
Leveraging Computational Intelligence Techniques for Diagnosing Degenerative Nerve Diseases: A Comprehensive Review, Open Challenges, and Future Research Directions

Abstract
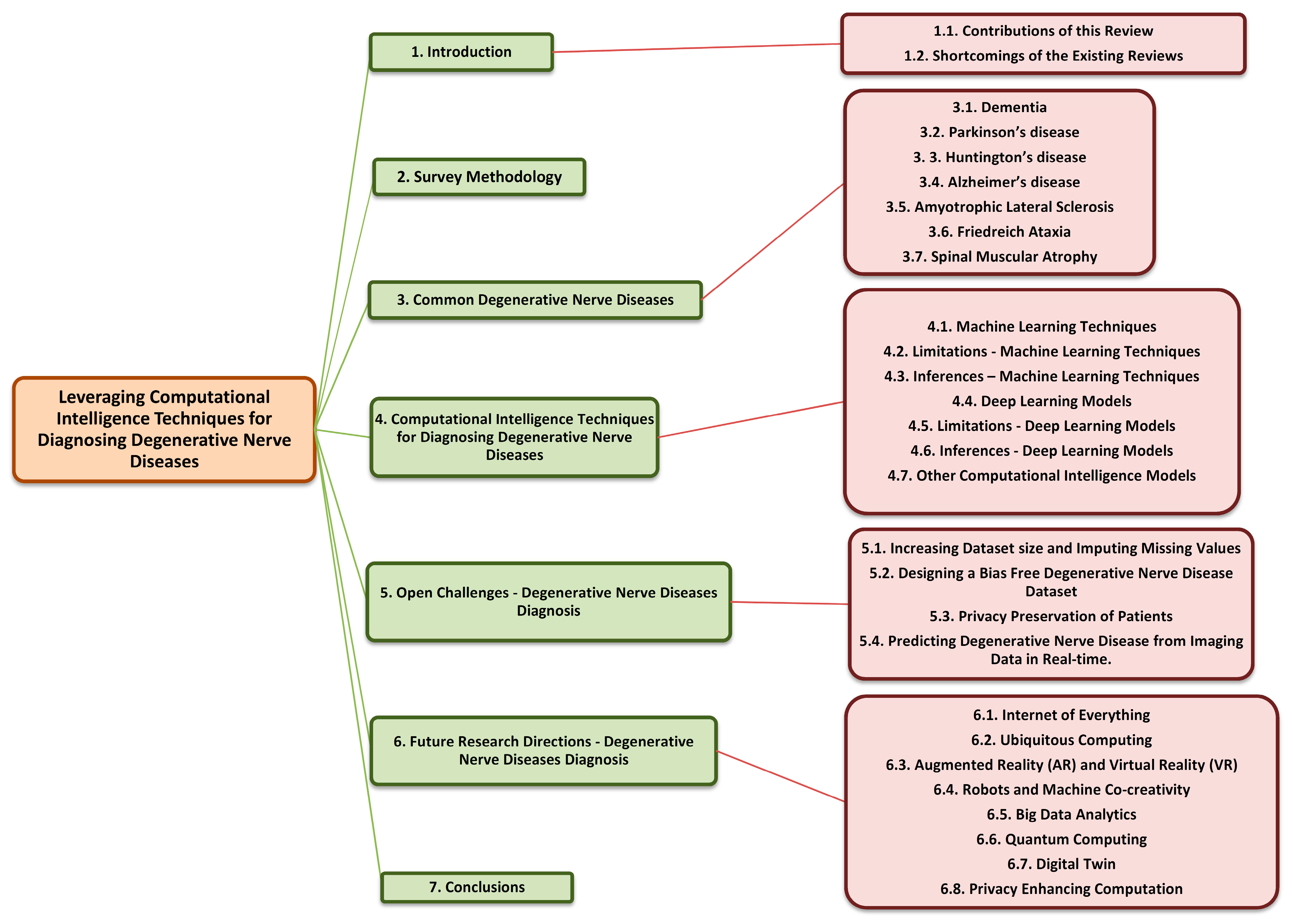
:1. Introduction
1.1. Contributions of This Review
- Through this paper, we present an extensive study of machine learning and deep learning models used for diagnosing degenerative nerve diseases and show that ML and DL have a high potential for facilitating the diagnosis of degenerative nerve diseases.
- We give a detailed account of the recent developments made to improve the accuracy, scalability, and sensitivity of various ML and DL algorithms mentioned in this paper.
- Key highlights and limitations of these newly developed models are also discussed in detail.
- Along with this, alternate research directions for the diagnosis of degenerative nerve diseases disorders using the fields of IoT (Internet of Things), quantum computing, Big data analytics, etc., are also touched upon.
1.2. Shortcomings of the Existing Reviews
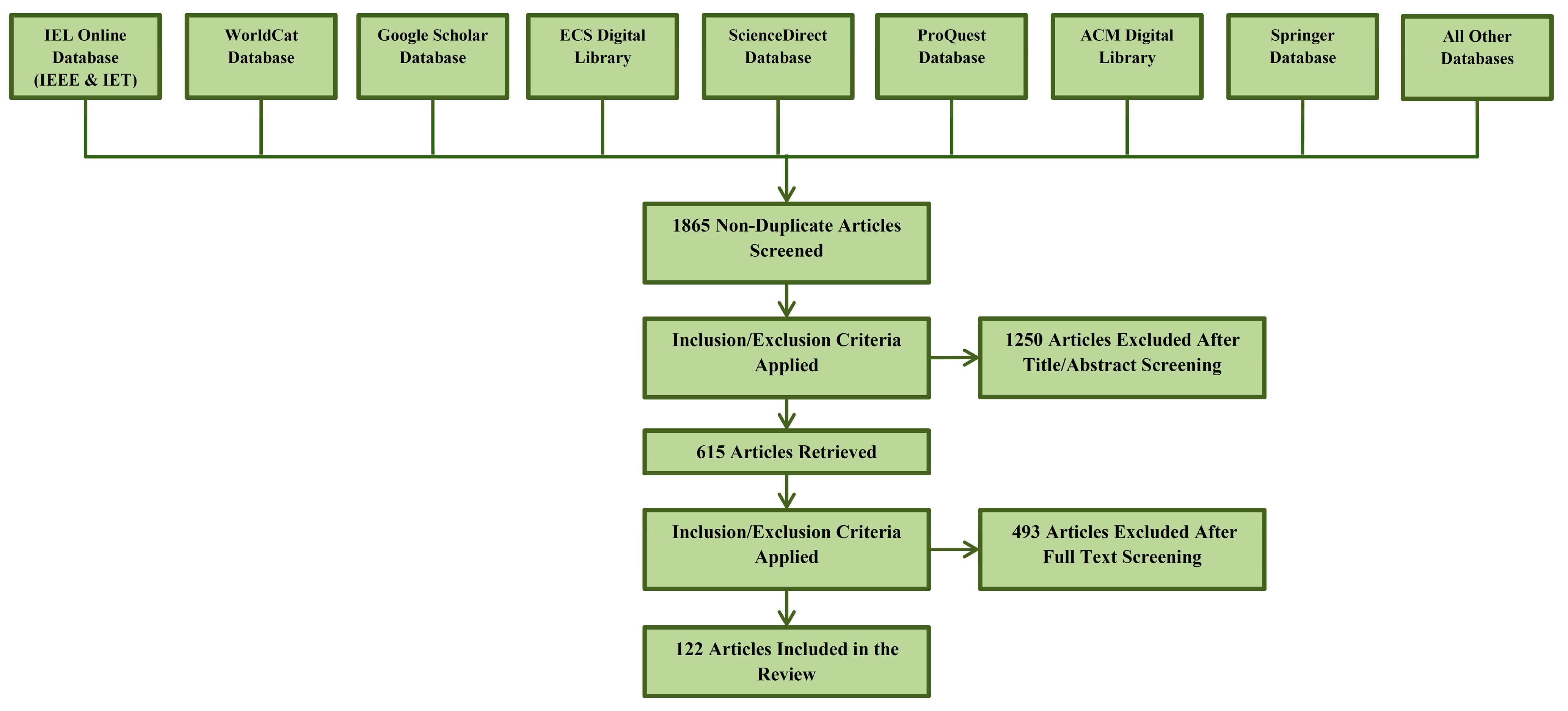
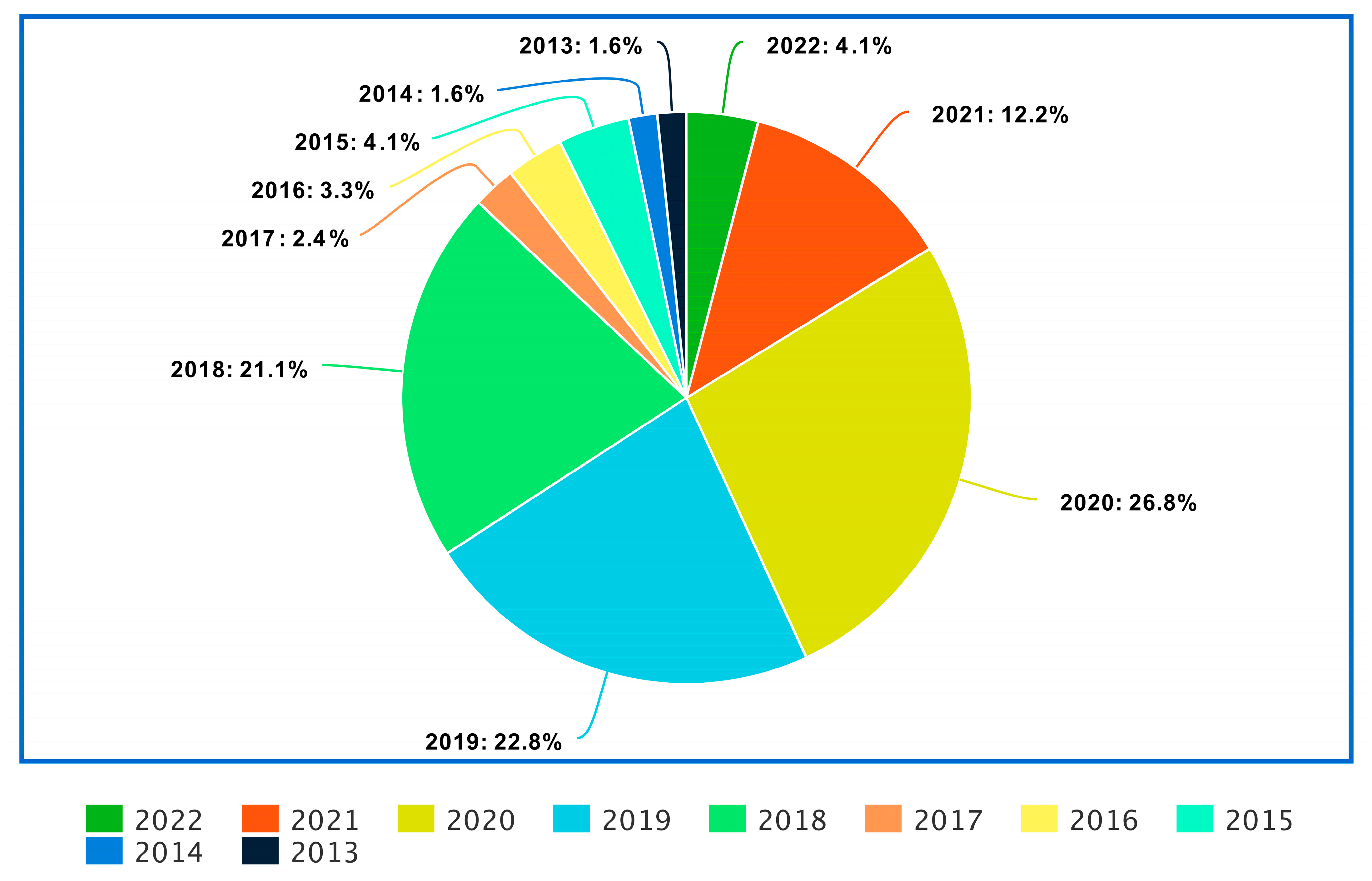
2. Survey Methodology
3. Common Degenerative Nerve Diseases
3.1. Dementia
3.2. Parkinson’s Disease
3.3. Huntington’s Disease
3.4. Alzheimer’s Disease
3.5. Amyotrophic Lateral Sclerosis
3.6. Friedreich Ataxia
3.7. Spinal Muscular Atrophy
4. Computational Intelligence Techniques for Diagnosing Degenerative Nerve Diseases
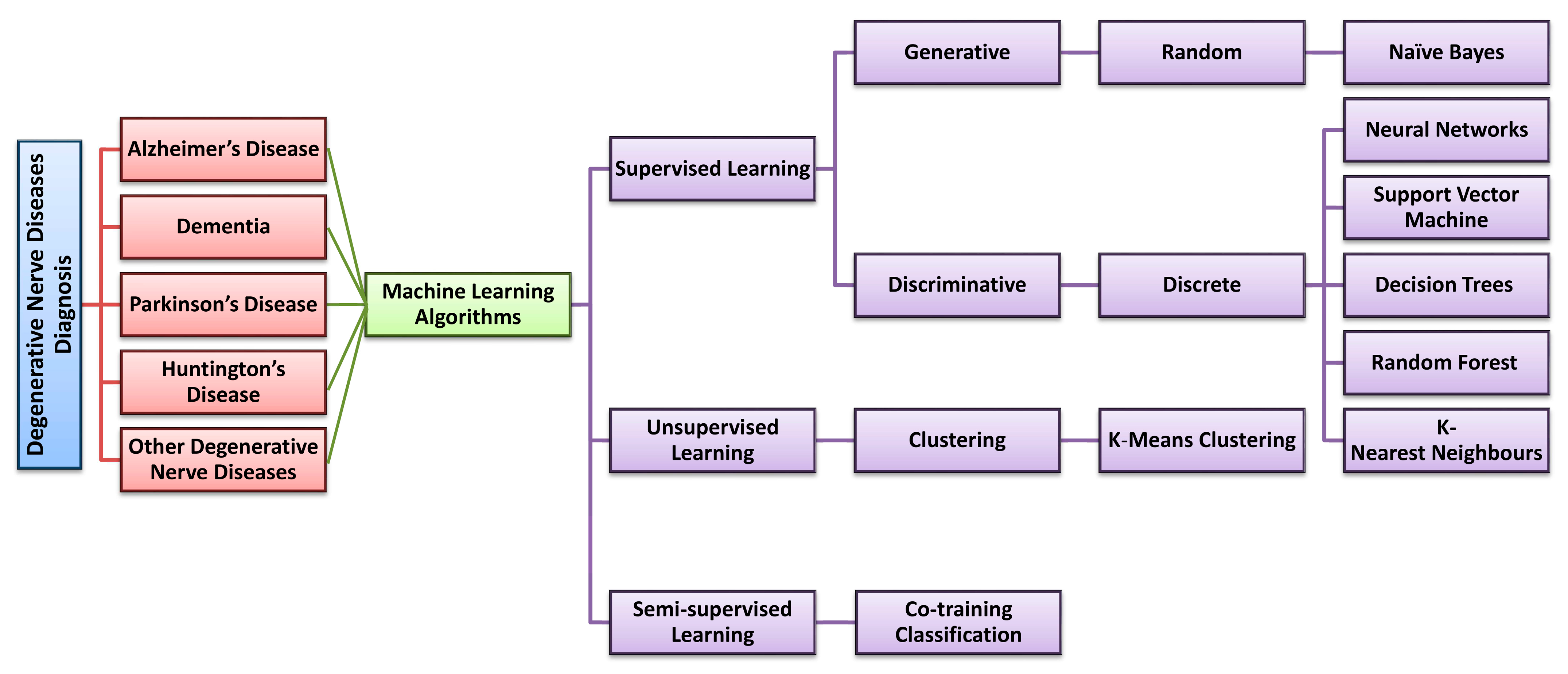
4.1. Machine Learning Techniques
4.1.1. Artificial Neural Network
4.1.2. Support Vector Machine
4.1.3. K-Means Clustering
4.1.4. Decision Tree
4.1.5. Random Forest
4.1.6. Naïve Bayes
4.1.7. K-Nearest Neighbor (KNN)
4.1.8. Extreme Learning Machine
4.1.9. Co-Training Classification
4.2. Limitations: Machine Learning Techniques
4.3. Inferences-Machine Learning Techniques
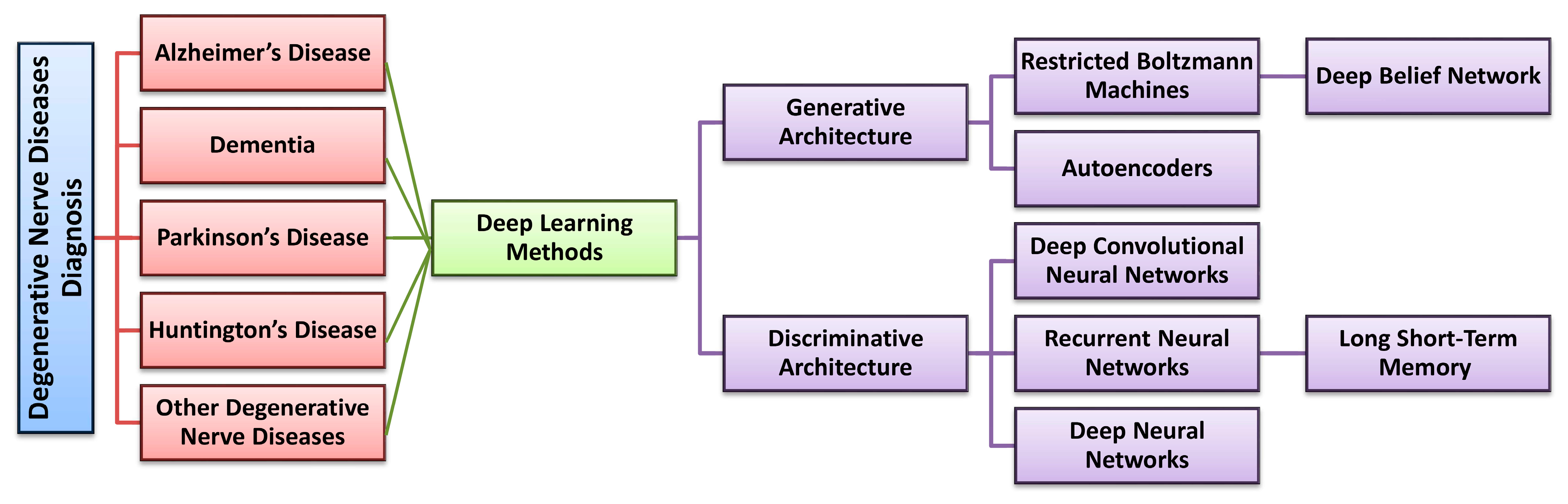
4.4. Deep Learning Models
4.4.1. Recurrent Neural Networks and Long Short-Term Memory
4.4.2. Autoencoder
4.4.3. Deep Belief Network
4.4.4. Deep Convolutional Neural Network
4.4.5. Deep Neural Network
4.5. Limitations-Deep Learning Models
4.6. Inferences-Deep Learning Models
4.7. Other Computational Intelligence Models
4.7.1. Probabilistic Neural Network
4.7.2. Deep Residual Network
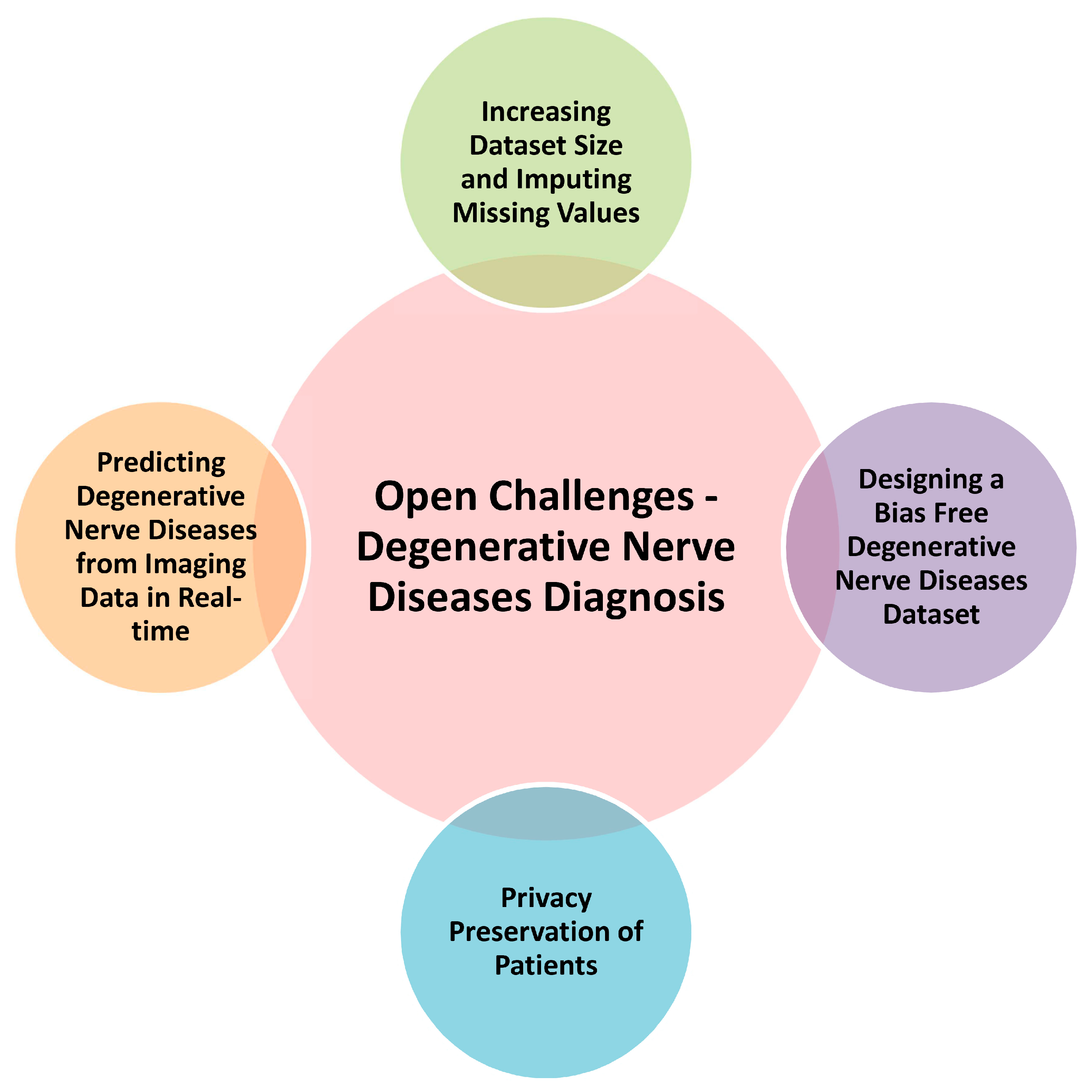
5. Open Challenges-Degenerative Nerve Diseases Diagnosis
5.1. Increasing Dataset Size and Imputing Missing Values
5.2. Designing a Bias Free Degenerative Nerve Diseases Dataset
5.3. Privacy Preservation of Patients
5.4. Predicting Degenerative Nerve Diseases from Imaging Data in Real-Time
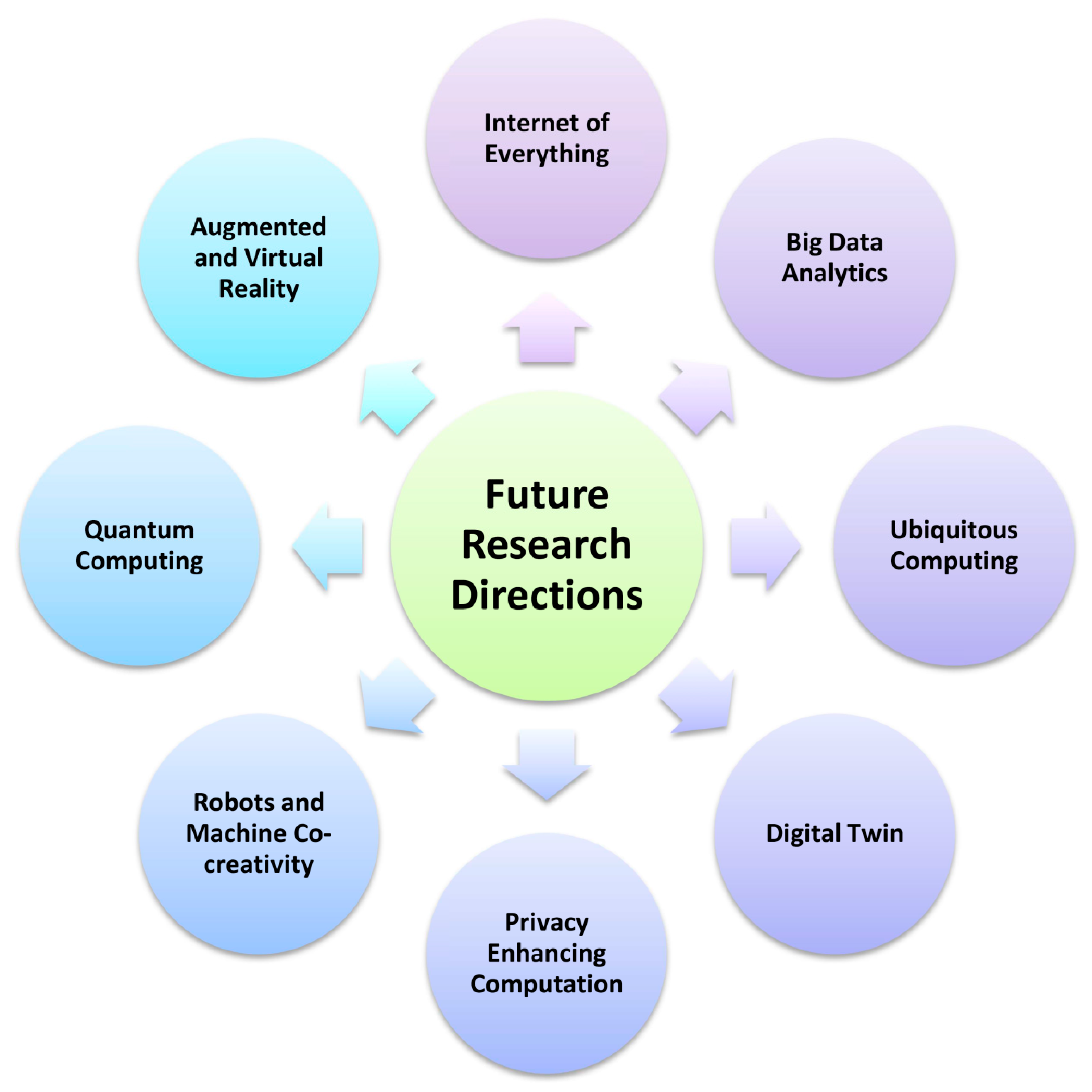
6. Future Research Directions: Degenerative Nerve Diseases Diagnosis
6.1. Internet of Everything
6.2. Ubiquitous Computing
6.3. Augmented Reality (AR) and Virtual Reality (VR)
6.4. Robots and Machine Co-Creativity
6.5. Big Data Analytics
6.6. Quantum Computing
6.7. Digital Twin
6.8. Privacy Enhancing Computation
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Acronym | Full Form |
|---|---|
| MRI | Magnetic resonance imaging |
| EEG | Electroencephalography |
| SPECT | Single photon emission computerized tomography |
| IoT | Internet of Things |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| DNA | Deoxyribonucleic acid |
| CAG | Cytosine, adenine, guanine |
| ALS | Amyotrophic lateral sclerosis |
| FXN | Frataxin |
| SMA | Spinal muscular atrophy |
| ANN | Artificial neural network |
| SVM | Support vector machine |
| DA | Dragonfly algorithm |
| FOG | Freezing of gait |
| LBD | Lewy body dementia |
| HPT | Hyper parameter tuning |
| OASIS | Outcome and assessment information set |
| CART | Classification and regression trees |
| PCA | Principal component analysis |
| KNN | K-nearest neighbor |
| LSTM | Long short-term memory |
| BRNN | Bidirectional recurrent neural networks |
| RNN | Recurrent neural networks |
| ADNI | Alzheimer’s Disease Neuroimaging Initiative |
| AD | Alzheimer’s disease |
| PET | Positron emission tomography |
| CT | Computed tomography |
| PD | Parkinson’s disease |
| DBN | Deep belief network |
| LDA | Linear discriminant analysis |
| ELM | Extreme learning machine |
| CNN | Convolutional neural network |
| DCNN | Deep convolutional neural network |
| HD | Huntington’s disease |
| ML | Machine learning |
| DL | Deep learning |
| AR | Augmented reality |
| VR | Virtual reality |
| AI | Artificial intelligence |
| DNN | Deep neural network |
| PNN | Probabilistic neural network |
| ROC | Receiver operating characteristic |
References
- World Health Organization. Dementia. 20 September 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 3 December 2022).
- Erkkinen, M.G.; Kim, M.O.; Geschwind, M.D. Clinical neurology and epidemiology of the major neurodegenerative diseases. Cold Spring Harb. Perspect. Biol. 2018, 10, a033118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pereira, T.M.C.; Côco, L.Z.; Ton, A.M.M.; Meyrelles, S.S.; Campos-Toimil, M.; Campagnaro, B.P.; Vasquez, E.C. The Emerging Scenario of the Gut–Brain Axis: The Therapeutic Actions of the New Actor Kefir against Neurodegenerative Diseases. Antioxidants 2021, 10, 1845. [Google Scholar] [CrossRef] [PubMed]
- Stephenson, J.; Nutma, E.; van der Valk, P.; Amor, S. Inflammation in CNS neurodegenerative diseases. Immunology 2018, 154, 204–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawal, M.; Olotu, F.A.; Soliman, M.E. Across the blood-brain barrier: Neurotherapeutic screening and characterization of naringenin as a novel CRMP-2 inhibitor in the treatment of Alzheimer’s disease using bioinformatics and computational tools. Comput. Biol. Med. 2018, 98, 168–177. [Google Scholar] [CrossRef]
- Mahendran, N.; Vincent, P.D.R.; Srinivasan, K.; Chang, C.Y. Improving the Classification of Alzheimer’s Disease Using Hybrid Gene Selection Pipeline and Deep Learning. Front. Genet. 2021, 12, 784814. [Google Scholar] [CrossRef]
- Yu, K.H.; Beam, A.L.; Kohane, I.S. Artificial intelligence in healthcare. Nat. Biomed. Eng. 2018, 2, 719–731. [Google Scholar] [CrossRef]
- Buch, V.H.; Ahmed, I.; Maruthappu, M. Artificial intelligence in medicine: Current trends and future possibilities. Br. J. Gen. Pract. 2018, 68, 143–144. [Google Scholar] [CrossRef] [Green Version]
- Kowalczyk, L.; Bajera, A.; Goszczynska, H.; Zalewska, E.; Krolicki, L. Integration of EEG and SPECT data acquired from simultaneous examinations. Biocybern. Biomed. Eng. 2013, 33, 196–203. [Google Scholar] [CrossRef]
- Rangaswamy, U.; Dharshini, S.A.P.; Yesudhas, D.; Gromiha, M.M. VEPAD-Predicting the effect of variants associated with Alzheimer’s disease using machine learning. Comput. Biol. Med. 2020, 124, 103933. [Google Scholar] [CrossRef]
- Dar, M.N.; Akram, M.U.; Yuvaraj, R.; Khawaja, S.G.; Murugappan, M. EEG-based emotion charting for Parkinson’s disease patients using Convolutional Recurrent Neural Networks and cross dataset learning. Comput. Biol. Med. 2022, 144, 105327. [Google Scholar] [CrossRef]
- Arvanitakis, Z.; Shah, R.C.; Bennett, D.A. Diagnosis and management of dementia. Jama 2019, 322, 1589–1599. [Google Scholar] [CrossRef] [PubMed]
- Utsumi, K.; Fukatsu, R.; Yamada, R.; Takamaru, Y.; Hara, Y.; Yasumura, S. Characteristics of initial symptoms and symptoms at diagnosis in probable dementia with Lewy body disease: Incidence of symptoms and gender differences. Psychogeriatrics 2020, 20, 737–745. [Google Scholar] [CrossRef] [PubMed]
- Hachinski, V.; Einhäupl, K.; Ganten, D.; Alladi, S.; Brayne, C.; Stephan, B.C.; Sweeney, M.D.; Zlokovic, B.; Iturria-Medina, Y.; Iadecola, C.; et al. Preventing dementia by preventing stroke: The Berlin Manifesto. Alzheimer’s Dement. 2019, 15, 961–984. [Google Scholar] [CrossRef]
- de Bie, R.M.; Clarke, C.E.; Espay, A.J.; Fox, S.H.; Lang, A.E. Initiation of pharmacological therapy in Parkinson’s disease: When, why, and how. Lancet Neurol. 2020, 19, 452–461. [Google Scholar] [CrossRef] [PubMed]
- Tolosa, E.; Garrido, A.; Scholz, S.W.; Poewe, W. Challenges in the diagnosis of Parkinson’s disease. Lancet Neurol. 2021, 20, 385–397. [Google Scholar] [CrossRef]
- Bandres-Ciga, S.; Diez-Fairen, M.; Kim, J.J.; Singleton, A.B. Genetics of Parkinson’s disease: An introspection of its journey towards precision medicine. Neurobiol. Dis. 2020, 137, 104782. [Google Scholar] [CrossRef]
- McColgan, P.; Tabrizi, S.J. Huntington’s disease: A clinical review. Eur. J. Neurol. 2018, 25, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Tabrizi, S.J.; Leavitt, B.R.; Landwehrmeyer, G.B.; Wild, E.J.; Saft, C.; Barker, R.A.; Blair, N.F.; Craufurd, D.; Priller, J.; Rickards, H.; et al. Targeting huntingtin expression in patients with Huntington’s disease. N. Engl. J. Med. 2019, 380, 2307–2316. [Google Scholar] [CrossRef]
- Valadão, P.A.C.; Santos, K.B.S.; e Vieira, T.H.F.; e Cordeiro, T.M.; Teixeira, A.L.; Guatimosim, C.; de Miranda, A.S. Inflammation in Huntington’s disease: A few new twists on an old tale. J. Neuroimmunol. 2020, 348, 577380. [Google Scholar] [CrossRef]
- Weller, J.; Budson, A. Current understanding of Alzheimer’s disease diagnosis and treatment. F1000Research 2018, 7, F1000 Faculty Rev-1161. [Google Scholar] [CrossRef]
- Alzheimer’s Association. 2018 Alzheimer’s disease facts and figures. Alzheimer’s Dement. 2018, 14, 367–429. [Google Scholar] [CrossRef]
- Breijyeh, Z.; Karaman, R. Comprehensive review on Alzheimer’s disease: Causes and treatment. Molecules 2020, 25, 5789. [Google Scholar] [CrossRef] [PubMed]
- Masrori, P.; Van Damme, P. Amyotrophic lateral sclerosis: A clinical review. Eur. J. Neurol. 2020, 27, 1918–1929. [Google Scholar] [CrossRef] [PubMed]
- Mathis, S.; Goizet, C.; Soulages, A.; Vallat, J.M.; Le Masson, G. Genetics of amyotrophic lateral sclerosis: A review. J. Neurol. Sci. 2019, 399, 217–226. [Google Scholar] [CrossRef]
- Mohassel, P.; Donkervoort, S.; Lone, M.A.; Nalls, M.; Gable, K.; Gupta, S.D.; Foley, A.R.; Hu, Y.; Saute, J.A.M.; Moreira, A.L.; et al. Childhood amyotrophic lateral sclerosis caused by excess sphingolipid synthesis. Nat. Med. 2021, 27, 1197–1204. [Google Scholar] [CrossRef]
- Delatycki, M.B.; Bidichandani, S.I. Friedreich ataxia-pathogenesis and implications for therapies. Neurobiol. Dis. 2019, 132, 104606. [Google Scholar] [CrossRef]
- Tai, G.; Corben, L.A.; Yiu, E.M.; Milne, S.C.; Delatycki, M.B. Progress in the treatment of Friedreich ataxia. Neurol. I Neurochir. Pol. 2018, 52, 129–139. [Google Scholar] [CrossRef]
- Lynch, D.R.; Johnson, J. Omaveloxolone: Potential new agent for Friedreich ataxia. Neurodegener. Dis. Manag. 2021, 11, 91–98. [Google Scholar] [CrossRef]
- Clay, A.; Hearle, P.; Schadt, K.; Lynch, D.R. New developments in pharmacotherapy for Friedreich ataxia. Expert Opin. Pharmacother. 2019, 20, 1855–1867. [Google Scholar] [CrossRef]
- Wirth, B. Spinal muscular atrophy: In the challenge lies a solution. Trends Neurosci. 2021, 44, 306–322. [Google Scholar] [CrossRef]
- Messina, S.; Sframeli, M. New treatments in spinal muscular atrophy: Positive results and new challenges. J. Clin. Med. 2020, 9, 2222. [Google Scholar] [CrossRef] [PubMed]
- Waldrop, M.A.; Karingada, C.; Storey, M.A.; Powers, B.; Iammarino, M.A.; Miller, N.F.; Connolly, A.M. Gene therapy for spinal muscular atrophy: Safety and early outcomes. Pediatrics 2020, 146, e20200729. [Google Scholar] [CrossRef] [PubMed]
- Darryl, C.; Bertini, E.; Swoboda, K.J.; Hwu, W.L.; Crawford, T.O.; Finkel, R.S.; Kirschner, J.; Kuntz, N.L.; Parsons, J.A.; Ryan, M.M.; et al. Nusinersen initiated in infants during the presymptomatic stage of spinal muscular atrophy: Interim efficacy and safety results from the Phase 2 NURTURE study. Neuromuscul. Disord. 2019, 29, 842–856. [Google Scholar]
- Myszczynska, M.A.; Ojamies, P.N.; Lacoste, A.; Neil, D.; Saffari, A.; Mead, R.; Hautbergue, G.M.; Holbrook, J.D.; Ferraiuolo, L. Applications of machine learning to diagnosis and treatment of neurodegenerative diseases. Nat. Rev. Neurol. 2020, 16, 440–456. [Google Scholar] [CrossRef]
- Świetlik, D.; Białowąs, J. Application of artificial neural networks to identify alzheimer’s disease using cerebral perfusion SPECT data. Int. J. Environ. Res. Public Health 2019, 16, 1303. [Google Scholar] [CrossRef] [Green Version]
- Basaia, S.; Agosta, F.; Wagner, L.; Canu, E.; Magnani, G.; Santangelo, R.; Filippi, M.; Alzheimer’s Disease Neuroimaging Initiative. Automated classification of Alzheimer’s disease and mild cognitive impairment using a single MRI and deep neural networks. NeuroImage Clin. 2019, 21, 101645. [Google Scholar] [CrossRef]
- Lins, A.J.C.C.; Muniz, M.T.C.; Garcia, A.N.M.; Gomes, A.V.; Cabral, R.M.; Bastos-Filho, C.J. Using artificial neural networks to select the parameters for the prognostic of mild cognitive impairment and dementia in elderly individuals. Comput. Methods Programs Biomed. 2017, 152, 93–104. [Google Scholar] [CrossRef]
- Pisner, D.A.; Schnyer, D.M. Support Vector Machine. In Machine Learning; Academic Press: Cambridge, MA, USA, 2020; pp. 101–121. [Google Scholar]
- Vichianin, Y.; Khummongkol, A.; Chiewvit, P.; Raksthaput, A.; Chaichanettee, S.; Aoonkaew, N.; Senanarong, V. Accuracy of Support-Vector Machines for Diagnosis of Alzheimer’s Disease, Using Volume of Brain Obtained by Structural MRI at Siriraj Hospital. Front. Neurol. 2021, 12, 481. [Google Scholar] [CrossRef]
- Bharanidharan, N.; Rajaguru, H. Dementia MRI Classification Using Hybrid Dragonfly Based Support Vector Machine. In Proceedings of the 2019 IEEE R10 Humanitarian Technology Conference (R10-HTC)(47129), Depok City, Indonesia, 12–14 November 2019; pp. 45–48. [Google Scholar]
- Battineni, G.; Chintalapudi, N.; Amenta, F. Machine learning in medicine: Performance calculation of dementia prediction by support vector machines (SVM). Inform. Med. Unlocked 2019, 16, 100200. [Google Scholar] [CrossRef]
- Lahmiri, S.; Shmuel, A. Detection of Parkinson’s disease based on voice patterns ranking and optimized support vector machine. Biomed. Signal Process. Control 2019, 49, 427–433. [Google Scholar] [CrossRef]
- Sinaga, K.P.; Yang, M.S. Unsupervised K-means clustering algorithm. IEEE Access 2020, 8, 80716–80727. [Google Scholar] [CrossRef]
- Li, B.; Zhang, Y.; Tang, L.; Gao, C.; Gu, D. Automatic Detection System for Freezing of Gait in Parkinson’s Disease Based on the Clustering Algorithm. In Proceedings of the 2018 2nd IEEE Advanced Information Management, Communicates, Electronic and Automation Control Conference (IMCEC), Xi’an, China, 25–27 May 2018; pp. 1640–1649. [Google Scholar]
- Holilah, D.; Bustamam, A.; Sarwinda, D. Detection of Alzheimer’s disease with segmentation approach using K-Means Clustering and Watershed Method of MRI image. In Journal of Physics: Conference Series; IOP Publishing: Bristol, UK, 2021; Volume 1725, p. 012009. [Google Scholar]
- Schumacher, J.; Peraza, L.R.; Firbank, M.; Thomas, A.J.; Kaiser, M.; Gallagher, P.; O’Brien, J.T.; Blamire, A.M.; Taylor, J.P. Dynamic functional connectivity changes in dementia with Lewy bodies and Alzheimer’s disease. NeuroImage Clin. 2019, 22, 101812. [Google Scholar] [CrossRef] [PubMed]
- Nikas, J.B.; Low, W.C. Application of clustering analyses to the diagnosis of Huntington disease in mice and other diseases with well-defined group boundaries. Comput. Methods Programs Biomed. 2011, 104, e133–e147. [Google Scholar] [CrossRef] [Green Version]
- Izza, Y.; Ignatiev, A.; Marques-Silva, J. On explaining decision trees. arXiv 2020, arXiv:2010.11034. [Google Scholar]
- Cheng, J.; Liu, H.P.; Lin, W.Y.; Tsai, F.J. Identification of contributing genes of Huntington’s disease by machine learning. BMC Med. Genom. 2020, 13, 176. [Google Scholar] [CrossRef] [PubMed]
- Naganandhini, S.; Shanmugavadivu, P. Effective diagnosis of Alzheimer’s disease using modified decision tree classifier. Procedia Comput. Sci. 2019, 165, 548–555. [Google Scholar] [CrossRef]
- Bari Antor, M.; Jamil, A.H.M.; Mamtaz, M.; Monirujjaman Khan, M.; Aljahdali, S.; Kaur, M.; Singh, P.; Masud, M. A comparative analysis of machine learning algorithms to predict alzheimer’s disease. J. Healthc. Eng. 2021, 2021, 9917919. [Google Scholar] [CrossRef] [PubMed]
- Moreira, L.B.; Namen, A.A. A hybrid data mining model for diagnosis of patients with clinical suspicion of dementia. Comput. Methods Programs Biomed. 2018, 165, 139–149. [Google Scholar] [CrossRef]
- Speiser, J.L.; Miller, M.E.; Tooze, J.; Ip, E. A comparison of random forest variable selection methods for classification prediction modeling. Expert Syst. Appl. 2019, 134, 93–101. [Google Scholar] [CrossRef]
- Xu, S.; Pan, Z. A novel ensemble of random forest for assisting diagnosis of Parkinson’s disease on small handwritten dynamics dataset. Int. J. Med. Inform. 2020, 144, 104283. [Google Scholar] [CrossRef]
- Latifah, E.; Abdullah, S.; Soemartojo, S.M. Identifying of factor associated with parkinson’s disease subtypes using random forest. In Journal of Physics: Conference Series; IOP Publishing: Bristol, UK, 2018; Volume 1108, p. 012064. [Google Scholar]
- Byeon, H. Is the random forest algorithm suitable for predicting parkinson’s disease with mild cognitive impairment out of parkinson’s disease with normal cognition? Int. J. Environ. Res. Public Health 2020, 17, 2594. [Google Scholar] [CrossRef] [Green Version]
- Zhao, T.; Hu, Y.; Zang, T.; Cheng, L. Identifying Alzheimer’s disease-related proteins by LRRGD. BMC Bioinform. 2019, 20, 570. [Google Scholar] [CrossRef]
- Berrar, D. Bayes’ Theorem and Naive BAYES Classifier. In Encyclopedia of Bioinformatics and Computational Biology: ABC of Bioinformatics; Elsevier Science Publisher: Amsterdam, The Netherlands, 2018; p. 403. [Google Scholar]
- Zhu, F.; Li, X.; Tang, H.; He, Z.; Zhang, C.; Hung, G.U.; Chiu, P.Y.; Zhou, W. Machine learning for the preliminary diagnosis of dementia. Sci. Program. 2020, 2020, 5629090. [Google Scholar] [CrossRef]
- Yadav, R.; Gautam, A.; Mishra, R.B. Classification of alzheimer using fmri data and brain network. Comput. Sci. Inf. Technol. 2018, 2018, 109–119. [Google Scholar]
- Mostafa, S.A.; Mustapha, A.; Mohammed, M.A.; Hamed, R.I.; Arunkumar, N.; Abd Ghani, M.K.; Jaber, M.M.; Khaleefah, S.H. Examining multiple feature evaluation and classification methods for improving the diagnosis of Parkinson’s disease. Cogn. Syst. Res. 2019, 54, 90–99. [Google Scholar] [CrossRef]
- Gou, J.; Ma, H.; Ou, W.; Zeng, S.; Rao, Y.; Yang, H. A generalized mean distance-based k-nearest neighbor classifier. Expert Syst. Appl. 2019, 115, 356–372. [Google Scholar] [CrossRef]
- Benyoussef, E.M.; Elbyed, A.; El Hadiri, H. 3D MRI classification using KNN and deep neural network for Alzheimer’s disease diagnosis. In Proceedings of the International Conference on Advanced Intelligent Systems for Sustainable Development, Tangier, Morocco, 12–14 July 2018; Springer: Cham, Switzerland, 2018; pp. 154–158. [Google Scholar]
- Durongbhan, P.; Zhao, Y.; Chen, L.; Zis, P.; De Marco, M.; Unwin, Z.C.; Venneri, A.; He, X.; Li, S.; Zhao, Y.; et al. A dementia classification framework using frequency and time-frequency features based on EEG signals. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 826–835. [Google Scholar] [CrossRef] [Green Version]
- Santander-Cruz, Y.; Salazar-Colores, S.; Paredes-García, W.J.; Guendulain-Arenas, H.; Tovar-Arriaga, S. Semantic Feature Extraction Using SBERT for Dementia Detection. Brain Sci. 2022, 12, 270. [Google Scholar] [CrossRef]
- Huang, G.B.; Zhu, Q.Y.; Siew, C.K. Extreme learning machine: Theory and applications. Neurocomputing 2006, 70, 489–501. [Google Scholar] [CrossRef]
- Patil, P.; Kumar, K.; Gaud, N.; Semwal, V.B. Clinical Human Gait Classification: Extreme Learning Machine Approach. In Proceedings of the 2019 1st International Conference on Advances in Science, Engineering and Robotics Technology (ICASERT), Dhaka, Bangladesh, 3–5 May 2019; pp. 1–6. [Google Scholar] [CrossRef]
- Lin, W.; Gao, Q.; Yuan, J.; Chen, Z.; Feng, C.; Chen, W.; Du, M.; Tong, T. Predicting Alzheimer’s disease conversion from mild cognitive impairment using an extreme learning machine-based grading method with multimodal data. Front. Aging Neurosci. 2020, 12, 77. [Google Scholar] [CrossRef] [Green Version]
- Olivares, R.; Munoz, R.; Soto, R.; Crawford, B.; Cárdenas, D.; Ponce, A.; Taramasco, C. An optimized brain-based algorithm for classifying Parkinson’s disease. Appl. Sci. 2020, 10, 1827. [Google Scholar] [CrossRef] [Green Version]
- Gelvez-Almeida, E.; Váasquez-Coronel, A.; Guatelli, R.; Aubin, V.; Mora, M. Classification of Parkinson’s disease patients based on spectrogram using local binary pattern descriptors. In Journal of Physics: Conference Series; IOP Publishing: Bristol, UK, 2022; Volume 2153, p. 012014. [Google Scholar]
- Akusok, A.; Eirola, E.; Björk, K.M.; Miche, Y.; Johnson, H.; Lendasse, A. Brute-force Missing Data Extreme Learning Machine for Predicting Huntington’s Disease. In Proceedings of the 10th International Conference on PErvasive Technologies Related to Assistive Environments, Island of Rhodes, Greece, 21–23 June 2017; pp. 189–192. [Google Scholar]
- Eirola, E.; Akusok, A.; Björk, K.M.; Johnson, H.; Lendasse, A. Predicting Huntington’s Disease: Extreme Learning Machine with Missing Values. In Proceedings of the ELM-2016, Singapore, 13–15 December 2016; Springer: Cham, Switzerland, 2018; pp. 195–206. [Google Scholar]
- Ouali, Y.; Hudelot, C.; Tami, M. An overview of deep semi-supervised learning. arXiv 2020, arXiv:2006.05278. [Google Scholar]
- Zhu, J.; Shi, J.; Liu, X.; Chen, X. Co-training based semi-supervised classification of Alzheimer’s disease. In Proceedings of the 2014 19th International Conference on Digital Signal Processing, Hong Kong, China, 20–23 August 2014; pp. 729–732. [Google Scholar]
- Lipton, Z.C.; Berkowitz, J.; Elkan, C. A critical review of recurrent neural networks for sequence learning. arXiv 2015, arXiv:1506.00019. [Google Scholar]
- Hopfield, J.J. Neural networks and physical systems with emergent collective computational abilities. Proc. Natl. Acad. Sci. USA 1982, 79, 2554–2558. [Google Scholar] [CrossRef]
- Hochreiter, S.; Schmidhuber, J. Long Short-Term Memory. Neural Comput. 1997, 9, 1735–1780. [Google Scholar] [CrossRef]
- Wang, T.; Qiu, R.G.; Yu, M. Predictive modeling of the progression of Alzheimer’s disease with recurrent neural networks. Sci. Rep. 2018, 8, 9161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fang, H.; Si, H.; Chen, L. Recurrent neural network for human activity recognition in smart home. In Proceedings of the 2013 Chinese Intelligent Automation Conference, Yangzhou, China, 1 January 2013; Springer: Berlin/Heidelberg, Germany, 2013; pp. 341–348. [Google Scholar]
- Liang, W.; Zhang, K.; Cao, P.; Liu, X.; Yang, J.; Zaiane, O. Rethinking modeling Alzheimer’s disease progression from a multi-task learning perspective with deep recurrent neural network. Comput. Biol. Med. 2021, 138, 104935. [Google Scholar] [CrossRef]
- Ghazi, M.M.; Nielsen, M.; Pai, A.; Cardoso, M.J.; Modat, M.; Ourselin, S.; Sørensen, L.; Alzheimer’s Disease Neuroimaging Initiative. Training recurrent neural networks robust to incomplete data: Application to Alzheimer’s disease progression modeling. Med. Image Anal. 2019, 53, 39–46. [Google Scholar] [CrossRef] [Green Version]
- Schmidhuber, J. Deep learning in neural networks: An overview. Neural Netw. 2015, 61, 85–117. [Google Scholar]
- Pinaya, W.H.; Scarpazza, C.; Garcia-Dias, R.; Vieira, S.; Baecker, L.; da Costa, P.F.; Redolfi, A.; Frisoni, G.B.; Pievani, M.; Calhoun, V.D.; et al. Normative modelling using deep autoencoders: A multi-cohort study on mild cognitive impairment and Alzheimer’s disease. bioRxiv 2020. [Google Scholar] [CrossRef]
- Kumar, S.; Sotiras, A. NormVAE: Normative Modeling on Neuroimaging Data using Variational Autoencoders. arXiv 2021, arXiv:2110.04903. [Google Scholar]
- Choi, H.; Kang, H.; Lee, D.S.; Alzheimer’s Disease Neuroimaging Initiative. Predicting aging of brain metabolic topography using variational autoencoder. Front. Aging Neurosci. 2018, 10, 212. [Google Scholar] [CrossRef] [Green Version]
- Xiong, Y.; Lu, Y. Deep Feature Extraction From the Vocal Vectors Using Sparse Autoencoders for Parkinson’s Classification. IEEE Access 2020, 8, 27821–27830. [Google Scholar] [CrossRef]
- Mohammadi, A.G.; Mehralian, P.; Naseri, A.; Sajedi, H. Parkinson’s disease diagnosis: The effect of autoencoders on extracting features from vocal characteristics. Array 2021, 11, 100079. [Google Scholar] [CrossRef]
- Menon, S.P. Deep learning for prediction of amyotrophic lateral sclerosis using stacked auto encoders. Int. J. Big Data Manag. 2020, 1, 119–134. [Google Scholar] [CrossRef]
- Hinton, G.E.; Osindero, S.; Teh, Y.W. A fast learning algorithm for deep belief nets. Neural Comput. 2006, 18, 1527–1554. [Google Scholar] [CrossRef]
- Al-Majeed, S.A.; Al-Tamimi, M.S.H. MR Images Classification of Alzheimer’s Disease Based on Deep Belief Network Method. Int. J. Adv. Sci. Technol. 2020, 29, 3078–3088. [Google Scholar]
- An, N.; Jin, L.; Ding, H.; Yang, J.; Yuan, J. A deep belief network-based method to identify proteomic risk markers for Alzheimer disease. arXiv 2020, arXiv:2003.05776. [Google Scholar]
- Shen, T.; Jiang, J.; Lu, J.; Wang, M.; Zuo, C.; Yu, Z.; Yan, Z. Predicting Alzheimer Disease From Mild Cognitive Impairment With a Deep Belief Network Based on 18F-FDG-PET Images. Mol. Imaging 2019. [Google Scholar] [CrossRef]
- Nilashi, M.; Ahmadi, H.; Sheikhtaheri, A.; Naemi, R.; Alotaibi, R.; Alarood, A.A.; Munshi, A.; Rashid, T.A.; Zhao, J. Remote tracking of Parkinson’s disease progression using ensembles of deep belief network and self-organizing map. Expert Syst. Appl. 2020, 159, 113562. [Google Scholar] [CrossRef]
- Valueva, M.V.; Nagornov, N.N.; Lyakhov, P.A.; Valuev, G.V.; Chervyakov, N.I. Application of the residue number system to reduce hardware costs of the convolutional neural network implementation. Math. Comput. Simul. 2020, 177, 232–243. [Google Scholar] [CrossRef]
- Fukushima, K. Neocognitron: A self-organizing neural network model for a mechanism of pattern recognition unaffected by shift in position. Biol. Cybern. 1980, 36, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Hussain, E.; Hasan, M.; Hassan, S.Z.; Azmi, T.H.; Rahman, M.A.; Parvez, M.Z. Deep learning based binary classification for alzheimer’s disease detection using brain mri images. In Proceedings of the 2020 15th IEEE Conference on Industrial Electronics and Applications (ICIEA), Kristiansand, Norway, 9–13 November 2020; pp. 1115–1120. [Google Scholar]
- Yue, L.; Gong, X.; Chen, K.; Mao, M.; Li, J.; Nandi, A.K.; Li, M. Auto-Detection of Alzheimer’s Disease Using Deep Convolutional Neural Networks. In Proceedings of the 2018 14th International Conference on Natural Computation, Fuzzy Systems and Knowledge Discovery (ICNC-FSKD), Huangshan, China, 28–30 July 2018; pp. 228–234. [Google Scholar] [CrossRef]
- Islam, J.; Zhang, Y. Brain MRI analysis for Alzheimer’s disease diagnosis using an ensemble system of deep convolutional neural networks. Brain Inform. 2018, 5, 2. [Google Scholar] [CrossRef] [Green Version]
- Frid, A.; Kantor, A.; Svechin, D.; Manevitz, L.M. Diagnosis of Parkinson’s disease from continuous speech using deep convolutional networks without manual selection of features. In Proceedings of the 2016 IEEE International Conference on the Science of Electrical Engineering (ICSEE), Eilat, Israel, 16–18 November 2016; pp. 1–4. [Google Scholar]
- Pereira, C.R.; Pereira, D.R.; Papa, J.P.; Rosa, G.H.; Yang, X.S. Convolutional neural networks applied for Parkinson’s disease identification. In Machine Learning for Health Informatics; Springer: Cham, Switzerland, 2016; pp. 377–390. [Google Scholar]
- Lee, T.; Sung, M.K.; Lee, S.; Yang, W.; Oh, J.; Kim, J.Y.; Hwang, S.; Ban, H.-J.; Choi, J.K. Convolutional neural network model to predict causal risk factors that share complex regulatory features. Nucleic Acids Res. 2019, 47, e146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samek, W.; Montavon, G.; Lapuschkin, S.; Anders, C.J.; Müller, K.R. Explaining deep neural networks and beyond: A review of methods and applications. Proc. IEEE 2021, 109, 247–278. [Google Scholar] [CrossRef]
- Wroge, T.J.; Özkanca, Y.; Demiroglu, C.; Si, D.; Atkins, D.C.; Ghomi, R.H. Parkinson’s disease diagnosis using machine learning and voice. In Proceedings of the 2018 IEEE Signal Processing in Medicine and Biology Symposium (SPMB), Philadelphia, PA, USA, 1 December 2018; pp. 1–7. [Google Scholar]
- Li, H.; Parikh, N.A.; He, L. A novel transfer learning approach to enhance deep neural network classification of brain functional connectomes. Front. Neurosci. 2018, 12, 491. [Google Scholar] [CrossRef] [Green Version]
- Yin, B.; Balvert, M.; van der Spek, R.A.; Dutilh, B.E.; Bohté, S.; Veldink, J.; Schönhuth, A. Using the structure of genome data in the design of deep neural networks for predicting amyotrophic lateral sclerosis from genotype. Bioinformatics 2019, 35, i538–i547. [Google Scholar] [CrossRef]
- Noor, M.B.T.; Zenia, N.Z.; Kaiser, M.S.; Mamun, S.A.; Mahmud, M. Application of deep learning in detecting neurological disorders from magnetic resonance images: A survey on the detection of Alzheimer’s disease, Parkinson’s disease and schizophrenia. Brain Inform. 2020, 7, 11. [Google Scholar] [CrossRef]
- Kshirsagar, P.R.; Akojwar, S.G.; Bajaj, N.D. A hybridised neural network and optimisation algorithms for prediction and classification of neurological disorders. Int. J. Biomed. Eng. Technol. 2018, 28, 307–321. [Google Scholar] [CrossRef]
- Ahmadlou, M.; Adeli, H. Enhanced probabilistic neural network with local decision circles: A robust classifier. Integr. Comput.-Aided Eng. 2010, 17, 197–210. [Google Scholar] [CrossRef]
- Hirschauer, T.J.; Adeli, H.; Buford, J.A. Computer-aided diagnosis of Parkinson’s disease using enhanced probabilistic neural network. J. Med. Syst. 2015, 39, 179. [Google Scholar] [CrossRef] [PubMed]
- Ramzan, F.; Khan, M.U.G.; Rehmat, A.; Iqbal, S.; Saba, T.; Rehman, A.; Mehmood, Z. A deep learning approach for automated diagnosis and multi-class classification of Alzheimer’s disease stages using resting-state fMRI and residual neural networks. J. Med. Syst. 2020, 44, 37. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Wu, P.; Wang, J.; Li, H.; Navab, N.; Yakushev, I.; Weber, W.; Schwaiger, M.; Huang, S.C.; Cumming, P.; et al. A 3d Deep Residual Convolutional Neural Network for Differential Diagnosis of Parkinsonian Syndromes on 18F-fdg pet images. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 3531–3534. [Google Scholar]
- Pasluosta, C.F.; Gassner, H.; Winkler, J.; Klucken, J.; Eskofier, B.M. An Emerging Era in the Management of Parkinson’s Disease: Wearable Technologies and the Internet of Things. IEEE J. Biomed. Health Inform. 2015, 19, 1873–1881. [Google Scholar] [CrossRef] [PubMed]
- Romero, L.E.; Chatterjee, P.; Armentano, R.L. An IoT approach for integration of computational intelligence and wearable sensors for Parkinson’s disease diagnosis and monitoring. Health Technol. 2016, 6, 167–172. [Google Scholar] [CrossRef]
- Dhyani, K.; Bhachawat, S.; Prabhu, J.; Kumar, M.S. A Novel Survey on Ubiquitous Computing. In Data Intelligence and Cognitive Informatics; Springer: Singapore, 2022; pp. 109–123. [Google Scholar]
- Kuosmanen, E.; Kan, V.; Visuri, A.; Vega, J.; Nishiyama, Y.; Dey, A.K.; Harper, S.; Ferreira, D. Mobile-based Monitoring of Parkinson’s Disease. In Proceedings of the 17th International Conference on Mobile and Ubiquitous Multimedia, Cairo, Egypt, 25–28 November 2018; pp. 441–448. [Google Scholar]
- Orlosky, J.; Itoh, Y.; Ranchet, M.; Kiyokawa, K.; Morgan, J.; Devos, H. Emulation of Physician Tasks in Eye-Tracked Virtual Reality for Remote Diagnosis of Neurodegenerative Disease. IEEE Trans. Vis. Comput. Graph. 2017, 23, 1302–1311. [Google Scholar] [CrossRef]
- Ramar, R.; Muthammal, S.; Dhamodharan, T.; Rajendran, G.K. Modelling Alzheimer’s People Brain Using Augmented Reality for Medical Diagnosis Analysis. In Proceedings of the International Conference on Intelligent Human Systems Integration, Modena, Italy, 19–21 February 2020; Springer: Cham, Switzerland, 2020; pp. 524–531. [Google Scholar]
- Kim, O.; Pang, Y.; Kim, J.H. The effectiveness of virtual reality for people with mild cognitive impairment or dementia: A meta-analysis. BMC Psychiatry 2019, 19, 219. [Google Scholar] [CrossRef] [Green Version]
- Astell, A.J.; Bouranis, N.; Hoey, J.; Lindauer, A.; Mihailidis, A.; Nugent, C.; Robillard, J.M. Technology and dementia: The future is now. Dement. Geriatr. Cogn. Disord. 2019, 47, 131–139. [Google Scholar] [CrossRef]
- Garrido, S.; Dunne, L.; Perz, J.; Chang, E.; Stevens, C.J. The use of music in aged care facilities: A mixed-methods study. J. Health Psychol. 2020, 25, 1425–1438. [Google Scholar] [CrossRef]
- Deetjen, U.; Meyer, E.T.; Schroeder, R. Big data for advancing dementia research: An evaluation of data sharing practices in research on age-related neurodegenerative diseases. In OECD Digital Economy Papers; OECD Publishing: Paris, France, 2015. [Google Scholar]
- Munir, K.; de Ramón-Fernández, A.; Iqbal, S.; Javaid, N. Neuroscience patient identification using big data and fuzzy logic—An Alzheimer’s disease case study. Expert Syst. Appl. 2019, 136, 410–425. [Google Scholar] [CrossRef]
- Chen, P.H.; Yang, F.Y.; Lee, D.D.; Yang, M.H. Data mining the comorbid associations between dementia and various kinds of illnesses using a medicine database. Comput. Electr. Eng. 2018, 70, 12–20. [Google Scholar] [CrossRef]
- Swarna, S.R.; Kumar, A.; Dixit, P.; Sairam, T.V.M. Parkinson’s Disease Prediction using Adaptive Quantum Computing. In Proceedings of the 2021 Third International Conference on Intelligent Communication Technologies and Virtual Mobile Networks (ICICV), Tirunelveli, India, 4–6 February 2021; pp. 1396–1401. [Google Scholar]
- Walsh, J.R.; Smith, A.M.; Pouliot, Y.; Li-Bland, D.; Loukianov, A.; Fisher, C.K. Generating digital twins with multiple sclerosis using probabilistic neural networks. arXiv 2020, arXiv:2002.02779. [Google Scholar]
- Keller, M.; Pastro, V.; Rotaru, D. Overdrive: Making SPDZ great again. In Proceedings of the Annual International Conference on the Theory and Applications of Cryptographic Techniques, Tel Aviv, Israel, 29 April 29–3 May 2018; Springer: Cham, Switzerland; pp. 158–189. [Google Scholar]
- Scheibner, J.; Raisaro, J.L.; Troncoso-Pastoriza, J.R.; Ienca, M.; Fellay, J.; Vayena, E.; Hubaux, J.P. Revolutionizing medical data sharing using advanced privacy-enhancing technologies: Technical, legal, and ethical synthesis. J. Med. Internet Res. 2021, 23, e25120. [Google Scholar] [CrossRef] [PubMed]







| Ref | Degenerative Nerve Diseases | Machine Learning Approaches Used | Learning Model | Dataset Used | Pre-Trained or Not | Key Contribution | Limitations | Metrics |
|---|---|---|---|---|---|---|---|---|
| [36] | Alzheimer’s disease | Artificial neural network | Supervised learning | Collected their own private dataset | Not pre-trained | Uses brain SPECT records of the patient to get a much more accurate result. | No significant difference in the sensitivity in comparison with discriminatory analysis. | Sensitivity: 93.8% Specificity: 100% |
| [37] | Alzheimer’s disease | Neural network | Supervised learning | ADNI dataset ADNI + Milan dataset | Pre-trained | A single cross section of a brain MRI scan is fed to the model to predict whether the subject has Alzheimer’s or not. | The model was not tested while considering cognitive and genetic biomarkers. | For ADNI dataset: Accuracy: 99.2% Sensitivity: 98.9% Specificity: 99.5% For ADNI + Milan dataset: Accuracy: 98.2% Sensitivity: 98.1% Specificity: 98.3% |
| [40] | Alzheimer’s disease | Support vector machine | Supervised learning | Collected their own private dataset | Not pre-trained | This paper studied patients of Alzheimer’s in Thailand using SVMs and concluded that the hippocampus is a good classifier, producing high accuracy. | The subjects studied were not critically affected by Alzheimer’s. Additionally, the number of subjects used for this study was low and not sufficient enough for proper testing. | Accuracy: 62.64% On using clinical parameters: - Accuracy: 83–90% |
| [41] | Dementia | Support vector machine | Supervised learning | OASIS | Not pre-trained | By combining SVM with DA, good accuracy is obtained. | Large kernel scale reduces sensitivity. | Only SVM: Accuracy: 67.57% SVM with DA: Accuracy: 81.08% SVM with PCA: Accuracy: 70.27% |
| [42] | Dementia | Support vector machine | Supervised learning | OASIS | Not pre-trained | Low gamma values as well as high regularized values are exhibiting better results. | The classification of the subject groups is not precise in some cases. | Accuracy: Nearly 70% Sensitivity: 65–82% |
| [45] | Parkinson’s disease | K-means clustering | Unsupervised learning | Collected their own private dataset | Pre-trained | Clusters formed are given to the FOG detection system in a random order. | Sampling frequency was not high so it resulted in fewer data to be updated. | Accuracy: 93.2% Sensitivity: 92.4% Specificity: 94.9% |
| [46] | Alzheimer’s disease | K-means clustering | Unsupervised learning | OASIS | Not pre-trained | Top- and bottom-hat filtering is used to increase MRI image quality which was then fed to the system. | The Watershed method is not able to segment more objects. | N/A |
| [47] | Dementia | K-means clustering | Unsupervised learning | Collected their own private dataset | N/A | A combination of the sliding window approach, k-means clustering, and dynamic network analyses was used. | Patients on dopaminergic medication were not detected by the model. | N/A |
| [50] | Huntington’s disease | Decision tree | Supervised learning | NCBI GSE33000 | Not pre-trained | A heterogeneous model, including random forest and rule induction models. | The mutant HTT gene may interfere with the promotion of Huntington’s disease pathogenesis. | Accuracy: 90.79 ± 4.57% Precision: 87.26 ± 6.95% Sensitivity/recall: 96.17 ± 3.30% |
| [51] | Alzheimer’s disease | Decision tree | Supervised learning | OASIS | Not pre-trained | Optimized using entropy and information gain. | Identification of symptoms to detect at an early stage. | Accuracy: 99.1% |
| [52] | Alzheimer’s disease | Decision tree | Supervised learning | OASIS | Not pre-trained | The model proposed was trained without fine tuning and then utilized the grid search to find the best possible parameters to fine tune. | Had a lower accuracy rate in comparison with other models. | Training accuracy: 100% Testing accuracy: 72% Test recall: 67% |
| [55] | Parkinson’s disease | Random forest | Supervised learning | NewHandPD | Not pre-trained | Combined with PCA, used to make a prediction based on handwritten data of the patients. | No general feature extraction method for different handwritings improved final voting performance. | Accuracy: 89.4% Specificity: 93.7% Sensitivity: 84.5% F1-Score: 87.7% |
| [56] | Parkinson’s disease | Random forest | Supervised learning | PPMI | Not pre-trained | Bootstrapping is performed where a random sample is taken from the available samples with replacement of data. | The decision trees might be open to overfitting. | Accuracy: 94.48% |
| [57] | Parkinson’s disease | Random forest | Supervised learning | Parkinson’s Dementia Clinical Epidemiology Data | Not pre-trained | Used explanatory variables that were randomly chosen from the samples. | A weighted voting system needs to be used to obtain a higher accuracy. | Accuracy: 65.6% Sensitivity: 70.6% Specificity: 60.0% |
| [60] | Dementia | Naïve Bayes | Supervised learning | Register based database of the Show Chwan health system | Not pre-trained | Multiplied the class prior probability with the likelihood of the disease in the datasets of the patients. | The study conducted may show selection bias. | Sensitivity: 92% Specificity: 95% |
| [61] | Alzheimer’s disease | Naïve Bayes | Supervised learning | OASIS | Not pre-trained | Processed MRI features are taken in partition vectors to feed the model. | Blood cell content, protein–protein and gene–gene interactions, etc., data were not incorporated. | Accuracy: 90% |
| [62] | Parkinson’s disease | Naïve Bayes | Supervised learning | - | Not pre-trained | Used a multi-feature evaluation approach. | May have some fluctuations that affect the final output. | Accuracy: 89.34% Recall: 89.3% Precision: 89.8% |
| [71] | Parkinson’s disease | Extreme learning machine | Hybrid of both supervised and unsupervised learning | Parkinson’s voice database | Pre-trained | Uses local binary pattern descriptors. | Not yet tested with databases of large-scale images. | Accuracy: 92.59% |
| [72] | Huntington’s disease | Extreme learning machine | Supervised learning | The HD dataset | Pre-trained | Imputes missing values using previously observed features. | The quality of prediction decreases as larger time intervals are taken into consideration. | F1 score: 91.9 ± 2.4% |
| [75] | Alzheimer’s disease | Co-training classification | Semi-supervised learning | ADNI | Not pre-trained | Uses multimodal neuroimaging data. | Various other co-training algorithms can be evaluated to improve the performance of the proposed system. | Accuracy: 92.91 ± 1.48% Sensitivity: 95.20 ± 1.63% Specificity: 90.70 ± 2.20% |
| Ref | Degenerative Nerve Diseases | Deep Learning Approach Used | Learning Model | Dataset Used | Pre-Trained or Not | Key Contribution | Limitations | Metrics |
|---|---|---|---|---|---|---|---|---|
| [79] | Alzheimer’s disease | Recurrent neural network | Supervised learning | NACC | Not pre-trained | An enhanced “many-to-one” RNN architecture is used to support the shift of time steps. This allows considering irregular visits of the patient. | The model is not equipped for early-stage predictions, which are important for beginning early treatment of the disorder. | Accuracy: 99.06 ± 0.43% |
| [85] | Alzheimer’s disease | Deep autoencoders | Unsupervised learning | ADNI | Not pre-trained | Generates accurate deviation maps and overcomes normative model variational autoencoders to estimate patient-level deviations with uncertainty estimates and also overcame the limitations of other approaches where subject-level deviations were found, which were supposed to be deterministic. | The generalizability of the approach is not yet validated. | N/A |
| [87] | Parkinson’s disease | Deep autoencoders | Unsupervised learning | PD dataset from database | Not pre-trained | Vocal impairments can be identified using sparse autoencoders. | Performance might not be the same if availability of data is not abundant. | Accuracy: 95% Sensitivity: 96% Specificity: 98% |
| [88] | Amyotrophic lateral sclerosis | Deep autoencoders | Unsupervised learning | PD dataset from UCI database | Not pre-trained | Uses deep autoencoders to denoise raw data. | Lack of availability of datasets decreases the scalability of the method. | Accuracy: 91.53% F1 score: 94.36% |
| [89] | Amyotrophic lateral sclerosis | Deep autoencoders | Unsupervised learning | PRO_ACT database | Not pre-trained | Uses stacked autoencoders to denoise raw available data. | Availability of better data must always be abundant to improve accuracy. | Accuracy: 87% |
| [94] | Parkinson’s disease | Deep belief network | Unsupervised learning | PD dataset from UCI database | Pre-trained | Hybrid of clustering and deep belief network was used with the aid of support vector regression. Self-organizing maps were also used to improve accuracy and scalability. | The dataset used had a limited number of features; hence, other datasets might show varied results. A supervised learning technique was used. | N/A |
| [97] | Alzheimer’s disease | Deep convolutional network | Supervised learning | OASIS | Pre-trained | Used a 12-layer CNN on brain MRI data to detect and classify Alzheimer’s disease. | Does not support multi-class classification. | Accuracy: 97.75% Demented Recall: 92% Non-demented Recall: 100% Demented Precision: 100% Non-demented Precision: 93% Demented F1 score: 97% Non-demented F1 score: 98% |
| [100] | Parkinson’s disease | Deep convolutional network | Supervised learning | Collected data on their own | Not pre-trained | Automating the process of diagnosis from continuous native speech with a relatively small set of training samples. | This model’s operation was considerably slow as it took longer training time. | Accuracy: 83.63% |
| [101] | Parkinson’s disease | Deep convolutional network | Supervised learning | HandPD | Not pre-trained | Extraction of features from various handwritings. | Slow speed of operations and large training time. | Accuracy: 78.18% |
| [102] | Amyotrophic lateral sclerosis | Deep convolutional network | Supervised learning | GWAS | Pre-trained | Use of CNN with vectors for predicting the recurring sequence of patterns in DNA and RNA binding proteins. The model also incorporated external domain knowledge, which aided in achieving higher performance. | The model assumed that the locus contains at least one casual variant; hence, the presence of false-positive GWAS signals may lead to significant loss in performance. | N/A |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bhachawat, S.; Shriram, E.; Srinivasan, K.; Hu, Y.-C. Leveraging Computational Intelligence Techniques for Diagnosing Degenerative Nerve Diseases: A Comprehensive Review, Open Challenges, and Future Research Directions. Diagnostics 2023, 13, 288. https://doi.org/10.3390/diagnostics13020288
Bhachawat S, Shriram E, Srinivasan K, Hu Y-C. Leveraging Computational Intelligence Techniques for Diagnosing Degenerative Nerve Diseases: A Comprehensive Review, Open Challenges, and Future Research Directions. Diagnostics. 2023; 13(2):288. https://doi.org/10.3390/diagnostics13020288
Chicago/Turabian StyleBhachawat, Saransh, Eashwar Shriram, Kathiravan Srinivasan, and Yuh-Chung Hu. 2023. "Leveraging Computational Intelligence Techniques for Diagnosing Degenerative Nerve Diseases: A Comprehensive Review, Open Challenges, and Future Research Directions" Diagnostics 13, no. 2: 288. https://doi.org/10.3390/diagnostics13020288