
Subcutaneous Stromal Cells and Visceral Adipocyte Size Are Determinants of Metabolic Flexibility in Obesity and in Response to Weight Loss Surgery
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Human Cohorts and Tissue Collection
2.2. Adipose Tissue Digestion and Isolation of Adipocytes and Stromal Cells
2.3. Flow Cytometry Analyses
2.4. Statistical Analyses
3. Results
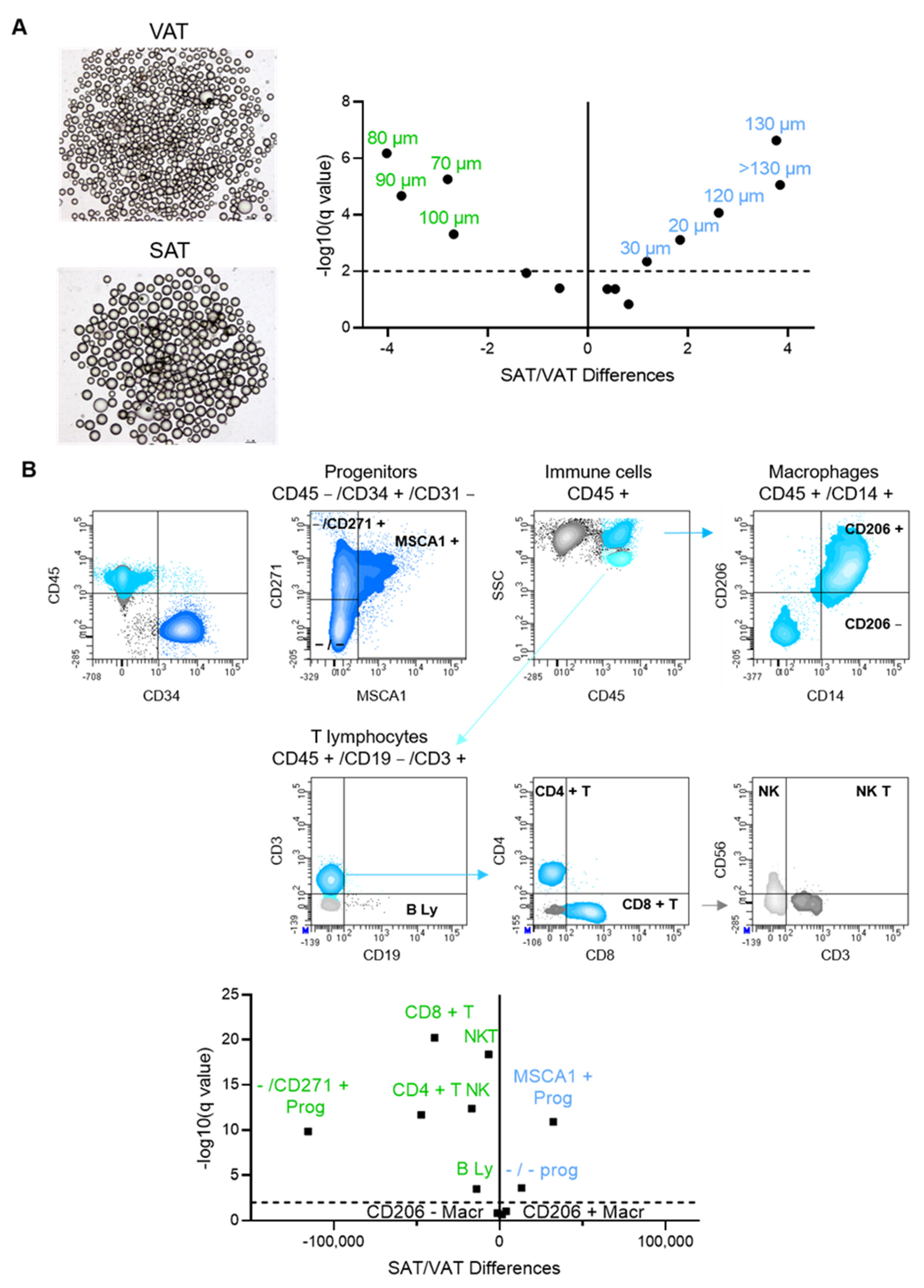
3.1. Fat Depot-Specific Cell Phenotypes in Patients with Severe Obesity
3.2. Cell Phenotypes of Expanded SAT and VAT Associated with Impaired Metabolic Flexibility in Obesity

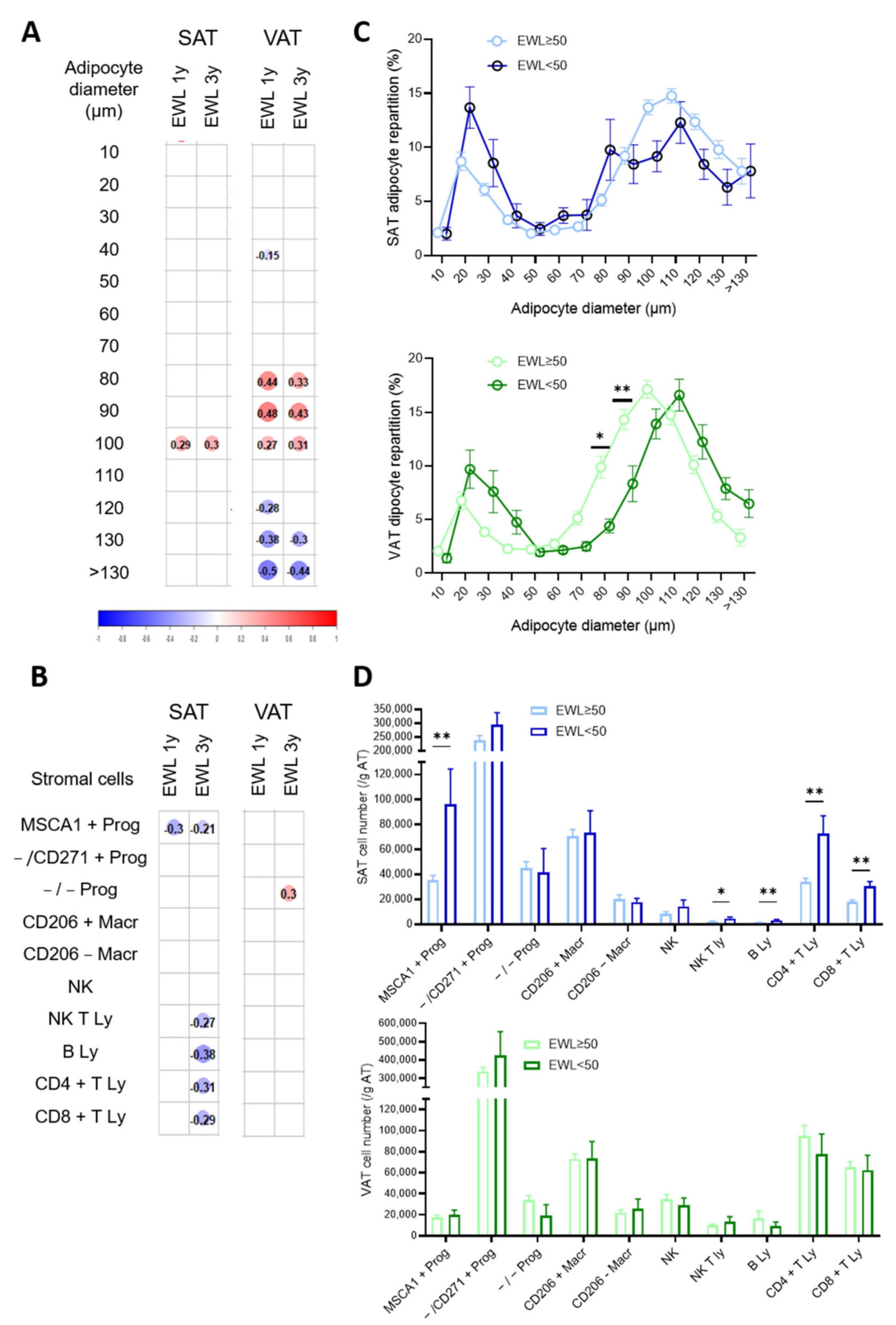
3.3. Cell Phenotypes of Expanded SAT and VAT Associated with Weight Loss at 1 and 3 Years after Bariatric Surgery
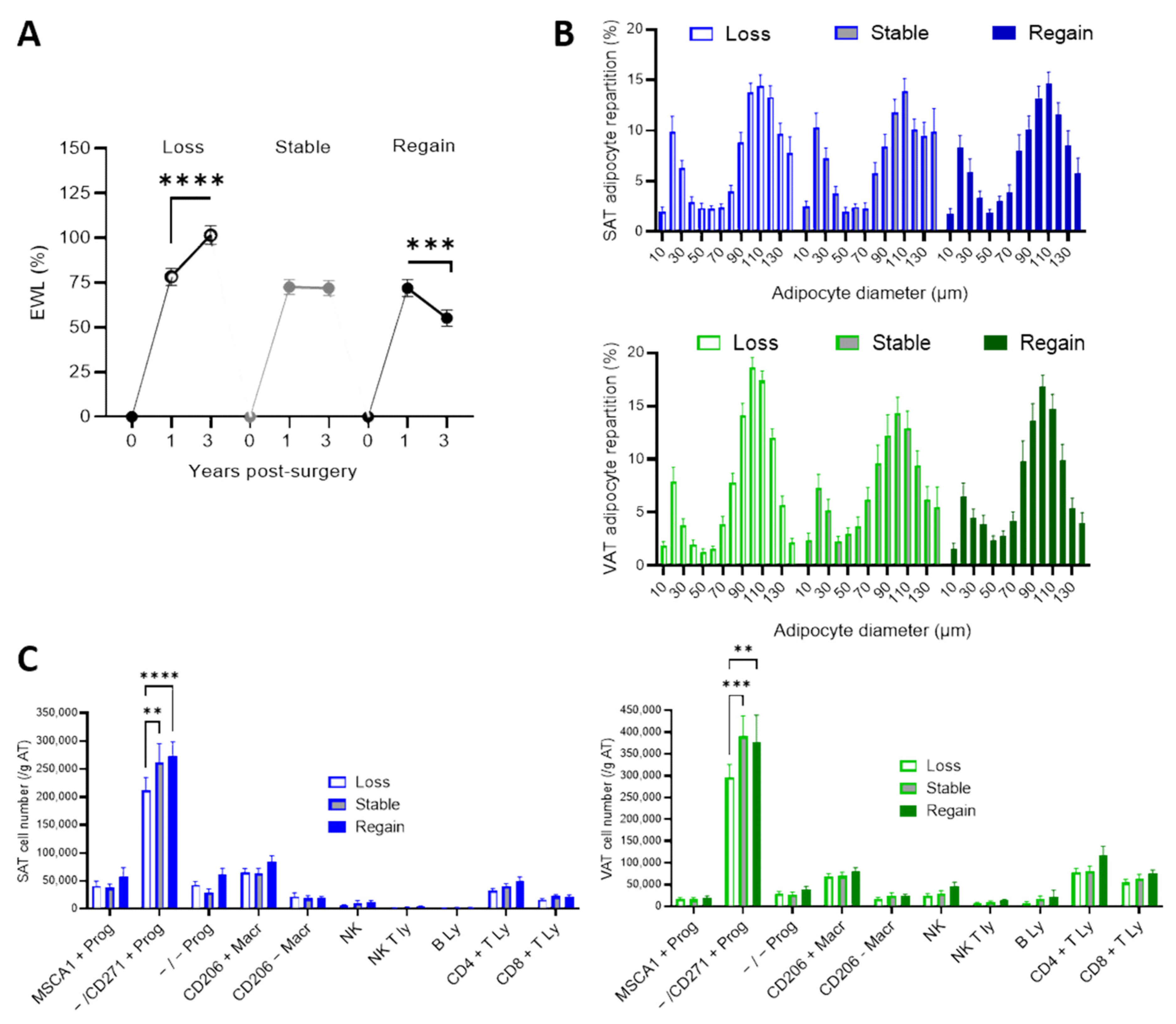
3.4. Weight Trajectories between 1 and 3 Years Post-Bariatric Surgery
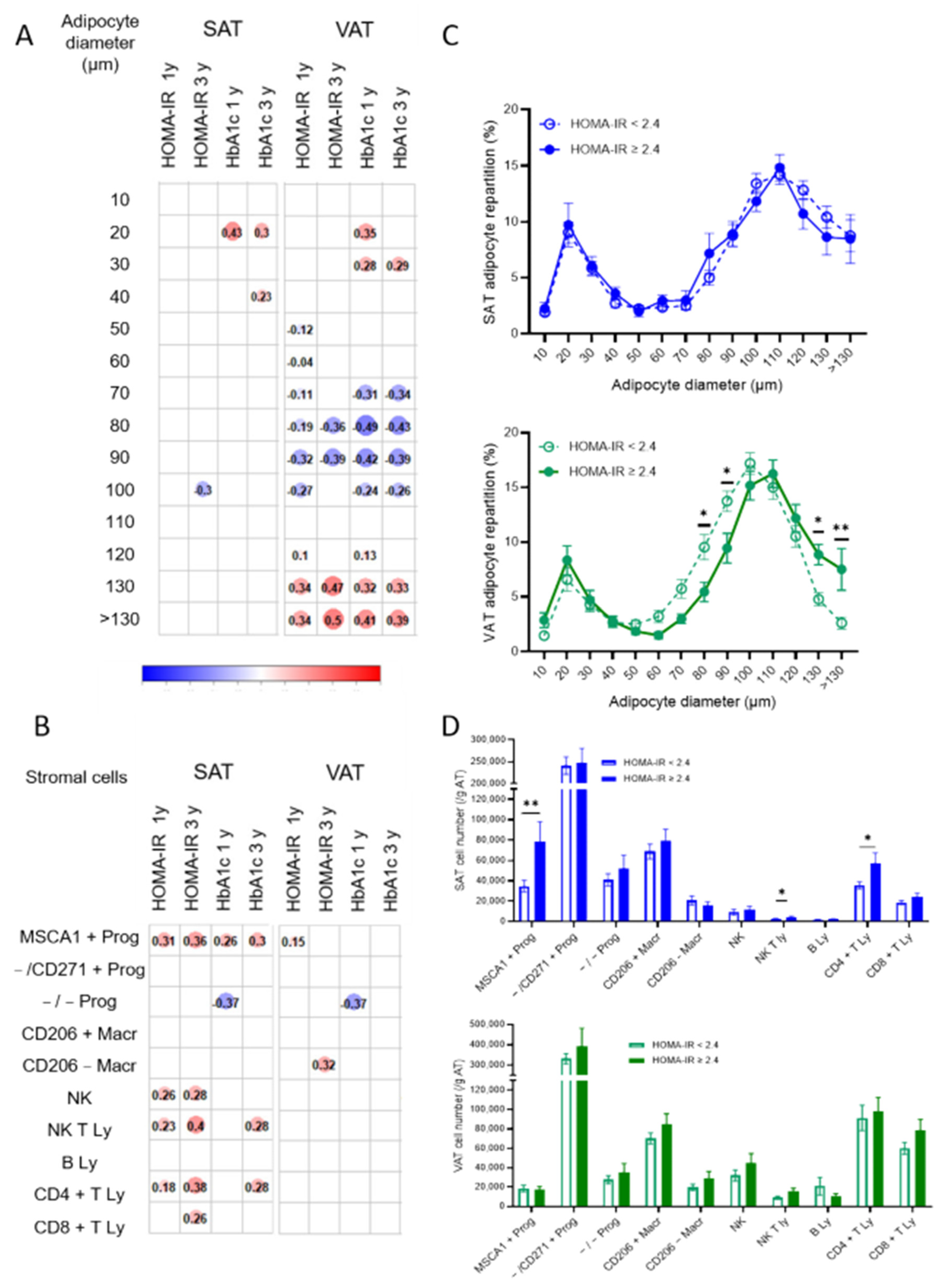
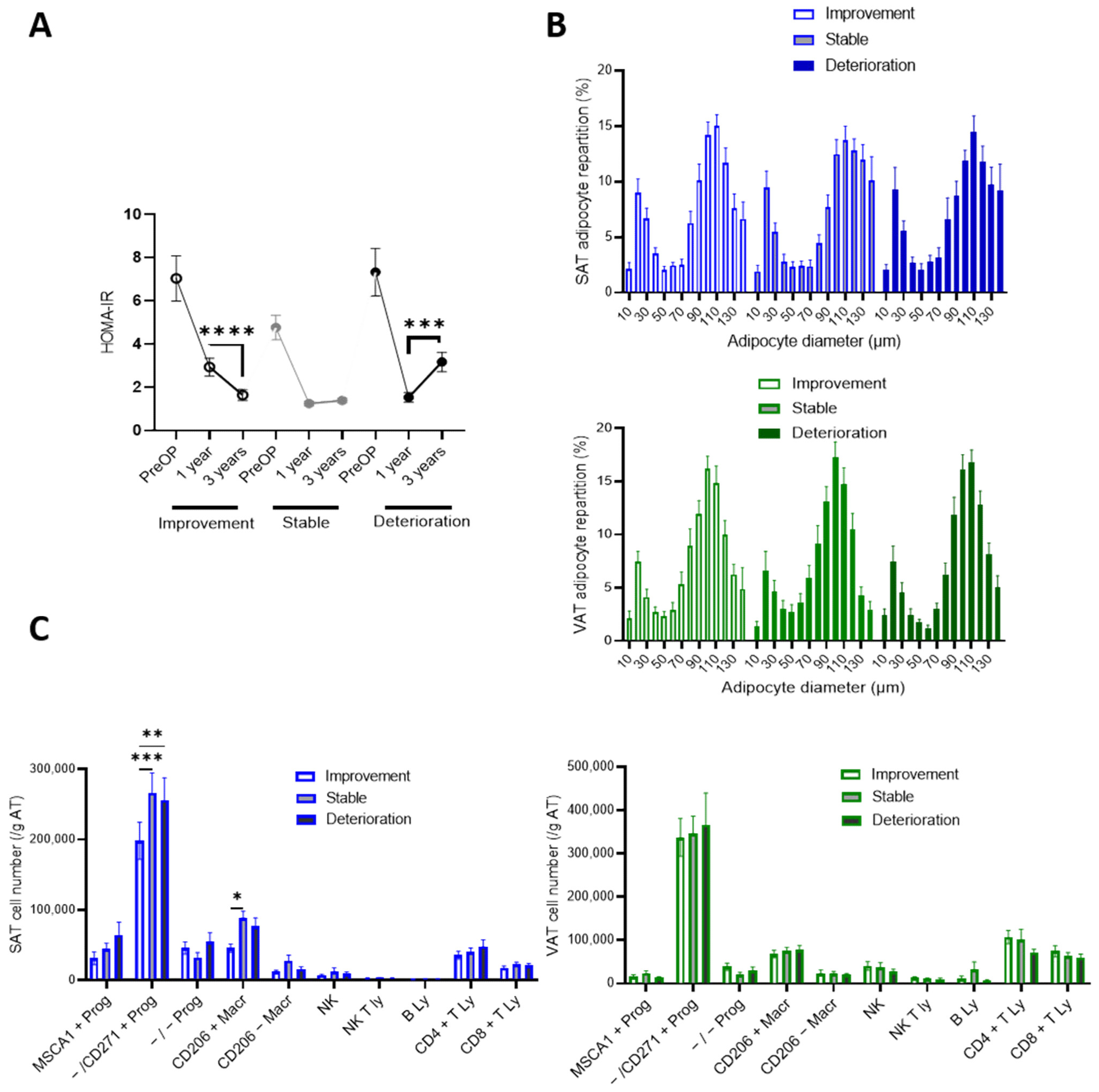
3.5. Cell Phenotypes of Expanded SAT and VAT Associated with Failure to Improve Insulin Resistance at 1 and 3 Years Post-Bariatric Surgery
3.6. Insulin Resistance Trajectories between 1 and 3 Years Post-Bariatric Surgery
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Despres, J.P.; Lemieux, I.; Bergeron, J.; Pibarot, P.; Mathieu, P.; Larose, E.; Rodes-Cabau, J.; Bertrand, O.F.; Poirier, P. Abdominal obesity and the metabolic syndrome: Contribution to global cardiometabolic risk. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 1039–1049. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.D. Role of body fat distribution and the metabolic complications of obesity. J. Clin. Endocrinol. Metab. 2008, 93, S57–S63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vijay, J.; Gauthier, M.F.; Biswell, R.L.; Louiselle, D.A.; Johnston, J.J.; Cheung, W.A.; Belden, B.; Pramatarova, A.; Biertho, L.; Gibson, M.; et al. Single-cell analysis of human adipose tissue identifies depot and disease specific cell types. Nat. Metab. 2020, 2, 97–109. [Google Scholar] [CrossRef] [PubMed]
- Esteve, D.; Boulet, N.; Belles, C.; Zakaroff-Girard, A.; Decaunes, P.; Briot, A.; Veeranagouda, Y.; Didier, M.; Remaury, A.; Guillemot, J.C.; et al. Lobular architecture of human adipose tissue defines the niche and fate of progenitor cells. Nat. Commun. 2019, 10, 2549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vishvanath, L.; Gupta, R.K. Contribution of adipogenesis to healthy adipose tissue expansion in obesity. J. Clin. Investig. 2019, 129, 4022–4031. [Google Scholar] [CrossRef] [Green Version]
- Marcelin, G.; Gautier, E.L.; Clement, K. Adipose Tissue Fibrosis in Obesity: Etiology and Challenges. Annu. Rev. Physiol. 2022, 84, 135–155. [Google Scholar] [CrossRef]
- Arner, P.; Ryden, M. Human white adipose tissue: A highly dynamic metabolic organ. J. Intern. Med. 2022, 291, 611–621. [Google Scholar] [CrossRef]
- Stefan, N. Causes, consequences, and treatment of metabolically unhealthy fat distribution. Lancet Diabetes Endocrinol. 2020, 8, 616–627. [Google Scholar] [CrossRef]
- Brissman, M.; Beamish, A.J.; Olbers, T.; Marcus, C. Prevalence of insufficient weight loss 5 years after Roux-en-Y gastric bypass: Metabolic consequences and prediction estimates: A prospective registry study. BMJ Open 2021, 11, e046407. [Google Scholar] [CrossRef]
- El Ansari, W.; Elhag, W. Weight Regain and Insufficient Weight Loss After Bariatric Surgery: Definitions, Prevalence, Mechanisms, Predictors, Prevention and Management Strategies, and Knowledge Gaps-a Scoping Review. Obes. Surg. 2021, 31, 1755–1766. [Google Scholar] [CrossRef]
- King, W.C.; Hinerman, A.S.; Belle, S.H.; Wahed, A.S.; Courcoulas, A.P. Comparison of the Performance of Common Measures of Weight Regain after Bariatric Surgery for Association with Clinical Outcomes. JAMA 2018, 320, 1560–1569. [Google Scholar] [CrossRef] [Green Version]
- Dicker, D.; Golan, R.; Aron-Wisnewsky, J.; Zucker, J.D.; Sokolowska, N.; Comaneshter, D.S.; Yahalom, R.; Vinker, S.; Clement, K.; Rudich, A. Prediction of Long-Term Diabetes Remission after RYGB, Sleeve Gastrectomy, and Adjustable Gastric Banding Using DiaRem and Advanced-DiaRem Scores. Obes. Surg. 2019, 29, 796–804. [Google Scholar] [CrossRef]
- Keshavjee, S.H.; Schwenger, K.J.P.; Yadav, J.; Jackson, T.D.; Okrainec, A.; Allard, J.P. Factors Affecting Metabolic Outcomes Post Bariatric Surgery: Role of Adipose Tissue. J. Clin. Med. 2021, 10, 714. [Google Scholar] [CrossRef]
- Wood, G.C.; Benotti, P.N.; Lee, C.J.; Mirshahi, T.; Still, C.D.; Gerhard, G.S.; Lent, M.R. Evaluation of the Association Between Preoperative Clinical Factors and Long-term Weight Loss After Roux-en-Y Gastric Bypass. JAMA Surg. 2016, 151, 1056–1062. [Google Scholar] [CrossRef]
- Diedisheim, M.; Poitou, C.; Genser, L.; Amouyal, C.; Bouillot, J.L.; Ciangura, C.; Oppert, J.M.; Clement, K.; Aron-Wisnewsky, J. Weight Loss After Sleeve Gastrectomy: Does Type 2 Diabetes Status Impact Weight and Body Composition Trajectories? Obes. Surg. 2021, 31, 1046–1054. [Google Scholar] [CrossRef]
- Cotillard, A.; Poitou, C.; Torcivia, A.; Bouillot, J.L.; Dietrich, A.; Kloting, N.; Gregoire, C.; Lolmede, K.; Bluher, M.; Clement, K. Adipocyte size threshold matters: Link with risk of type 2 diabetes and improved insulin resistance after gastric bypass. J. Clin. Endocrinol. Metab. 2014, 99, E1466–E1470. [Google Scholar] [CrossRef]
- Goldstein, N.; Kezerle, Y.; Gepner, Y.; Haim, Y.; Pecht, T.; Gazit, R.; Polischuk, V.; Liberty, I.F.; Kirshtein, B.; Shaco-Levy, R.; et al. Higher Mast Cell Accumulation in Human Adipose Tissues Defines Clinically Favorable Obesity Sub-Phenotypes. Cells 2020, 9, 1508. [Google Scholar] [CrossRef]
- Muir, L.A.; Baker, N.A.; Washabaugh, A.R.; Neeley, C.K.; Flesher, C.G.; DelProposto, J.B.; Geletka, L.M.; Ghaferi, A.A.; Finks, J.F.; Singer, K.; et al. Adipocyte hypertrophy-hyperplasia balance contributes to weight loss after bariatric surgery. Adipocyte 2017, 6, 134–140. [Google Scholar] [CrossRef] [Green Version]
- Mechanick, J.I.; Apovian, C.; Brethauer, S.; Timothy Garvey, W.; Joffe, A.M.; Kim, J.; Kushner, R.F.; Lindquist, R.; Pessah-Pollack, R.; Seger, J.; et al. Clinical Practice Guidelines for the Perioperative Nutrition, Metabolic, and Nonsurgical Support of Patients Undergoing Bariatric Procedures-2019 Update: Cosponsored by American Association of Clinical Endocrinologists/American College of Endocrinology, The Obesity Society, American Society for Metabolic and Bariatric Surgery, Obesity Medicine Association, and American Society of Anesthesiologists. Obesity 2020, 28, O1–O58. [Google Scholar] [CrossRef]
- Ledoux, S.; Sami, O.; Calabrese, D.; Le Gall, M.; Flamant, M.; Coupaye, M. Gastric bypass specifically impairs liver parameters as compared with sleeve gastrectomy, independently of evolution of metabolic disorders. Surg. Obes. Relat. Dis. 2019, 15, 220–226. [Google Scholar] [CrossRef]
- Neeland, I.J.; Poirier, P.; Despres, J.P. Cardiovascular and Metabolic Heterogeneity of Obesity: Clinical Challenges and Implications for Management. Circulation 2018, 137, 1391–1406. [Google Scholar] [CrossRef] [PubMed]
- Ye, R.Z.; Richard, G.; Gevry, N.; Tchernof, A.; Carpentier, A.C. Fat Cell Size: Measurement Methods, Pathophysiological Origins, and Relationships With Metabolic Dysregulations. Endocr. Rev. 2022, 43, 35–60. [Google Scholar] [CrossRef] [PubMed]
- Verboven, K.; Wouters, K.; Gaens, K.; Hansen, D.; Bijnen, M.; Wetzels, S.; Stehouwer, C.D.; Goossens, G.H.; Schalkwijk, C.G.; Blaak, E.E.; et al. Abdominal subcutaneous and visceral adipocyte size, lipolysis and inflammation relate to insulin resistance in male obese humans. Sci. Rep. 2018, 8, 4677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Backdahl, J.; Franzen, L.; Massier, L.; Li, Q.; Jalkanen, J.; Gao, H.; Andersson, A.; Bhalla, N.; Thorell, A.; Ryden, M.; et al. Spatial mapping reveals human adipocyte subpopulations with distinct sensitivities to insulin. Cell Metab. 2021, 33, 2301. [Google Scholar] [CrossRef] [PubMed]
- Hagberg, C.E.; Li, Q.; Kutschke, M.; Bhowmick, D.; Kiss, E.; Shabalina, I.G.; Harms, M.J.; Shilkova, O.; Kozina, V.; Nedergaard, J.; et al. Flow Cytometry of Mouse and Human Adipocytes for the Analysis of Browning and Cellular Heterogeneity. Cell Rep. 2018, 24, 2746–2756.e5. [Google Scholar] [CrossRef] [Green Version]
- Sengenes, C.; Lolmede, K.; Zakaroff-Girard, A.; Busse, R.; Bouloumie, A. Preadipocytes in the human subcutaneous adipose tissue display distinct features from the adult mesenchymal and hematopoietic stem cells. J. Cell Physiol. 2005, 205, 114–122. [Google Scholar] [CrossRef]
- Esteve, D.; Boulet, N.; Volat, F.; Zakaroff-Girard, A.; Ledoux, S.; Coupaye, M.; Decaunes, P.; Belles, C.; Gaits-Iacovoni, F.; Iacovoni, J.S.; et al. Human white and brite adipogenesis is supported by MSCA1 and is impaired by immune cells. Stem. Cells 2015, 33, 1277–1291. [Google Scholar] [CrossRef]
- Duffaut, C.; Zakaroff-Girard, A.; Bourlier, V.; Decaunes, P.; Maumus, M.; Chiotasso, P.; Sengenes, C.; Lafontan, M.; Galitzky, J.; Bouloumie, A. Interplay Between Human Adipocytes and T Lymphocytes in Obesity. CCL20 as an Adipochemokine and T Lymphocytes as Lipogenic Modulators. Arterioscler. Thromb. Vasc. Biol. 2009, 29, 1608–1614. [Google Scholar] [CrossRef] [Green Version]
- MacLean, P.S.; Higgins, J.A.; Giles, E.D.; Sherk, V.D.; Jackman, M.R. The role for adipose tissue in weight regain after weight loss. Obes. Rev. 2015, 16 (Suppl. 1), 45–54. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.J.; Wu, Y.; Fried, S.K. Adipose tissue remodeling in pathophysiology of obesity. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 371–376. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pre-Surgery (n = 161) | Mean |
|---|---|
| Age (years) | 41.8 |
| Weight (kg) | 121.1 |
| BMI (kg/m2) | 44.2 |
| HOMA-IR | 5.6 |
| HbA1c (%) | 6 |
| 1 Year Post-surgery (n = 153) | |
| Total weight loss (%) | 31 |
| Excess weight loss (%) | 74.3 |
| HOMA-IR | 1.9 |
| HbA1c (%) | 5.3 |
| 3 Years Post-surgery (n = 78) | |
| Total weight loss (%) | 31.3 |
| Excess weight loss (%) | 76.5 |
| HOMA-IR | 2.1 |
| HbA1c (%) | 5.4 |
| Progenitors | CD45 − /CD34 + /CD31 − |
|---|---|
| Immature | MSCA1 − /CD271 − |
| Adipogenic | MSCA1 + |
| Myofibrogenic | MSCA1 − /CD271 + |
| Immunecells | CD45 + |
| NK cells | CD3 − /CD56 + |
| NKT cells | CD3 + /CD56 + |
| B lymphocytes | CD19 + /CD3 − |
| Helper T lymphocytes | CD19 − /CD3 + /CD4 + |
| Cytotoxic T lymphocytes | CD19 − /CD3 + /CD8 + |
| Resident macrophages | CD14 + /CD206 + |
| Recruited macrophages | CD14 + /CD206 − |
| Characteristic | Without Diabetes (n = 119) | With Diabetes (n = 42) | p Value | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Age (years) | 39.3 | 10.2 | 48.9 | 10.1 | <0.0001 |
| BMI (kg/m2) | 44.3 | 5.8 | 44 | 5.4 | 0.73 |
| HOMA-IR | 4.5 | 2.3 | 8.5 | 5.2 | <0.0001 |
| HbA1c (%) | 5.6 | 0.4 | 7.1 | 1.2 | <0.0001 |
| Characteristic | 3 y EWL Success (n = 65) | 3 y EWL Failure (n = 13) | p Value | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| 3 y EWL (%) | 85 | 25.4 | 35.2 | 12.1 | < 0.0001 |
| Age prior BS (years) | 42 | 10 | 47 | 12 | 0.16 |
| BMI prior BS (Kg/m2) | 43.6 | 5.6 | 46.1 | 5.7 | 0.14 |
| HOMA-IR prior BS | 6 | 4.3 | 7.8 | 5 | 0.17 |
| HbA1c prior Bs (%) | 5.9 | 0.9 | 6.7 | 1.4 | 0.0064 |
| Characteristic | 3 y IR Improvement (n = 49) | 3 y Persistent | p Value | ||
|---|---|---|---|---|---|
| IR (n = 19) | |||||
| Mean | SD | Mean | SD | ||
| 3 y HOMA-IR | 1.3 | 0.5 | 4 | 1.8 | <0.0001 |
| Age prior BS (years) | 42.6 | 10 | 44.2 | 12.4 | 0.65 |
| BMI prior BS (kg/m2) | 44.1 | 5.8 | 44.9 | 5.9 | 0.63 |
| HOMA-IR prior BS | 4.7 | 2.3 | 10.4 | 5.8 | <0.0001 |
| HbA1c prior Bs (%) | 5.8 | 0.6 | 6.6 | 1.2 | 0.0009 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ledoux, S.; Boulet, N.; Belles, C.; Zakaroff-Girard, A.; Bernard, A.; Germain, A.; Decaunes, P.; Briot, A.; Galitzky, J.; Bouloumié, A. Subcutaneous Stromal Cells and Visceral Adipocyte Size Are Determinants of Metabolic Flexibility in Obesity and in Response to Weight Loss Surgery. Cells 2022, 11, 3540. https://doi.org/10.3390/cells11223540
Ledoux S, Boulet N, Belles C, Zakaroff-Girard A, Bernard A, Germain A, Decaunes P, Briot A, Galitzky J, Bouloumié A. Subcutaneous Stromal Cells and Visceral Adipocyte Size Are Determinants of Metabolic Flexibility in Obesity and in Response to Weight Loss Surgery. Cells. 2022; 11(22):3540. https://doi.org/10.3390/cells11223540
Chicago/Turabian StyleLedoux, Séverine, Nathalie Boulet, Chloé Belles, Alexia Zakaroff-Girard, Arnaud Bernard, Albéric Germain, Pauline Decaunes, Anaïs Briot, Jean Galitzky, and Anne Bouloumié. 2022. "Subcutaneous Stromal Cells and Visceral Adipocyte Size Are Determinants of Metabolic Flexibility in Obesity and in Response to Weight Loss Surgery" Cells 11, no. 22: 3540. https://doi.org/10.3390/cells11223540