Effectiveness of Virtual Reality-Based Interventions for Children and Adolescents with ADHD: A Systematic Review and Meta-Analysis

 ,
,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection of Studies
2.3. Data Extraction and Analysis
2.4. Summary Measures
2.5. Synthesis of Results (Statistical Analysis Plan)
2.6. Assessment of Risk of Bias in Individual Studies
2.7. Assessment of the Degree of Evidence of the Set of Studies
2.7.1. Risk of Bias of the Set of Studies
2.7.2. Heterogeneity
2.7.3. Indirect Evidence
2.7.4. Imprecision
2.7.5. Publication Bias
3. Results
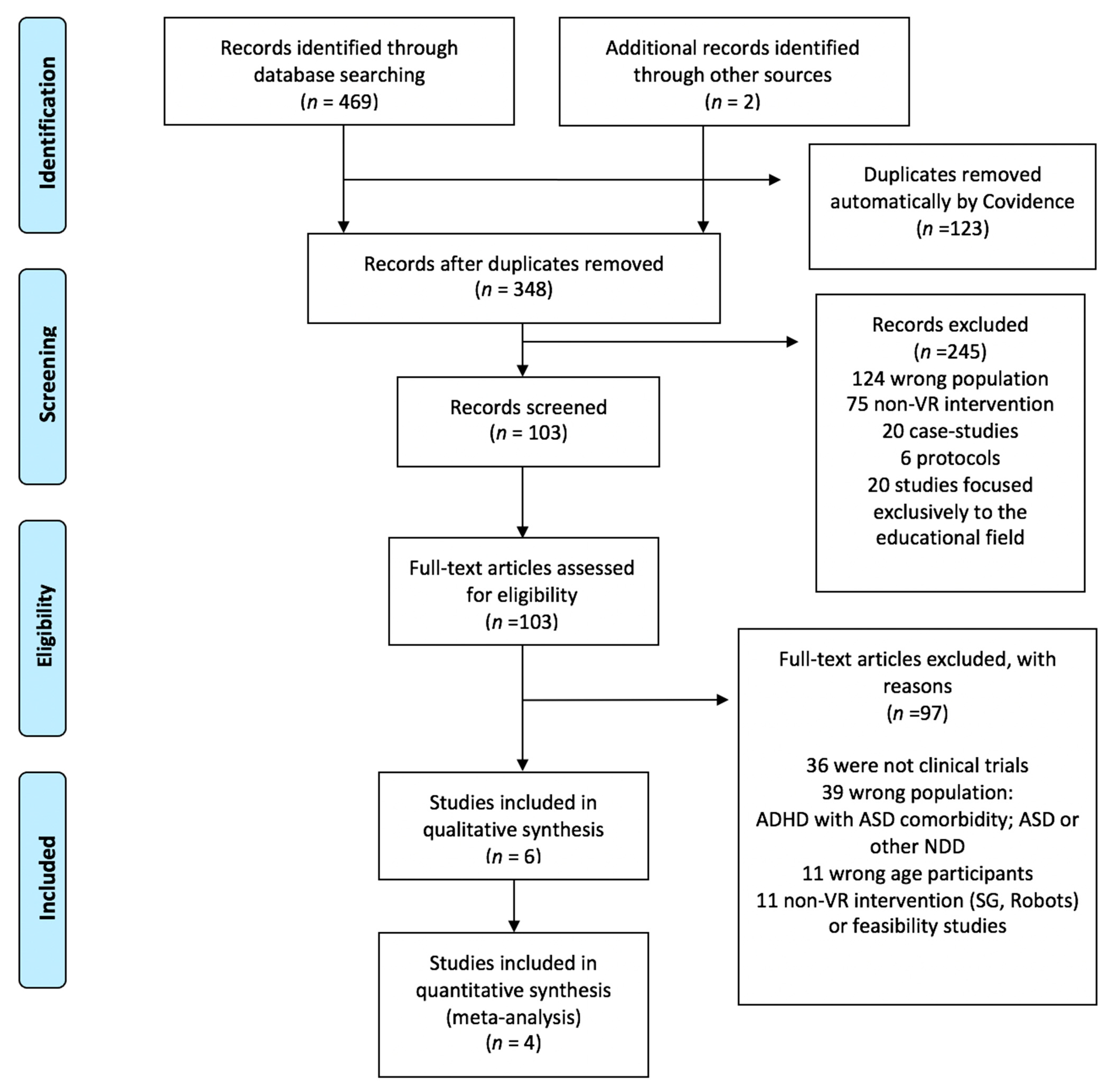
3.1. Study Selection and Characteristics
3.2. Characteristics of the Studies Included in the Meta-Analysis
3.3. Interventions
3.4. Effect of the VR-Based Interventions on the Different Factors of Sustained Attention and Impulsivity in Children with ADHD
3.5. Degree of Evidence from the Set of Studies
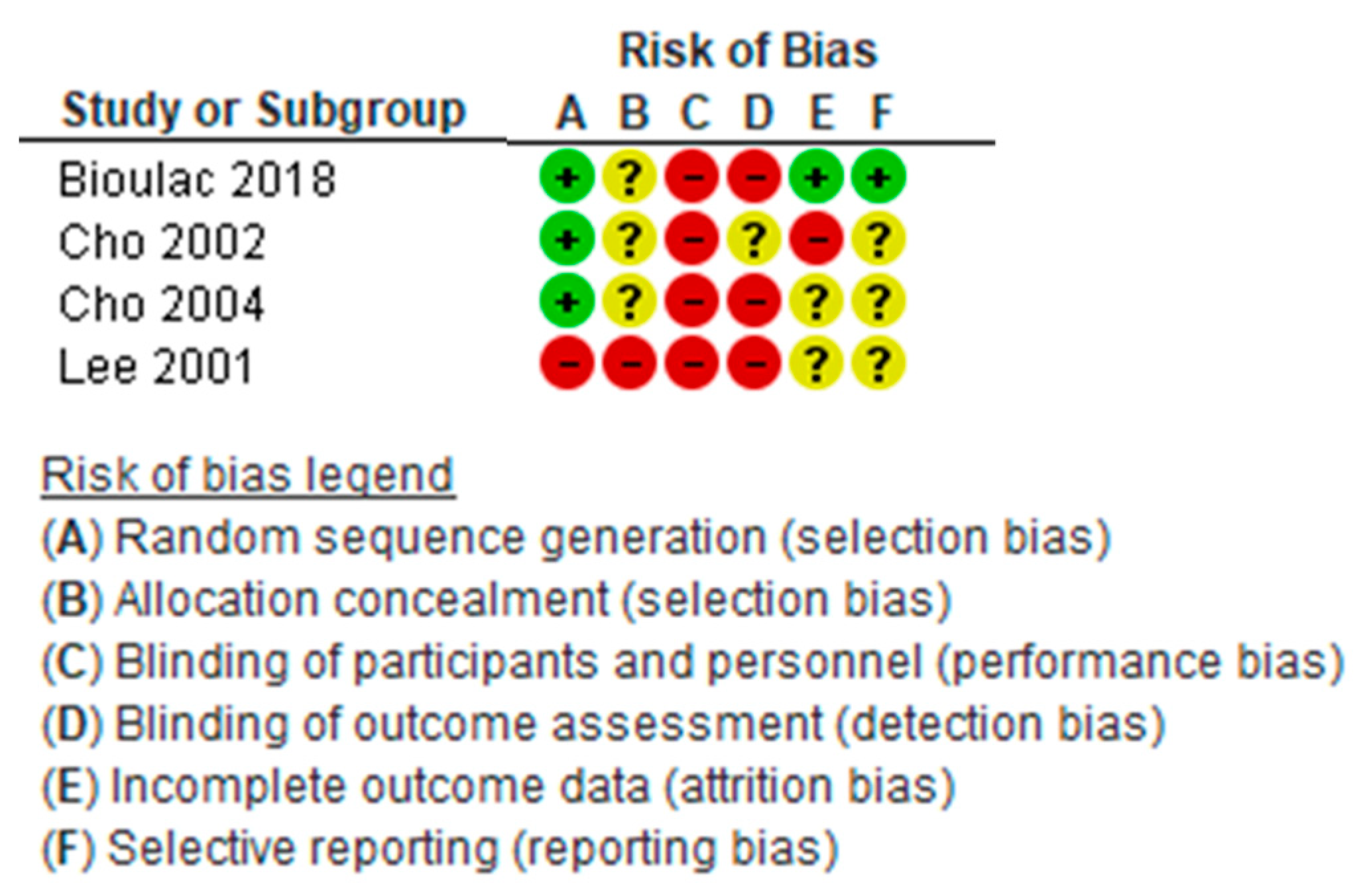
3.5.1. Risk of Bias of Individual Studies
3.5.2. Heterogeneity
3.5.3. Indirect Evidence
3.5.4. Imprecision
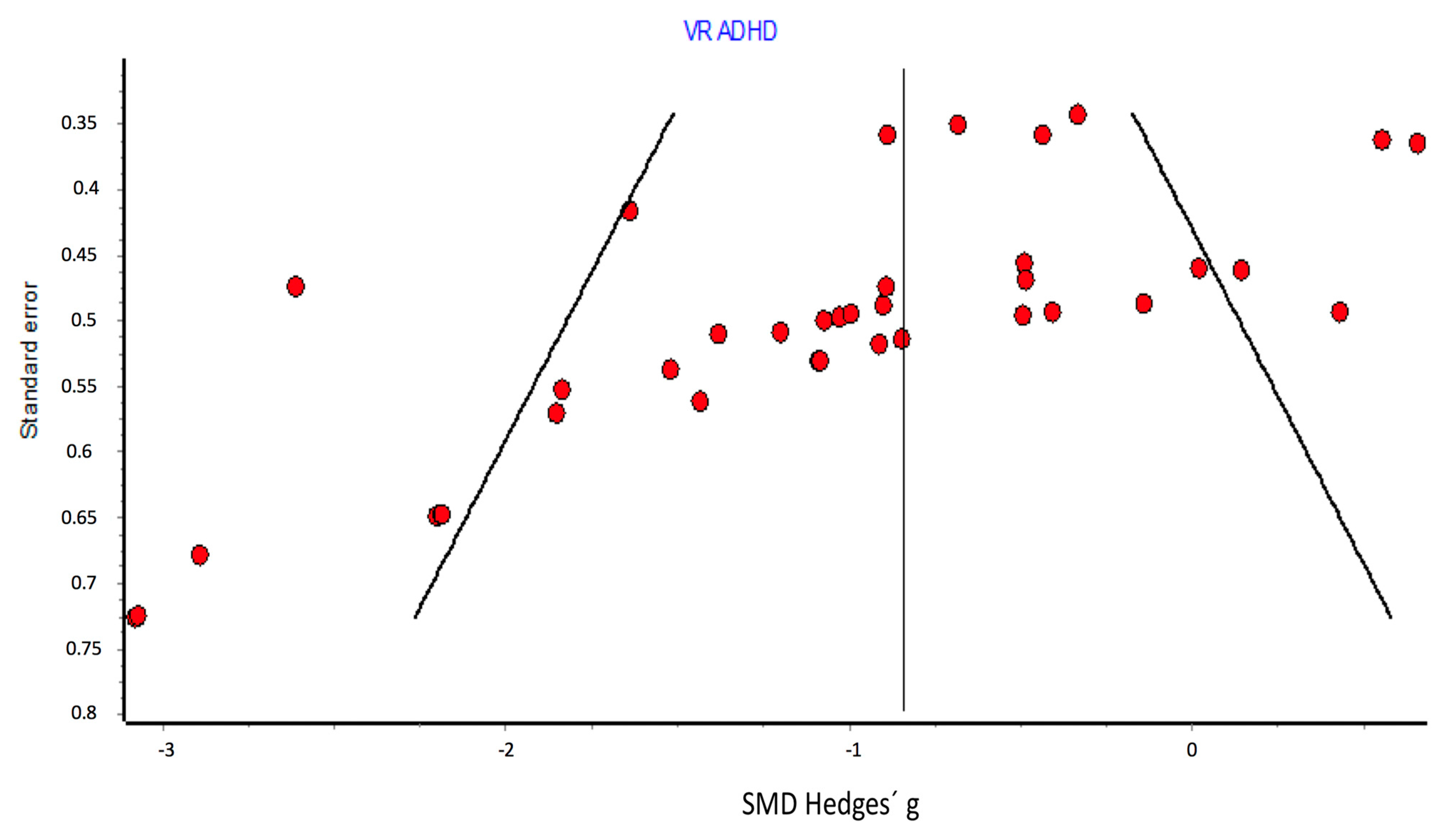
3.5.5. Publication Bias
4. Discussion
4.1. Effect of VR-Based Interventions on Each Type of Outcome (Omissions, Commissions, Correct Hits, Reaction Time, Perceptual Sensitivity)
4.2. GRADE Quality of Evidence
4.2.1. Assessment of Risk of Bias in the Individual Studies
4.2.2. Assessment of Heterogeneity
4.2.3. Assessment of Indirect Measurement
4.2.4. Assessment of Imprecision
4.2.5. Assessment of Publication Bias
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alqithami, S.; Alzahrani, M.; Alzahrani, A.; Mustafa, A. AR-Therapist: Design and Simulation of an AR-Game Environment as a CBT for Patients with ADHD. Healthcare 2019, 7, 146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- APA. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013; p. 947. [Google Scholar]
- Barkley, R.A. Behavioral inhibition, sustained attention, and executive functions: Constructing a unifying theory of ADHD. Psychol. Bull. 1997, 121, 65–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Areces, D.; Dockrell, J.; García, T.; González-Castro, P.; Rodríguez, C. Analysis of cognitive and attentional profiles in children with and without ADHD using an innovative virtual reality tool. PLoS ONE 2018, 13, e0201039. [Google Scholar] [CrossRef] [PubMed]
- Keshav, N.U.; Vogt-Lowell, K.; Vahabzadeh, A.; Sahin, N.T. Digital Attention-Related Augmented-Reality Game: Significant Correlation between Student Game Performance and Validated Clinical Measures of Attention-Deficit/Hyperactivity Disorder (ADHD). Children 2019, 6, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kokol, P.; Vošner, H.B.; Završnik, J.; Vermeulen, J.; Shohieb, S.; Peinemann, F. Serious Game-based Intervention for Children with Developmental Disabilities. Curr. Pediatr. Rev. 2020, 16, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Hall, J.; Kellett, S.; Berrios, R.; Bains, M.K.; Scott, S. Efficacy of Cognitive Behavioral Therapy for Generalized Anxiety Disorder in Older Adults: Systematic Review, Meta-Analysis, and Meta-Regression. Am. J. Geriatr. Psychiatry 2016, 24, 1063–1073. [Google Scholar] [CrossRef] [Green Version]
- Cochrane. Cochrane Handbook for Systematic Reviews of Interventions. Available online: https://handbook-5-1.cochrane.org/2020 (accessed on 8 December 2020).
- Guyatt, G.H.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; Debeer, H. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- Shamseer, L.; Sampson, M.; Bukutu, C.; Schmid, C.H.; Nikles, J.; Tate, R.; Johnston, B.C.; Zucker, D.; Shadish, W.R.; Kravitz, R.; et al. CONSORT extension for reporting N-of-1 trials (CENT) 2015: Explanation and elaboration. BMJ 2015, 350, h1793. [Google Scholar] [CrossRef] [Green Version]
- Valentine, A.Z.; Brown, B.J.; Groom, M.J.; Young, E.; Hollis, C.; Hall, C.L. A systematic review evaluating the implementation of technologies to assess, monitor and treat neurodevelopmental disorders: A map of the current evidence. Clin. Psychol. Rev. 2020, 80, 101870. [Google Scholar] [CrossRef]
- Baron, I.S. Neuropsychological Evaluation of the Child; Oxford University Press: Oxford, UK, 2004. [Google Scholar]
- Rizzo, A.A.; Bowerly, T.; Buckwalter, J.G.; Klimchuk, D.; Mitura, R.; Parsons, T.D. A Virtual Reality Scenario for All Seasons: The Virtual Classroom. CNS Spectr. 2006, 11, 35–44. [Google Scholar] [CrossRef] [Green Version]
- Shiroma, E.J.; Ferguson, P.L.; Pickelsimer, E.E. Prevalence of Traumatic Brain Injury in an Offender Population: A Meta-Analysis. J Head Trauma Rehabil. 2012, 27, E1–E10. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Rind, D.; Devereaux, P.J.; Montori, V.M.; Freyschuss, B.; Vist, G.; et al. GRADE guidelines 6. Rating the quality of evidence—Imprecision. J. Clin. Epidemiol. 2011, 64, 1283–1293. [Google Scholar] [CrossRef] [PubMed]
- MetaXL. Available online: https://www.epigear.com/index_files/metaxl.html (accessed on 8 December 2020).
- Furuya-Kanamori, L.; Barendregt, J.J.; Doi, S.A. A new improved graphical and quantitative method for detecting bias in meta-analysis. Int. J. Evid. Based Healthc. 2018, 16, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Begg, C.B.; Mazumdar, M. Operating Characteristics of a Rank Correlation Test for Publication Bias. Biometrics 1994, 50, 1088. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Manshaee, G.; Tabrizi, M.; Ghamarani, A.; Rasti, J. Comparison of the effectiveness of virtual reality with medication on the memory of attention deficit hyperactivity disorder students. Int. Arch. Heal. Sci. 2020, 7, 37–42. [Google Scholar] [CrossRef]
- Bul, K.; Kato, P.M.; Van Der Oord, S.; Danckaerts, M.; Vreeke, L.J.; Willems, A.; Van Oers, H.J.; Heuvel, R.V.D.; Birnie, D.; Amelsvoort, T.A.M.J.V.; et al. Behavioral Outcome Effects of Serious Gaming as an Adjunct to Treatment for Children With Attention-Deficit/Hyperactivity Disorder: A Randomized Controlled Trial. J. Med. Internet. Res. 2016, 18, e26. [Google Scholar] [CrossRef]
- Cho, B.H.; Kim, S.; Shin, D.I.; Lee, J.H.; Min Lee, S.; Young Kim, I.; Kim, S.I. Neurofeedback training with virtual reality for inattention and impulsiveness. Cyberpsychol. Behav. 2004, 7, 519–526. [Google Scholar] [CrossRef]
- Bioulac, S.; Micoulaud-Franchi, J.-A.; Maire, J.; Bouvard, M.P.; Rizzo, A.A.; Sagaspe, P.; Philip, P. Virtual Remediation Versus Methylphenidate to Improve Distractibility in Children With ADHD: A Controlled Randomized Clinical Trial Study. J. Atten. Disord. 2020, 24, 326–335. [Google Scholar] [CrossRef] [Green Version]
- Cho, B.H.; Ku, J.; Jang, D.P.; Kim, S.; Lee, Y.H.; Kim, I.Y.; Lee, J.H.; I Kim, S. The Effect of Virtual Reality Cognitive Training for Attention Enhancement. CyberPsychol. Behav. 2002, 5, 129–137. [Google Scholar] [CrossRef]
- Lee, J.M.; Cho, B.H.; Ku, J.H.; Kim, J.S.; Lee, J.H.; Kim, I.Y.; Kim, S.I. A study on the system for treatment of ADHD using virtual reality. In Proceedings of the 23rd Annual EMBS International Conference, Istanbul, Turkey, 25–28 October 2001. [Google Scholar]
- Ioannidis, J. The Mass Production of Redundant, Misleading, and Conflicted Systematic Reviews and Meta-analyses. Milbank Q. 2016, 94, 485–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parsons, T.; Bowerly, T.; Buckwalter, J.G.; Rizzo, A.A. A Controlled Clinical Comparison of Attention Performance in Children with ADHD in a Virtual Reality Classroom Compared to Standard Neuropsychological Methods. Child Neuropsychol. 2007, 13, 363–381. [Google Scholar] [CrossRef] [PubMed]
- Coleman, B.; Marion, S.; Rizzo, A.; Turnbull, J.; Nolty, A. Virtual Reality Assessment of Classroom—Related Attention: An Ecologically Relevant Approach to Evaluating the Effectiveness of Working Memory Training. Front. Psychol. 2019, 10, 1851. [Google Scholar] [CrossRef] [Green Version]
- Pollak, Y.; Weiss, P.L.; Rizzo, A.A.; Weizer, M.; Shriki, L.; Shalev, R.S.; Gross-Tsur, V. The Utility of a Continuous Performance Test Embedded in Virtual Reality in Measuring ADHD-Related Deficits. J. Dev. Behav. Pediatr. 2009, 30, 2–6. [Google Scholar] [CrossRef] [PubMed]
- Mesa-Gresa, P.; Gil-Gómez, H.; Lozano, J.A.; Gil-Gómez, J.-A. Effectiveness of Virtual Reality for Children and Adolescents with Autism Spectrum Disorder: An Evidence-Based Systematic Review. Sensors 2018, 18, 2486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fabiano, G.A.; Schatz, N.K.; Aloe, A.M.; Chacko, A.; Chronis-Tuscano, A. A Systematic Review of Meta-Analyses of Psychosocial Treatment for Attention-Deficit/Hyperactivity Disorder. Clin. Child Fam. Psychol. Rev. 2015, 18, 77–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayuso, D.M.R. Activities of daily living. An. Psicol. 2007, 23, 264–271. [Google Scholar]
- Romero-Ayuso, D.; Castillero-Perea, Á.; González, P.; Navarro, E.; Molina-Massó, J.P.; Funes, M.J.; Ariza-Vega, P.; Toledano-González, A.; Triviño-Juárez, J.M. Assessment of cognitive instrumental activities of daily living: A systematic review. Disabil. Rehabil. 2019, 2019, 1–17. [Google Scholar] [CrossRef]
- Riva, G.; Mancuso, V.; Cavedoni, S.; Stramba-Badiale, C. Virtual reality in neurorehabilitation: A review of its effects on multiple cognitive domains. Expert Rev. Med. Devices 2020, 17, 1035–1061. [Google Scholar] [CrossRef]
- Bikic, A.; Reichow, B.; McCauley, S.A.; Ibrahim, K.; Sukhodolsky, D.G. Meta-analysis of organizational skills interventions for children and adolescents with Attention-Deficit/Hyperactivity Disorder. Clin. Psychol. Rev. 2017, 52, 108–123. [Google Scholar] [CrossRef]
- Pfiffner, L.J.; Hinshaw, S.P.; Owens, E.; Zalecki, C.; Kaiser, N.M.; Villodas, M.; McBurnett, K. A two-site randomized clinical trial of integrated psychosocial treatment for ADHD-inattentive type. J. Consult. Clin. Psychol. 2014, 82, 1115–1127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navarro, E.; González, P.; López-Jaquero, V.; Montero, F.; Molina, J.P.; Romero-Ayuso, D. Adaptive, Multisensorial, Physiological and Social: The Next Generation of Telerehabilitation Systems. Front. Aging Neurosci. 2018, 12, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Key Seach Terms | |
|---|---|
| Population | (ADHD OR attention deficit OR hyperactivity disorder) AND children |
| Intervention | virtual reality OR virtual environment OR virtual rehabilitation OR augmented reality OR serious games |
| Comparation | neurorehabilitation OR cognitive training OR cognitive therapy OR neuropsychological rehabilitation OR neuropsychological training OR neuropsychological therapy OR attention training |
| Outcome | cognition OR attention OR sustained attention OR impulsivity OR cognitive impulsivity OR executive function |
| Authors and Year | Title | Measures | Intervention: Experimental Group | Intervention: Comparison Group | Outcome/Results |
|---|---|---|---|---|---|
| Bioulac, S., Micoulad-Franchi, J.A., Maire, J., Bouvard, M.P., Rizzo, A.A., Sagaspe, P. & Philip, P. 2020 [23] | Virtual Remediation versus methylphenidate to improve distractibility in children with ADHD: A controlled randomized clinical trial study | ADHD-RS Symptom Inventory according to DSM-IV Continuous Performance Test (CPT) Virtual AULA (HMD) | The experimental group received VR-based intervention. No. of participants = 16 children with ADHD, between 7 and 11 years old, with Diagnosis according to DSM-IV; with an IQ > 85 and a Score > 28 on the ADHD-RS. No. of sessions = 12 Duration of sessions = 30 min, Frequency of sessions = 2 times a week Intervention period = 6 weeks Children were asked to detect letters while inhibiting various distractors (e.g., falling pencils, footsteps, intercom announcements, etc.) | Group with long-acting methylphenidate (QUASYM) No. of participants = 16 A clinical interview was conducted every two weeks for 8 weeks. The maximum dosage was 1 mg/Kg. Group with placebo psychotherapy training No. of participants = 16 Duration of sessions = 30 min Intervention period = 6–8 weeks, No. of sessions = 12 The intervention focused on attention, support and psychoeducation. | The children who received the VR-based intervention obtained higher performance in the tasks and tests of sustained attention both in the CPT and in the virtual AULA tests. After intervention, there were no differences in the number of omissions in the CPT between the VR-based intervention group and methylphenidate group (p = 0.03). There were differences due to commission errors between these two groups, being lower in VR-based intervention group (p = 0.001); The number of hits in the virtual classroom cognitive remediation group was significantly higher than in the psychotherapy group (p < 0.001). There were no differences in the number of commissions between the groups with psychotherapy and pharmacological treatment. In the CPT task, there were significant differences in the number of commissions between the virtual classroom cognitive rehabilitation group and the methylphenidate group (p = 0.05). No child in the VR-based intervention group reported adverse effects, such as cybersickness. |
| Cho, et al., 2002 [24] | The Effect of Virtual Reality Cognitive Training for Attention Enhancement | Continuous Performance Test (CPT) | VR-based intervention group (HMD) No. of participants = 9 No. of sessions = 8 Duration of sessions = 20 min Intervention period = 2 weeks Treatment focuses on tasks of sustained, selective, divided or alternating attention, with different tasks where they have to stop an activity at a signal, as a flag, comparing objects and observe similarities, etc. | Group Non-VR No. of participants = 9 Cognitive rehabilitation similar to VR but using a computer Control group No. of participants = 9 They received no intervention | Perceptual sensitivity decreased in all groups, being higher and significant in the VR-based intervention group (p < 0.01). Only the response bias decreased in the VR-based intervention group (p < 0.01). Correct hits on the CPT was higher in the VR-based intervention group, although the differences were not statistically significant. |
| Cho et al., 2004 [22] | Neurofeedback training with VR for inattention and impulsiveness | Continuous Performance Test CPT | VR-based intervention group (HMD) VE was a classroom No. of participants = 10 No. of sessions = 8 Duration of sessions = 20 min Intervention period = 2 weeks | Non-VR Group = 9 Cognitive rehabilitation similar to VR but using a computer. Control Group = 9 They received no intervention. | The VR-based intervention group improved the number of correct responses after the intervention (p < 0.001), decreased its reaction time (p < 0.001), the perceptual sensitivity (p < 0.01) and commissions (p < 0.05) after the intervention. Response bias increased in all groups (p < 0.001). The group that improved the most in the impulsivity parameters was the VR-based intervention one. |
| Lee et al., 2001 [25] | A study on the system for treatment of ADHD using virtual reality | Continuous Performance Test (CPT) | VR-based intervention group HDM and tracking system with three EEG electrodes (Cz, grounded in the right and left ears). The EEG signal acquisition frequency was 256 Hz. They extracted the frequency parameters Delta (0.5–3 Hz), Theta (4–7 Hz), Alpha (8–12 Hz), SMR (12–15 Hz) and Beta (15–18 Hz). The data was updated every 0.5 s. No. of participants = 10 No. of sessions = 10 Duration of each session = 10 min Intervention period = 2 weeks When the child’s Beta threshold value increased (15–18 Hz), there was a small change in the virtual environment. The virtual task was centered on dinosaurs, where information about them was presented and then the child was asked to answer a series of questions about the information presented. | Control Group No. of participants = 10 They received no intervention | The VR-based intervention group showed a reduction of omissions and commissions versus the control group. The perceptual sensitivity decreased after VR-based intervention |
| Global Effect | ||||||||
|---|---|---|---|---|---|---|---|---|
| No. Studies (Comparisons) | Risk of Bias | Inconsistency Heterogeneity | Indirect Evidence | Imprecision | Publication Bias | SMD (CI 95%) | Quality of Evidence | |
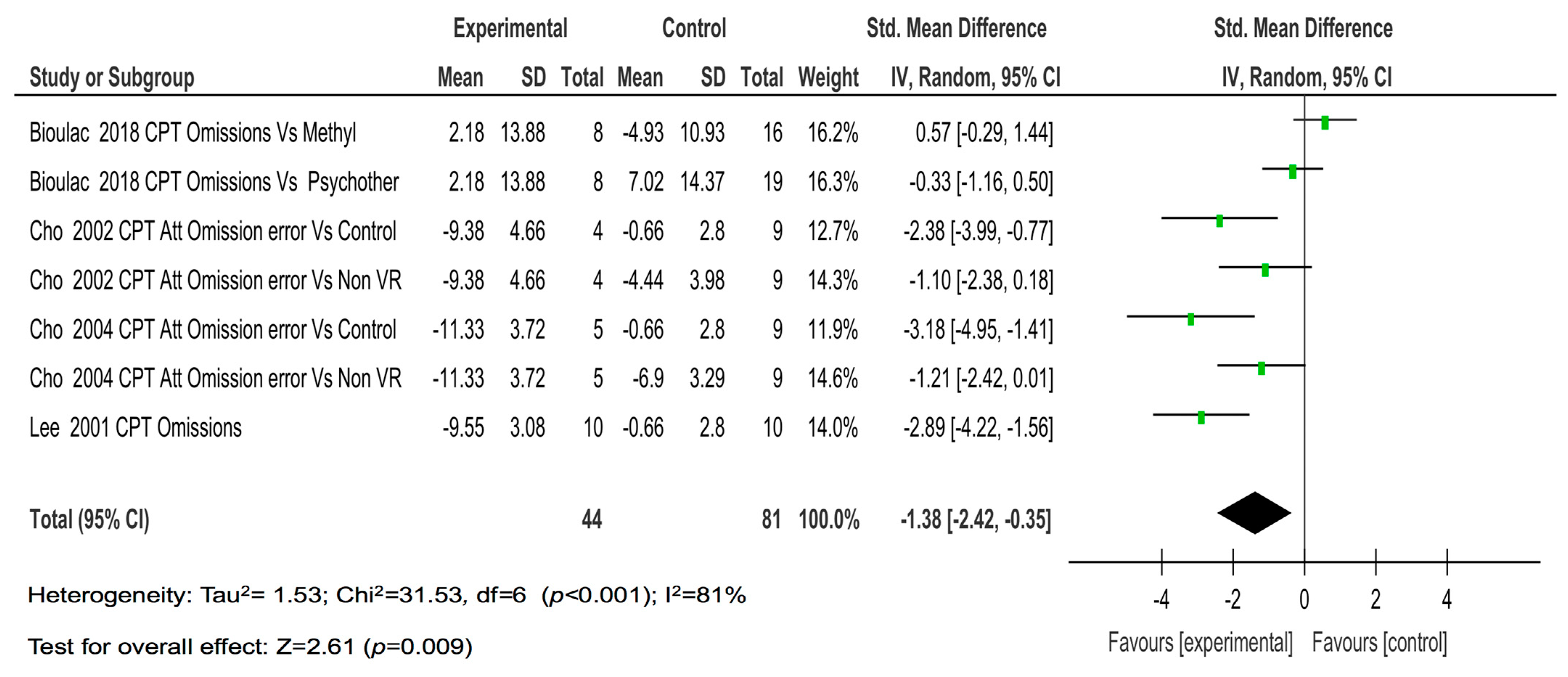
| Omissions | 4 (7) | High (−1) | High (−1) | No (-) | No (-) | Low (-) | −1.38 (−2.2, −0.35) | Low |
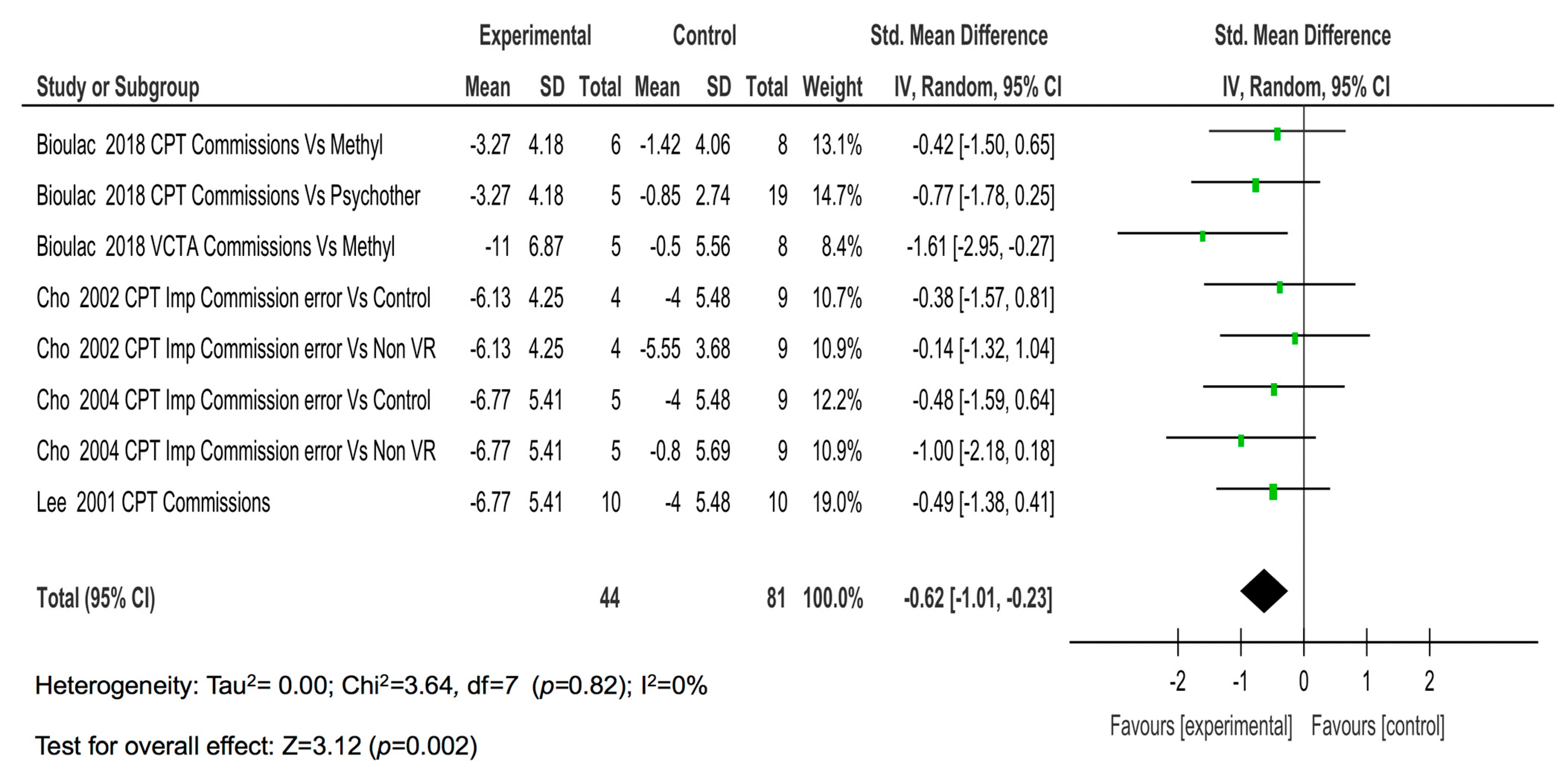
| Commissions | 4 (8) | High (−1) | Null | No (-) | No (-) | Low (-) | −0.62 (−1.01, −0.23) | Moderate |
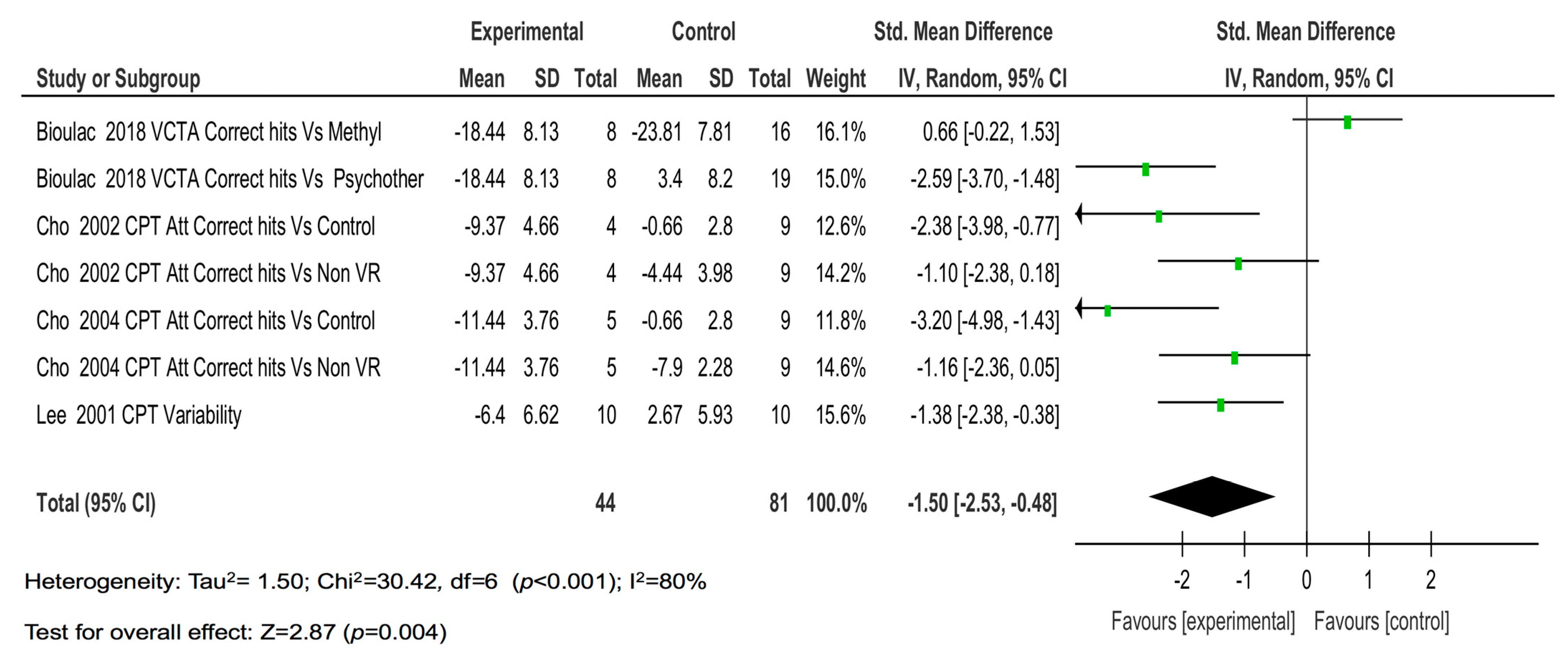
| Correct hits | 4 (7) | High (−1) | High (−1) | No (-) | No (-) | Low (-) | −1.50 (−2.53, −0.38) | Low |
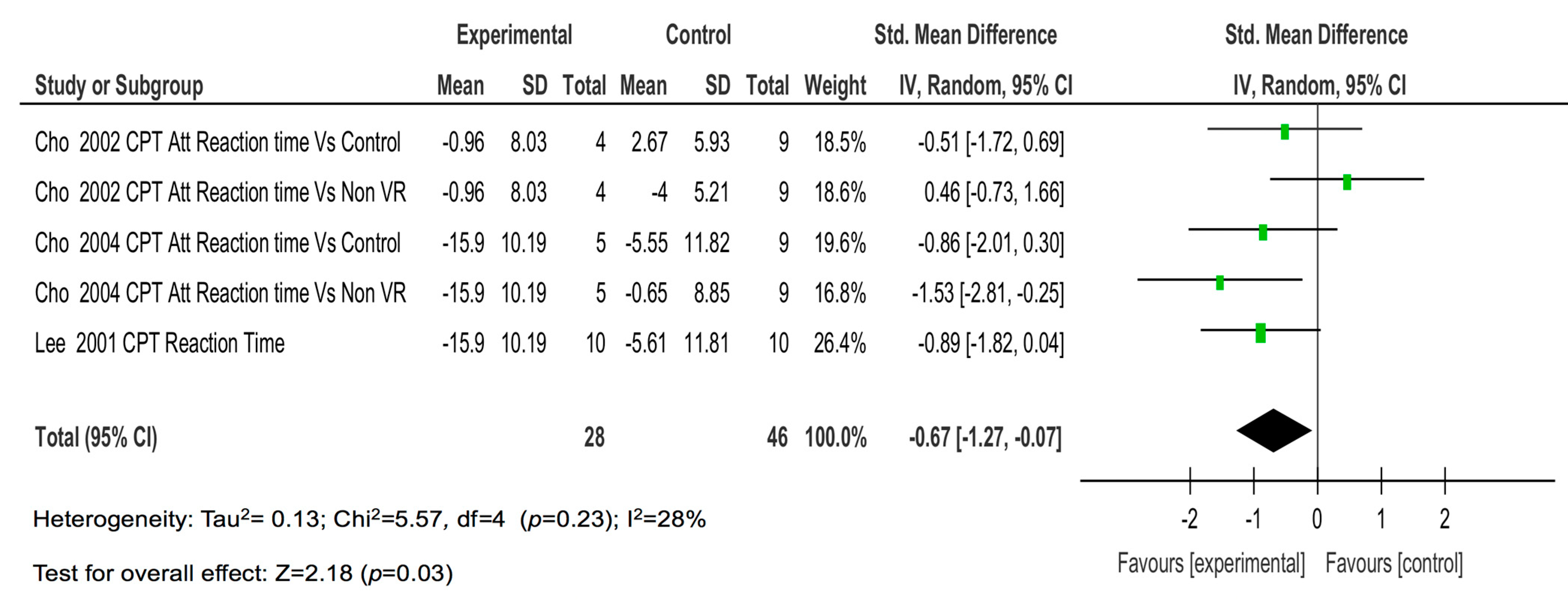
| Reaction time | 4 (5) | High (−1) | Low | No (-) | No (-) | Low (-) | −0.67 (−1.27, −0.07) | Moderate |
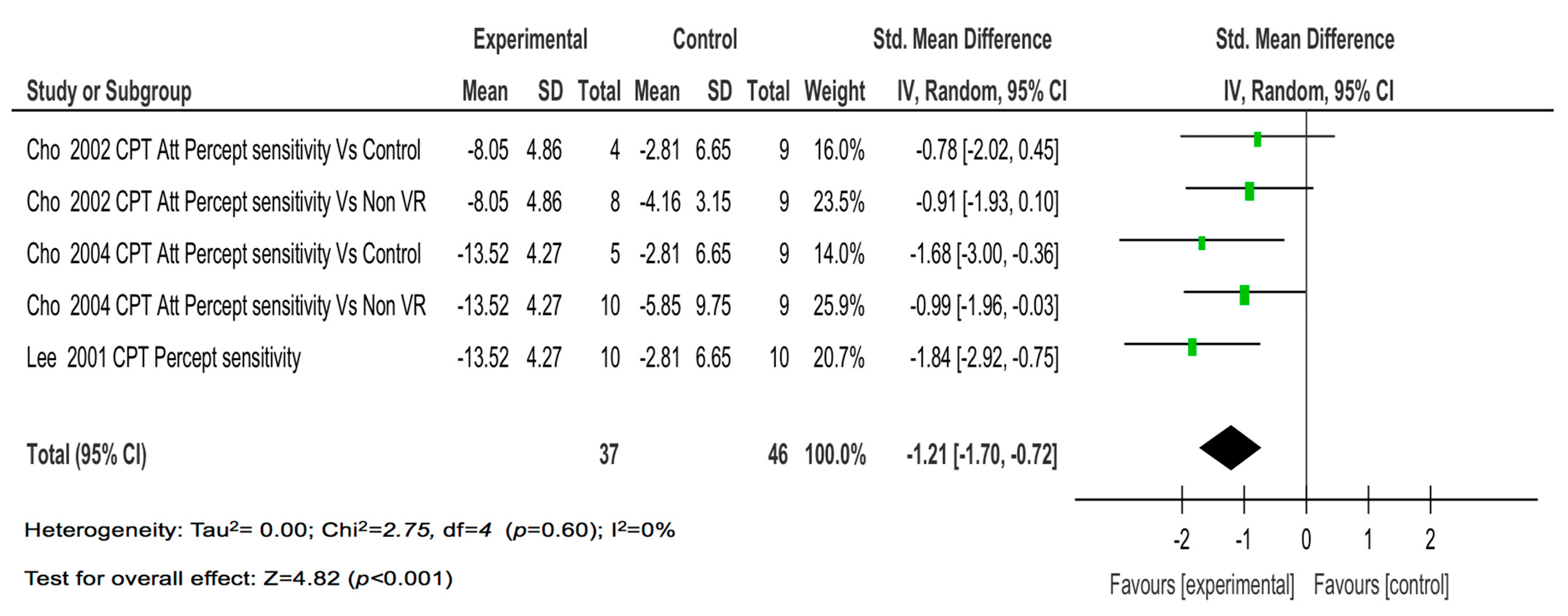
| Perceptual sensitivity | 4 (5) | High (−1) | Moderate | No (-) | No (-) | Low (-) | −1.07 (−1.92, −0.22) | Moderate |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romero-Ayuso, D.; Toledano-González, A.; Rodríguez-Martínez, M.d.C.; Arroyo-Castillo, P.; Triviño-Juárez, J.M.; González, P.; Ariza-Vega, P.; Del Pino González, A.; Segura-Fragoso, A. Effectiveness of Virtual Reality-Based Interventions for Children and Adolescents with ADHD: A Systematic Review and Meta-Analysis. Children 2021, 8, 70. https://doi.org/10.3390/children8020070
Romero-Ayuso D, Toledano-González A, Rodríguez-Martínez MdC, Arroyo-Castillo P, Triviño-Juárez JM, González P, Ariza-Vega P, Del Pino González A, Segura-Fragoso A. Effectiveness of Virtual Reality-Based Interventions for Children and Adolescents with ADHD: A Systematic Review and Meta-Analysis. Children. 2021; 8(2):70. https://doi.org/10.3390/children8020070
Chicago/Turabian StyleRomero-Ayuso, Dulce, Abel Toledano-González, María del Carmen Rodríguez-Martínez, Palma Arroyo-Castillo, José Matías Triviño-Juárez, Pascual González, Patrocinio Ariza-Vega, Antonio Del Pino González, and Antonio Segura-Fragoso. 2021. "Effectiveness of Virtual Reality-Based Interventions for Children and Adolescents with ADHD: A Systematic Review and Meta-Analysis" Children 8, no. 2: 70. https://doi.org/10.3390/children8020070