Novak, E.; Tibrewala, A.; Vatterott, A.M.; Lawler, C.; Damiano, R.J.; Moon, M.R.; et al. Systemic Inflammatory Response Syndrome after Transcatheter or Surgical Aortic Valve Replacement. Heart 2015, 101, 537–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Churpek, M.M.; Snyder, A.; Han, X.; Sokol, S.; Pettit, N.; Howell, M.D.; Edelson, D.P. Quick Sepsis-Related Organ Failure Assessment, Systemic Inflammatory Response Syndrome, and Early Warning Scores for Detecting Clinical Deterioration in Infected Patients Outside the Intensive Care Unit. Am. J. Respir. Crit. Care Med. 2017, 195, 906–911. [Google Scholar] [CrossRef] [Green Version]
- Zonneveld, R.; Molema, G.; Plötz, F.B. Analyzing Neutrophil Morphology, Mechanics, and Motility in Sepsis: Options and Challenges for Novel Bedside Technologies. Crit. Care Med. 2016, 44, 218–228. [Google Scholar] [CrossRef] [Green Version]
- Arora, P.; Gupta, P.K.; Lingaiah, R.; Mukhopadhyay, A.K. Volume, Conductivity, and Scatter Parameters of Leukocytes as Early Markers of Sepsis and Treatment Response. J. Lab. Physicians 2019, 11, 029–033. [Google Scholar] [CrossRef]
- Chaves, F.; Tierno, B.; Xu, D. Neutrophil Volume Distribution Width: A New Automated Hematologic Parameter for Acute Infection. Arch. Pathol. Lab. Med. 2006, 130, 378–380. [Google Scholar] [CrossRef]
- Crouser, E.D.; Parrillo, J.E.; Seymour, C.; Angus, D.C.; Bicking, K.; Tejidor, L.; Magari, R.; Careaga, D.; Williams, J.; Closser, D.R.; et al. Improved Early Detection of Sepsis in the ED With a Novel Monocyte Distribution Width Biomarker. Chest 2017, 152, 518–526. [Google Scholar] [CrossRef] [PubMed]
- Albertsmeier, M.; Prix, N.J.; Winter, H.; Bazhin, A.; Werner, J.; Angele, M.K. Monocyte-Dependent Suppression of T-Cell Function in Postoperative Patients and Abdominal Sepsis. Shock 2017, 48, 651–656. [Google Scholar] [CrossRef] [PubMed]
- Monneret, G.; Venet, F. Sepsis-Induced Immune Alterations Monitoring by Flow Cytometry as a Promising Tool for Individualized Therapy: MECHANISMS SUSTAINING SEPSIS-INDUCED IMMUNOSUPPRESSION. Cytometry 2016, 90, 376–386. [Google Scholar] [CrossRef] [PubMed]
- Greve, B.; Beller, C.; Cassens, U.; Sibrowski, W.; Göhde, W. The Impact of Erythrocyte Lysing Procedures on the Recovery of Hematopoietic Progenitor Cells in Flow Cytometric Analysis. Stem Cells 2006, 24, 793–799. [Google Scholar] [CrossRef]
- Greve, B.; Beller, C.; Cassens, U.; Sibrowski, W.; Severin, E.; Göhde, W. High-Grade Loss of Leukocytes and Hematopoietic Progenitor Cells Caused by Erythrocyte-Lysing Procedures for Flow Cytometric Analyses. J. Hematother. Stem Cell Res. 2003, 12, 321–330. [Google Scholar] [CrossRef]
- Kong, K.; Kendall, C.; Stone, N.; Notingher, I. Raman Spectroscopy for Medical Diagnostics—From in-Vitro Biofluid Assays to in-Vivo Cancer Detection. Adv. Drug Deliv. Rev. 2015, 89, 121–134. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.; Kim, K.; Jung, J.; Heo, J.; Cho, S.; Lee, S.; Chang, G.; Jo, Y.; Park, H.; Park, Y. Quantitative Phase Imaging Techniques for the Study of Cell Pathophysiology: From Principles to Applications. Sensors 2013, 13, 4170–4191. [Google Scholar] [CrossRef]
- Park, Y.; Depeursinge, C.; Popescu, G. Quantitative Phase Imaging in Biomedicine. Nat. Photonics 2018, 12, 578–589. [Google Scholar] [CrossRef]
- Kemper, B.; von Bally, G. Digital Holographic Microscopy for Live Cell Applications and Technical Inspection. Appl. Opt. 2008, 47, A52. [Google Scholar] [CrossRef]
- Hoffmann, E.K.; Lambert, I.H.; Pedersen, S.F. Physiology of Cell Volume Regulation in Vertebrates. Physiol. Rev. 2009, 89, 193–277. [Google Scholar] [CrossRef]
- Liu, P.Y.; Chin, L.K.; Ser, W.; Chen, H.F.; Hsieh, C.-M.; Lee, C.-H.; Sung, K.-B.; Ayi, T.C.; Yap, P.H.; Liedberg, B.; et al. Cell Refractive Index for Cell Biology and Disease Diagnosis: Past, Present and Future. Lab. Chip 2016, 16, 634–644. [Google Scholar] [CrossRef] [PubMed]
- Zangle, T.A.; Teitell, M.A. Live-Cell Mass Profiling: An Emerging Approach in Quantitative Biophysics. Nat. Methods 2014, 11, 1221–1228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bardyn, M.; Rappaz, B.; Jaferzadeh, K.; Crettaz, D.; Tissot, J.-D.; Moon, I.; Turcatti, G.; Lion, N.; Prudent, M. Red Blood Cells Ageing Markers: A Multi-Parametric Analysis. Blood Transfus. 2017, 15, 239. [Google Scholar] [CrossRef] [PubMed]
- Seo, K.W.; Seo, E.; Lee, S.J. Cellular Imaging Using Phase Holographic Microscopy: For the Study of Pathophysiology of Red Blood Cells and Human Umbilical Vein Endothelial Cells. J. Vis. 2014, 17, 235–244. [Google Scholar] [CrossRef]
- Marquet, P.; Depeursinge, C.; Magistretti, P.J. Review of Quantitative Phase-Digital Holographic Microscopy: Promising Novel Imaging Technique to Resolve Neuronal Network Activity and Identify Cellular Biomarkers of Psychiatric Disorders. Neurophoton 2014, 1, 020901. [Google Scholar] [CrossRef] [Green Version]
- Kemper, B.; Carl, D.; Schnekenburger, J.; Bredebusch, I.; Schäfer, M.; Domschke, W.; von Bally, G. Investigation of Living Pancreas Tumor Cells by Digital Holographic Microscopy. J. Biomed. Opt. 2006, 11, 034005. [Google Scholar] [CrossRef]
- Ekpenyong, A.E.; Man, S.M.; Achouri, S.; Bryant, C.E.; Guck, J.; Chalut, K.J. Bacterial Infection of Macrophages Induces Decrease in Refractive Index. J. Biophoton. 2013, 6, 393–397. [Google Scholar] [CrossRef]
- Kastl, L.; Isbach, M.; Dirksen, D.; Schnekenburger, J.; Kemper, B. Quantitative Phase Imaging for Cell Culture Quality Control: Label-Free Cell Culture Quality Control. Cytometry 2017, 91, 470–481. [Google Scholar] [CrossRef] [Green Version]
- Bettenworth, D.; Lenz, P.; Krausewitz, P.; Brückner, M.; Ketelhut, S.; Domagk, D.; Kemper, B. Quantitative Stain-Free and Continuous Multimodal Monitoring of Wound Healing In Vitro with Digital Holographic Microscopy. PLoS ONE 2014, 9, e107317. [Google Scholar] [CrossRef] [Green Version]
- Kühn, J.; Shaffer, E.; Mena, J.; Breton, B.; Parent, J.; Rappaz, B.; Chambon, M.; Emery, Y.; Magistretti, P.; Depeursinge, C.; et al. Label-Free Cytotoxicity Screening Assay by Digital Holographic Microscopy. ASSAY Drug Dev. Technol. 2013, 11, 101–107. [Google Scholar] [CrossRef] [Green Version]
- Greve, B.; Sheikh-Mounessi, F.; Kemper, B.; Ernst, I.; Götte, M.; Eich, H.T. Survivin, a Target to Modulate the Radiosensitivity of Ewing’s Sarcoma. Strahlenther Onkol 2012, 188, 1038–1047. [Google Scholar] [CrossRef] [PubMed]
- Lenz, P.; Bettenworth, D.; Krausewitz, P.; Brückner, M.; Ketelhut, S.; von Bally, G.; Domagk, D.; Kemper, B. Digital Holographic Microscopy Quantifies the Degree of Inflammation in Experimental Colitis. Integr. Biol. 2013, 5, 624–630. [Google Scholar] [CrossRef] [PubMed]
- Bokemeyer, A.; Tepasse, P.R.; Quill, L.; Lenz, P.; Rijcken, E.; Vieth, M.; Ding, N.; Ketelhut, S.; Rieder, F.; Kemper, B.; et al. Quantitative Phase Imaging Using Digital Holographic Microscopy Reliably Assesses Morphology and Reflects Elastic Properties of Fibrotic Intestinal Tissue. Sci. Rep. 2019, 9, 19388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bettenworth, D.; Bokemeyer, A.; Poremba, C.; Ding, N.S.; Ketelhut, S.; Lenz, P.; Kemper, B. Quantitative Phase Microscopy for Evaluation of Intestinal Inflammation and Wound Healing Utilizing Label-Free Biophysical Markers. Histol. Histopathol. 2018, 33, 417–432. [Google Scholar] [CrossRef]
- Yoon, J.; Jo, Y.; Kim, M.; Kim, K.; Lee, S.; Kang, S.-J.; Park, Y. Identification of Non-Activated Lymphocytes Using Three-Dimensional Refractive Index Tomography and Machine Learning. Sci. Rep. 2017, 7, 6654. [Google Scholar] [CrossRef] [Green Version]
- Delirezh, N. Comparison the Effects of Two Monocyte Isolation Methods, Plastic Adherence and Magnetic Activated Cell Sorting Methods, on Phagocytic Activity of Generated Dendritic Cells. Cell J. 2013, 15, 6. [Google Scholar]
- Nielsen, M.C.; Andersen, M.N.; Møller, H.J. Monocyte Isolation Techniques Significantly Impact the Phenotype of Both Isolated Monocytes and Derived Macrophages in Vitro. Immunology 2020, 159, 63–74. [Google Scholar] [CrossRef]
- Lenz, P.; Brückner, M.; Ketelhut, S.; Heidemann, J.; Kemper, B.; Bettenworth, D. Multimodal Quantitative Phase Imaging with Digital Holographic Microscopy Accurately Assesses Intestinal Inflammation and Epithelial Wound Healing. JoVE 2016, 54460. [Google Scholar] [CrossRef]
- Kemper, B.; Carl, D.; Höink, A.; von Bally, G.; Bredebusch, I.; Schnekenburger, J. Modular Digital Holographic Microscopy System for Marker Free Quantitative Phase Contrast Imaging of Living Cells; Grzymala, R., Haeberle, O., Eds.; SPIE: Strasbourg, France; p. 61910T.
- Min, J.; Yao, B.; Trendafilova, V.; Ketelhut, S.; Kastl, L.; Greve, B.; Kemper, B. Quantitative Phase Imaging of Cells in a Flow Cytometry Arrangement Utilizing Michelson Interferometer-based Off-axis Digital Holographic Microscopy. J. Biophotonics 2019, 12, e201900085. [Google Scholar] [CrossRef]
- Marquet, P.; Rappaz, B.; Magistretti, P.J.; Cuche, E.; Emery, Y.; Colomb, T.; Depeursinge, C. Digital Holographic Microscopy: A Noninvasive Contrast Imaging Technique Allowing Quantitative Visualization of Living Cells with Subwavelength Axial Accuracy. Opt. Lett. 2005, 30, 468. [Google Scholar] [CrossRef] [Green Version]
- Popescu, G.; Park, Y.; Lue, N.; Best-Popescu, C.; Deflores, L.; Dasari, R.R.; Feld, M.S.; Badizadegan, K. Optical Imaging of Cell Mass and Growth Dynamics. Am. J. Physiol. -Cell Physiol. 2008, 295, C538–C544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barer, R. Interference Microscopy and Mass Determination. Nature 1952, 169, 366–367. [Google Scholar] [CrossRef] [PubMed]
- Russ, J.C.; Neal, F.B. The Image Processing Handbook, 0 ed.; CRC Press: Boca Raton, FL, USA, 2018; ISBN 978-1-315-21411-5. [Google Scholar]
- Bradley Efron, R.J.T.A. Introduction to the Bootstrap; Monographs on Statistics and Applied Probability; Chapman & Hall/CRC: Boca Raton, FL, USA, 1994. [Google Scholar]
- Sulzgruber, P.; Thaler, B.; Koller, L.; Baumgartner, J.; Pilz, A.; Steininger, M.; Schnaubelt, S.; Fleck, T.; Laufer, G.; Steinlechner, B.; et al. CD4+CD28null T Lymphocytes Are Associated with the Development of Atrial Fibrillation after Elective Cardiac Surgery. Sci. Rep. 2018, 8, 9624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Day, J.R.S.; Taylor, K.M. The Systemic Inflammatory Response Syndrome and Cardiopulmonary Bypass. Int. J. Surg. 2005, 3, 129–140. [Google Scholar] [CrossRef] [Green Version]
- Leães, P.E.; Neumann, J.; Jung, L.A.; Blacher, C.; Lucchese, F.; Clausell, N. Lymphocyte’s Activation and Apoptosis After Coronary Artery Bypass Graft: A Comparative Study of Two Membrane Oxygenators–One with and Another without a Venous-Arterial Shunt. ASAIO J. 2004, 50, 611–618. [Google Scholar] [CrossRef] [PubMed]
- Warren, O.; Smith, A.; Alexiou, C.; Rogers, P.; Jawad, C.; Vincent, N.; Darzi, A.; Athanasiou, T. The Inflammatory Response to Cardiopulmonary Bypass: Part 1—Mechanisms of Pathogenesis. J. Cardiothorac. Vasc. Anesth. 2009, 23, 223–231. [Google Scholar] [CrossRef]
- Likosky, D.S.; Wallace, A.S.; Prager, R.L.; Jacobs, J.P.; Zhang, M.; Harrington, S.D.; Saha-Chaudhuri, P.; Theurer, P.F.; Fishstrom, A.; Dokholyan, R.S.; et al. Sources of Variation in Hospital-Level Infection Rates after Coronary Artery Bypass Grafting: An Analysis of The Society of Thoracic Surgeons Adult Heart Surgery Database. Ann. Thorac. Surg. 2015, 100, 1570–1576. [Google Scholar] [CrossRef] [Green Version]
- Mocanu, V.; Buth, K.J.; Johnston, L.B.; Davis, I.; Hirsch, G.M.; Légaré, J.-F. The Importance of Continued Quality Improvement Efforts in Monitoring Hospital-Acquired Infection Rates: A Cardiac Surgery Experience. Ann. Thorac. Surg. 2015, 99, 2061–2069. [Google Scholar] [CrossRef] [Green Version]
- Serraino, G.F.; Provenzano, M.; Jiritano, F.; Michael, A.; Ielapi, N.; Mastroroberto, P.; Andreucci, M.; Serra, R. Risk Factors for Acute Kidney Injury and Mortality in High Risk Patients Undergoing Cardiac Surgery. PLoS ONE 2021, 16, e0252209. [Google Scholar] [CrossRef]
- Mossanen, J.C.; Jansen, T.U.; Pracht, J.; Liepelt, A.; Buendgens, L.; Stoppe, C.; Goetzenich, A.; Simon, T.-P.; Autschbach, R.; Marx, G.; et al. Elevated Circulating CD14++CD16+ Intermediate Monocytes Are Independently Associated with Extracardiac Complications after Cardiac Surgery. Sci. Rep. 2020, 10, 947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stoppelkamp, S.; Veseli, K.; Stang, K.; Schlensak, C.; Wendel, H.P.; Walker, T. Identification of Predictive Early Biomarkers for Sterile-SIRS after Cardiovascular Surgery. PLoS ONE 2015, 10, e0135527. [Google Scholar] [CrossRef] [PubMed]
- Boss, D.; Kühn, J.; Jourdain, P.; Depeursinge, C.; Magistretti, P.J.; Marquet, P. Measurement of Absolute Cell Volume, Osmotic Membrane Water Permeability, and Refractive Index of Transmembrane Water and Solute Flux by Digital Holographic Microscopy. J. Biomed. Opt. 2013, 18, 036007. [Google Scholar] [CrossRef] [PubMed]
- Pavillon, N.; Kühn, J.; Moratal, C.; Jourdain, P.; Depeursinge, C.; Magistretti, P.J.; Marquet, P. Early Cell Death Detection with Digital Holographic Microscopy. PLoS ONE 2012, 7, e30912. [Google Scholar] [CrossRef] [PubMed]
- Jaferzadeh, K.; Moon, I. Quantitative Investigation of Red Blood Cell Three-Dimensional Geometric and Chemical Changes in the Storage Lesion Using Digital Holographic Microscopy. J. Biomed. Opt. 2015, 20, 111218. [Google Scholar] [CrossRef] [PubMed]
- Raimondi, F.; Ferrara, T.; Capasso, L. Automated Determination of Neutrophil Volume as Screening Test for Late-Onset Sepsis in Very Low Birth Infants. Pediatric Infect. Dis. J. 2010, 29, 288. [Google Scholar] [CrossRef]
- Bhargava, M.; Saluja, S.; Sindhuri, U.; Saraf, A.; Sharma, P. Elevated Mean Neutrophil Volume+CRP Is a Highly Sensitive and Specific Predictor of Neonatal Sepsis. Int. Jnl. Lab. Hem. 2014, 36, e11–e14. [Google Scholar] [CrossRef]
- Lee, A.-J.; Kim, S.-G. Mean Cell Volumes of Neutrophils and Monocytes Are Promising Markers of Sepsis in Elderly Patients. Blood Res. 2013, 48, 193. [Google Scholar] [CrossRef] [Green Version]
- Parker, D. CD80/CD86 Signaling Contributes to the Proinflammatory Response of Staphylococcus Aureus in the Airway. Cytokine 2018, 107, 130–136. [Google Scholar] [CrossRef]
- Chalut, K.J.; Ekpenyong, A.E.; Clegg, W.L.; Melhuish, I.C.; Guck, J. Quantifying Cellular Differentiation by Physical Phenotype Using Digital Holographic Microscopy. Integr. Biol. (Camb) 2012, 4, 280–284. [Google Scholar] [CrossRef]
- Khmaladze, A.; Matz, R.L.; Epstein, T.; Jasensky, J.; Banaszak Holl, M.M.; Chen, Z. Cell Volume Changes during Apoptosis Monitored in Real Time Using Digital Holographic Microscopy. J. Struct. Biol. 2012, 178, 270–278. [Google Scholar] [CrossRef] [PubMed]
- Marie, C.; Muret, J.; Fitting, C.; Losser, M.R.; Payen, D.; Cavaillon, J.M. Reduced Ex Vivo Interleukin-8 Production by Neutrophils in Septic and Nonseptic Systemic Inflammatory Response Syndrome. Blood 1998, 91, 3439–3446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perros, A.J.; Esguerra-Lallen, A.; Rooks, K.; Chong, F.; Engkilde-Pedersen, S.; Faddy, H.M.; Hewlett, E.; Naidoo, R.; Tung, J.-P.; Fraser, J.F.; et al. Coronary Artery Bypass Grafting Is Associated with Immunoparalysis of Monocytes and Dendritic Cells. J. Cell Mol. Med. 2020, 24, 4791–4803. [Google Scholar] [CrossRef]
- Tank, A.W.; Lee Wong, D. Peripheral and Central Effects of Circulating Catecholamines. Compr. Physiol. 2015, 5, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Dimitrov, S.; Lange, T.; Born, J. Selective Mobilization of Cytotoxic Leukocytes by Epinephrine. J. Immunol. 2010, 184, 503–511. [Google Scholar] [CrossRef] [Green Version]
- Mustard, J.F.; Packham, M.A. Platelets, Thrombosis and Drugs. Drugs 1975, 9, 19–76. [Google Scholar] [CrossRef]
- Ichikawa, J.; Osada, Y.; Kodaka, M.; Nishiyama, K.; Komori, M. Association Between Platelet Count and Postoperative Blood Loss in Patients Undergoing Cardiac Surgery With Cardiopulmonary Bypass and Fresh Frozen Plasma Administration Guided by Thromboelastometry. Circ. J. 2018, 82, 677–683. [Google Scholar] [CrossRef] [Green Version]
- Maisel, A.S.; Knowlton, K.U.; Fowler, P.; Rearden, A.; Ziegler, M.G.; Motulsky, H.J.; Insel, P.A.; Michel, M.C. Adrenergic Control of Circulating Lymphocyte Subpopulations. Effects of Congestive Heart Failure, Dynamic Exercise, and Terbutaline Treatment. J. Clin. Investig. 1990, 85, 462–467. [Google Scholar] [CrossRef] [Green Version]
- Jonasson, L.; Backteman, K.; Ernerudh, J. Loss of Natural Killer Cell Activity in Patients with Coronary Artery Disease. Atherosclerosis 2005, 183, 316–321. [Google Scholar] [CrossRef]
- Sproston, N.R.; Ashworth, J.J. Role of C-Reactive Protein at Sites of Inflammation and Infection. Front. Immunol. 2018, 9, 754. [Google Scholar] [CrossRef]
- Szalai, A.J.; van Ginkel, F.W.; Dalrymple, S.A.; Murray, R.; McGhee, J.R.; Volanakis, J.E. Testosterone and IL-6 Requirements for Human C-Reactive Protein Gene Expression in Transgenic Mice. J. Immunol. 1998, 160, 5294–5299. [Google Scholar] [PubMed]
- Rani, M.; Nicholson, S.E.; Zhang, Q.; Schwacha, M.G. Damage-Associated Molecular Patterns (DAMPs) Released after Burn Are Associated with Inflammation and Monocyte Activation. Burns 2017, 43, 297–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shubin, N.J.; Pham, T.N.; Staudenmayer, K.L.; Parent, B.A.; Qiu, Q.; O’Keefe, G.E. A Potential Mechanism for Immune Suppression by Beta-Adrenergic Receptor Stimulation Following Traumatic Injury. J. Innate Immun. 2018, 10, 202–214. [Google Scholar] [CrossRef]
- Xin, L.; Xiao, W.; Che, L.; Liu, J.; Miccio, L.; Bianco, V.; Memmolo, P.; Ferraro, P.; Li, X.; Pan, F. Label-Free Assessment of the Drug Resistance of Epithelial Ovarian Cancer Cells in a Microfluidic Holographic Flow Cytometer Boosted through Machine Learning. ACS Omega 2021, 6, 31046–31057. [Google Scholar] [CrossRef] [PubMed]
- Dannhauser, D.; Rossi, D.; Causa, F.; Memmolo, P.; Finizio, A.; Wriedt, T.; Hellmers, J.; Eremin, Y.; Ferraro, P.; Netti, P.A. Optical Signature of Erythrocytes by Light Scattering in Microfluidic Flows. Lab. Chip 2015, 15, 3278–3285. [Google Scholar] [CrossRef] [Green Version]
- Ugele, M.; Weniger, M.; Stanzel, M.; Bassler, M.; Krause, S.W.; Friedrich, O.; Hayden, O.; Richter, L. Label-Free High-Throughput Leukemia Detection by Holographic Microscopy. Adv. Sci. 2018, 5, 1800761. [Google Scholar] [CrossRef] [PubMed]
- Girshovitz, P.; Shaked, N.T. Fast Phase Processing in Off-Axis Holography Using Multiplexing with Complex Encoding and Live-Cell Fluctuation Map Calculation in Real-Time. Opt. Express 2015, 23, 8773–8787. [Google Scholar] [CrossRef]
- Backoach, O.; Kariv, S.; Girshovitz, P.; Shaked, N.T. Fast Phase Processing in Off-Axis Holography by CUDA Including Parallel Phase Unwrapping. Opt. Express 2016, 24, 3177–3188. [Google Scholar] [CrossRef]
- Nissim, N.; Dudaie, M.; Barnea, I.; Shaked, N.T. Real-Time Stain-Free Classification of Cancer Cells and Blood Cells Using Interferometric Phase Microscopy and Machine Learning. Cytom. A 2021, 99, 511–523. [Google Scholar] [CrossRef]
- Belashov, A.V.; Zhikhoreva, A.A.; Belyaeva, T.N.; Salova, A.V.; Kornilova, E.S.; Semenova, I.V.; Vasyutinskii, O.S. Machine Learning Assisted Classification of Cell Lines and Cell States on Quantitative Phase Images. Cells 2021, 10, 2587. [Google Scholar] [CrossRef]
- Hohlstein, P.; Gussen, H.; Bartneck, M.; Warzecha, K.T.; Roderburg, C.; Buendgens, L.; Trautwein, C.; Koch, A.; Tacke, F. Prognostic Relevance of Altered Lymphocyte Subpopulations in Critical Illness and Sepsis. JCM 2019, 8, 353. [Google Scholar] [CrossRef] [Green Version]
- Gawdat, K.; Legere, S.; Wong, C.; Myers, T.; Marshall, J.S.; Hassan, A.; Brunt, K.R.; Kienesberger, P.C.; Pulinilkunnil, T.; Legare, J.-F. Changes in Circulating Monocyte Subsets (CD16 Expression) and Neutrophil-to-Lymphocyte Ratio Observed in Patients Undergoing Cardiac Surgery. Front. Cardiovasc. Med. 2017, 4. [Google Scholar] [CrossRef] [Green Version]
- Hewing, B.; Ellerbroek, R.; Au, S.; Stangl, V.; Dreger, H.; Laule, M.; Grubitzsch, H.; Knebel, F.; Baumann, G.; Ludwig, A.; et al. Levels of Circulating Intermediate Monocytes Decrease after Aortic Valve Replacement in Patients with Severe Aortic Stenosis. Thromb Haemost 2017, 117, 2346–2355. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, A.; Fukuzawa, K.; Yamashita, T.; Yoshida, A.; Sasaki, N.; Emoto, T.; Takei, A.; Fujiwara, R.; Nakanishi, T.; Yamashita, S.; et al. Circulating Intermediate CD14++CD16+monocytes Are Increased in Patients with Atrial Fibrillation and Reflect the Functional Remodelling of the Left Atrium. Europace 2016, euv422. [Google Scholar] [CrossRef]
- Holmannova, D.; Kolackova, M.; Kunes, P.; Krejsek, J.; Mandak, J.; Andrys, C. Impact of Cardiac Surgery on the Expression of CD40, CD80, CD86 and HLA-DR on B Cells and Monocytes. Perfusion 2016, 31, 391–400. [Google Scholar] [CrossRef]
- Greco, M.; Mazzei, A.; Palumbo, C.; Verri, T. Flow Cytometric Analysis of Monocytes Polarization and Reprogramming from Inflammatory to Immunosuppressive Phase during Sepsis. 14.
- Coillie, S.; Wiernicki, B.; Xu, J. Molecular and Cellular Functions of CTLA-4. Adv. Exp. Med. Biol. 2020, 7–32. [Google Scholar] [CrossRef]
- Quadrini, K.J.; Patti-Diaz, L.; Maghsoudlou, J.; Cuomo, J.; Hedrick, M.N.; McCloskey, T.W. A Flow Cytometric Assay for HLA‐DR Expression on Monocytes Validated as a Biomarker for Enrollment in Sepsis Clinical Trials. Cytometry 2021, 100, 103–114. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Correlations between DHM parameter changes and alterations of flow cytometric markers and epinephrine dose prior- and post-surgery (d1-PreOP) Δ indicates parameter differences between measurement days d1 and PreOP (d1-PreOP) | ||
| Parameter 1 | Parameter 2 | Pearson Correlation Coefficient |
| ∆V-L | ∆CD19abs | −0.514 ** |
| ∆V-L | ∆Epinephrine dose | −0.484 * |
| ∆V-M | ∆Necrosis/late ∆apoptosis | 0.479 * |
| ∆ncell-L | ∆CD86 | 0.464 * |
| ∆FF-M | ∆mHLA-DR | 0.464 * |
| ∆ncell-M | ∆Necrosis/late apoptosis | −0.44 * |
| ∆V-M | ∆ncell-M | −0.431 * |
| ∆ncell-M | ∆mCD206 | 0.405 * |
| ∆FF-M | ∆ncell-M | 0.401 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Steike, D.R.; Hessler, M.; Korsching, E.; Lehmann, F.; Schmidt, C.; Ertmer, C.; Schnekenburger, J.; Eich, H.T.; Kemper, B.; Greve, B. Digital Holographic Microscopy for Label-Free Detection of Leukocyte Alternations Associated with Perioperative Inflammation after Cardiac Surgery. Cells 2022, 11, 755. https://doi.org/10.3390/cells11040755
Steike DR, Hessler M, Korsching E, Lehmann F, Schmidt C, Ertmer C, Schnekenburger J, Eich HT, Kemper B, Greve B. Digital Holographic Microscopy for Label-Free Detection of Leukocyte Alternations Associated with Perioperative Inflammation after Cardiac Surgery. Cells. 2022; 11(4):755. https://doi.org/10.3390/cells11040755
Chicago/Turabian StyleSteike, David Rene, Michael Hessler, Eberhard Korsching, Florian Lehmann, Christina Schmidt, Christian Ertmer, Jürgen Schnekenburger, Hans Theodor Eich, Björn Kemper, and Burkhard Greve. 2022. "Digital Holographic Microscopy for Label-Free Detection of Leukocyte Alternations Associated with Perioperative Inflammation after Cardiac Surgery" Cells 11, no. 4: 755. https://doi.org/10.3390/cells11040755