
Lung Ultrasound, Clinical and Analytic Scoring Systems as Prognostic Tools in SARS-CoV-2 Pneumonia: A Validating Cohort

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Selection of Participants
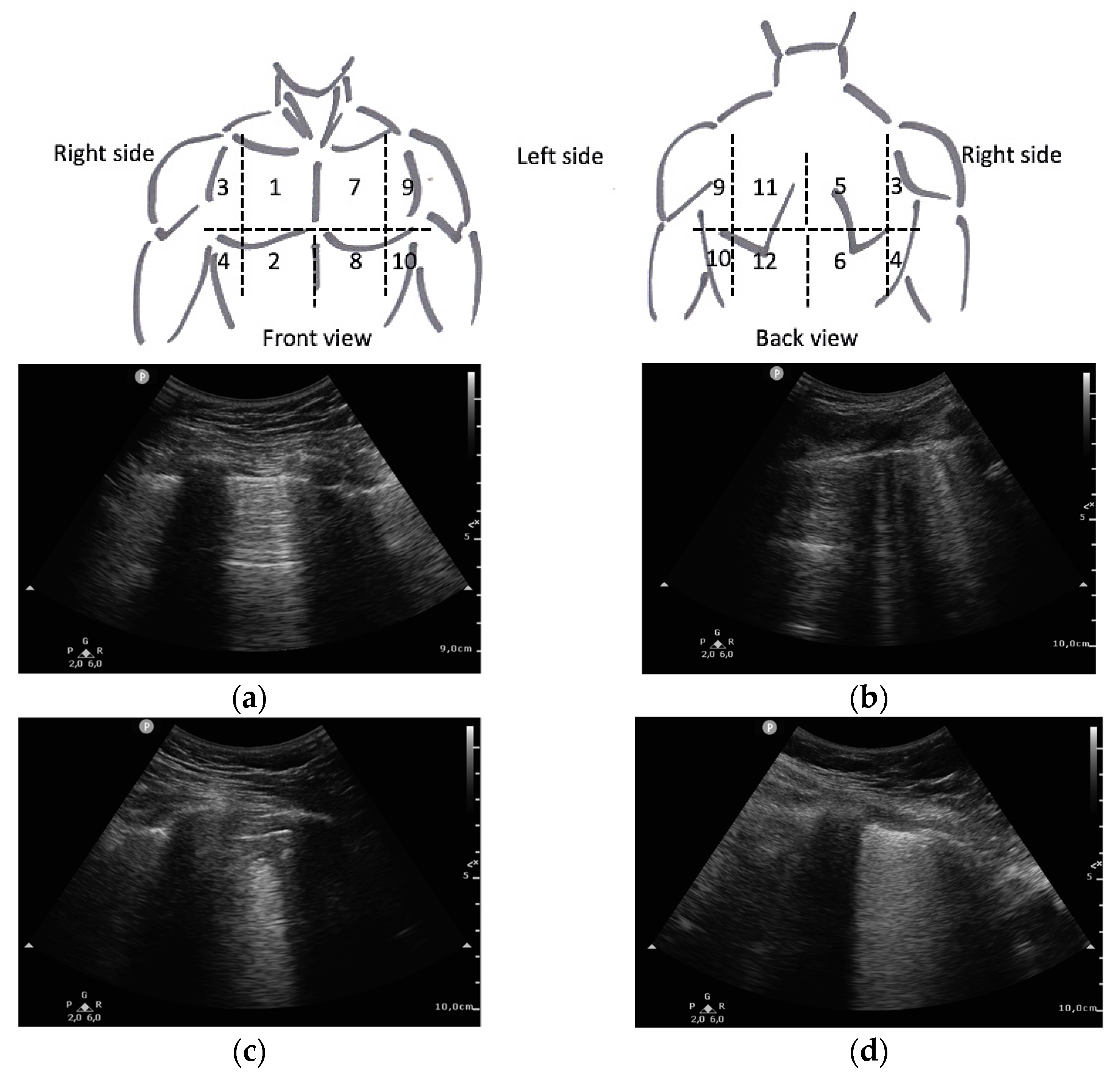
2.3. Measurements
2.4. Outcomes
2.5. Scores Selection
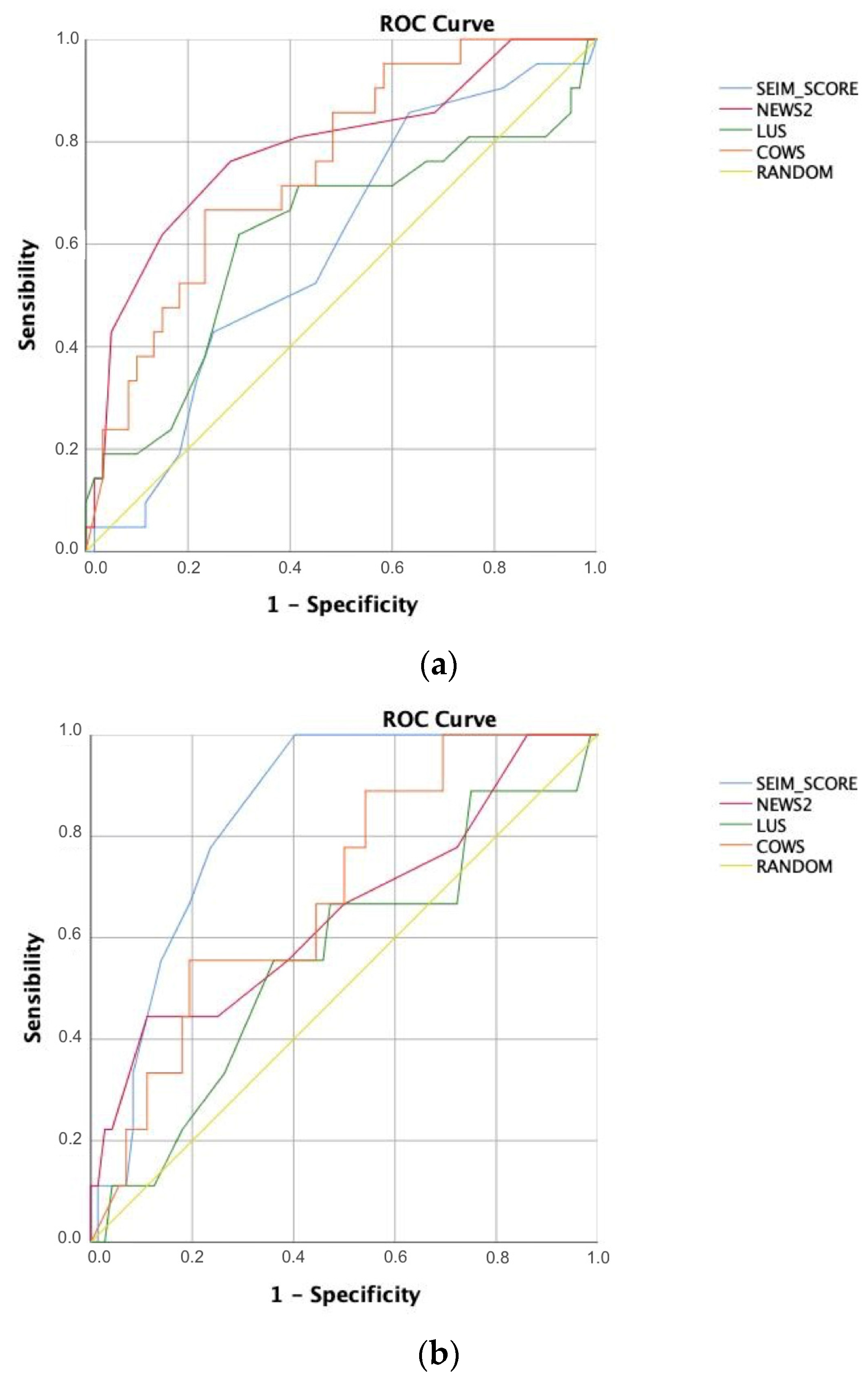
2.6. Analysis
3. Results
3.1. Characteristics of Study Subjects
3.2. Main Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 81) | Poor Outcome (n = 21) | Favourable Outcome (n = 60) | p-Value | Dead 28 Days (n = 9) | Alive 28 Days (n = 72) | p-Value | |
|---|---|---|---|---|---|---|---|
| Age | 62 | 61 | 62 | 0.550 | 73 | 59 | 0.001 ** |
| (median, IQR) | (52–72) | (47.5–72.3) | (52.8–71.3) | (72–78) | (51–70) | ||
| Sex | |||||||
| Male (%) | 66.7 | 75 | 63.9 | 0.362 | 55.6 | 68.1 | |
| Female (%) | 33.3 | 25 | 36.1 | 44.4 | 31.9 | 0.292 | |
| Weight [kg] | 84 | 84 | 84 | 0.852 | 83.9 | 84 | 0.733 |
| (mean, SD) | (1.9) | (3.3) | (2.3) | (7.3) | (1.9) | ||
| Height [cm] | 168.7 | 168 | 168.9 | 0.653 | 165 | 169 | 0.868 |
| (mean, SD) | (1.1) | (2.1) | (1.3) | (3.7) | (1.2) | ||
| Dementia (%) | 2.5 | 0 | 3.3 | 0.412 | 0 | 2.7 | 0.635 |
| COPD 1 (%) | 4.9 | 10 | 3.3 | 0.229 | 33.3 | 1.4 | 0.001 ** |
| Chronic renal disease (%) | 12.4 | 15 | 11.7 | 0.678 | 33.3 | 9.7 | 0.023 * |
| Diabetes mellitus (%) | 28.4 | 25 | 30 | 0.698 | 55.6 | 25 | 0.153 |
| Hypertension (%) | 46.9 | 30 | 53.3 | 0.081 | 55.6 | 45.8 | 0.854 |
| Obesity (%) | 34.6 | 40 | 33.3 | 0.600 | 44.4 | 33.3 | 0.505 |
| Neoplasia (%) | 15.2 | 20 | 13.6 | 0.414 | 33.3 | 12.9 | 0.064 |
| Hepatitis B virus (%) | 0 | 0 | 0 | - | 0 | 0 | - |
| Cerebrovascular disease (%) | 5.1 | 5 | 5.1 | 0.964 | 0 | 5.7 | 0.491 |
| Cardiovascular disease (%) | 8.9 | 0 | 11.9 | 0.119 | 0 | 10 | 0.352 |
| Heart failure (%) | 7.6 | 15 | 5.1 | 0.122 | 22.2 | 5.7 | 0.050 |
| Immunosuppression (%) | 6.4 | 10 | 5.1 | 0.400 | 22.2 | 4.3 | 0.023 * |
| Number of comorbidities | 1 | 1 | 1 | 0.402 | 2 | 1 | 0.006 ** |
| (median, IQR) | (0–2) | (0–2) | (0–2) | (2–3) | (0–2) | ||
| Days of symptoms | 8 | 7 | 9 | 0.071 | 5 | 8 | 0.057 |
| (median, IQR) | (5–10) | (4.75–9) | (6–10) | (4–6) | (7–10) | ||
| Dyspnea (%) | 69.1 | 75 | 66.7 | 0.513 | 66.7 | 69.4 | 0.705 |
| Cough (%) | 76.5 | 75 | 76.7 | 0.851 | 66.7 | 77.8 | 0.914 |
| Altered consciousness (%) | 3.7 | 5 | 3.3 | 0.724 | 22.2 | 1.3 | 0.001 ** |
| Fever (%) | 44.4 | 50 | 41.7 | 0.466 | 44.4 | 44.4 | 0.598 |
| SaO2 2 [%] | 96.2 | 95.2 | 96.6 | 0.012 * | 95 | 96.4 | 0.014 * |
| (mean, SD) | (0.2) | (0.6) | (0.2) | (0.9) | (0.24) | ||
| Supplementary O2 (%) | 64.2 | 85 | 56.7 | 0.025 * | 77.8 | 62.5 | 0.502 |
| RR 3 [breaths/min] | 24 | 26 | 21 | 0.009 ** | 24 | 24 | 0.245 |
| (median, IQR) | (20–28) | (24–28) | (18–24.5) | (22–28) | (21–28) | ||
| HR 4 [beats/min] | 81 | 85 | 76 | 0.030 * | 82 | 81 | 0.692 |
| (median, IQR) | (70–90) | (79.5–96) | (67.8–89) | (73–86) | (70–90) | ||
| SBP 5 (mmHg) | 127.3 | 127.5 | 127.2 | 0.939 | 130.9 | 126.8 | 0.893 |
| (mean, SD) | (1.7) | (2.9) | (2.1) | (7.3) | (1.7) | ||
| Rx. thorax [RALE 6] | 4 | 4 | 4 | 0.019 * | 5 | 4 | 0.001 ** |
| (median, IQR) | (3–5) | (3–5) | (3–5) | (5–8) | (3–5) | ||
| CT PTE 7 (%) | 8,6 | 5 | 10,0 | 0.504 | 11.1 | 8.3 | 0.682 |
| PaO2-FiO2 8 ratio | 366.3 | 306.2 | 388.3 | 0.001 ** | 289.9 | 373.1 | 0.015 * |
| (mean, SD) | (10.8) | (23) | (11.1) | (30.8) | (10.8) | ||
| Glucose [mg/dL] | 147.2 | 126.75 | 154 | 0.139 | 160.7 | 145.5 | 0.862 |
| (mean, SD) | (7.5) | (9.5) | (9.4) | (22.2) | (8) | ||
| eGFR 9 | 0.001 ** | ||||||
| [ml/min/1.73 m2 9] | 80 | 75 | 81 | 0.330 | 52.6 | 83.4 | |
| (mean, SD) | (2.8) | (5.9) | (3.1) | (7.4) | (2.7) | ||
| AST 10 [U/L] | 52.6 | 66 | 48.6 | 0.920 | 39.2 | 47.6 | 0.837 |
| (mean, SD) | (6.3) | (17.7) | (6.1) | (6.7) | (6.5) | ||
| Ferritin [ng/mL] | 824.6 | 745.8 | 848.4 | 681.5 | 832.5 | ||
| (mean, SD) | (80.7) | (132.7) | (99.3) | 0.814 | (183.3) | (87.7) | 0.914 |
| >700 ng/mL (%) | 44.4 | 45 | 43.3 | 0.852 | 33.3 | 45.2 | 0.731 |
| LDH 11 [U/L] | 337.2 | 365.9 | 329.6 | 0.738 | 339.8 | 336.9 | 0.849 |
| (mean, SD) | (13.3) | (33.4) | (14) | 0.254 | (44.9) | (14) | 0.769 |
| >400 U/L (%) | 21 | 30 | 18.3 | 22.2 | 20.8 | ||
| CRP 12 [mg/L] | 91.5 | 84.2 | 92.4 | 0.473 | 91.5 | 91.5 | 0.681 |
| (mean, SD) | (6.8) | (14.1) | (7.7) | (23) | (7.1) | ||
| >15 mg/mL (%) | 95.1 | 100 | 93.3 | 0.240 | 100 | 94.4 | 0.497 |
| Lymphocyte [103/μL] | 0.87 | 0.83 | 0.88 | 0.763 | 0.7 | 0.89 | 0.101 |
| (mean, SD) | (0.05) | (0.1) | (0,06) | (0.15) | (0.05) | ||
| Neutrophil-lymphocyte ratio | 6.4 | 7.3 | 6.1 | 0.540 | 8.6 | 6.1 | 0.264 |
| (mean, SD) | (0.46) | (0.8) | (0.6) | 0.711 | (2.1) | (0.4) | 0.706 |
| >10 (%) | 17.3 | 7.31 | 16.7 | 11.1 | 18.1 | ||
| Platelets [103/μL] | 200.6 | 163.4 | 214 | 0.008 ** | 152.6 | 206.6 | 0.020 * |
| (mean, SD) | (8.3) | (12.7) | (9.9) | (20.6) | (8.8) | ||
| D dimer [mg/L] | 1.68 | 1.1 | 1.9 | 0.144 | 4.4 | 1.3 | 0.168 |
| (mean, SD) | (0.5) | (0.3) | (0.6) | 0.538 | (3.9) | (0.2) | 0.587 |
| >15 mg/mL (%) | 19.7 | 10 | 23.3 | 11.1 | 20.8 | ||
| NT-proBNP 13 [pg/mL] | 815 | 1007.7 | 741.8 | 0.180 | 2086.9 | 593.8 | 0.038 * |
| (mean, SD) | (171.2) | (372.5) | (188.7) | (731.9) | (136.6) | ||
| NEWS2 | 4 | 6 | 3 | 0.001 ** | 5 | 3 | 0.041 * |
| (median, IQR) | (2–6) | (5–7) | (2–5) | (3–7) | (2–6) | ||
| ECO LUS total | 15 | 18 | 14 | 0.177 | 18 | 15 | 0.541 |
| (median, IQR) | (10–19) | (13.5–19) | (9.8–18.3) | 0.019 * | (10–19) | (10–19) | 0.271 |
| >15 (%) | 49.4 | 70 | 43.3 | 66.7 | 47,2 | ||
| SEIMC Score | 6 | 6 | 6 | 0.516 | 11 | 5 | 0.008 ** |
| (median, IQR) | (4–10) | (5–10) | (4–9) | (9–14) | (4–8) | ||
| COWS | 0.52 | 0.72 | 0.47 | 0.019 * | 0.71 | 0.5 | 0.243 |
| (mean, SD) | (0.05) | (0.10) | (0.06) | (0.15) | (0.06) |
Appendix B
| Poor Outcome p-Value (CI) | Dead 28 Days p-Value (CI) | |
|---|---|---|
| LUS vs. NEWS2 | 0.028 * (−0.319–0.018) | 0.507 (−0.357–0.176) |
| LUS vs. SEIMC | 0.004 ** (−0.471–0.090) | 0.812 (−0.172–0.220) |
| LUS vs. COWS | < 0.001 ** (−0.201–0.067) | 0.007 ** (−0.226–0.036) |
| COWS vs. NEWS2 | 0.590 (−0.160–0.233) | 0.676 (−0.151–0.091) |
| COWS vs. SEIMC | 0.059 (−0.006–0.322) | 0.081 (−0.318–0.018) |
| NEWS2 vs. SEIMC | 0.049 * (0.0003–0.385) | 0.126 (−0.435–0.054) |
References
- COVID-19 Map—Johns Hopkins Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/map.html (accessed on 1 June 2021).
- Ministerio de Sanidad, Consumo y Bienestar Social—Profesionales—Situación Actual Coronavirus. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/situacionActual.htm (accessed on 10 June 2021).
- Instituto de Salud Carlos III. Informe No° 81. In Situación de COVID-19 en España a 2 de Junio de 2021; Ministerio de Ciencia. e Innovación: Madrid, Spain, 2021; Volume 1. [Google Scholar]
- Budinger, G.R.S.; Misharin, A.V.; Ridge, K.M.; Singer, B.D.; Wunderink, R.G. Distinctive Features of Severe SARS-CoV-2 Pneumonia. J. Clin. Investig. 2021, 131, e149412. [Google Scholar] [CrossRef]
- Royal College of Physicians. National Early Warning Score (NEWS) 2; Standardising the Assessment of Acute-Illness Severity in the NHS Updated Report of a Working Party Executive Summary and Recommendations; Royal College of Physicians: London, UK, 2017; pp. 1–15. [Google Scholar]
- Webb, B.J.; Peltan, I.D.; Jensen, P.; Hoda, D.; Hunter, B.; Silver, A.; Starr, N.; Buckel, W.; Grisel, N.; Hummel, E.; et al. Clinical Criteria for COVID-19—Associated Hyperinflammatory Syndrome: A Cohort Study. Lancet Rheumatol. 2020, 2, 754–763. [Google Scholar] [CrossRef]
- Soldati, G.; Smargiassi, A.; Inchingolo, R.; Buonsenso, D.; Perrone, T.; Briganti, D.F.; Perlini, S.; Torri, E.; Mariani, A.; Mossolani, E.E.; et al. Proposal for International Standardization of the Use of Lung Ultrasound for Patients with COVID-19. J. Ultrasound Med. 2020, 39, 1413–1419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boero, E.; Rovida, S.; Schreiber, A.; Berchialla, P.; Charrier, L.; Cravino, M.M.; Converso, M.; Gollini, P.; Puppo, M.; Gravina, A.; et al. The COVID-19 Worsening Score (COWS)—A Predictive Bedside Tool for Critical Illness. Echocardiography 2021, 38, 207–216. [Google Scholar] [CrossRef]
- Berenguer, J.; Borobia, A.M.; Ryan, P.; Rodríguez-Banõ, J.; Bellón, J.M.; Jarrín, I.; Carratalà, J.; Pachón, J.; Carcas, A.J.; Yllescas, M.; et al. Development and Validation of a Prediction Model for 30-Day Mortality in Hospitalised Patients with COVID-19: The COVID-19 SEIMC Score. Thorax 2021, 76, 1–10. [Google Scholar] [CrossRef]
- Dietrich, C.F.; Mathis, G.; Blaivas, M.; Volpicelli, G.; Seibel, A.; Atkinson, N.S.; Cui, X.W.; Mei, F.; Schreiber-Dietrich, D.; Yi, D. Lung Artefacts and Their Use. Med. Ultrason. 2016, 18, 488–499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allinovi, M.; Parise, A.; Giacalone, M.; Amerio, A.; Delsante, M.; Odone, A.; Franci, A.; Gigliotti, F.; Amadasi, S.; Delmonte, D.; et al. Lung Ultrasound May Support Diagnosis and Monitoring of COVID-19 Pneumonia. Ultrasound Med. Biol. 2020, 46, 2908–2917. [Google Scholar] [CrossRef]
- Casella, F.; Barchiesi, M.; Leidi, F.; Russo, G.; Casazza, G.; Valerio, G.; Torzillo, D.; Ceriani, E.; Medico, M.D.; Brambilla, A.M.; et al. Lung Ultrasonography: A Prognostic Tool in Non-ICU Hospitalized Patients with COVID-19 Pneumonia. Eur. J. Intern. Med. 2021, 85, 34–40. [Google Scholar] [CrossRef]
- Song, G.; Qiao, W.; Wang, X.; Yu, X. Association of Lung Ultrasound Score with Mortality and Severity of COVID-19: A Meta-Analysis and Trial Sequential Analysis. Int. J. Infect. Dis. 2021, 603–609. [Google Scholar] [CrossRef]
- Nouvenne, A.; Zani, M.D.; Milanese, G.; Parise, A.; Baciarello, M.; Bignami, E.G.; Odone, A.; Sverzellati, N.; Meschi, T.; Ticinesi, A. Lung Ultrasound in COVID-19 Pneumonia: Correlations with Chest CT on Hospital Admission. Respiration 2020, 99, 617–624. [Google Scholar] [CrossRef]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G.M. Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis Or Diagnosis (TRIPOD): The TRIPOD Statement. J. Br. Surg. 2015, 102, 148–158. [Google Scholar] [CrossRef] [Green Version]
- Kevadiya, B.D.; Machhi, J.; Herskovitz, J.; Oleynikov, M.D.; Blomberg, W.R.; Bajwa, N.; Soni, D.; Das, S.; Hasan, M.; Patel, M.; et al. Diagnostics for SARS-CoV-2 Infections. Nat. Mater. 2021, 20, 593–605. [Google Scholar] [CrossRef] [PubMed]
- Mento, F.; Perrone, T.; Macioce, V.N.; Tursi, F.; Buonsenso, D.; Torri, E.; Smargiassi, A.; Inchingolo, R.; Soldati, G.; Demi, L. On the Impact of Different Lung Ultrasound Imaging Protocols in the Evaluation of Patients Affected by Coronavirus Disease 2019. J. Ultrasound Med. 2021, 40, 2235–2238. [Google Scholar] [CrossRef]
- Myrstad, M.; Ihle-Hansen, H.; Tveita, A.A.; Andersen, E.L.; Nygård, S.; Tveit, A.; Berge, T. National Early Warning Score 2 (NEWS2) on Admission Predicts Severe Disease and in-Hospital Mortality from COVID-19—A Prospective Cohort Study. Scand. J. Trauma Resusc. Emerg. Med. 2020, 28, 66. [Google Scholar] [CrossRef] [PubMed]
- Liang, W.; Liang, H.; Ou, L.; Chen, B.; Chen, A.; Li, C.; Li, Y.; Guan, W.; Sang, L.; Lu, J.; et al. Development and Validation of a Clinical Risk Score to Predict the Occurrence of Critical Illness in Hospitalized Patients with COVID-19. JAMA Intern. Med. 2020, 180, 1081–1089. [Google Scholar] [CrossRef] [PubMed]
- Swets, J.A. Measuring the Accuracy of Diagnostic Systems. Science 1988, 240, 1285–1293. [Google Scholar] [CrossRef] [Green Version]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the Areas under Two or More Correlated Receiver Operating Characteristic Curves: A Nonparametric Approach. Biometrics 1988, 44, 837. [Google Scholar] [CrossRef]
- Jasiński, T.; Stefaniak, J. COVID-19 and Haemodynamic Failure: A Point of View on Mechanisms and Treatment. Anaesthesiol. Intensive Ther. 2020, 52, 409–417. [Google Scholar] [CrossRef]
- Manson, J.J.; Crooks, C.; Naja, M.; Ledlie, A.; Goulden, B.; Liddle, T.; Khan, E.; Mehta, P.; Martin-Gutierrez, L.; Waddington, K.E.; et al. COVID-19-Associated Hyperinflammation and Escalation of Patient Care: A Retrospective Longitudinal Cohort Study. Lancet Rheumatol. 2020, 2, 594–602. [Google Scholar] [CrossRef]
- Schalekamp, S.; Bleeker-Rovers, C.P.; Beenen, L.F.M.; Quarles van Ufford, H.M.E.; Gietema, H.A.; Lauran Stöger, J.; Harris, V.; Reijers, M.H.E.; Rahamat-Langendoen, J.; Korevaar, D.A.; et al. Chest CT in the Emergency Department for Diagnosis of COVID-19 Pneumonia: Dutch Experience. Radiology 2021, 298, 98–106. [Google Scholar] [CrossRef]
- Liu, H.; Chen, J.; Yang, Q.; Lei, F.; Zhang, C.; Qin, J.-J.; Chen, Z.; Zhu, L.; Song, X.; Bai, L.; et al. Development and Validation of a Risk Score Using Complete Blood Count to Predict In-Hospital Mortality in COVID-19 Patients. Med 2021, 2, 435–447. [Google Scholar] [CrossRef]
- Grifoni, E.; Valoriani, A.; Cei, F.; Vannucchi, V.; Moroni, F.; Pelagatti, L.; Tarquini, R.; Landini, G.; Masotti, L. The CALL Score for Predicting Outcomes in Patients With COVID-19. Clin. Infect. Dis. 2021, 72, 182–183. [Google Scholar] [CrossRef]
- Alfaro-Martínez, J.J.; Calbo Mayo, J.; Molina Cifuentes, M.; Abizanda Soler, P.; Guillén Martínez, S.; Rodríguez Marín, Y.; Sirvent Segovia, A.E.; Nuñez Ares, A.; Alcaraz Barcelona, M.; Paterna Mellinas, G.; et al. Generation and Validation of In-Hospital Mortality Prediction Score in COVID-19 Patients: Alba-Score. Curr. Med. Res. Opin. 2021, 37, 719–726. [Google Scholar] [CrossRef] [PubMed]
- Sorlini, C.; Femia, M.; Nattino, G.; Bellone, P.; Gesu, E.; Francione, P.; Paternò, M.; Grillo, P.; Ruffino, A.; Bertolini, G.; et al. The Role of Lung Ultrasound as a Frontline Diagnostic Tool in the Era of COVID-19 Outbreak. Intern. Emerg. Med. 2021, 16, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Yoshioka, T.; Funada, S.; Luo, Y. The Inherent Problems with the Generalizability of the CALL Score: Towards Reliable Clinical Prediction Models for Coronavirus Disease 2019 (COVID-19). Clin. Infect. Dis. 2020, 73, e2818. [Google Scholar] [CrossRef] [PubMed]
- García Clemente, M.M.; Herrero Huertas, J.; Fernández Fernández, A.; De La Escosura Muñoz, C.; Enríquez Rodríguez, A.I.; Pérez Martínez, L.; Gómez Mañas, S.; Iscar Urrutia, M.; López González, F.J.; Madrid Carbajal, C.J.; et al. Assessment of Risk Scores in COVID-19. Int. J. Clin. Pract. 2020, e13705. [Google Scholar] [CrossRef]
- Saleh, A.; Ahmed, M.; Abdel-lateif, A. Comparison of the Mortality Prediction of Different ICU Scoring Systems (APACHE II and III, SAPS II, and SOFA) in Acute Respiratory Distress Syndrome Patients. Chest 2016, 149, A147. [Google Scholar] [CrossRef]
- Shi, Y.; Pandita, A.; Hardesty, A.; McCarthy, M.; Aridi, J.; Weiss, Z.F.; Beckwith, C.G.; Farmakiotis, D. Validation of Pneumonia Prognostic Scores in a Statewide Cohort of Hospitalised Patients with COVID-19. Int. J. Clin. Pract. 2021, 75, e13926. [Google Scholar] [CrossRef]
- Holten, A.R.; Nore, K.G.; Tveiten, C.E.V.W.K.; Olasveengen, T.M.; Tonby, K. Predicting Severe COVID-19 in the Emergency Department. Resusc. Plus 2020, 4, 100042. [Google Scholar] [CrossRef]
- Kamran, S.M.; Mirza, Z.-H.; Moeed, H.A.; Naseem, A.; Hussain, M.; Fazal, I.; Saeed, F.; Alamgir, W.; Saleem, S.; Riaz, S. CALL Score and RAS Score as Predictive Models for Coronavirus Disease 2019. Cureus 2020, 12, 11368. [Google Scholar] [CrossRef]



| Vs. Poor Outcome | Vs. Dead at 28 Days | |||
|---|---|---|---|---|
| p | OR (CI) | p | OR (CI) | |
| NEWS2 | 0.001 ** | 1.611 (1.228–2.113) | 0.041 * | 1.315 (1.012–1.710) |
| LUS > 15 | 0.019 * | 3.5 (1.192–10.275) | 0.271 | 2.235 (0.519–9.636) |
| SEIMC Score | 0.516 | 1.034 (0.935–1.143) | 0.008 ** | 1.190 (1.046–1.354) |
| COWS | 0.019 * | 3.968 (1.251–12.573) | 0.243 | 2.552 (0.530–12.283) |
| (a) | ||||
|---|---|---|---|---|
| Poor Outcome | AUC | Optimal Cut-Off Point Value | Sensitivity | Specificity |
| NEWS2 | 0.785 * | >5 | 0.619 | 0.850 |
| LUS | 0.617 | >17 | 0.619 | 0.700 |
| SEIMC Score | 0.593 | >9 | 0.333 | 0.783 |
| COWS | 0.751 * | ≥0.1007 | 0.857 | 0.617 |
| (b) | ||||
| Dead 28 Days | AUC | Optimal Cut-Off Point Value | Sensitivity | Specificity |
| NEWS2 | 0.654 | >5 | 0.444 | 0.887 |
| LUS | 0.560 | >17 | 0.556 | 0.634 |
| SEIMC Score | 0.840 * | >9 | 0.667 | 0.803 |
| COWS | 0.690 | ≥0.1007 | 0.889 | 0.431 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gil-Rodríguez, J.; Martos-Ruiz, M.; Peregrina-Rivas, J.-A.; Aranda-Laserna, P.; Benavente-Fernández, A.; Melchor, J.; Guirao-Arrabal, E. Lung Ultrasound, Clinical and Analytic Scoring Systems as Prognostic Tools in SARS-CoV-2 Pneumonia: A Validating Cohort. Diagnostics 2021, 11, 2211. https://doi.org/10.3390/diagnostics11122211
Gil-Rodríguez J, Martos-Ruiz M, Peregrina-Rivas J-A, Aranda-Laserna P, Benavente-Fernández A, Melchor J, Guirao-Arrabal E. Lung Ultrasound, Clinical and Analytic Scoring Systems as Prognostic Tools in SARS-CoV-2 Pneumonia: A Validating Cohort. Diagnostics. 2021; 11(12):2211. https://doi.org/10.3390/diagnostics11122211
Chicago/Turabian StyleGil-Rodríguez, Jaime, Michel Martos-Ruiz, José-Antonio Peregrina-Rivas, Pablo Aranda-Laserna, Alberto Benavente-Fernández, Juan Melchor, and Emilio Guirao-Arrabal. 2021. "Lung Ultrasound, Clinical and Analytic Scoring Systems as Prognostic Tools in SARS-CoV-2 Pneumonia: A Validating Cohort" Diagnostics 11, no. 12: 2211. https://doi.org/10.3390/diagnostics11122211