
Deep Learning on Histopathological Images for Colorectal Cancer Diagnosis: A Systematic Review

 ,
,  ,
,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
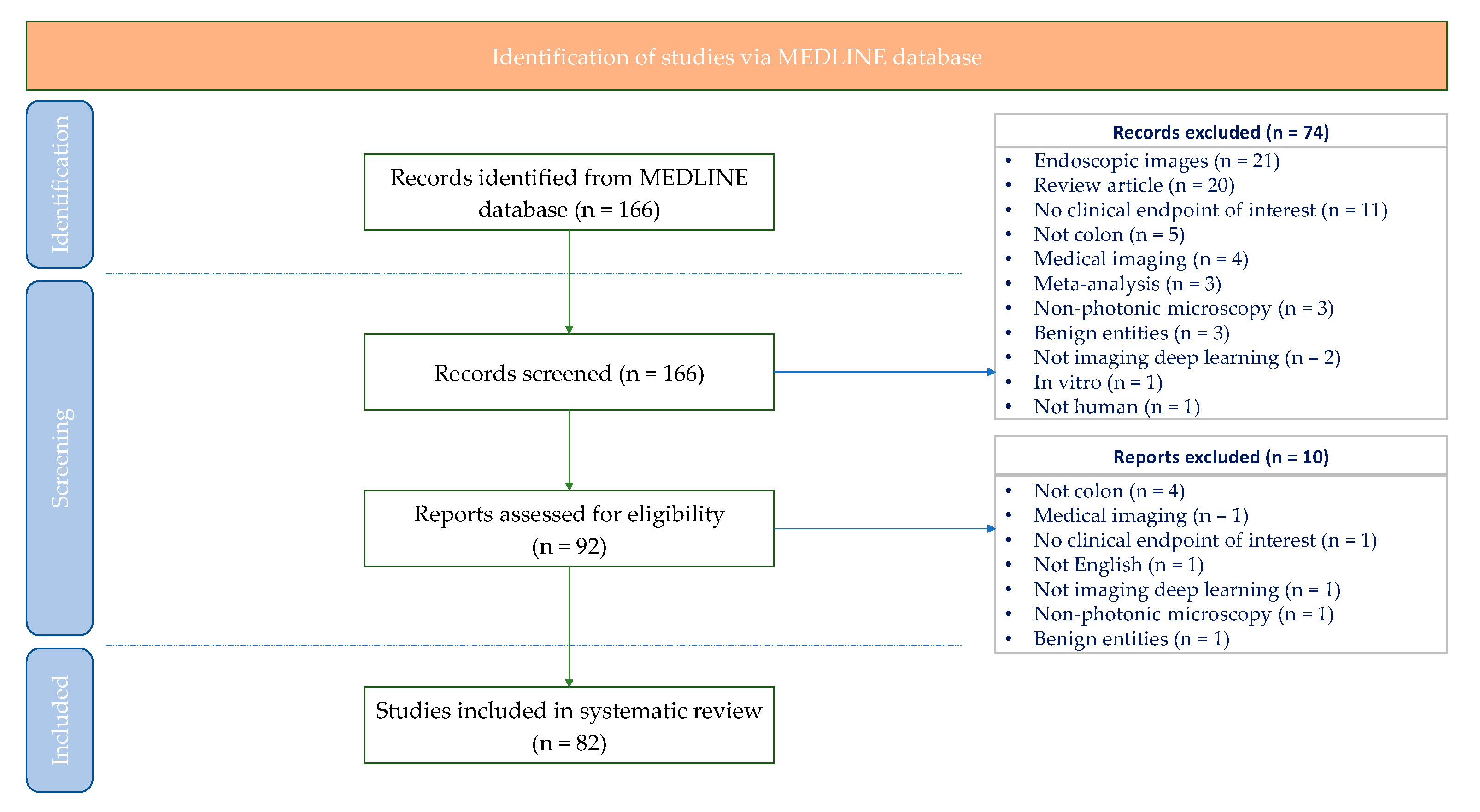
2.1. Search Strategy
2.2. Study Eligibility Criteria
2.3. Study Selection
2.4. Data Extraction
3. Results
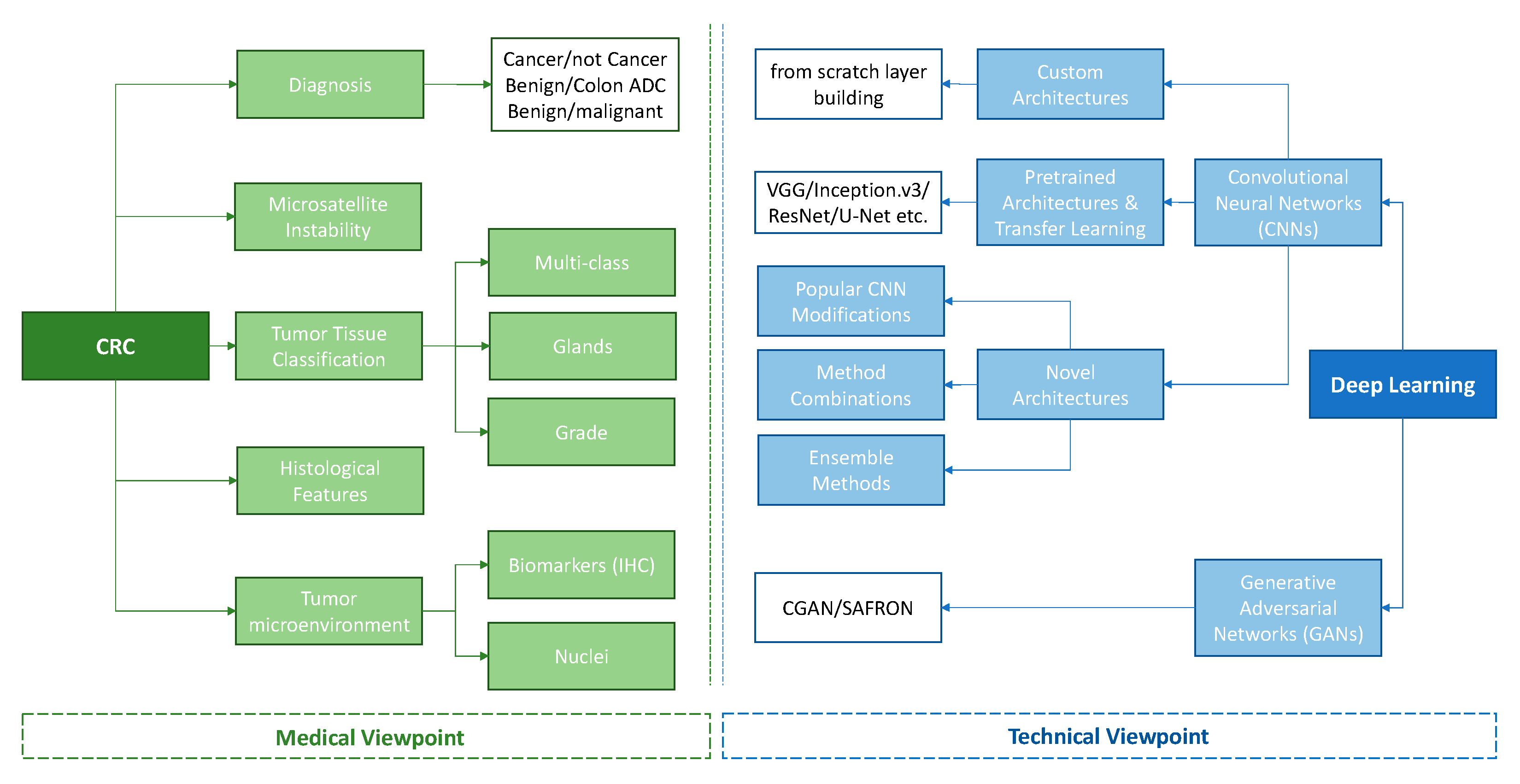
3.1. Medical Viewpoint
3.1.1. Diagnosis
3.1.2. Tumor Tissue Classification (Non-Neoplastic, Benign, Malignant, Grade, Architecture and Cellular Characteristics)
3.1.3. Tumor Microenvironment
3.1.4. Histological Features Related to Prognosis, Metastasis and Survival
3.1.5. Microsatellite Instability
3.2. Technical Viewpoint
3.2.1. Custom CNN Architecture
3.2.2. Popular Architectures with Transfer Learning
3.2.3. Novel Architectures
3.2.4. Improving Training with GANs

{kind=link}
{kind=link}
{kind=link}
| Year | First Author | Journal | Aim of Medical Research | Technical Method | Classification Details | Dataset | Performance Metrics |
|---|---|---|---|---|---|---|---|
| 2016 | Sirinukunwattana [84] | IEEE Trans Med Imaging | Detection and classification of nuclei | Custom CNN architecture (7-versions) based on the spatially Constrain Regression (a priori) | 4-class: epithelial, inflammatory, fibroblast, miscellaneous | >20,000 annotated nuclei from 100 histology images from 10 WSIs | Detection Precision: 0.781, Recall: 0.827, F1 score: 0.802, Classification F1 score: 0.784, AUC: 0.917, Combined detection and classification F1 score: 0.692 |
| Xu [81] | Neurocomputing | Classification of epithelial and stromal regions | Custom Simple CNN Architecture with 4 Layers (2 × CL and 2 FC) with SVM | Binary (epithelium/stroma) | 1376 IHC-stained images of CRC | Classification F1 score: 100%, ACC: 100%, MCC: 100% | |
| 2017 | Chen [87] | Med Image Anal | Detection and classification of nuclei | Custom CNN: Novel deep contour-aware network | Binary (bening/malignant) | (1) 2015 MICCAI Gland Segmentation Challenge, Training 85 Images Testing 80, (2) 2015 MICCAI Nuclei Segmentation Challenge: Training 15 Images, Testing 18 images | Detection results (MICCAI Glas): F1 score = 0.887, DICE index 0.868 Hausdorff = 74.731 Segmentation results: D1 and D2 metrics from Challenge |
| Popovici [80] | Bioinformatics | Prediction of molecular subtypes | VGG-f (MatConvNet library) | 5-class: subtypes (Budinská et al., 2013) Μolecular subtypes (denoted A-E) | PETACCURACY:3 clinical trial (Van Cutsem et al., 2009) 300 H/E images | ACC: 0.84, Confusion metrics Precision and Recall per class | |
| Xu [63] | IEEE Trans Biomed Eng | Classification of Glands | Custom architecture: 3 channel fusions, one based on Faster R-CNN and two based on VGG-16 | Binary (bening/malignant) | 2015 MICCAI Gland Segmentation Challenge, Training 85 Images Testing 80 Images | Detection results (MICCAI Glas): F1 score (0.893 + 0.843)/2, DICE index (0.908 + 0.833)/2, Hausdorff (44.129 + 116.821)/2 | |
| Haj-Hassan [54] | J Pathol Inform | Tumor tissue classification | Custom Simple CNN (2CL and 1FC), with or without initial segmentation | 3-class: benign hyperplasia, intraepithelial neoplasia, carcinoma | CHU Nancy Brabois Hospital: 16 multispectral images | Dice and Jaccard with std for segmentation ACC: 99.17% | |
| Xu [57] | BMC Bioinformatics | Tumor tissue classification | Alexnet—SVM (shared by the Cognitive Vision team at ImageNet LSVRC 2013) | (1) Binary (cancer/not cancer (2) 6-class: normal (N), ADC, mucinous carcinoma (MC),serrated carcinoma (SC), papillary carcinoma (PC), cribriform comedo-type adenocarcinoma (CCTA) | 2014 MICCAI 2014 Brain Tumor Digital Pathology Challenge and CRC image dataset (1) Total 717 H/E Total 693 | ACC: (1) Binary: 98% (2) Multiclass: 87.2% | |
| Jia [41] | IEEE Trans Med Imaging | Diagnosis | 3 Stage VGG-16 (publicly available Caffe toolbox) | (1) Binary (Cancer/non cancer) (2) Binary: TMAs (Cancer/non-Cancer) | (1) 330/580 images (CA/NC) (2) 30/30 images (CA/NC) | (2) ODS: 0.447, F-measure: 0.622 (CA), 0.998 (NC) | |
| Kainz [65] | PeerJ | Classification of Glands | 2 × custom CNNs (4 × CL, 2 × FC) | 4-class (benign, benign background, malignant, malignant background) add background for each class of the challenge | 2015 MICCAI Gland Segmentation Challenge, Training 85 Images (37 benign and 48 malignant). Testing 80 (37/43) | Detection results (MICCAI Glas): F1 score = (0.68 + 0.61)/2, DICE index (0.75 + 0.65)/2, Hausdorff (103.49 + 187.76)/2 | |
| Awan [67] | Sci Rep | Grading of CRC | UNET-based architecture | (A) Binary (normal/cancer) (B) 3-class: normal/low grade/high grade | 38 WSIs, extracted 139 parts (71 normal, 33 low grade, 35 high grade) | (A) Binary ACC: 97% (B) 3-vlass ACC: 91% | |
| Wang [58] | Annu Int Conf IEEE Eng Med Biol Soc | Tumor tissue classification | Simple architecture consisting of 1 CL and 1 FC, which is simultaneously operated in both decomposed images | 8-class: tumor epithelium, simple stroma, complex stroma, immune cells, debris, normal mucosal glands, adipose tissue, background | University Medical Center Mannheim 1.000 images | ACC: 92.6 ± 1.2 | |
| 2018 | Bychkov [92] | Sci Rep | Survival | VGG-16 followed by a recurrent ResNet | Binary (low/high risk 5-year disease-specific survival) | Helsinki University Central Hospital, 420 ΤΜAs | Hazard Ratio: 2.3; CI 95%: 1.79–3.03, AUC 0.69 |
| Eycke [66] | Med Image Anal | Tumor tissue classification/IHC biomarkers quantification | VGG-based architecture including residual units | Binary (bening/malignant) | 2015 MICCAI Gland Segmentation Challenge, Training 85 Images Testing 80 (37/43) | Detection results (MICCAI Glas): F1 score = (0.895 + 0.788)/2, DICE index (0.902 + 0.841)/2, Hausdorff (42.943 + 105.926)/2 | |
| Weis [83] | Diagn Pathol | Evaluation of tumor budding | Custom architecture consisting of 8 layers | Binary (Tumor bud/no tumor) | HeiData Training dataset 6292 images, 20 IHC pan-cytokeratin WSIs | R2 value: 0.86 | |
| Höfener [85] | Comput Med Imaging Graph | Nuclei detection | 2 × Custom CNN architectures based on PMaps approach | No classification, just nuclei detection | Same with Sirinukunwattana et al., >20,000 annotated nuclei from 100 histology images, from 10 WSI | F1 score of 22 different configurations of CNNs Best F1 score: 0.828 | |
| Graham [64] | Med Image Anal | Diagnosis | Custom complex architecture, named Mild-net | Binary (bening/malignant) | (1) MICCAI Gland Segmentation Challenge, (2) same as Awan et al., 2017 | (1) F1 socre: (0.914 + 0.844)/2, Dice: (0.913 + 0.836)/2, Hausdorff (41.54 + 105.89)/2 (2) F1 score: 0.825, Dice: 0.875, Hausdorff: 160.14 | |
| 2019 | Yoon [38] | J Digit Imaging | Diagnosis | 6 VGG-based approaches | Binary (normal/Cancer) | Center for CRC, National Cancer Center, Korea, 57 WSIs, 10.280 patches | ACC: 93.48%, SP: 92.76%, SE: 95.1% |
| Sari [69] | IEEE Trans Med Imaging | Grading of CRC | Feature Extraction from Deep Belief Network and classification employing linear SVM, Comparison with Alexnet, GoogleNet, Inceptionv3, and autoencoders | (1) 3-class: normal (N), Low Grade (LG), High Grade (HG) (2) 5-class: Normal, Low (1), Low (1–2), Low (2), High | (1) 3236 images 1001 N, 1703 LG, 532 HG) (2) 1468 images | (1) mean ACC: 96.13 (2) mean ACC: 79.28 | |
| Kather [99] | PLoS Med | Prediction of survival | 5 different well-known architectures pre-trained with ImageNet (1) VGG-19, (2) AlexNet, (3) SqueezeNet, (4) GoogleNet, (5) ResNet | 9-class: adipose tissue, background, debris, lymphocytes, mucus, smooth muscle, normal colon mucosa, cancer-associated stroma, CRC epithelium/survival predictions | (1) NCT, UMM 86 WSIs (100.000 patches) (2) 25 WSIs DACHS (3) 862 WSIs TCGA WSIs (4) 409 WSIs DACHS | 9-class: ACC: 94–99% | |
| Geessink [98] | Cell Onocol | Quantification of tumor–stroma ratio (TSR) for prognosis | Custom architecture proposed by Ciombi et al., 2017 (not included by our search) | 9-class: tumor, intratumoral stroma, necrosis, muscle, healthy epithelium, fatty tissue, lymphocytes, mucus, erythrocytes | Laboratory for Pathology Eastern Netherlands 74 WSIs | Overall ACC: 94.6% | |
| Shapcott [26] | Front Bioeng Biotechnol | Classification of nuclei | CNN based on Tensorflow “ciFar” model | 4-class: epithelial/inflammatory/ fibroblast/other | 853 images, 142 TCGA images | Detection ACC: 65% Classification ACC: 76% | |
| Qaiser [44] | Med Image Anal | Diagnosis | Custom architecture with (4 × CL + (ELU), 2FC + Dropout | Binary: tumor/non-tumor | (1) Warwick-UHCW 75 H/E WSIs (112.500 patches), (2) Warwick-Osaka 50 H/E WSIs (75.000 patches) | (A) PHP/CNN: F1 score 0.9243, Precision 0.9267 (B) PHP/CNN: F1 score 0.8273, Precision 0.8311 | |
| Swiderska-Chadaj [75] | Med Image Anal | Detection of lymphocytes | 4-different architectures: (1) Custom with 12CL, (2) U-net, (3) YOLLO (based on YOLO detector), (4) LSM (Sirinukunwattana et al. 2016) | 3-class: regular lymphocyte distribution/clustered cells/artifacts | 28 IHC WSIs | U-Net F1: 0.80 Recall: 0.74 Precision: 0.86 | |
| Graham [86] | Med Image Anal | Classification of nuclei | Novel CNN architecture (named HoVer-Net) based on Preact-ResNet50 | 4-class: normal, malignant, dysplastic epithelial/inflammatory/miscellaneous/spindle-shaped nuclei (fibroblast, muscle, endothelial) | (1) CoNSeP dataset, 16 WSIs, 41 H/E tiles, (2) Kumar (TCGA) 30 images, (3) CPM-15 (TCGA) 15 images, (4) CPM-17 (TCGA) 32 images, (5) TNBC (Curie Institute) 50 images, (6) CRCHisto 100 images | (1) Dice: 0.853, AJI: 0.571, DQ: 0.702, SQ: 0.778, PQ: 0.547, (2) Dice: 0.826, AJI: 0.618, DQ: 0.770, SQ: 0.773, PQ: 0.597, (4) Dice: 0.869, AJI: 0.705, DQ: 0.854, SQ: 0.814, PQ: 0.697 | |
| Rączkowski [56] | Sci Rep | Tumor tissue classification | Novel architecture (named ARA-CNN), based on ResNet and DarkNet | (A) Binary: tumor/stroma (B) 8-class: tumor epithelium, simple stroma, complex stroma, immune cells, debris, normal mucosal glands, adipose tissue, background | 5000 patches (same as Kather et al., 2016) | (1) AUC 0.998 ACC: 99.11 ± 0.97% (2) AUC 0.995 ACC: 92.44 ± 0.81% | |
| Sena [55] | Oncol Lett | Tumor tissue classification | Custom CNN (4CL, 3FC) | 4-class: normal mucosa, preneoplastic lesion, adenoma, cancer | Modena University Hospital, 393 WSIs | ACC: 81.7 | |
| 2020 | Iizuka [53] | Sci Rep | Tumor tissue classification | (1) Inception v3, (2) also train an RNN using the features extracted by the Inception | 3-class: adenocarcinoma/adenoma/non-neoplastic | Hiroshima University Hospital, Haradoi Hospital, TCGA, 4.036 WSIs | (1) AUC: (ADC: 0.967, Adenoma: 0.99), (2) AUC: (ADC: 0.963, Adenoma: 0.992) |
| Shaban [68] | IEEE Trans Med Imaging | Grading of CRC | Novel context-aware framework, consisting of two stacked CNNs | 3-Class: Normal, Low Grade, High Grade | Same as Awan et al., 2017 30000 patches | ACC: 95.70 | |
| Holland [52] | J Pathol Inform | Diagnosis | (1) ResNet (Turi Create library framework), (2) SqueezeNet (Turi Create library framework), (3) AlexNet (TensorFlow) | Binary (benign/malignant) | 10 slides, 1000 overlapping images | (1) ResNET: ACC: 98%, (2) AlexNet: ACC: 92.1% (3) SqueezeNet: ACC: 80.4% | |
| Echle [102] | Gastroenterology | MSI prediction | A modified version of Sufflenet (no details) | Binary (MSI/MSS) | TCGA, Darmkrebs: Chancen der Verhütung durch Screening (DACHS), “Quick and Simple and Reliable” trial (QUASAR), Netherlands Cohort Study (NLCS) QUASAR | Cross-validation cohort: mean AUC 0.92, AUPRC of 0.63 Validation cohort: AUROC 0.95 (without image-preprocessing) and AUROC 0.96 (after color normalization) | |
| Song [50] | BMJ | Diagnosis | A novel architecture based on DeepLab v2 and ResNet-34. Comparison with ResNet-50, DenseNet, Inception.v3, U-Net and DeepLab.v3 | Binary (colorectal adenoma/non-neoplasm) | Chinese People’s Liberation Army General Hospital, 411 slides CJFH and Cancer Hospital, Chinese Academy of Medical Sciences 168 slides | ACC: 90.4, AUC 0.92 | |
| Zhao [98] | EBioMedicine | Quantification of Tumor–stroma ratio (TSR) for prognosis | VGG-19 pre-trained on the ImageNet using transfer learning with SGDM | 9-class: Adipose, Background, Debris, Lymphocyte aggregates, Mucus, Muscle, Normal mucosa, Stroma, Tumor epithelium | TCGA-COAD (461 patients), TCGA-READ (172 patients) Same as Kather et al., 2019 | Pearson r (for TSR evaluation between CNN and pathologists): 0.939 ICC Mean difference in TSR evaluation between CNN and pathologists: 0.01 Stroma-high vs. stroma-low patients HR (OS): 1.72 (discovery cohort) and 2.08 (validation study) | |
| Cao [103] | Theranostics | MSI prediction | An ensemble pipeline for the likelihood of each patch, which is extracted from ResNet-18 | Binary (MSI/MSS) | TCGA (429 frozen slides), Tongshu Biotechnology Co. (785 FFPE slides) | (a) TCGA-COAD test set: AUC 0.8848 (b) External Validation set: AUC 0.8504 | |
| Xu [39] | J Pathol Inform | Diagnosis | Inception v3 pre-trained on ImageNet | Binary (normal/cancer) | St. Paul’s Hospital, 307 H/E images | Median ACC: 99.9% (normal slides), median ACC: 94.8% (cancer slides) Independent dataset: median ACC: 88.1%, AUROC 0.99 | |
| Jang [77] | World J Gastroenterol | Prediction of IHC biomarkers | (A) Simple CNN architecture for the initial binary problem (B) Inception.v3 for the main classification problem | A) Binary (tissue/no-tissue), B) Binary (normal/tumor), C) Binary (APC, KRAS, PIK3CA, SMAD4, TP53) wild-type/mutation | TCGA 629 WSIs (frozen tissue sections 7 FFPE) Seoul St. Mary Hospital (SMH) 142 WSIs | Frozen WSIs: AUC 0.693–0.809 FFPE WSIs: 0.645–0.783 | |
| Medela [113] | J Pathol Inform | Tumor tissue classification | The authors proposed several different functions. For the evaluation, a ResNet backbone was employed, with modified last layer | 8-class: tumor epithelium, simple stroma, complex stroma, immune cells, debris and mucus, mucosal glands, adipose tissue, background | University Medical Center Mannheim, 5.000 H/E images | With K = 3: BAC: 85.0 ± 0.6 Silhouette: 0.37 ± 0.02 Davis–Bouldin: 1.41 ± 0.08 With K = 5: BAC: 84.4 ± 0.8 Silhouette: 0.37 ± 0.02 Davis–Bouldin: 1.43 ± 0.09 With K = 7: BAC: 84.5 ± 0.3 Silhouette: 0.37 ± 0.02 Davis–Bouldin: 1.43 ± 0.09 | |
| Skrede [93] | Lancet | Survival | An ensemble approach with ten different CNN models based on DoMorev1 | 3-class (good/poor prognosis/uncertain) | >12.000.000 image tiles | Uncertain vs. good prognosis HR: 1.89 unadjusted and 1.56 adjusted Poor vs. good prognosis HR: 3.84 unadjusted and 3.04 adjusted Comparison of 3-year cancer-SP: survival of the good prognosis group to the uncertain and poor prognosis groups: SE: 52%, SP: 78%, PDV:19%, NPV: 94%, ACC: 76% Comparison of 3-year cancer- SP: survival of the good and uncertain prognosis groups with the poor prognosis group: SE: 69%, SP: 66%, PDV: 17%, NPV: 96%, ACC: 67%, AUC: 0.713 | |
| 2021 | Sirinukunwattana [109] | Gut | Consensus molecular subtypes (CMSs) prediction | Inception v3, as well as adversarial learning | 4-class: CMS1, CMS2, CMS3, CMS4 | (1) FOCUS 510 H/E slides, (2) TCGA 431 H/E slides, (3) GRAMPIAN 265 H/E slides Total: 1.206 slides | (1) AUC 0.88, (2) AUC 0.81, (3) AUC 0.82 |
| Yamashita [104] | Lancet Oncol | MSI prediction | 2-stage novel architecture based on a modified MobileNetV2 architecture pre-trained on ImageNet and fine-tuned by transfer learning on the Stanford-CRC dataset | (1) 7-classes: adipose tissue, necrotic debris, lymphocytes, mucin, stroma or smooth muscle, normal colorectal epithelium, and colorectal ADC epithelium (2) Binary (MSI/MSS) | Stanford-CRC dataset (internal): 66,578 tiles from 100 WSIs TCGA (external): 287,543 tiles from 484 WSIs | Internal: AUROC 0.931, External: AUROC 0.779 NPV:93.7%, SE:76.0%, SP:66.6% Reader study Model AUROC 0.865 Pathologist AUROC 0.605 | |
| Zhou [37] | Comput Med Imaging Graph | Tumor tissue classification | A novel 3-framework based on ResNet. Each framework employs different CNN for (a) Image-level binary classification (CA/NC), (b) Cell-level providing the cancer probability in heatmap, (c) Combination framework which merges the output of the previous ones | Binary (cancer/normal) | TCGA 1346 H/E WSIs, First Affiliated Hospital of Zhejiang University, First Affiliated Hospital of Soochow University, Nanjing First Hospital 50 slides | ACC: 0.946 Precision: 0.9636 Recall: 0.9815 F1 score: 0.9725 | |
| Masud [49] | Sensors | Diagnosis | Custom simple CNN architecture with 3 CL, two max pooling 1 batch normalization and 1 dropout | Binary (Colon ADC/colon benign) | LC25000 dataset, James A. Haley Veterans’ Hospital, 5.000 images of Colon ADC, 5.000 images of Colon Benign Tissue | Peak classification ACC: 96.33% F-measure score 96.38% for colon and lung cancer identification | |
| Kwak [88] | Front Oncol | Lymph Node Metastasis (LNM) prediction | U-Net based architecture without (no details) | 7-class: normal colon mucosa, stroma, lymphocytes, mucus, adipose tissue, smooth muscle, colon cancer epithelium | TCGA 1000.000 patches | LNM positive group/LNM negative group: OR = 26.654 (PTS score) Ability of PTS score to identify LNM in colon cancer: AUC 0.677 | |
| Krause [108] | J Pathol | MSI prediction | A conditional generative adversarial network (CGAN) for synthetic image generation with 6-CL for both the generator and discriminator network, and a modified ShuffleNet for classification | Binary (MSS/MSI) | TCGA (same as Kather et al., 2019) NLCS cohort (same as Echle et al., 2020) | AUROC 0.742 (patient cohort 1), 0.757 (patient cohort 2), 0.743 (synthetic images), 0.777 (both patient cohorts and synthetic images) | |
| Pai [72] | Histopathology | Tumor microenvironment | CNN developed on the deep learning platform (Aiforia Technologies, Helsinki, Finland) (No details of architecture) | (A) 7-class: carcinoma, tumor budding/poorly differentiated clusters, stroma, necrosis, mucin, smooth muscle, fat (B) 3-class: immature stroma, mature stroma, inflammatory stroma (C) 3-class: low grade carcinoma, high grade carcinoma, signet ring cell carcinoma (D) TILs identification | Stanford University Medical Center (same as Ma et al., 2019) 230 H/E TMAs | MMRD classifying SE: 88% and SP: 73% ICC between pathologists and model for TB/PDCs, type of stroma, carcinoma grade and TILs: 0.56 to 0.88 | |
| Wang [45] | BMC Med | Diagnosis | AI approach uses Inception.v3 CNN architecture with weights initialized from transfer learning | Binary (cancer/not cancer) | 14,234 CRC WSIs and 170.099 patches | ACC: 98.11%, AUC 99.83%, SP: 99.22%, SE: 96.99% | |
| Riasatian [112] | Med Image Anal | Tumor tissue classification | Proposed a novel architecture (called KimiaNet) based on the DenseNet | 8-class: tumor epithelium, simple stroma, complex stroma, immune cells, debris, normal mucosal glands, adipose tissue, background | TCGA 5.000 patches | ACC: 96.38% (KN-I) and 96.80% (KN-IV) | |
| Jiao [70] | Comput Methods Programs Biomed | Tumor microenvironment | (1) For the foreground, tissue detection employs based on U-NET (2) For 9-class problem, employs the same VGG-19 architecture as Kather et al. and Jhao et al. | 9-class: adipose tissue, background, debris, lymphocytes, mucus, smooth muscle, normal colon mucosa, cancer-associated stroma, colorectal ADC epithelium | TCGA 441 H/E images | PFI Stroma HR: 1.665 Necrosis HR: 1.552 Lymphocyte HR: 1.512 | |
| Nearchou [73] | Cancers | Classification of Desmoplastic reaction (DR) | DenseNet neural network, integrated within HALO® | Binary (Immature/other DR type) | 528 stage II and III CRC patients treated at the National Defense Medical College Hospital, Japan | Classifier’s performance: Dice score: 0.87 for the segmentation of myxoid stroma (test set: 40 patient samples) | |
| Lee [107] | Int J Cancer | MSI prediction | A framework of an initial CNN architecture based on binary classification of patches, followed by an Inception.v3 | (A) Binary (tissue/non-tissue) (B) Binary (normal/tumor) (C) Binary (MSS/MSI-H) | TCGA (COAD, READ) 1.336 frozen slides, 584 FFPE WSIs Seoul St. Mary’s Hospital 125 MSS FFPE WSIs, 149 MSI-H FFPE WSIs and 77 MSS FFPE WSIs | TCGA dataset: AUC 0.892 SMH dataset: AUC 0.972 | |
| Wulczyn [94] | NPJ Digit Med | Survival | (1) Tumor segmentation model based on Inception v3, (2) Prognostic model based on Mobile net | Binary (tumor/not tumor) | 27.300 slides Validation dataset 1: 9.340 Validation dataset 2:7.140 | Validation dataset 1: AUC 0.70 (95% CI: 0.66–0.73) Validation dataset 2: 0.69 (95% CI: 0.64–0.72) | |
| Shimada [111] | J Gastroenterol | Tumor mutational burden (TMB) prediction | Inception.v3 | (A) Binary (neoplastic/non-neoplastic) (B) Binary (TMB-High/TMB-Low) | Japanese cohort TCGA 201 H/E images | AUC 0.910 | |
| Bian [74] | Cancers | Prediction of IHC biomarkers | (1) Modification of Inceptionv3 adding residual block for cellular biomarker distribution prediction and (2) employs Shufflenet.v2, for tumor gene mutation detection | Binary (biomarkers prediction) CD3/CD20, panCK, DAP Binary (tumor mutation genes) APC, TP53, KRAS | Peking University Cancer Hospital and Institute (8697 H/E image patches), TCGA-Colon ADC (COAD) project (50,801 H/E image patches) | Biomarker’s prediction: ACC: 90.4% Tumor gene mutation detection: AUC = 0.76 (APC), AUC = 0.77 (KRAS), AUC = 0.79 (TP53) | |
| Schiele [100] | Cancers | Survival | InceptionResNet.v2 network, pre-trained on images from the ImageNet from Keras | Binary (low/high metastasis risk) | University Hospital Augsburg 291 pT3 and pT4 CRC patients | AUC 0.842, SP: 79.5%, SE: 75.6%, ACC: 75.8% | |
| Theodosi [101] | Microsc Res Tech | Survival | Pre-trained VGG-16 | Binary (5-year survivors/non-survivors) | University Hospital of Patras 162 IHC AIB1 images | ML system: Mean Overall Classification ACC: 87% DL system: Classification ACC: 97% | |
| Wang [105] | Bioinformatics | MSI prediction | A platform for automated classification where each user can define his own problem. Different popular architectures have been embedded (Inception-V3, ResNet50, Vgg19, MobileNetV2, ShuffleNetV2, and MNASNET) | Binary (MSI/MSS) | TCGA and WSIs | mean ROC (AUC 0.647 ± 0.029) | |
| Khened [115] | Sci Rep | Slide Image Segmentation and Analysis | A novel ensemble CNN framework with three pre-trained architectures: (a) U-net with DenceNet as the backbone, (b) U-Net with Inception-ResNet.v2 (Inception.v4), (c) Deeplabv3Plus with Xception | (1) Camelyon16: Binary (normal/metastasis), (2) Camelyon17: 4-class: (negative, ITC, Micro and Macro) | DigestPath 660 H/E images (250 with lesions, 410 with no lesions) | Dice: 0.782 | |
| Chuang [91] | Mod Pathol | Detection of nodal micro- and macro-metastasis | ResNet-50 | 3-class: Micrometastasis/Macrometastasis/Isolated tumor cells | Department of Pathology, Chang Gung Memorial Hospital in Linkou, Taiwan, 3182 H/E WSIs | Slides with >1 lymph node: Macromatastasis: AUC 0.9993, Micrometastasis: AUC 0.9956 Slides with a single lymph node: Macromatastasis: AUC 0.9944, Micrometastasis: AUC 0.9476 Algorithm ACC: 98.50% (95% CI: 97.75–99.25%) | |
| Jones [96] | Histopathology | Survival | Νo details for DL | 7-class: background, necrosis, epithelium, desmoplastic stroma, inflamed stroma, mucin, non-neoplastic mesenchymal components of bowel wall | Oxford Transanal Endoscopic Microsurgery (TEM) database H/E FFPE 150 patients | For desmoplastic to inflamed stroma ratio: AUC: 0.71, SE: 0.92, SP: 0.50, PPV: 0.30, NPV: 0.97 For stroma to immune ratio: AUC: 0.64, SE: 0.92, SP: 0.45, PPV: 0.27, NPV: 0.96 | |
| Pham [71] | Sci Rep | Tumor tissue classification | Time-frequency, time-space, long short-term memory (LSTM) networks | (1) binary (stroma/tumor), (2) 8-class: tumor, simple stroma, complex stroma, immune cells (lymphoid), debris, normal mucosal glands (mucosa), adipose tissue, background | Colorectal cancer data: University Medical Center Mannheim, 625 non-overlapping for each 8 types of tissue images, total 5000 tissue images | (1) ACC: 100, SE: 100, SP: 100, Precision: 100, F1-score: 1 (2) ACC: 99.96% | |
| Sarker [82] | Cancers | Prediction of IHC biomarker | U-net architecture with, in total, 23 convolutional layers | Binary (ICOS-positive cell/background) | Northern Ireland Biobank (same as Gray et al., 2017) | U-net highest performance: ACC: 98.93%, Dice: 68.84%, AJI = 53.92% (Backbone: ResNet101, optimizer: Adam, loss function: BCE, batch size: 8) | |
| Ben Hamida [61] | Comput Biol Med | Tumor tissue classification | (1) Comparison of 4 different architectures Alexnet, VGG-16, ResNet, DenseNet, Inceptionv3, with transfer learning strategy (2) Comparison of SegNet and U-Net for semantic Segmentation | (A) 8-class: tumor, stroma, tissue, necrosis, immune, fat, background, trash (B) Binary (tumor/no-tumor) | (1) AiCOLO (396 H/E slides), (2) NCT Biobank, University Medical Center Mannheim (100.000 H/E patches), (3) CRC-5000 dataset (5.000 images), (4) Warwick (16 H/E) | (1) ResNet On AiCOLO-8: overall ACC: 96.98% On CRC-5000: ACC: 96.77% On NCT-CRC-HE-100κ: ACC: 99.76% On merged: ACC: 99.98% (2) On AiCOLO-2 UNet: ACC: 76.18%, SegNet: ACC:81.22% | |
| Gupta [36] | Diagnostics | Tumor tissue classification | (a) VGG, ResNet, Inception, and IR-v2 for transfer learning, (b) Five types of customized architectures based on Inception-ResNet-v2 | Binary (normal/abnormal) | Chang Cung Memorial Hospital, 215 H/E WSIs, 1.303.012 patches | (a) IR-v2 performed better than the others: AUC 0.97, F-score: 0.97 (b) IR-v2 Type 5: AUC 0.99, F-score: 0.99 | |
| Terradillos [51] | J Pathol Inform | Diagnosis | Two-class classifier based on the Xception model architecture | Binary (benign/malignant) | Basurto University Hospital 14.712 images | SE: 0.8228 ± 0.1575 SP: 0.9114 ± 0.0814 | |
| Paladini [59] | J Imaging | Tumor tissue classification | 2 × Ensemble approach ResNet-101, ResNeXt-50, Inception-v3 and DensNet-161. (1) Mean-Ensemble-CNN approach, the predicted class of each image is assigned using the average of the predicted probabilities of four trained models. (2) In the NN-Ensemble-CNN approach, the deep features corresponding to the last FC layer are extracted from the four trained models | 1st database: 8-class (tumor epithelium, simple stroma, complex stroma, immune cells, debris, normal glands, adipose tissue, background) 2nd database: 7-class (tumor, complex stroma, stroma, smooth muscle, benign, inflammatory, debris) | Kather-CRC-2016 Database (5000 CRC images) and CRC-TP Database (280,000 CRC images) | Kather-CRC-2016 Database: Mean-Ensemble-CNN mean ACC: 96.16% NN-Ensemble-CNN mean ACC: 96.14% CRC-TP Database: Mean-Ensemble-CNN ACC: 86.97% Mean-Ensemble-CNN F1-Score: 86.99% NN-Ensemble-CNN ACC: 87.26% NN-Ensemble-CNN F1-Score: 87.27% | |
| Nguyen [110] | Mod Pathol | Consensus molecular subtypes (CMSs) prediction | A system for tissue detection in WSIs based on an ensemble learning method with two raters, VGG and CapsuleNet | Mucin-to-tumor area ratio quantification and binary classification: high/low mucin tumor | TCGA (871 slides) Bern (775 slides) The Cancer Imaging Archive (TCIA) (373 images) | ICC between pathologists and model for mucin-to-tumor area ratio score: 0.92 | |
| Toğaçar [48] | Comput Biol Med | Diagnosis | DarkNet-19 model based on the YOLO object detection model | Binary (benign/colon ADC) | 10.000 images | Colon ADC: ACC: 99.96% Colon benign: ACC: 99.96% Overall ACC: 99.69% | |
| Zhao [95] | Cancer Immunol Immunother | Lymph Node Metastasis (LNM) prediction | Same CNN as Zhao et al., 2020 (VGG-19 pre-trained on the ImageNet using transfer learning with SGDM) | 7-class: tumor epithelium, stroma, mucus, debris, normal mucosa, smooth muscle, lymphocytes, adipose | Training 279 H/E WSIs and Validation 194 H/E WSIs | High CLR density OS in the discovery cohort HR: 0.58 High CLR density OS in the validation cohort HR: 0.45 | |
| Kiehl [89] | EJC | Lymph Node Metastasis (LNM) prediction | ResNet18 pre-trained on H&E-stained slides of the CAMELYON16 challenge | Binary (LNM positive/LNM negative) | DACHS cohort (2,431 patients) TCGA (582 patients) | AUROC on the internal test set: 71% AUROC on the TCGA set: 61.2% | |
| Xu [76] | Caner Cell Int | Quantification of tumor–stroma ratio (TSR) for prognosis | VGG-19 with or w/o transfer learning | 9-class: adipose, background, debris, lymphocytes, mucus, muscle, normal mucosa, stroma, tumor epithelium | 283.000 H/E tiles, 154.400 IHC tiles from 243 slides from 121 patients, 22.500 IHC tiles from 114 slides from 57 patients | Test dataset: ACC 0.973, 95% CI 0.971–0.975 | |
| Yu [47] | Nat Commun | Diagnosis | No details for deep learning | Binary (cancer/not cancer) | 13.111 WSIs, 62,919 patches | Patch-level diagnosis AUC: 0.980 ± 0.014 Patient-level diagnosis AUC: 0.974 ± 0.013 | |
| Jiao [60] | Comput Methods Programs Biomed | Tumor tissue classification | Deep embedding-based logistic regression (DELR), using active learning for sample selection strategy | 8-class: adipose, debris, lymphocytes, mucus, smooth muscle, normal mucosa, stroma, tumor epithelium | 180.082 patches | AUC: >0.95 | |
| Brockmoeller [90] | J Pathol | Lymph Nodes Metastasis (LNM) prediction | ShuffleNet with transfer learning for end-to-end prediction | (A) Prediction: Any Lymph Node Metastasis (B) >1 lymph node positive | Køge/Roskilde and Slagelse Hospitals/pT2 cohort (311 H/E sections) Retrospective Danish Study/pT1 cohort (203 H/E sections) | pT1 CRC >1 LNM AUROC: 0.733 Any LNM AUROC: 0.567 pT2 CRC >1 LNM AUROC: 0.733 Any LNM AUROC: 0.711 | |
| Mittal [40] | Cancers | Diagnosis | Custom architecture with 12 CN and 3 FC | Binary (cancer/normal) | 15 TMAs | ACC:98%, SP: 98.6%, SE: 98.2% | |
| Kim [114] | Sci Rep | Tumor tissue classification | Combination of InceptionResNet.v2 with PCA and Wavelet transform | 5-class: ADC, high-grade adenoma with dysplasia, low-grade adenoma with dysplasia, carcinoid, hyperplastic polyp | Yeouido St. Mary’s Hospital 390 WSIs | Dice: 0.804 ± 0.125 ACC: 0.957 ± 0.025 Jac: 0.690 ± 0.174 | |
| Tsuneki [62] | Diagnostics | Tumor tissue classification | The authors use the EfficientNetB1 model starting with pre-trained weights on ImageNet | 4-class: poorly differentiated ADC, well-to-moderately ADC, adenoma, non-neoplastic) | 1.799 H/E WSIs | AUC 0.95 | |
| Bustos [106] | Biomolecules | Tumor tissue classification/MSI prediction | Resnet-34 pre-trained on ImageNet | (A) 9-class: adipose, background, debris, lymphocytes, mucus, smooth muscle, normal colon epithelium, cancer-associated stroma, colorectal ADC epithelium (B) Binary (MSI-H/MSS) | 72 TMAs | (A) Validation test: AUC 0.98 (B) MSI AUC 0.87 ± 0.03 | |
| Bilal [78] | Lancet Digit Health | Prediction of molecular pathways and mutations | 2 × pre-trained models (1) ResNet-18, (2) adaptive ResNet-34 | Binary: (1) High/low mutation density (2) MSI/MSS (3) Chromosomal instability (CIN)/Genomic stability (4) CIMP-high/CIMP-low (5) BRAFmut/BRAFWT (6) TP53mut/TP53WT (7) KRASmut/KRASWT | TCGA (502 slides) Pathology Artificial Intelligence Platform (PAIP) challenge—47 slides (12 microsatellite instable and 35 microsatellite stable) | Mean AUROC Hypermutation: (0.81 [SD 0.03] vs. 0.71), MSI (0.86 [0.04] vs. 0.74), CIN (0.83 [0.02] vs. 0.73), BRAF mutation (0.79 [0.01] vs. 0.66), TP53mut (0.73 [0.02] vs. 0.64), KRAS mutation (0.60 [SD 0.04] vs. 0.60), CIMP-high status 0.79 (SD 0.05) | |
| Nguyen [42] | Sci Rep | Diagnosis | Same approach with Nquyen et al., 2021, presented in Mod Pathol | 3-class: Tumor/Normal/Other tissue | 54 TMA slides | SVEVC: Tumor: Recall:0.938, Precision:0.976, F1-score: 0.957, ACC: 0.939 Normal: Recall: 0.864, Precision: 0.873, F1-score: 0.915, ACC: 0.982 Other tissue: Recall: 0.964, Precision: 0.772, F1-score: 0.858, ACC: 0.947 Overall (average): Recall: 0.922, Precision: 0.907, F1-score: 0.910, ACC: 0.956 | |
| Shen [46] | IEEE/ACM Trans Comput Biol Bioinform | Diagnosis | A DenseNet based architecture of CNN, in an overall framework which employs a Monte Carlo adaptively sampling to localize patches | 3-class: loose non-tumor tissue/dense non-tumor tissue/gastrointestinal cancer tissues | (i) TCGA-STAD 432 samples (ii) TCGA-COAD 460 samples (iii) TCGA-READ 171 samples | DP-FTD: AUC 0.779, FROC 0.817 DCRF-FTD: AUC 0.786, FROC 0.821 | |
| 2022 | Schrammen [79] | J Pathol | Diagnosis/Prediction of IHC biomarkers | Novel method called Slide-Level Assessment Model (SLAM), uses an end-to-end neural network based on ShuffleNet | 3-class: Positive tumor slides, Negative tumor slides, Non-tumor slides (A) Binary: BRAF status (mutated or non-mutated) (B) Binary (MSI/MMR) (C) Binary: High grade (grade 3–4)/Low grade (grade 1–2) | (A) Darmkrebs: Chancen der Verhütung durch Screening (DACHS) 2.448 H/E slides B) Yorkshire Cancer Research Bowel Cancer Improvement Program (YCR-BCIP) 889 H/E slides | DACHS cohort Tumor detection AUROC: 0.980 Tumor grading AUROC: 0.751 MSI/MMRD or MSS/MMRP AUROC: 0.909 BRAF status detection AUROC: 0.821 YCR-BCIP cohort MSI/MMRD status detection AUROC: 0.900 |
| Hosseinzadeh Kassani [43] | Int J Med Inform | Diagnosis | A comparative study between popular architectures (ResNet, VGG, MobileNet, Inceptionv3, InceptionResnetv2, ResNeXt, SE-ResNet, SE-ResNeXt) | Binary (Cancerous/Healthy regions) | DigestPath, 250 H/E WSIs, 1.746 patches | Dice: 82.74% ± 1.77 ACC: 87.07% ± 1.56 F1 score: 82.79% ± 1.79 | |
| Deshpande [116] | Med Image Anal | Diagnosis | Novel GAN architecture, called SAFRON, including loss function which enables generation of images of arbitrarily large sizes after training on relatively small image patches | Binary (benign/malignant) | (A) CRAG (Graham et al., 2019, Awan et al., 2017) 213 colorectal tissue images (B) DigestPath 46 images | ResNet model median classification ACC: 97% with generated images added to the Baseline set, and 93% without |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Douaiher, J.; Ravipati, A.; Grams, B.; Chowdhury, S.; Alatise, O.; Are, C. Colorectal Cancer-Global Burden, Trends, and Geographical Variations. J. Surg. Oncol. 2017, 115, 619–630. [Google Scholar] [CrossRef] [PubMed]
- Sawicki, T.; Ruszkowska, M.; Danielewicz, A.; Niedźwiedzka, E.; Arłukowicz, T.; Przybyłowicz, K.E. A Review of Colorectal Cancer in Terms of Epidemiology, Risk Factors, Development, Symptoms and Diagnosis. Cancers 2021, 13, 2025. [Google Scholar] [CrossRef] [PubMed]
- Müller, M.F.; Ibrahim, A.E.K.; Arends, M.J. Molecular Pathological Classification of Colorectal Cancer. Virchows Arch. 2016, 469, 125–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marzouk, O.; Schofield, J. Review of Histopathological and Molecular Prognostic Features in Colorectal Cancer. Cancers 2011, 3, 2767–2810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jass, J.R. Classification of Colorectal Cancer Based on Correlation of Clinical, Morphological and Molecular Features. Histopathology 2007, 50, 113–130. [Google Scholar] [CrossRef] [PubMed]
- Sideris, M.; Papagrigoriadis, S. Molecular Biomarkers and Classification Models in the Evaluation of the Prognosis of Colorectal Cancer. Anticancer Res. 2014, 34, 2061–2068. [Google Scholar] [PubMed]
- Pallag, A.; Roşca, E.; Ţiţ, D.M.; Muţiu, G.; Bungău, S.G.; Pop, O.L. Monitoring the Effects of Treatment in Colon Cancer Cells Using Immunohistochemical and Histoenzymatic Techniques. Rom. J. Morphol. Embryol. 2015, 56, 1103–1109. [Google Scholar] [PubMed]
- Vogel, J.D.; Eskicioglu, C.; Weiser, M.R.; Feingold, D.L.; Steele, S.R. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Treatment of Colon Cancer. Dis. Colon Rectum 2017, 60, 999–1017. [Google Scholar] [CrossRef] [PubMed]
- Kelly, M.; Soles, R.; Garcia, E.; Kundu, I. Job Stress, Burnout, Work-Life Balance, Well-Being, and Job Satisfaction among Pathology Residents and Fellows. Am. J. Clin. Pathol. 2020, 153, 449–469. [Google Scholar] [CrossRef] [PubMed]
- Pena, G.P.; Andrade-Filho, J.S. How Does a Pathologist Make a Diagnosis? Arch. Pathol. Lab. Med. 2009, 133, 124–132. [Google Scholar] [CrossRef] [PubMed]
- van Putten, P.G.; Hol, L.; van Dekken, H.; Han van Krieken, J.; van Ballegooijen, M.; Kuipers, E.J.; van Leerdam, M.E. Inter-Observer Variation in the Histological Diagnosis of Polyps in Colorectal Cancer Screening. Histopathology 2011, 58, 974–981. [Google Scholar] [CrossRef] [Green Version]
- Smits, L.J.H.; Vink-Börger, E.; Lijnschoten, G.; Focke-Snieders, I.; Post, R.S.; Tuynman, J.B.; Grieken, N.C.T.; Nagtegaal, I.D. Diagnostic Variability in the Histopathological Assessment of Advanced Colorectal Adenomas and Early Colorectal Cancer in a Screening Population. Histopathology 2022, 80, 790–798. [Google Scholar] [CrossRef]
- Huang, S.; Yang, J.; Fong, S.; Zhao, Q. Artificial Intelligence in Cancer Diagnosis and Prognosis: Opportunities and Challenges. Cancer Lett. 2020, 471, 61–71. [Google Scholar] [CrossRef] [PubMed]
- Thakur, N.; Yoon, H.; Chong, Y. Current Trends of Artificial Intelligence for Colorectal Cancer Pathology Image Analysis: A Systematic Review. Cancers 2020, 12, 1884. [Google Scholar] [CrossRef] [PubMed]
- WHO Classification of Tumours Editorial Board. WHO Classification of Tumors: Digestive System Tumours, 5th ed.; International Agency for Research on Cancer: Lyon, France, 2019; ISBN 978-92-832-4499-8. [Google Scholar]
- Vilar, E.; Gruber, S.B. Microsatellite Instability in Colorectal Cancer—the Stable Evidence. Nat. Rev. Clin. Oncol. 2010, 7, 153–162. [Google Scholar] [CrossRef] [Green Version]
- Nojadeh, J.N.; Behrouz Sharif, S.; Sakhinia, E. Microsatellite Instability in Colorectal Cancer. EXCLI J. 2018, 17, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Tamura, K.; Kaneda, M.; Futagawa, M.; Takeshita, M.; Kim, S.; Nakama, M.; Kawashita, N.; Tatsumi-Miyajima, J. Genetic and Genomic Basis of the Mismatch Repair System Involved in Lynch Syndrome. Int. J. Clin. Oncol. 2019, 24, 999–1011. [Google Scholar] [CrossRef] [PubMed]
- Boland, C.R.; Goel, A. Microsatellite Instability in Colorectal Cancer. Gastroenterology 2010, 138, 2073–2087.e3. [Google Scholar] [CrossRef]
- Kang, S.; Na, Y.; Joung, S.Y.; Lee, S.I.; Oh, S.C.; Min, B.W. The Significance of Microsatellite Instability in Colorectal Cancer after Controlling for Clinicopathological Factors. Medicine 2018, 97, e0019. [Google Scholar] [CrossRef]
- Arjmand, A.; Tsipouras, M.G.; Tzallas, A.T.; Forlano, R.; Manousou, P.; Giannakeas, N. Quantification of Liver Fibrosis—A Comparative Study. Appl. Sci. 2020, 10, 447. [Google Scholar] [CrossRef] [Green Version]
- Aeffner, F.; Zarella, M.; Buchbinder, N.; Bui, M.; Goodman, M.; Hartman, D.; Lujan, G.; Molani, M.; Parwani, A.; Lillard, K.; et al. Introduction to Digital Image Analysis in Whole-Slide Imaging: A White Paper from the Digital Pathology Association. J. Pathol. Inform. 2019, 10, 9. [Google Scholar] [CrossRef]
- Patel, A.; Balis, U.G.J.; Cheng, J.; Li, Z.; Lujan, G.; McClintock, D.S.; Pantanowitz, L.; Parwani, A. Contemporary Whole Slide Imaging Devices and Their Applications within the Modern Pathology Department: A Selected Hardware Review. J. Pathol. Inform. 2021, 12, 50. [Google Scholar] [CrossRef] [PubMed]
- Jirik, M.; Gruber, I.; Moulisova, V.; Schindler, C.; Cervenkova, L.; Palek, R.; Rosendorf, J.; Arlt, J.; Bolek, L.; Dejmek, J.; et al. Semantic Segmentation of Intralobular and Extralobular Tissue from Liver Scaffold H&E Images. Sensors 2020, 20, 7063. [Google Scholar] [CrossRef]
- Shapcott, M.; Hewitt, K.J.; Rajpoot, N. Deep Learning With Sampling in Colon Cancer Histology. Front. Bioeng. Biotechnol. 2019, 7, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deng, J.; Dong, W.; Socher, R.; Li, L.-J.; Li, K.; Fei-Fei, L. ImageNet: A large-scale hierarchical image database. In Proceedings of the 2009 IEEE Conference on Computer Vision and Pattern Recognition, Miami, FL, USA, 20–25 June 2009; Volume 7, pp. 248–255. [Google Scholar]
- Graupe, D. Principles of Artificial Neural Networks, Advanced Series in Circuits and Systems; World Scientific: London, UK, 2013; Volume 7. [Google Scholar]
- Liu, Y.; Gadepalli, K.; Norouzi, M.; Dahl, G.E.; Kohlberger, T.; Boyko, A.; Venugopalan, S.; Timofeev, A.; Nelson, P.Q.; Corrado, G.S.; et al. Detecting Cancer Metastases on Gigapixel Pathology Images. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017. [Google Scholar]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. ImageNet Classification with Deep Convolutional Neural Networks. Commun. ACM 2017, 60, 84–90. [Google Scholar] [CrossRef]
- Szegedy, C.; Liu, W.; Jia, Y.; Sermanet, P.; Reed, S.; Anguelov, D.; Erhan, D.; Vanhoucke, V.; Rabinovich, A. Going Deeper with Convolutions. In Proceedings of the 2015 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), IEEE, Boston, MA, USA, 7–12 June 2015; pp. 1–9. [Google Scholar] [CrossRef] [Green Version]
- Simonyan, K.; Zisserman, A. Very Deep Convolutional Networks for Large-Scale Image Recognition. In Proceedings of the 3rd International Conference on Learning Representations, Conference Track Proceedings, San Diego, CA, USA, 7–9 May 2015. [Google Scholar] [CrossRef]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely Connected Convolutional Networks. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; pp. 2261–2269. [Google Scholar] [CrossRef] [Green Version]
- Goodfellow, I.J.; Pouget-Abadie, J.; Mirza, M.; Xu, B.; Warde-Farley, D.; Ozair, S.; Courville, A.; Bengio, Y. Generative Adversarial Networks. Commun. ACM 2020, 63, 139–144. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.; Huang, Y.; Sahoo, P.K.; You, J.F.; Chiang, S.F.; Onthoni, D.D.; Chern, Y.J.; Chao, K.Y.; Chiang, J.M.; Yeh, C.Y.; et al. Colon Tissues Classification and Localization in Whole Slide Images Using Deep Learning. Diagnostics 2021, 11, 1398. [Google Scholar] [CrossRef]
- Zhou, C.; Jin, Y.; Chen, Y.; Huang, S.; Huang, R.; Wang, Y.; Zhao, Y.; Chen, Y.; Guo, L.; Liao, J. Histopathology Classification and Localization of Colorectal Cancer Using Global Labels by Weakly Supervised Deep Learning. Comput. Med. Imaging Graph. 2021, 88, 101861. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.; Lee, J.; Oh, J.E.; Kim, H.R.; Lee, S.; Chang, H.J.; Sohn, D.K. Tumor Identification in Colorectal Histology Images Using a Convolutional Neural Network. J. Digit. Imaging 2019, 32, 131–140. [Google Scholar] [CrossRef]
- Xu, L.; Walker, B.; Liang, P.-I.; Tong, Y.; Xu, C.; Su, Y.; Karsan, A. Colorectal Cancer Detection Based on Deep Learning. J. Pathol. Inform. 2020, 11, 28. [Google Scholar] [CrossRef] [PubMed]
- Mittal, P.; Condina, M.R.; Klingler-Hoffmann, M.; Kaur, G.; Oehler, M.K.; Sieber, O.M.; Palmieri, M.; Kommoss, S.; Brucker, S.; McDonnell, M.D.; et al. Cancer Tissue Classification Using Supervised Machine Learning Applied to Maldi Mass Spectrometry Imaging. Cancers 2021, 13, 5388. [Google Scholar] [CrossRef] [PubMed]
- Jia, Z.; Huang, X.; Chang, E.I.C.; Xu, Y. Constrained Deep Weak Supervision for Histopathology Image Segmentation. IEEE Trans. Med. Imaging 2017, 36, 2376–2388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, H.-G.; Blank, A.; Dawson, H.E.; Lugli, A.; Zlobec, I. Classification of Colorectal Tissue Images from High Throughput Tissue Microarrays by Ensemble Deep Learning Methods. Sci. Rep. 2021, 11, 2371. [Google Scholar] [CrossRef]
- Hosseinzadeh Kassani, S.; Hosseinzadeh Kassani, P.; Wesolowski, M.J.; Schneider, K.A.; Deters, R. Deep Transfer Learning Based Model for Colorectal Cancer Histopathology Segmentation: A Comparative Study of Deep Pre-Trained Models. Int. J. Med. Inform. 2022, 159, 104669. [Google Scholar] [CrossRef] [PubMed]
- Qaiser, T.; Tsang, Y.-W.; Taniyama, D.; Sakamoto, N.; Nakane, K.; Epstein, D.; Rajpoot, N. Fast and Accurate Tumor Segmentation of Histology Images Using Persistent Homology and Deep Convolutional Features. Med. Image Anal. 2019, 55, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, K.S.; Yu, G.; Xu, C.; Meng, X.H.; Zhou, J.; Zheng, C.; Deng, Z.; Shang, L.; Liu, R.; Su, S.; et al. Accurate Diagnosis of Colorectal Cancer Based on Histopathology Images Using Artificial Intelligence. BMC Med. 2021, 19, 76. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Ke, J. Sampling Based Tumor Recognition in Whole-Slide Histology Image with Deep Learning Approaches. IEEE/ACM Trans. Comput. Biol. Bioinform. 2021, 14, 1. [Google Scholar] [CrossRef]
- Yu, G.; Sun, K.; Xu, C.; Shi, X.-H.; Wu, C.; Xie, T.; Meng, R.-Q.; Meng, X.-H.; Wang, K.-S.; Xiao, H.-M.; et al. Accurate Recognition of Colorectal Cancer with Semi-Supervised Deep Learning on Pathological Images. Nat. Commun. 2021, 12, 6311. [Google Scholar] [CrossRef]
- Toğaçar, M. Disease Type Detection in Lung and Colon Cancer Images Using the Complement Approach of Inefficient Sets. Comput. Biol. Med. 2021, 137, 104827. [Google Scholar] [CrossRef]
- Masud, M.; Sikder, N.; Nahid, A.-A.; Bairagi, A.K.; AlZain, M.A. A Machine Learning Approach to Diagnosing Lung and Colon Cancer Using a Deep Learning-Based Classification Framework. Sensors 2021, 21, 748. [Google Scholar] [CrossRef] [PubMed]
- Song, Z.; Yu, C.; Zou, S.; Wang, W.; Huang, Y.; Ding, X.; Liu, J.; Shao, L.; Yuan, J.; Gou, X.; et al. Automatic Deep Learning-Based Colorectal Adenoma Detection System and Its Similarities with Pathologists. BMJ Open 2020, 10, e036423. [Google Scholar] [CrossRef]
- Terradillos, E.; Saratxaga, C.; Mattana, S.; Cicchi, R.; Pavone, F.; Andraka, N.; Glover, B.; Arbide, N.; Velasco, J.; Etxezarraga, M.; et al. Analysis on the Characterization of Multiphoton Microscopy Images for Malignant Neoplastic Colon Lesion Detection under Deep Learning Methods. J. Pathol. Inform. 2021, 12, 27. [Google Scholar] [CrossRef]
- Holland, L.; Wei, D.; Olson, K.; Mitra, A.; Graff, J.; Jones, A.; Durbin-Johnson, B.; Mitra, A.; Rashidi, H. Limited Number of Cases May Yield Generalizable Models, a Proof of Concept in Deep Learning for Colon Histology. J. Pathol. Inform. 2020, 11, 5. [Google Scholar] [CrossRef] [PubMed]
- Iizuka, O.; Kanavati, F.; Kato, K.; Rambeau, M.; Arihiro, K.; Tsuneki, M. Deep Learning Models for Histopathological Classification of Gastric and Colonic Epithelial Tumours. Sci. Rep. 2020, 10, 1504. [Google Scholar] [CrossRef] [Green Version]
- Haj-Hassan, H.; Chaddad, A.; Harkouss, Y.; Desrosiers, C.; Toews, M.; Tanougast, C. Classifications of Multispectral Colorectal Cancer Tissues Using Convolution Neural Network. J. Pathol. Inform. 2017, 8, 1. [Google Scholar] [CrossRef]
- Sena, P.; Fioresi, R.; Faglioni, F.; Losi, L.; Faglioni, G.; Roncucci, L. Deep Learning Techniques for Detecting Preneoplastic and Neoplastic Lesions in Human Colorectal Histological Images. Oncol. Lett. 2019, 18, 6101–6107. [Google Scholar] [CrossRef] [Green Version]
- Rączkowski, Ł.; Możejko, M.; Zambonelli, J.; Szczurek, E. ARA: Accurate, Reliable and Active Histopathological Image Classification Framework with Bayesian Deep Learning. Sci. Rep. 2019, 9, 14347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, Y.; Jia, Z.; Wang, L.B.; Ai, Y.; Zhang, F.; Lai, M.; Chang, E.I.C. Large Scale Tissue Histopathology Image Classification, Segmentation, and Visualization via Deep Convolutional Activation Features. BMC Bioinform. 2017, 18, 281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.; Shi, J.; Zhang, Q.; Ying, S. Histopathological Image Classification with Bilinear Convolutional Neural Networks. Proc. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. EMBS 2017, 2017, 4050–4053. [Google Scholar] [CrossRef]
- Paladini, E.; Vantaggiato, E.; Bougourzi, F.; Distante, C.; Hadid, A.; Taleb-Ahmed, A. Two Ensemble-CNN Approaches for Colorectal Cancer Tissue Type Classification. J. Imaging 2021, 7, 51. [Google Scholar] [CrossRef]
- Jiao, Y.; Yuan, J.; Qiang, Y.; Fei, S. Deep Embeddings and Logistic Regression for Rapid Active Learning in Histopathological Images. Comput. Methods Programs Biomed. 2021, 212, 106464. [Google Scholar] [CrossRef] [PubMed]
- Ben Hamida, A.; Devanne, M.; Weber, J.; Truntzer, C.; Derangère, V.; Ghiringhelli, F.; Forestier, G.; Wemmert, C. Deep Learning for Colon Cancer Histopathological Images Analysis. Comput. Biol. Med. 2021, 136, 104730. [Google Scholar] [CrossRef] [PubMed]
- Tsuneki, M.; Kanavati, F. Deep Learning Models for Poorly Differentiated Colorectal Adenocarcinoma Classification in Whole Slide Images Using Transfer Learning. Diagnostics 2021, 11, 2074. [Google Scholar] [CrossRef]
- Xu, Y.; Li, Y.; Wang, Y.; Liu, M.; Fan, Y.; Lai, M.; Chang, E.I.C. Gland Instance Segmentation Using Deep Multichannel Neural Networks. IEEE Trans. Biomed. Eng. 2017, 64, 2901–2912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graham, S.; Chen, H.; Gamper, J.; Dou, Q.; Heng, P.A.; Snead, D.; Tsang, Y.W.; Rajpoot, N. MILD-Net: Minimal Information Loss Dilated Network for Gland Instance Segmentation in Colon Histology Images. Med. Image Anal. 2019, 52, 199–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kainz, P.; Pfeiffer, M.; Urschler, M. Segmentation and Classification of Colon Glands with Deep Convolutional Neural Networks and Total Variation Regularization. PeerJ 2017, 2017, e3874. [Google Scholar] [CrossRef]
- Van Eycke, Y.R.; Balsat, C.; Verset, L.; Debeir, O.; Salmon, I.; Decaestecker, C. Segmentation of Glandular Epithelium in Colorectal Tumours to Automatically Compartmentalise IHC Biomarker Quantification: A Deep Learning Approach. Med. Image Anal. 2018, 49, 35–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Awan, R.; Sirinukunwattana, K.; Epstein, D.; Jefferyes, S.; Qidwai, U.; Aftab, Z.; Mujeeb, I.; Snead, D.; Rajpoot, N. Glandular Morphometrics for Objective Grading of Colorectal Adenocarcinoma Histology Images. Sci. Rep. 2017, 7, 2220–2243. [Google Scholar] [CrossRef] [PubMed]
- Shaban, M.; Awan, R.; Fraz, M.M.; Azam, A.; Tsang, Y.W.; Snead, D.; Rajpoot, N.M. Context-Aware Convolutional Neural Network for Grading of Colorectal Cancer Histology Images. IEEE Trans. Med. Imaging 2020, 39, 2395–2405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sari, C.T.; Gunduz-Demir, C. Unsupervised Feature Extraction via Deep Learning for Histopathological Classification of Colon Tissue Images. IEEE Trans. Med. Imaging 2019, 38, 1139–1149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiao, Y.; Li, J.; Qian, C.; Fei, S. Deep Learning-Based Tumor Microenvironment Analysis in Colon Adenocarcinoma Histopathological Whole-Slide Images. Comput. Methods Programs Biomed. 2021, 204, 106047. [Google Scholar] [CrossRef] [PubMed]
- Pham, T.D. Time-Frequency Time-Space Long Short-Term Memory Networks for Image Classification of Histopathological Tissue. Sci. Rep. 2021, 11, 13703. [Google Scholar] [CrossRef] [PubMed]
- Pai, R.K.; Hartman, D.; Schaeffer, D.F.; Rosty, C.; Shivji, S.; Kirsch, R.; Pai, R.K. Development and Initial Validation of a Deep Learning Algorithm to Quantify Histological Features in Colorectal Carcinoma Including Tumour Budding/Poorly Differentiated Clusters. Histopathology 2021, 79, 391–405. [Google Scholar] [CrossRef] [PubMed]
- Nearchou, I.P.; Ueno, H.; Kajiwara, Y.; Lillard, K.; Mochizuki, S.; Takeuchi, K.; Harrison, D.J.; Caie, P.D. Automated Detection and Classification of Desmoplastic Reaction at the Colorectal Tumour Front Using Deep Learning. Cancers 2021, 13, 1615. [Google Scholar] [CrossRef] [PubMed]
- Bian, C.; Wang, Y.; Lu, Z.; An, Y.; Wang, H.; Kong, L.; Du, Y.; Tian, J. Immunoaizer: A Deep Learning-based Computational Framework to Characterize Cell Distribution and Gene Mutation in Tumor Microenvironment. Cancers 2021, 13, 1659. [Google Scholar] [CrossRef] [PubMed]
- Swiderska-Chadaj, Z.; Pinckaers, H.; van Rijthoven, M.; Balkenhol, M.; Melnikova, M.; Geessink, O.; Manson, Q.; Sherman, M.; Polonia, A.; Parry, J.; et al. Learning to Detect Lymphocytes in Immunohistochemistry with Deep Learning. Med. Image Anal. 2019, 58, 101547. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Li, Y.; Wang, Y.; Zhang, S.; Huang, Y.; Yao, S.; Han, C.; Pan, X.; Shi, Z.; Mao, Y.; et al. A Deep Learning Quantified Stroma-Immune Score to Predict Survival of Patients with Stage II–III Colorectal Cancer. Cancer Cell Int. 2021, 21, 585. [Google Scholar] [CrossRef]
- Jang, H.J.; Lee, A.; Kang, J.; Song, I.H.; Lee, S.H. Prediction of Clinically Actionable Genetic Alterations from Colorectal Cancer Histopathology Images Using Deep Learning. World J. Gastroenterol. 2020, 26, 6207–6223. [Google Scholar] [CrossRef]
- Bilal, M.; Raza, S.E.A.; Azam, A.; Graham, S.; Ilyas, M.; Cree, I.A.; Snead, D.; Minhas, F.; Rajpoot, N.M. Development and Validation of a Weakly Supervised Deep Learning Framework to Predict the Status of Molecular Pathways and Key Mutations in Colorectal Cancer from Routine Histology Images: A Retrospective Study. Lancet Digit. Health 2021, 3, e763–e772. [Google Scholar] [CrossRef]
- Schrammen, P.L.; Ghaffari Laleh, N.; Echle, A.; Truhn, D.; Schulz, V.; Brinker, T.J.; Brenner, H.; Chang-Claude, J.; Alwers, E.; Brobeil, A.; et al. Weakly Supervised Annotation-Free Cancer Detection and Prediction of Genotype in Routine Histopathology. J. Pathol. 2022, 256, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Popovici, V.; Budinská, E.; Dušek, L.; Kozubek, M.; Bosman, F. Image-Based Surrogate Biomarkers for Molecular Subtypes of Colorectal Cancer. Bioinformatics 2017, 33, 2002–2009. [Google Scholar] [CrossRef] [Green Version]
- Xu, J.; Luo, X.; Wang, G.; Gilmore, H.; Madabhushi, A. A Deep Convolutional Neural Network for Segmenting and Classifying Epithelial and Stromal Regions in Histopathological Images. Neurocomputing 2016, 191, 214–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarker, M.M.K.; Makhlouf, Y.; Craig, S.G.; Humphries, M.P.; Loughrey, M.; James, J.A.; Salto-tellez, M.; O’Reilly, P.; Maxwell, P. A Means of Assessing Deep Learning-based Detection of ICOS Protein Expression in Colon Cancer. Cancers 2021, 13, 3825. [Google Scholar] [CrossRef] [PubMed]
- Weis, C.A.; Kather, J.N.; Melchers, S.; Al-ahmdi, H.; Pollheimer, M.J.; Langner, C.; Gaiser, T. Automatic Evaluation of Tumor Budding in Immunohistochemically Stained Colorectal Carcinomas and Correlation to Clinical Outcome. Diagn. Pathol. 2018, 13, 64. [Google Scholar] [CrossRef] [PubMed]
- Sirinukunwattana, K.; Raza, S.E.A.; Tsang, Y.W.; Snead, D.R.J.; Cree, I.A.; Rajpoot, N.M. Locality Sensitive Deep Learning for Detection and Classification of Nuclei in Routine Colon Cancer Histology Images. IEEE Trans. Med. Imaging 2016, 35, 1196–1206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Höfener, H.; Homeyer, A.; Weiss, N.; Molin, J.; Lundström, C.F.; Hahn, H.K. Deep Learning Nuclei Detection: A Simple Approach Can Deliver State-of-the-Art Results. Comput. Med. Imaging Graph. 2018, 70, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Graham, S.; Vu, Q.D.; Raza, S.E.A.; Azam, A.; Tsang, Y.W.; Kwak, J.T.; Rajpoot, N. Hover-Net: Simultaneous Segmentation and Classification of Nuclei in Multi-Tissue Histology Images. Med. Image Anal. 2019, 58, 101563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.; Qi, X.; Yu, L.; Dou, Q.; Qin, J.; Heng, P.A. DCAN: Deep Contour-Aware Networks for Object Instance Segmentation from Histology Images. Med. Image Anal. 2017, 36, 135–146. [Google Scholar] [CrossRef]
- Kwak, M.S.; Lee, H.H.; Yang, J.M.; Cha, J.M.; Jeon, J.W.; Yoon, J.Y.; Kim, H.I. Deep Convolutional Neural Network-Based Lymph Node Metastasis Prediction for Colon Cancer Using Histopathological Images. Front. Oncol. 2021, 10, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kiehl, L.; Kuntz, S.; Höhn, J.; Jutzi, T.; Krieghoff-Henning, E.; Kather, J.N.; Holland-Letz, T.; Kopp-Schneider, A.; Chang-Claude, J.; Brobeil, A.; et al. Deep Learning Can Predict Lymph Node Status Directly from Histology in Colorectal Cancer. Eur. J. Cancer 2021, 157, 464–473. [Google Scholar] [CrossRef] [PubMed]
- Brockmoeller, S.; Echle, A.; Ghaffari Laleh, N.; Eiholm, S.; Malmstrøm, M.L.; Plato Kuhlmann, T.; Levic, K.; Grabsch, H.I.; West, N.P.; Saldanha, O.L.; et al. Deep Learning Identifies Inflamed Fat as a Risk Factor for Lymph Node Metastasis in Early Colorectal Cancer. J. Pathol. 2022, 256, 269–281. [Google Scholar] [CrossRef] [PubMed]
- Chuang, W.Y.; Chen, C.C.; Yu, W.H.; Yeh, C.J.; Chang, S.H.; Ueng, S.H.; Wang, T.H.; Hsueh, C.; Kuo, C.F.; Yeh, C.Y. Identification of Nodal Micrometastasis in Colorectal Cancer Using Deep Learning on Annotation-Free Whole-Slide Images. Mod. Pathol. 2021, 34, 1901–1911. [Google Scholar] [CrossRef]
- Bychkov, D.; Linder, N.; Turkki, R.; Nordling, S.; Kovanen, P.E.; Verrill, C.; Walliander, M.; Lundin, M.; Haglund, C.; Lundin, J. Deep Learning Based Tissue Analysis Predicts Outcome in Colorectal Cancer. Sci. Rep. 2018, 8, 3395. [Google Scholar] [CrossRef] [PubMed]
- Skrede, O.J.; De Raedt, S.; Kleppe, A.; Hveem, T.S.; Liestøl, K.; Maddison, J.; Askautrud, H.A.; Pradhan, M.; Nesheim, J.A.; Albregtsen, F.; et al. Deep Learning for Prediction of Colorectal Cancer Outcome: A Discovery and Validation Study. Lancet 2020, 395, 350–360. [Google Scholar] [CrossRef]
- Wulczyn, E.; Steiner, D.F.; Moran, M.; Plass, M.; Reihs, R.; Tan, F.; Flament-Auvigne, I.; Brown, T.; Regitnig, P.; Chen, P.H.C.; et al. Interpretable Survival Prediction for Colorectal Cancer Using Deep Learning. Npj Digit. Med. 2021, 4, 71. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Yao, S.; Li, Z.; Wu, L.; Xu, Z.; Pan, X.; Lin, H.; Xu, Y.; Yang, S.; Zhang, S.; et al. The Crohn’s-like Lymphoid Reaction Density: A New Artificial Intelligence Quantified Prognostic Immune Index in Colon Cancer. Cancer Immunol. Immunother. 2021. [Google Scholar] [CrossRef] [PubMed]
- Jones, H.J.S.; Cunningham, C.; Askautrud, H.A.; Danielsen, H.E.; Kerr, D.J.; Domingo, E.; Maughan, T.; Leedham, S.J.; Koelzer, V.H. Stromal Composition Predicts Recurrence of Early Rectal Cancer after Local Excision. Histopathology 2021, 79, 947–956. [Google Scholar] [CrossRef]
- Geessink, O.G.F.; Baidoshvili, A.; Klaase, J.M.; Ehteshami Bejnordi, B.; Litjens, G.J.S.; van Pelt, G.W.; Mesker, W.E.; Nagtegaal, I.D.; Ciompi, F.; van der Laak, J.A.W.M. Computer Aided Quantification of Intratumoral Stroma Yields an Independent Prognosticator in Rectal Cancer. Cell. Oncol. 2019, 42, 331–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, K.; Li, Z.; Yao, S.; Wang, Y.; Wu, X.; Xu, Z.; Wu, L.; Huang, Y.; Liang, C.; Liu, Z. Artificial Intelligence Quantified Tumour-Stroma Ratio Is an Independent Predictor for Overall Survival in Resectable Colorectal Cancer. EBioMedicine 2020, 61, 103054. [Google Scholar] [CrossRef]
- Kather, J.N.; Krisam, J.; Charoentong, P.; Luedde, T.; Herpel, E.; Weis, C.A.; Gaiser, T.; Marx, A.; Valous, N.A.; Ferber, D.; et al. Predicting Survival from Colorectal Cancer Histology Slides Using Deep Learning: A Retrospective Multicenter Study. PLoS Med. 2019, 16, e1002730. [Google Scholar] [CrossRef] [PubMed]
- Schiele, S.; Arndt, T.T.; Martin, B.; Miller, S.; Bauer, S.; Banner, B.M.; Brendel, E.M.; Schenkirsch, G.; Anthuber, M.; Huss, R.; et al. Deep Learning Prediction of Metastasis in Locally Advanced Colon Cancer Using Binary Histologic Tumor Images. Cancers 2021, 13, 2074. [Google Scholar] [CrossRef]
- Theodosi, A.; Ouzounis, S.; Kostopoulos, S.; Glotsos, D.; Kalatzis, I.; Asvestas, P.; Tzelepi, V.; Ravazoula, P.; Cavouras, D.; Sakellaropoulos, G. Employing Machine Learning and Microscopy Images of AIB1-Stained Biopsy Material to Assess the 5-Year Survival of Patients with Colorectal Cancer. Microsc. Res. Tech. 2021, 84, 2421–2433. [Google Scholar] [CrossRef] [PubMed]
- Echle, A.; Grabsch, H.I.; Quirke, P.; van den Brandt, P.A.; West, N.P.; Hutchins, G.G.A.; Heij, L.R.; Tan, X.; Richman, S.D.; Krause, J.; et al. Clinical-Grade Detection of Microsatellite Instability in Colorectal Tumors by Deep Learning. Gastroenterology 2020, 159, 1406–1416.e11. [Google Scholar] [CrossRef] [PubMed]
- Cao, R.; Yang, F.; Ma, S.C.; Liu, L.; Zhao, Y.; Li, Y.; Wu, D.H.; Wang, T.; Lu, W.J.; Cai, W.J.; et al. Development and Interpretation of a Pathomics-Based Model for the Prediction of Microsatellite Instability in Colorectal Cancer. Theranostics 2020, 10, 11080–11091. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, R.; Long, J.; Longacre, T.; Peng, L.; Berry, G.; Martin, B.; Higgins, J.; Rubin, D.L.; Shen, J. Deep Learning Model for the Prediction of Microsatellite Instability in Colorectal Cancer: A Diagnostic Study. Lancet Oncol. 2021, 22, 132–141. [Google Scholar] [CrossRef]
- Wang, Y.; Coudray, N.; Zhao, Y.; Li, F.; Hu, C.; Zhang, Y.-Z.; Imoto, S.; Tsirigos, A.; Webb, G.I.; Daly, R.J.; et al. HEAL: An Automated Deep Learning Framework for Cancer Histopathology Image Analysis. Bioinformatics 2021, 37, 4291–4295. [Google Scholar] [CrossRef] [PubMed]
- Bustos, A.; Payá, A.; Torrubia, A.; Jover, R.; Llor, X.; Bessa, X.; Castells, A.; Carracedo, Á.; Alenda, C. XDEEP-MSI: Explainable Bias-Rejecting Microsatellite Instability Deep Learning System in Colorectal Cancer. Biomolecules 2021, 11, 1786. [Google Scholar] [CrossRef]
- Lee, S.H.; Song, I.H.; Jang, H.J. Feasibility of Deep Learning-Based Fully Automated Classification of Microsatellite Instability in Tissue Slides of Colorectal Cancer. Int. J. Cancer 2021, 149, 728–740. [Google Scholar] [CrossRef]
- Krause, J.; Grabsch, H.I.; Kloor, M.; Jendrusch, M.; Echle, A.; Buelow, R.D.; Boor, P.; Luedde, T.; Brinker, T.J.; Trautwein, C.; et al. Deep Learning Detects Genetic Alterations in Cancer Histology Generated by Adversarial Networks. J. Pathol. 2021, 254, 70–79. [Google Scholar] [CrossRef] [PubMed]
- Sirinukunwattana, K.; Domingo, E.; Richman, S.D.; Redmond, K.L.; Blake, A.; Verrill, C.; Leedham, S.J.; Chatzipli, A.; Hardy, C.; Whalley, C.M.; et al. Image-Based Consensus Molecular Subtype (ImCMS) Classification of Colorectal Cancer Using Deep Learning. Gut 2021, 70, 544–554. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.G.; Lundström, O.; Blank, A.; Dawson, H.; Lugli, A.; Anisimova, M.; Zlobec, I. Image-Based Assessment of Extracellular Mucin-to-Tumor Area Predicts Consensus Molecular Subtypes (CMS) in Colorectal Cancer. Mod. Pathol. 2022, 35, 240–248. [Google Scholar] [CrossRef]
- Shimada, Y.; Okuda, S.; Watanabe, Y.; Tajima, Y.; Nagahashi, M.; Ichikawa, H.; Nakano, M.; Sakata, J.; Takii, Y.; Kawasaki, T.; et al. Histopathological Characteristics and Artificial Intelligence for Predicting Tumor Mutational Burden-High Colorectal Cancer. J. Gastroenterol. 2021, 56, 547–559. [Google Scholar] [CrossRef]
- Riasatian, A.; Babaie, M.; Maleki, D.; Kalra, S.; Valipour, M.; Hemati, S.; Zaveri, M.; Safarpoor, A.; Shafiei, S.; Afshari, M.; et al. Fine-Tuning and Training of Densenet for Histopathology Image Representation Using TCGA Diagnostic Slides. Med. Image Anal. 2021, 70, 102032. [Google Scholar] [CrossRef] [PubMed]
- Medela, A.; Picon, A. Constellation Loss: Improving the Efficiency of Deep Metric Learning Loss Functions for the Optimal Embedding of Histopathological Images. J. Pathol. Inform. 2020, 11, 38. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Yoon, H.; Thakur, N.; Hwang, G.; Lee, E.J.; Kim, C.; Chong, Y. Deep Learning-Based Histopathological Segmentation for Whole Slide Images of Colorectal Cancer in a Compressed Domain. Sci. Rep. 2021, 11, 6047. [Google Scholar] [CrossRef]
- Khened, M.; Kori, A.; Rajkumar, H.; Krishnamurthi, G.; Srinivasan, B. A Generalized Deep Learning Framework for Whole-Slide Image Segmentation and Analysis. Sci. Rep. 2021, 11, 11579. [Google Scholar] [CrossRef]
- Deshpande, S.; Minhas, F.; Graham, S.; Rajpoot, N. SAFRON: Stitching Across the Frontier Network for Generating Colorectal Cancer Histology Images. Med. Image Anal. 2022, 77, 102337. [Google Scholar] [CrossRef] [PubMed]
- van der Laak, J.; Litjens, G.; Ciompi, F. Deep Learning in Histopathology: The Path to the Clinic. Nat. Med. 2021, 27, 775–784. [Google Scholar] [CrossRef]
- Wang, Y.; He, X.; Nie, H.; Zhou, J.; Cao, P.; Ou, C. Application of Artificial Intelligence to the Diagnosis and Therapy of Colorectal Cancer. Am. J. Cancer Res. 2020, 10, 3575–3598. [Google Scholar] [PubMed]
- Montezuma, D.; Monteiro, A.; Fraga, J.; Ribeiro, L.; Gonçalves, S.; Tavares, A.; Monteiro, J.; Macedo-Pinto, I. Digital Pathology Implementation in Private Practice: Specific Challenges and Opportunities. Diagnostics 2022, 12, 529. [Google Scholar] [CrossRef]
- Baxi, V.; Edwards, R.; Montalto, M.; Saha, S. Digital Pathology and Artificial Intelligence in Translational Medicine and Clinical Practice. Mod. Pathol. 2022, 35, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, S.P.; Neto, P.C.; Fraga, J.; Montezuma, D.; Monteiro, A.; Monteiro, J.; Ribeiro, L.; Gonçalves, S.; Pinto, I.M.; Cardoso, J.S. CAD Systems for Colorectal Cancer from WSI Are Still Not Ready for Clinical Acceptance. Sci. Rep. 2021, 11, 14358. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, H.; Kiyuna, T. Requirements for Implementation of Artificial Intelligence in the Practice of Gastrointestinal Pathology. World J. Gastroenterol. 2021, 27, 2818–2833. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Davri, A.; Birbas, E.; Kanavos, T.; Ntritsos, G.; Giannakeas, N.; Tzallas, A.T.; Batistatou, A. Deep Learning on Histopathological Images for Colorectal Cancer Diagnosis: A Systematic Review. Diagnostics 2022, 12, 837. https://doi.org/10.3390/diagnostics12040837
Davri A, Birbas E, Kanavos T, Ntritsos G, Giannakeas N, Tzallas AT, Batistatou A. Deep Learning on Histopathological Images for Colorectal Cancer Diagnosis: A Systematic Review. Diagnostics. 2022; 12(4):837. https://doi.org/10.3390/diagnostics12040837
Chicago/Turabian StyleDavri, Athena, Effrosyni Birbas, Theofilos Kanavos, Georgios Ntritsos, Nikolaos Giannakeas, Alexandros T. Tzallas, and Anna Batistatou. 2022. "Deep Learning on Histopathological Images for Colorectal Cancer Diagnosis: A Systematic Review" Diagnostics 12, no. 4: 837. https://doi.org/10.3390/diagnostics12040837