
Factors Influencing the Prognosis of Patients with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome

 , , ,
, , ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Ethics
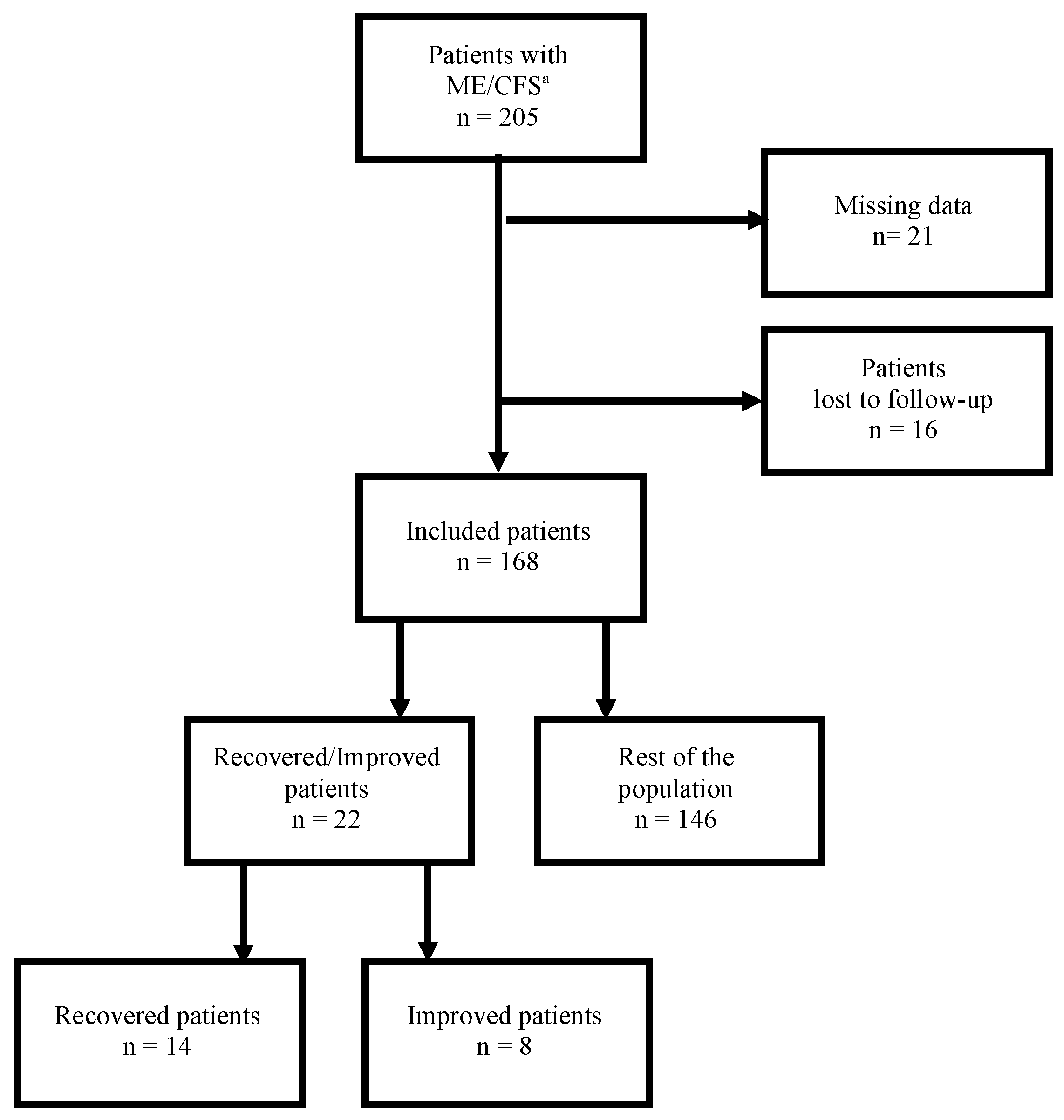
2.2. Study Population
2.3. Exclusion Criteria
2.4. Study Design
Review of Patients’ Medical Records
Initial Assessment
Follow-Up Visits
2.5. Measures
2.5.1. Self-Reported Changes
2.5.2. Fatigue Scales
2.5.3. Functional Impairment
2.5.4. PEM and Baseline Symptoms
2.5.5. Occupational Status
2.6. Defining Recovery and Significant Improvement
2.7. Patients’ Grouping
2.8. Statistical Analysis
3. Results
4. Discussion
4.1. Recovery and Improvement Rates
4.2. Age at Disease Onset
4.3. Diagnostic Delay
4.4. Time of Follow-Up
4.5. Baseline Fatigue Severity
4.6. Comorbidities
4.7. Comparison between Recovered and Significantly Improved Patients
4.8. Work-Related Outcomes
4.9. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carruthers, B.M.; van de Sande, M.I.; De Meirleir, K.L.; Klimas, N.G.; Broderick, G.; Mitchell, T.; Staines, D.; Powles, A.C.P.; Speight, N.; Vallings, R.; et al. Myalgic Encephalomyelitis: International Consensus Criteria. J. Intern. Med. 2011, 270, 327–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carruthers, B.M.; Jain, A.K.; De Meirleir, K.L.; Peterson, D.L.; Klimas, N.G.; Lerner, A.M.; Bested, A.C.; Flor-Henry, P.; Joshi, P.; Powles, A.C.P.; et al. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Clinical Working Case Definition, Diagnostic and Treatment Protocols. J. Chronic Fatigue Syndr. 2003, 11, 7–115. [Google Scholar] [CrossRef]
- Fukuda, K.; Straus, S.E.; Hickie, I.; Sharpe, M.C.; Dobbins, J.G.; Komaroff, A. The Chronic Fatigue Syndrome: A Comprehensive Approach to Its Definition and Study. Ann. Intren. Med. 1994, 121, 953–959. [Google Scholar] [CrossRef]
- Committee on the Diagnostic Criteria for Myalgic Encephalomyelitis/Chronic Fatigue Syndrome; Board on the Health of Select Populations; Institute of Medicine. Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness. Mil. Med. 2015, 180, 721–723. [Google Scholar] [CrossRef] [Green Version]
- Collin, S.M.; Crawley, E. Specialist Treatment of Chronic Fatigue Syndrome/ME: A Cohort Study among Adult Patients in England. BMC Health Serv. Res. 2017, 17, 488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brurberg, K.G.; Fønhus, M.S.; Larun, L.; Flottorp, S.; Malterud, K. Case Definitions for Chronic Fatigue Syndrome/Myalgic Encephalomyelitis (CFS/ME): A Systematic Review. BMJ Open 2014, 4, e003973. [Google Scholar] [CrossRef]
- Twisk, F.N. Accurate Diagnosis of Myalgic Encephalomyelitis and Chronic Fatigue Syndrome Based upon Objective Test Methods for Characteristic Symptoms. World J. Methodol. 2015, 5, 68. [Google Scholar] [CrossRef] [Green Version]
- Jason, L.A.; Sunnquist, M.; Brown, A.; Evans, M.; Newton, J.L. Are Myalgic Encephalomyelitis and Chronic Fatigue Syndrome Different Illnesses? A Preliminary Analysis. J. Health Psychol. 2016, 21, 3–15. [Google Scholar] [CrossRef] [Green Version]
- Adamowicz, J.L.; Caikauskaite, I.; Friedberg, F. Defining Recovery in Chronic Fatigue Syndrome: A Critical Review. Qual. Life Res. 2014, 23, 2407–2416. [Google Scholar] [CrossRef]
- Peterson, P.K.; Schenck, C.H.; Sherman, R. Chronic Fatigue Syndrome in Minnesota. Minn. Med. 1991, 74, 21–26. [Google Scholar]
- Wilson, A.; Hickie, I.; Lloyd, A.; Hadzi-Pavlovic, D.; Boughton, C.; Dwyer, J.; Wakefield, D. Longitudinal Study of Outcome of Chronic Fatigue Syndrome. BMJ 1994, 308, 756–759. [Google Scholar] [CrossRef] [PubMed]
- Bombardier, C.H.; Buchwald, D. Outcome and Prognosis of Patients With Chronic Fatigue vs Chronic Fatigue Syndrome. Arch. Intern. Med. 1995, 155, 2105–2110. [Google Scholar] [CrossRef] [PubMed]
- Vercoulen, J.H.; Swanink, C.M.; Fennis, J.F.; Galama, J.M.; van der Meer, J.W.; Bleijenberg, G. Prognosis in Chronic Fatigue Syndrome: A Prospective Study on the Natural Course. J. Neurol. Neurosurg. Psychiatry 1996, 60, 489–494. [Google Scholar] [CrossRef] [Green Version]
- van der Werf, S.P.; de Vree, B.; Alberts, M.; van der Meer, J.W.M.; Bleijenberg, G. Natural Course and Predicting Self-Reported Improvement in Patients with Chronic Fatigue Syndrome with a Relatively Short Illness Duration. J. Psychosom. Res. 2002, 53, 749–753. [Google Scholar] [CrossRef]
- Cairns, R.; Hotopf, M. A Systematic Review Describing the Prognosis of Chronic Fatigue Syndrome. Occup. Med. 2005, 55, 20–31. [Google Scholar] [CrossRef] [Green Version]
- Joyce, J. The Prognosis of Chronic Fatigue and Chronic Fatigue Syndrome: A Systematic Review. QJM 1997, 90, 223–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rowe, P.C.; Underhill, R.A.; Friedman, K.J.; Gurwitt, A.; Medow, M.S.; Schwartz, M.S.; Speight, N.; Stewart, J.M.; Vallings, R.; Rowe, K.S. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Diagnosis and Management in Young People: A Primer. Front. Pediatr. 2017, 5, 121. [Google Scholar] [CrossRef] [Green Version]
- Clark, M.R.; Katon, W.; Russo, J.; Kith, P.; Sintay, M.; Buchwald, D. Chronic Fatigue: Risk Factors for Symptom Persistence in a 2 1/2-Year Follow-up Study. Am. J. Med. 1995, 98, 187–195. [Google Scholar] [CrossRef]
- Tiersky, L.A.; DeLuca, J.; Hill, N.; Dhar, S.K.; Johnson, S.K.; Lange, G.; Rappolt, G.; Natelson, B.H. Longitudinal Assessment of Neuropsychological Functioning, Psychiatric Status, Functional Disability and Employment Status in Chronic Fatigue Syndrome. Appl. Neuropsychol. 2001, 8, 41–50. [Google Scholar] [CrossRef]
- Sharpe, M.; Hawton, K.; Seagroatt, V.; Pasvol, G. Follow up of Patients Presenting with Fatigue to an Infectious Diseases Clinic. BMJ 1992, 305, 147–152. [Google Scholar] [CrossRef] [Green Version]
- Pheley, A.M.; Melby, D.; Schenck, C.; Mandel, J.; Peterson, P.K. Can We Predict Recovery in Chronic Fatigue Syndrome? Minn. Med. 1999, 82, 52–56. [Google Scholar] [PubMed]
- Matthews, R.M.; Komaroff, A.L. Changes in Functional Status in Chronic Fatigue Syndrome Over a Decade. J. Chronic Fatigue Syndr. 2007, 14, 33–42. [Google Scholar] [CrossRef]
- Reyes, M.; Dobbins, J.G.; Nisenbaum, R.; Subedar, N.S.; Randall, B.; Reeves, W.C. Chronic Fatigue Syndrome Progression and Self-Defined Recovery. J. Chronic Fatigue Syndr. 1999, 5, 17–27. [Google Scholar] [CrossRef]
- Nisenbaum, R.; Jones, J.F.; Unger, E.R.; Reyes, M.; Reeves, W.C. A Population-Based Study of the Clinical Course of Chronic Fatigue Syndrome. Health Qual. Life Outcomes 2003, 1, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nyland, M.; Naess, H.; Birkeland, J.S.; Nyland, H. Longitudinal Follow-up of Employment Status in Patients with Chronic Fatigue Syndrome after Mononucleosis. BMJ Open 2014, 4, e005798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersen, M.M.; Permin, H.; Albrecht, F. Illness and Disability in Danish Chronic Fatigue Syndrome Patients at Diagnosis and 5-Year Follow-Up. J. Psychosom. Res. 2004, 56, 217–229. [Google Scholar] [CrossRef]
- Lawrie, S.M.; Manders, D.N.; Geddes, J.R.; Pelosi, A.J. A Population-Based Incidence Study of Chronic Fatigue. Psychol. Med. 1997, 27, 343–353. [Google Scholar] [CrossRef]
- Jason, L.A.; Porter, N.; Brown, M.; Anderson, V.; Brown, A.; Hunnell, J.; Lerch, A. CFS: A Review of Epidemiology and Natural History Studies. Bull. IACFS ME 2009, 17, 88–106. [Google Scholar]
- Taylor, R.R.; Jason, L.A.; Curie, C.J. Prognosis of Chronic Fatigue in a Community-Based Sample. Psychosom. Med. 2002, 64, 319–327. [Google Scholar] [CrossRef] [Green Version]
- Ciccone, D.S.; Chandler, H.K.; Natelson, B.H. Illness Trajectories in the Chronic Fatigue Syndrome: A Longitudinal Study of Improvers versus Non-Improvers. J. Nerv. Ment. Dis. 2010, 198, 486–493. [Google Scholar] [CrossRef]
- Theorell, T.; Blomkvist, V.; Lindh, G.; Evengård, B. Critical Life Events, Infections, and Symptoms during the Year Preceding Chronic Fatigue Syndrome (CFS): An Examination of CFS Patients and Subjects with a Nonspecific Life Crisis. Psychosom. Med. 1999, 61, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Buchwald, D.S.; Rea, T.D.; Katon, W.J.; Russo, J.E.; Ashley, R.L. Acute Infectious Mononucleosis: Characteristics of Patients Who Report Failure to Recover. Am. J. Med. 2000, 109, 531–537. [Google Scholar] [CrossRef]
- Torres-Harding, S.R.; Jason, L.A.; Taylor, R.R. Fatigue Severity, Attributions, Medical Utilization, and Symptoms in Persons with Chronic Fatigue. J. Behav. Med. 2002, 25, 99–113. [Google Scholar] [CrossRef]
- Bierl, C.; Nisenbaum, R.; Hoaglin, D.C.; Randall, B.; Jones, A.-B.; Unger, E.R.; Reeves, W.C. Regional Distribution of Fatiguing Illnesses in the United States: A Pilot Study. Popul. Health Metr. 2004, 2, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jason, L.A.; Corradi, K.; Gress, S.; Williams, S.; Torres-Harding, S. Causes of Death Among Patients With Chronic Fatigue Syndrome. Health Care Women Int. 2006, 27, 615–626. [Google Scholar] [CrossRef]
- Chalder, T.; Berelowitz, G.; Pawlikowska, T.; Watts, L.; Wessely, S.; Wright, D.; Wallace, E.P. Development of a Fatigue Scale. J. Psychosom. Res. 1993, 37, 147–153. [Google Scholar] [CrossRef] [Green Version]
- Krupp, L.B.; LaRocca, N.G.; Muir-Nash, J.; Steinberg, A.D. The Fatigue Severity Scale: Application to Patients With Multiple Sclerosis and Systemic Lupus Erythematosus. Arch. Neurol. 1989, 46, 1121–1123. [Google Scholar] [CrossRef]
- Larson, R.D. Psychometric Properties of the Modified Fatigue Impact Scale. Int. J. MS Care 2013, 15, 15–20. [Google Scholar] [CrossRef] [Green Version]
- Wagner, D.; Nisenbaum, R.; Heim, C.; Jones, J.F.; Unger, E.R.; Reeves, W.C. Psychometric Properties of the CDC Symptom Inventory for Assessment of Chronic Fatigue Syndrome. Popul. Health Metr. 2005, 3, 8. [Google Scholar] [CrossRef] [Green Version]
- Devendorf, A.R.; Jackson, C.T.; Sunnquist, M.; Jason, L.A. Defining and Measuring Recovery from Myalgic Encephalomyelitis and Chronic Fatigue Syndrome: The Physician Perspective. Disabil. Rehabil. 2019, 41, 158–165. [Google Scholar] [CrossRef]
- Friedberg, F.; Dechene, L.; McKenzie, M.J.; Fontanetta, R. Symptom Patterns in Long-Duration Chronic Fatigue Syndrome. J. Psychosom. Res. 2000, 48, 59–68. [Google Scholar] [CrossRef]
- Ray, C.; Jefferies, S.; Weir, W.R.C. Coping and Other Predictors of Outcome in Chronic Fatigue Syndrome: A 1-Year Follow-Up. J. Psychosom. Res. 1997, 43, 405–415. [Google Scholar] [CrossRef]
- Ghali, A.; Richa, P.; Lacout, C.; Gury, A.; Beucher, A.-B.; Homedan, C.; Lavigne, C.; Urbanski, G. Epidemiological and Clinical Factors Associated with Post-Exertional Malaise Severity in Patients with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. J. Transl. Med. 2020, 18, 246. [Google Scholar] [CrossRef] [PubMed]
- Vandvik, P.O.; Wilhelmsen, I.; Ihlebæk, C.; Farup, P.G. Comorbidity of Irritable Bowel Syndrome in General Practice: A Striking Feature with Clinical Implications. Aliment. Pharmacol. Ther. 2004, 20, 1195–1203. [Google Scholar] [CrossRef] [PubMed]
- Creed, F.H.; Tomenson, B.; Chew-Graham, C.; Macfarlane, G.J.; Davies, I.; Jackson, J.; Littlewood, A.; McBeth, J. Multiple Somatic Symptoms Predict Impaired Health Status in Functional Somatic Syndromes. Int.J. Behav. Med. 2013, 20, 194–205. [Google Scholar] [CrossRef] [PubMed]
- Myhill, S.; Booth, N.E.; McLaren-Howard, J. Chronic Fatigue Syndrome and Mitochondrial Dysfunction. Int. J. Clin. Exp. Med. 2009, 2, 1–16. [Google Scholar]
- Hatziagelaki, E.; Adamaki, M.; Tsilioni, I.; Dimitriadis, G.; Theoharides, T.C. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome—Metabolic Disease or Disturbed Homeostasis Due to Focal Inflammation in the Hypothalamus? J. Pharmacol. Exp. Ther. 2018, 367, 155–167. [Google Scholar] [CrossRef] [Green Version]
- Broderick, G.; Fuite, J.; Kreitz, A.; Vernon, S.D.; Klimas, N.; Fletcher, M.A. A Formal Analysis of Cytokine Networks in Chronic Fatigue Syndrome. Brain Behav. Immun. 2010, 24, 1209–1217. [Google Scholar] [CrossRef] [Green Version]
- Hoad, A.; Spickett, G.; Elliott, J.; Newton, J. Postural Orthostatic Tachycardia Syndrome Is an Under-Recognized Condition in Chronic Fatigue Syndrome. QJM 2008, 101, 961–965. [Google Scholar] [CrossRef]
- Devendorf, A.R.; McManimen, S.L.; Jason, L.A. Suicidal Ideation in Non-Depressed Individuals: The Effects of a Chronic, Misunderstood Illness. J. Health Psychol. 2020, 25, 2106–2117. [Google Scholar] [CrossRef]
- Report Viewer|NINDS Common Data Elements. Available online: https://www.commondataelements.ninds.nih.gov/report-viewer/23534/Modified%20Fatigue%20Impact%20Scale%20(MFIS)(accessed on 20 July 2022).



{kind=link}
{kind=link}
| Patients with Recovery/Significant Improvement | The Rest of the Study Population | p | |
|---|---|---|---|
| Epidemiological characteristics | |||
| Patients, n (%) | 22 (13.1) | 146 (86.9) | |
| Female, n (%) | 16 (72.7) | 103 (70.5) | 0.83 |
| BMI, kg/m2 | 24.2 (21.4–26.7) | 22.8 (20–26.2] | 0.25 |
| Age at data collection, years | 49.1 (39.5–57.3) | 43.8 (35.8–49.6) | 0.07 |
| Age at disease onset, years | 45 (32.5–48.3) | 32 (25–40) | 0.002 |
| Age at diagnosis, years | 45.5 (34.3–51) | 40 (32–46) | 0.14 |
| Diagnostic delay, months | 23 (16–40) | 55 (24–102) | 0.0004 |
| Time of follow-up, months | 46 (34–56) | 32.5 (19–49) | 0.013 |
| Family history of fatigue, n (%) | 1 (4.5) | 8 (5.5) | >0.99 |
| Sudden onset of the illness, n (%) | 14 (64.1) | 74 (50.7) | 0.26 |
| Identified illness precipitants | 18 (81.1) | 107 (73.3) | 0.39 |
| Infectious precipitants | 14 (64.1) | 74 (50.7) | 0.26 |
| Non-infectious precipitants | 4 (18.2) | 33 (22.6) | 0.79 |
| Baseline fatigue assessment | |||
| Fatigue severity scale | 5.9 (5.2–6.4) | 5.9 (5.2–6.5] (n = 130) | 0.34 |
| Fatigue scale | 25 (20–27) | 24 (21–28] (n = 119) | 0.60 |
| MFIS a physical | 28 (26–32.8) | 30 (26–33] (n = 119) | 0.69 |
| MFIS cognitive | 25.5 (19.3–30.8) | 29 (22–33] (n = 119) | 0.12 |
| MFIS psychosocial | 6 (5.6) | 6 (4–7] (n = 119) | 0.52 |
| Baseline PEM b assessment | |||
| PEM frequency | 3 (2.25–3) | 3 (3–3) | 0.90 |
| PEM intensity | 4 (4–4) | 4 (2.5–4) | 0.16 |
| PEM severity | 10 (8–12) | 12 (7.5–12) | 0.30 |
| Clinical manifestations, n (%) | |||
| Difficulty processing information | 22 (100) | 140 (95.9) | >0.99 |
| Short-term memory loss | 17 (77.3) | 130 (89) | 0.16 |
| Headaches | 16 (72.7) | 106 (72.6) | 0.99 |
| Myalgia | 20 (90.9) | 127 (87) | >0.99 |
| Arthralgia | 13 (59.1) | 96 (65.8) | 0.54 |
| Disturbed sleep patterns | 19 (86.4) | 123 (84.2) | >0.99 |
| Unrefreshed sleep | 20 (90.9) | 140 (98.6) | 0.28 |
| Neurosensory and perceptual disturbances | 18 (81.8) | 132 (90.4) | 0.26 |
| Motor disturbances | 21 (95.5) | 136 (93.1) | >0.99 |
| Flu-like symptoms | 10 (45.5) | 89 (61) | 0.17 |
| Recurrent infections | 8 (36.4) | 53 (36.3) | >0.99 |
| Gastrointestinal impairments | 20 (90.9) | 118 (83.1) | >0.99 |
| Urinary impairments | 4 (18.2) | 51 (36.1) | 0.15 |
| Orthostatic intolerance | 6 (27.3) | 62 (42.5) | 0.18 |
| Palpitation | 14 (63.6) | 94(64.4) | 0.12 |
| Vertigo | 16 (72.2) | 78 (53.4) | 0.09 |
| Respiratory involvement | 10 (45.5) | 82 (56.2) | 0.35 |
| Intolerance to extreme temperatures | 13 (59.1) | 103 (70.6) | 0.28 |
| Comorbidities, n (%) | |||
| Reactional depression | 8 (36.4) | 52 (35.6) | 0.95 |
| Hashimoto’s thyroiditis | 3 (13.6) | 11 (7.5) | 0.02 |
| Fibromyalgia | 1 (4.5) | 31 (21.2) | 0.08 |
| Irritable bowel syndrome | 5 (22.7) | 59 (40.4) | 0.04 |
| Estimate | p-Value | OR (95% CI) a | |
|---|---|---|---|
| Intercept | −3.566 | 0.002 | 0.03 (0.002–0.252) |
| Age at onset | 0.054 | 0.028 | 1.06 (1.007–1.110) |
| Diagnostic delay | −0.017 | 0.036 | 0.98 (0.964–0.996) |
| Time of follow-up | 0.019 | 0.121 | 1.02 (0.995–1.044) |
| Thyroiditis | 0.355 | 0.720 | 1.43 (0.160–8.895) |
| Irritable bowel syndrome | −1.052 | 0.090 | 0.35 (0.090–1.087) |
| N° a | R/I b | Age at R/I, Years | Work Status at Diagnosis | Work-Related Outcomes |
|---|---|---|---|---|
| 1 | I | 61.6 | Forklift operator on sick leave | Not able to return to working, but can do handiwork and gardening 4 h/day |
| 2 | R | 46.6 | Working as a cook. Part-time | Recovered 9 months after redundancy and returned to full-time work |
| 3 | R | 30.5 | Office work. Part-time | Returned to full-time work |
| 4 | R | 30.5 | Forklift operator. Part-time | Recovered after reducing hardship at work. Full-time work |
| 5 | I | 50.0 | Hairdresser. Part-time | Not able to return to working but can do sewing work 2 h/day |
| 6 | R | 56.0 | Nurse. Part-time | Returned to full-time work |
| 7 | R | 34.0 | Working in a fashion store. Part-time | Returned to full-time work |
| 8 | I | 39.3 | Working as a cleaner on sick leave | Professional retraining. Half-time work |
| 9 | R | 34.5 | Working in sales. Part-time | Returned to full-time work |
| 10 | R | 42.3 | Working in a bar on sick leave | Returned to full-time work |
| 11 | R | 59.2 | Plumber on sick leave | Recovered 9 months after being recognized as a disabled worker and returned to full-time work |
| 12 | R | 46.0 | Working in computer field. Part-time | Returned to full-time work |
| 13 | I | 48.9 | School teacher on sick leave | Part-time work |
| 14 | I | 46.7 | Working in computer field on sick leave | Improved 6 months after being recognized as a disabled worker (2nd degree invalidity). Not able to return to working |
| 15 | I | 56.5 | School teacher on sick leave | Not able to return to working |
| 16 | I | 53.3 | Assistant manager on sick leave | Not able to return to working |
| 17 | R | 41.3 | Working in a restaurant on sick leave | Returned to full-time work |
| 18 | R | 60.3 | Assistant nurse on sick leave | Recovered 10 months after being recognized as a disabled worker (2nd degree invalidity) and was able to get another full-time job |
| 19 | R | 53.5 | Manager in an educational service on sick leave | Recovered 2 years after early retirement and was able to get another full-time job |
| 20 | R | 42.9 | Project manager. Part-time | Returned to full-time work |
| 21 | I | 32.3 | Working in a museum on sick leave | Not able to return to working |
| 22 | R | 35.1 | Working in sales on sick leave | Recovered after being recognized as a disabled worker and was able to get another full-time job |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghali, A.; Lacout, C.; Fortrat, J.-O.; Depres, K.; Ghali, M.; Lavigne, C. Factors Influencing the Prognosis of Patients with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Diagnostics 2022, 12, 2540. https://doi.org/10.3390/diagnostics12102540
Ghali A, Lacout C, Fortrat J-O, Depres K, Ghali M, Lavigne C. Factors Influencing the Prognosis of Patients with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Diagnostics. 2022; 12(10):2540. https://doi.org/10.3390/diagnostics12102540
Chicago/Turabian StyleGhali, Alaa, Carole Lacout, Jacques-Olivier Fortrat, Karine Depres, Maria Ghali, and Christian Lavigne. 2022. "Factors Influencing the Prognosis of Patients with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome" Diagnostics 12, no. 10: 2540. https://doi.org/10.3390/diagnostics12102540