
The Impact of a Positive Biofire® FilmArray® Gastrointestinal Panel Result on Clinical Management and Outcomes


1
Azrieli Faculty of Medicine, Bar-Ilan University, Safed 1311502, Israel
2
The Clinical Microbiology Laboratory, Tzafon Medical Center, Poriya, Tiberias 1528001, Israel
*
Author to whom correspondence should be addressed.
†
These authors contributed equally to this work.
Diagnostics 2023, 13(6), 1094; https://doi.org/10.3390/diagnostics13061094
Submission received: 7 February 2023
/
Revised: 2 March 2023
/
Accepted: 10 March 2023
/
Published: 14 March 2023
(This article belongs to the Section Diagnostic Microbiology and Infectious Disease)
Abstract
:The gold standard diagnostic method for gastrointestinal infections is stool culture, which has limited sensitivity and long turnaround time. Infection diagnosis recently shifted to syndrome-based panel assays. This study employed the FilmArray® Gastrointestinal Panel, which detects 22 pathogens simultaneously, to investigate gastrointestinal infection and pathogen distribution in 91 stool samples of patients hospitalized at the Tzafon Medical Center, Israel, during 2020, and to compare the clinical and demographic data of negative vs. positive samples. Among the 61 positive samples (67%), the most common pathogen was Campylobacter (34.4%). Positive test results were associated with a slightly younger patient age (p = 0.012), significantly higher post-diagnosis use of antibiotics (63.9% vs. 36.7%; p = 0.014), and shorter length of stay and time to discharge (p = 0.035, p = 0.003, respectively) than negative test results. To conclude, the FilmArray® Gastrointestinal Panel enabled the early identification of causative infectious agents and enhanced clinical management and outcomes.
1. Introduction
Gastrointestinal infections (GIs) pose a global threat to public health and are associated with high rates of morbidity and mortality [1]. According to the results of the Global Burden of Disease Study 2016, acute gastroenteritis was responsible for approximately 89.5 million disability-adjusted life years lost and 1.45 million deaths per year [2]. In the United States, about 179 million people suffer from diarrheal illnesses each year [3].
GIs have been linked to the development of other health conditions, such as Reiter’s syndrome, Guillain–Barré syndrome and irritable bowel syndrome (IBS) [4,5]. Symptoms may include vomiting, diarrhea, abdominal pain and fever [6].
Given the nonspecific signs presented in GIs, the etiology is often unknown. Primary treatment, based on clinical manifestations, may include the use of antimicrobial agents [7]. However, inappropriate antibiotic use may lead to the emergence of multidrug-resistant organisms, especially among vulnerable populations [7,8]. Furthermore, in viral gastroenteritis or uncomplicated bacterial gastroenteritis, antibiotics can be harmful. For example, in non-typhoid Salmonella infections, antibiotics increase the risk of disease relapse and prolonged carriage, and in Shiga-toxin-producing Escherichia coli (E. coli) infections, antibiotics elevate the risk of hemolytic uremic syndrome [6]. Therefore, an accurate diagnosis is critical in order to assure etiology-directed treatment regimens and reduce any possible complications.
A wide range of pathogens has been attributed to GI etiology [9,10]. In bacterial gastroenteritis, the gold standard diagnostic method is stool culture [11]. However, this technique is limited due to the fact that some bacteria have non-conventional growth requirements; the time to result is usually long (2–5 days), and inappropriate sample handling is possible and might affect the result, as in cases of collecting the stool sample after antibiotic treatment onset.
Other conventional diagnostic methods include microscopic examination for parasitic pathogens and enzyme immunoassays (EIAs), which are used to identify viral, bacterial and parasitic infections [11].
In recent years, there has been an applicative leap in infectious disease diagnostics, from traditional to syndromic-based diagnosis, using molecular assays that simultaneously detect several pathogens including viruses, fungi, parasites and bacteria within a few hours [12]. One such platform is the Biofire® FilmArray® (BioFire® Diagnostics, Inc., Salt Lake City, UT, USA), which provides different panels for the detection of common pathogens associated with diverse infectious conditions, including respiratory tract infections, meningitis and GIs.
The FilmArray® Gastrointestinal Panel (GIP) has the most comprehensive array of targets (22 in total), checking for bacteria, viruses and parasites known to cause IGE. Different works have shown that the specificity and sensitivity of the GIP are 97.1% and 94.5–100%, respectively [11,13]. The run time is about an hour, and the required amount of sample is small (200 μL). This technology carries out nucleic acid extraction followed by polymerase chain reaction (PCR) in which different DNA targets are amplified and detected [11]. Thus, it screens multiple pathogens within a single test run, has high detection rates and wide detection coverage. However, its main disadvantage is its high cost and the lack of interpretable quantification [11,14].
The current study investigated GI pathogens’ distribution in stool samples of patients who were hospitalized at the Tzafon Medical Center, Poriya, Israel, during 2020. Clinical and demographic data of patients with negative vs. positive GIP were compared and the antibiotic status was thoroughly examined (including changes in antibiotic treatment after the test result and antibiotic treatment at discharge). The main aim of this study was to assess the impact of a positive GIP result on clinical management and outcome. We found that a positive GIP result was significantly associated with a higher post-diagnosis use of antibiotics (63.9% vs. 36.7%), and a shorter length of stay and time to discharge (p = 0.035, p= 0.003, respectively) than a negative GIP result. Therefore, the early identification of GI pathogens by the FilmArray® Gastrointestinal Panel enhances clinical management and outcomes.
2. Materials and Methods
2.1. Study Design
This study retrospectively analyzed 91 records of patients, aged 0–100 years, who were admitted to the Tzafon Medical Center, Poriya, Israel, during 2020, with a suspicion of IGE. Stool samples were collected as part of the routine medical care service and tested with the Biofire® FilmArray® GIP following the request of an infectious disease specialist. Clinical and demographic data were collected from patients’ medical records including age, ethnicity, gender, chronic diseases, acute complications, vaccination status (the routinely administered vaccines in Israel), time passed from hospitalization to GIP test, time passed from GIP test result to discharge from hospital, length of stay (LOS), death during hospitalization and whether GIP result has led to discharge. In addition, data concerning antibiotic status were collected including antibiotics administration before and after test result, changes in antibiotic treatment following the test result and treatment on discharge. The study was approved by the institutional review board (IRB) of the Tzafon Medical Center, approval no. POR-0105-20. The IRB waived the need for informed consent.
2.2. Sample Collection and Biofire® FilmArray® GIP Test
Stool samples were collected and sent to the clinical microbiology laboratory at the medical center. Each sample was tested by the Biofire® FilmArray® GIP according to the manufacturer’s instructions. Briefly, stool samples were transported into Cary Blair transport media (FecalSwab, Copan Diagnostics Inc., Murrieta, CA, USA) and the tube was inverted several times. Afterwards, a hydration solution was injected into the FilmArray® GI pouch, 200 μL of sample were mixed with the provided buffer and the mixture was injected into the test pouch (provided with all necessary reagents in a freeze-dried state). The pouch was inserted into the instrument. At the end of each run (~1 h per each sample), results were presented on the computer’s software; when pathogen was detected, the software introduced the pathogen name on the computer screen. When no pathogen was detected, a “Negative” result was presented. A positive result was reported to the clinical staff by phone.
The Biofire® FilmArray® system detects seven bacteria: Campylobacter jejuni (C. jejuni), Campylobacter Coli (C. coli), Campylobacter upsaliensis (C. upsaliensis), Clostridiodes difficile (C. difficile), Plesiomonas shigelloides (P. shigelloides), Salmonella spp., Yersenia enterocolitica (Y. enterocolitica), Vibrio parahaemolyticus (V. parahaemolyticus), Vibrio vulnificus (V. vulnificus), and Vibrio cholera (V. cholera); six diarrheagenic Shigella spp./E. coli: enteroaggregative E. coli (EAEC), enteropathogenic E. coli (EPEC), enterotoxigenic E.coli (ETEC), Shiga-like toxin producing E. coli (STEC), E. coli O157, and enteroinvasive E. coli (EIEC)/Shigella spp.; four parasites: Cryptosporidium, Cyclospora cayetanensis (C. cayetanensis), Entamoeba histolytica (E. histolytica), and Giardia lamblia (G. lamblia); and five viruses: Adenovirus F 40/41, Astrovirus, Norovirus GI/GII, Rotavirus A and Sapovirus [13].
2.3. Stool Culture
Stool samples were cultured as part of the routine GI diagnosis in Israel, which included testing for Salmonella, Shigella and Campylobacter. To this end, all study specimens were inoculated on Xylose Lysin Deoxycholate (XLD) agar (Hylabs Ltd., Rehovot, Israel) and Salmonella Shigella (SS) agar (Hylabs Ltd.) and incubated at 37 °C for the detection of Salmonella and Shigella. Samples were also inoculated on Campylobacter CVA agar (Hylabs Ltd.) and incubated at 42 °C under microaerophilic conditions for the detection of Campylobacter. After 48 h incubation, suspicious colonies were further identified using the Matrix-Assisted Laser Desorption Ionization–Time of Flight (MALDI–TOF) technique by the Bruker Biotyper system (Bruker Daltonics, Bremen, Germany) [15].
2.4. Statistical Analysis
The study patients were grouped according to their GIP result into positive (GIP+) and negative (GIP−) groups. All measured variables and derived parameters were tabulated by descriptive statistics. Chi-squared test was applied for assessing the difference in categorial variables between the two groups. The two-sample t-test for independent groups was applied for testing the statistical significance of the difference in quantitative measurements between the study groups.
All tests were two-tailed, and a p-value of 5% or less was considered statistically significant.
The data were analyzed using the R ® software 9.4 (R score team, 2022).
3. Results
This study included records of 91 patients; 61 (67%) had a positive GIP result and 30 (33%) had a negative result.
3.1. Distribution of Causative Agents
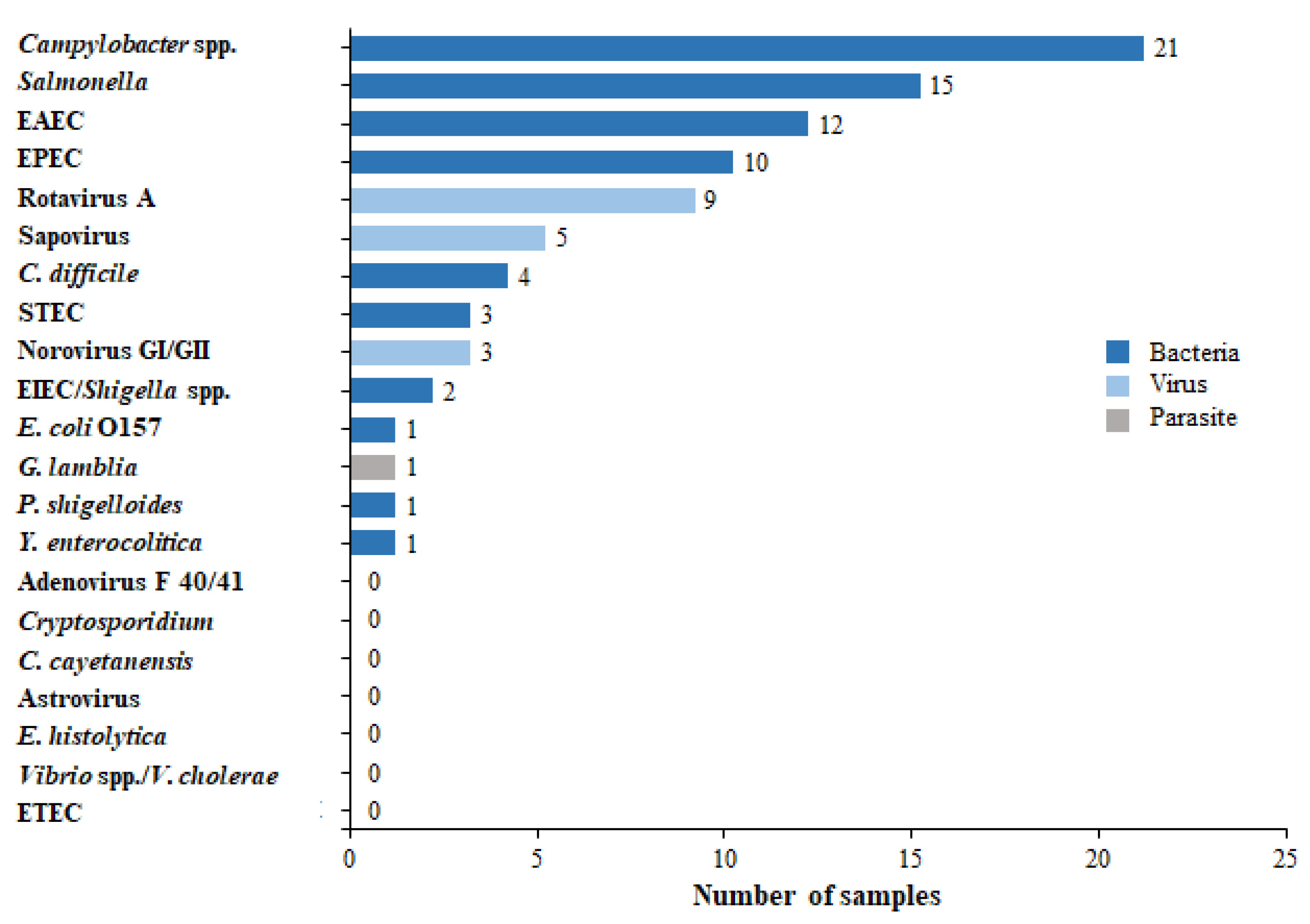
A total of 88 pathogens were detected in the 61 positive samples. Among the 61 positive results, 43 (70.5%) were attributed to bacterial etiology with the most common bacteria being Campylobacter (21/43, 48.8%) and Salmonella (15/43, 34.9%) (Figure 1); 17 (27.9%) patients had a viral etiology, with the most common viruses being Rotavirus (9/17, 52.9%) and Sapovirus (5/17, 29.4%); and only one parasite (1/61, 1.6%) was detected—G. lamblia.
3.2. Comparison of Culture and GIP Test Results
We found a significant association between the GIP result and the stool culture result (p = 0.0176). Within the GIP+ group, Campylobacter was detected in 12 (19.7%) specimens and Salmonella in 9 (14.7%). No pathogens were detected in stool cultures within the GIP− group. Blood cultures were performed for 68 patients. Within the GIP+ group, one sample was positive for Salmonella.
3.3. Coinfections
Of the 61 GIP+ group patients, 23 (37.7%) had multiple pathogens detected, with either 2, 3 or 4 pathogens detected in 20 (32.8%), 1 (4.3%) and 1 (4.3%) of the positive specimens, respectively (Figure 2).
The most common pathogens detected as coinfections were EAEC and EPEC, found in 4 (17.4%) specimens, followed by Campylobacter and EAEC in 3 samples (13%).
3.4. Distribution of Causative Agents, Per Age Groups
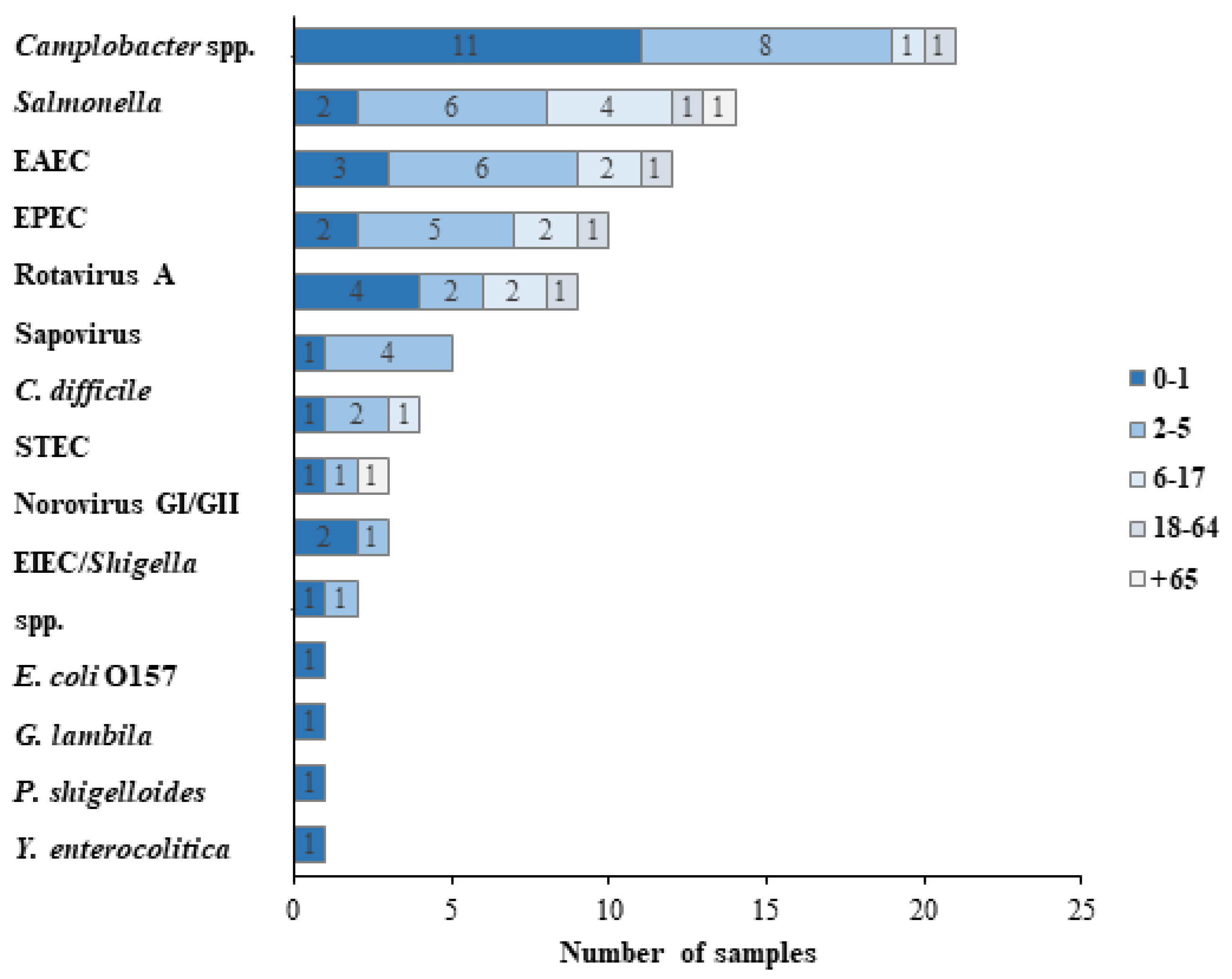
The analysis of pathogens by age group showed that 21 (34.4%) patients in the GIP+ group were under the age of 1 year, 23 (37.7%) were in the range of 2–5 years, 10 (16.4%) were between 6 to 17 years, 4 (6.5%) were older than 18 years and younger than 65 (18–64), and 2 (3.3%) were older than 65 (65+) (Figure 3).
Within the 0–1 group, the most common pathogen was Campylobacter (11/21, 52.4%), followed by Rotavirus A (4/21, 19%). Similarly, Campylobacter was the most prevalent agent within the 2–5 group (8/23, 34.8%), followed by Salmonella (6/23, 26.1%) and EAEC (6/23, 26.1%). Within the 6–17 group, the most common pathogen was Salmonella (4/10, 40%).
3.5. General Demographic and Clinical Data of Patients with a Positive Result vs. a Negative Result of the Gastrointestinal Panel
No significant differences were found between the positive and negative GIP groups in terms of ethnicity, gender, vaccination status and chronic disease (Table 1). Thirty-one (50.8%) patients in the GIP+ group were males, 60.7% were Arabs, 96.7% were vaccinated, and 8.2% had a chronic disease. In the GIP− group, most (60%) patients were female, 56.7% were Jewish, and 10% had a chronic disease.
In contrast, we found a significant association between the GIP result and the patient’s age, with the GIP+ patients being a bit younger (p = 0.012). The mean age of the GIP+ was 7.3 ± 15.8 years while the mean age of GIP− was 18.9 ± 27.4 years.
3.6. Antibiotic Status, Length of Stay and Outcomes
A significantly higher use of antibiotics after the GIP test result (p = 0.014) was found among patients from the GIP+ group (63.9%) compared to GIP− (36.7%) (Table 2). No significant difference was found between the two groups in terms of antibiotic use prior to testing, nor in terms of change in antibiotics/discontinuation of antibiotics treatment after test.
The time to sample was not significantly different between the GIP+ and GIP− groups; however, both the time to discharge and duration of hospitalization were significantly higher in the GIP− group compared to GIP+ (p = 0.035, p= 0.003, respectively).
Furthermore, the treatment received on discharge was more common in the GIP+ group (50.8%) compared to the GIP− group (26.7%) (p = 0.029).
4. Discussion
The current main GI etiology detected by the GIP in the current study was bacterial (70.5%), with the most common being Campylobacter (48.8%) and Salmonella (34.9%). Both pathogens play an essential role in GIs, as reported in other studies [10,16]. The incidence of Campylobacter infections has been increasing worldwide along the years and it is considered a leading cause of bacterial GIs [17]. According to a recent report of the Foodborne Diseases Active Surveillance Network in the USA (FoodNet), during 2019, the incidence of Campylobacter spp. per 100,000 population was the highest (19.5%), followed by Salmonella (17.1%) [18]. In a study from Washington, Campylobacter spp. and Salmonella spp. were very common (20.9% and 12.4%, respectively); however, the most common pathogen detected was C. difficile (55%), compared to 6.6% in our study [19]. This may result from different stewardships of the GIP usage. In our medical center, the use of the GIP is authorized following a consult with an infectious disease specialist. Additionally, C. difficile presence is tested via another molecular platform, the GeneXpert® system (Cepheid, Sunnyvale, CA, USA). Thus, stool samples of patients suspected of C. difficile infections will probably not be tested by the GIP, and this may explain the low rate (6.6%) of C. difficile in our study compared to other studies (51.1–55%) [19,20]. Another factor that affects C. difficile prevalence is the patient’s age; while C. difficile is more common in the elderly, Campylobacter and Salmonella are common in all ages, but particularly in children [21,22]. The average age in our study was 11.2 years, as compared to 57 years [20] and 47.4 years [19]. Therefore, the higher rates of C. difficile in these previous studies are reasonable.
The routine diagnosis of stool culture in clinical microbiology laboratories in Israel constitutes testing for three bacteria: Campylobacter, Salmonella and Shigella. In the current study, Campylobacter was detected by stool culture in 19.7% of specimens, compared to 34.4% in the GIP; Salmonella was detected by both culture and the GIP in 14.7% of the positive samples. No Shigella was detected by stool culture, and only one case (1.6%) was detected by GIP. These results reinforce previous reports, according to which the GIP has a higher positivity rate compared to culture [19,23,24,25,26]. This can be attributed to the main limits of culture, including the difficulties in culturing bacteria when the sample was collected after antibiotic administration or when the causative bacterium is fastidious and has special growth requirements. Ours and previous results highlight the importance of incorporating molecular methods as part of the routine testing of stool specimens in microbiology laboratories.
Of the 61 positive GIPs, 37.7% had multiple pathogens detected. Previous studies have reported on various rates of coinfections being in the range of 10.2–51.7%. The notable coinfection rate sheds light on the challenge of determining the predominant agent in a considerable number of cases. Such cases require further investigations, as some pathogens may be regarded as irrelevant; for example, the presence of C. difficile in infants and young children is thought to be asymptomatic colonization [27]. Another example is the long shedding of the pathogen, such as in cases of Salmonella and Norovirus [13], and thus a former ancient infection should be taken into consideration. Since the GIP lacks quantification, it is important to promote multiplex molecular assays that quantify the pathogens involved in GIs, especially when more than one pathogen is detected, as this can distinguish infection from carriage. Additionally, the evidence of high coinfection percentages indicates that stool culture should be used as a complementary tool in some cases.
The analysis of pathogens by age group showed that Campylobacter was the most common pathogen among children in their first year of life (52.4%) and in the 2–5 years group (34.8%). Similar findings were reported in a previous study according to which Campylobacter caused the highest associated burden of diarrhea in 0–1-year-old children from Loreto, Peru and Venda, and South Africa [28]. Generally, certain age groups including children below the age of 4 and people older than 75 years are more vulnerable to Campylobacter infections [20]. Risk factors to gastroenteritis in young children include high exposure to outsourced food services, in which food handling, storage and cooking might sometimes be improper [22].
In contrast to our findings, EPEC was the main pathogen (23%) in a study from France with 172 children (median age, 1.10 years) [26]. However, atypical EPEC strains found in both diarrheal and asymptomatic individuals cast doubt on EPEC’s role in human infections [29]. It should be noted that while the prevalence of Campylobacter infections is well studied in developed countries [30,31], less data exist regarding these infections’ burden in developing countries, apparently due to the inconsistency and low sensitivity of culture; thus, it is possible that the contribution of Campylobacter to GI is underestimated [32].
Comparison of the positive and negative GIP groups found no significant differences between the patients except for the patient’s age, with the GIP+ patients being younger. This result is not surprising as children, especially under the age of 5 years, are one of the most affected groups [33].
Concerning the antibiotic status, a significantly higher use of antibiotics after the GIP test result (p-value = 0.014) was found in the GIP+ group compared to the GIP− group. This result is reasonable, given the fact that 71.7% of GIP+ results were attributed to bacterial etiology. A similar observation was reported in a previous study from Columbia, in which 80.1% of the patients with a positive GIP result started an antibiotic treatment following the test result, compared to 62.5% of patients with a negative GIP result (p < 0.00001) [20].
Although no significant difference between the groups was seen in terms of antibiotic change/discontinuation, the use of the GIP seems to be worthwhile, as treatment was changed/discontinued for a considerable number of patients in both groups (50% and 36% in GIP− and GIP+, respectively). Previous studies linked a significant increase in targeted antibiotics and decreased use of unnecessary antibiotics to the use of the GIP [34,35,36].
Another parameter, which did not significantly vary between GIP groups but is worth considering, is time to discharge; GIP+ patients were discharged in a shorter time compared to the GIP− group (1.5 vs. 3 days, respectively). This outcome may be linked to previous studies’ findings, according to which the use of the GIP, instead of the routine culture method, allowed the removal of patients from unnecessary isolation [37,38,39]. In this regard, it should be emphasized that a negative GIP result is also valuable and influences clinical management.
The duration of hospitalization was significantly lower (p = 0.003) in the GIP+ group compared to GIP−. Moreover, change in diagnosis following GIP test result and treatment received on discharge were significantly higher within the GIP+ group (p = 0.036, 0.029, respectively). Torres-Miranda et al. found a shorter LOS among patients whose samples were detected by the GIP, compared to patients in the period before using the GIP. Additionally, an earlier initiation of optimal antibiotics was seen in the GIP group [19]. Thus, all of these results, once again, highlight the gains of using the GIP in comparison to conventional stool culturing.
The study’s main limitation is the small sample size; further studies with a larger number of samples should be performed in order to ultimately determine the benefits of GIP use.
5. Conclusions
The GIP offers syndromic testing in a much shorter time compared to traditional methods. The GIP reduces antibiotic misuse and length of stay, which both indirectly decrease healthcare-associated costs and enhance the patient’s clinical management. Additionally, a positive GIP result facilitates and expedites the decision-making process by the physicians, including the determination of whether to stop or change antibiotic treatment, choosing the targeted antibiotic, and introducing/removing a patient from isolation, which also has important implications for infection control. Overall, the introduction of the FilmArray® GIP to the clinical laboratory presents a remarkable advance for the diagnosis of IGE.
Author Contributions
Conceptualization, D.C., H.R. and A.P.; Data curation, D.C., H.R. and M.A.; Formal analysis, D.C., H.R., M.A. and A.P.; Investigation, D.C., H.R. and M.A.; Methodology, D.C., H.R. and M.A; Project administration, M.A. and A.P.; Supervision, M.A. and A.P.; Validation, D.C., H.R., M.A. and A.P.; Visualization, D.C., H.R., M.A. and A.P.; Writing—original draft, D.C., H.R., M.A. and A.P.; Writing—review & editing, D.C., H.R., M.A. and A.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of the Tzafon Medical Center, approval no. POR-0105-20.
Informed Consent Statement
Patient consent was waived since this was a retrospective study which was based on existing data in the medical records of patients. All data were saved anonymously.
Data Availability Statement
The data used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
We thank Wadie Abu Dahoud for the statistical analysis.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Walker, C.L.F.; Rudan, I.; Liu, L.; Nair, H.; Theodoratou, E.; Bhutta, Z.A.; O’Brien, K.L.; Campbelt, H.; Backt, R.E. Global burden of childhood pneumonia and diarrhoea. Lancet 2013, 381, 1405–1416. [Google Scholar] [CrossRef] [PubMed]
- Hay, S.I.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdule, A.M.; Abebo, T.A.; Abera, S.F.; Aboyans, V.; et al. Global, regional, and national Disability-Adjusted Life-Years (DALYs) for 333 diseases and injuries and Healthy Life Expectancy (HALE) for 195 countries and territories, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 90, 1260–1344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scallan, E.; Griffin, P.M.; Angulo, F.J.; Tauxe, R.V.; Hoekstra, R.M. Foodborne illness acquired in the United States-unspecified agents. Emerg. Infect. Dis. 2011, 17, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Bereswill, S.; Kist, M. Recent developments in Campylobacter pathogenesis. Curr. Opin. Infect. Dis. 2003, 16, 487–491. [Google Scholar] [CrossRef]
- Halvorson, H.A.; Schlett, C.D.; Riddle, M.S. Postinfectious irritable bowel syndrome—A meta-analysis. Am. J. Gastroenterol. 2006, 101, 1894–1899, quiz 1942. [Google Scholar] [CrossRef]
- Elliott, E.J. Acute gastroenteritis in children. BMJ 2007, 334, 35–40. [Google Scholar] [CrossRef] [Green Version]
- Bruzzese, E.; Giannattasio, A.; Guarino, A. Antibiotic treatment of acute gastroenteritis in children. F1000Res 2018, 7, 193. [Google Scholar] [CrossRef]
- Lim, C.J.; Kong, D.C.; Stuart, R.L. Reducing inappropriate antibiotic prescribing in the residential care setting: Current perspectives. Clin. Interv. Aging 2014, 9, 165–177. [Google Scholar] [CrossRef] [Green Version]
- Sidoti, F.; Ritta, M.; Costa, C.; Cavallo, R. Diagnosis of viral gastroenteritis: Limits and potential of currently available procedures. J. Infect. Dev. Ctries. 2015, 9, 551–561. [Google Scholar] [CrossRef] [Green Version]
- Humphries, R.M.; Linscott, A.J. Practical Guidance for Clinical Microbiology Laboratories: Diagnosis of Bacterial Gastroenteritis. Clin. Microbiol. Rev. 2015, 28, 3–31. [Google Scholar] [CrossRef] [Green Version]
- Murphy, C.N.; Fowler, R.C.; Iwen, P.C.; Fey, P.D. Evaluation of the BioFire FilmArray(R) GastrointestinalPanel in a Midwestern Academic Hospital. Eur. J. Clin. Microbiol. Infect. Dis. 2017, 36, 747–754. [Google Scholar] [CrossRef]
- Dumkow, L.E.; Worden, L.J.; Rao, S.N. Syndromic diagnostic testing: A new way to approach patient care in the treatment of infectious diseases. J. Antimicrob. Chemother. 2021, 76 (Suppl. S3), iii4–iii11. [Google Scholar] [CrossRef]
- Buss, S.N.; Leber, A.; Chapin, K.; Fey, P.D.; Bankowski, M.J.; Jones, M.K.; Rogatcheva, M.; Kanack, K.J.; Bourzac, K.M. Multicenter evaluation of the BioFire FilmArray gastrointestinal panel for etiologic diagnosis of infectious gastroenteritis. J. Clin. Microbiol. 2015, 53, 915–925. [Google Scholar] [CrossRef] [Green Version]
- Chhabra, P.; Gregoricus, N.; Weinberg, G.A.; Halasa, N.; Chappell, J.; Hassan, F.; Selvarangan, R.; Mijatovic-Rustempasic, S.; Ward, M.L.; Bowen, M.; et al. Comparison of three multiplex gastrointestinal platforms for the detection of gastroenteritis viruses. J. Clin. Virol. 2017, 95, 66–71. [Google Scholar] [CrossRef] [Green Version]
- Singhal, N.; Kumar, M.; Kanaujia, P.K.; Virdi, J.S. MALDI-TOF mass spectrometry: An emerging technology for microbial identification and diagnosis. Front. Microbiol. 2015, 6, 791. [Google Scholar] [CrossRef] [Green Version]
- Calderaro, A.; Martinelli, M.; Buttrini, M.; Montecchini, S.; Covan, S.; Rossi, S.; Ferraglia, F.; Montagna, P.; Pinardi, F.; Larini, S.; et al. Contribution of the FilmArray((R)) Gastrointestinal Panel in the laboratory diagnosis of gastroenteritis in a cohort of children: A two-year prospective study. Int. J. Med. Microbiol. 2018, 308, 514–521. [Google Scholar] [CrossRef]
- Igwaran, A.; Okoh, A.I. Human campylobacteriosis: A public health concern of global importance. Heliyon 2019, 5, e02814. [Google Scholar] [CrossRef]
- Tack, D.M.; Ray, L.; Griffin, P.M.; Cieslak, P.R.; Dunn, J.; Rissman, T.; Jervis, R.; Lathrop, S.; Muse, A.; Duwell, M.; et al. Preliminary Incidence and Trends of Infections with Pathogens Transmitted Commonly Through Food—Foodborne Diseases Active Surveillance Network, 10 U.S. Sites, 2016–2019. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 509–514. [Google Scholar] [CrossRef]
- Torres-Miranda, D.; Akselrod, H.; Karsner, R.; Secco, A.; Silva-Cantillo, D.; Siegel, M.O.; Roberts, A.D.; Simon, G.L. Use of BioFire FilmArray gastrointestinal PCR panel associated with reductions in antibiotic use, time to optimal antibiotics, and length of stay. BMC Gastroenterol. 2020, 20, 246. [Google Scholar] [CrossRef]
- O’Neal, M.; Murray, H.; Dash, S.; Al-Hasan, M.N.; Justo, J.A.; Bookstaver, P.B. Evaluating appropriateness and diagnostic stewardship opportunities of multiplex polymerase chain reaction gastrointestinal testing within a hospital system. Ther. Adv. Infect. Dis. 2020, 7, 2049936120959561. [Google Scholar] [CrossRef]
- Levesque, S.; Fournier, E.; Carrier, N.; Frost, E.; Arbeit, R.D.; Michaud, S. Campylobacteriosis in urban versus rural areas: A case-case study integrated with molecular typing to validate risk factors and to attribute sources of infection. PLoS ONE 2013, 8, e83731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bassal, R.; Dichtiar, R.; Boker, L.K. Risk Factors for Multiple Infections with Salmonella, Shigella, and Campylobacter in Single Individuals Identified in Israel between 1999 and 2020: A Case-Case Control Study. Isr. Med. Assoc. J. 2022, 24, 360–363. [Google Scholar] [PubMed]
- Yoo, I.H.; Kang, H.M.; Suh, W.; Cho, H.; Yoo, I.Y.; Jo, S.J.; Park, Y.J.; Jeoung, D.C. Quality Improvements in Management of Children with Acute Diarrhea Using a Multiplex-PCR-Based Gastrointestinal Pathogen Panel. Diagnostics 2021, 11, 1175. [Google Scholar] [CrossRef] [PubMed]
- Ruzante, J.M.; Olin, K.; Munoz, B.; Nawrocki, J.; Selvarangan, R.; Meyers, L. Real-time gastrointestinal infection surveillance through a cloud-based network of clinical laboratories. PLoS ONE 2021, 16, e0250767. [Google Scholar] [CrossRef]
- Cybulski, R.J., Jr.; Bateman, A.C.; Bourassa, L.; Bryan, A.; Beail, B.; Matsumoto, J.; Cookson, B.T.; Fang, F.C. Clinical Impact of a Multiplex Gastrointestinal Polymerase Chain Reaction Panel in Patients with Acute Gastroenteritis. Clin. Infect. Dis. 2018, 67, 1688–1696. [Google Scholar] [CrossRef]
- Truong, J.; Cointe, A.; Le Roux, E.; Bidet, P.; Michel, M.; Boize, J.; Mariani-Kurkdjian, P.; Caseris, M.; Hobson, C.A.; Desmarest, M.; et al. Clinical impact of a gastrointestinal PCR panel in children with infectious diarrhoea. Arch. Dis. Child. 2022, 107, 601–605. [Google Scholar] [CrossRef]
- Brennhofer, S.A.; Rogawski McQuade, E.T.; Liu, J.; Guerrant, R.L.; Platts-Mills, J.A.; Warren, C.A. Clostridioides difficile colonization among very young children in resource-limited settings. Clin. Microbiol. Infect. 2022, 28, 996–1002. [Google Scholar] [CrossRef]
- Platts-Mills, J.A.; Babji, S.; Bodhidatta, L.; Gratz, J.; Haque, R.; Havt, A.; McCromick, B.J.J.; McGrath, M.; Olortegui, M.P.; Samie, A.; et al. Pathogen-specific burdens of community diarrhoea in developing countries: A multisite birth cohort study (MAL-ED). Lancet Glob. Health 2015, 3, e564–e575. [Google Scholar] [CrossRef] [Green Version]
- Hu, J.; Torres, A.G. Enteropathogenic Escherichia coli: Foe or innocent bystander? Clin. Microbiol. Infect. 2015, 21, 729–734. [Google Scholar] [CrossRef] [Green Version]
- Crim, S.M.; Iwamoto, M.; Huang, J.Y.; Griffin, P.M.; Gilliss, D.; Cronquist, A.B.; Cartter, M.; Tobin-D’Angelo, M.; Blythe, D.; Smith, K.; et al. Incidence and trends of infection with pathogens transmitted commonly through food—Foodborne Diseases Active Surveillance Network, 10 U.S. sites, 2006–2013. MMWR Morb. Mortal. Wkly. Rep. 2014, 63, 328–332. [Google Scholar]
- Jore, S.; Viljugrein, H.; Brun, E.; Heier, B.T.; Borck, B.; Ethelberg, S.; Hakkinen, M.; Kuusi, M.; Reiersen, J.; Hansson, I.; et al. Trends in Campylobacter incidence in broilers and humans in six European countries, 1997–2007. Prev. Vet. Med. 2010, 93, 33–41. [Google Scholar] [CrossRef]
- Platts-Mills, J.A.; Kosek, M. Update on the burden of Campylobacter in developing countries. Curr. Opin. Infect. Dis. 2014, 27, 444–450. [Google Scholar] [CrossRef] [Green Version]
- Sell, J.; Dolan, B. Common Gastrointestinal Infections. Prim. Care 2018, 45, 519–532. [Google Scholar] [CrossRef]
- Beal, S.G.; Tremblay, E.E.; Toffel, S.; Velez, L.; Rand, K.H. A Gastrointestinal PCR Panel Improves Clinical Management and Lowers Health Care Costs. J. Clin. Microbiol. 2018, 56, e01457-17. [Google Scholar] [CrossRef] [Green Version]
- Axelrad, J.E.; Freedberg, D.E.; Whittier, S.; Greendyke, W.; Lebwohl, B.; Green, D.A. Impact of Gastrointestinal Panel Implementation on Health Care Utilization and Outcomes. J. Clin. Microbiol. 2019, 57, e01775-18. [Google Scholar] [CrossRef] [Green Version]
- Keske, S.; Zabun, B.; Aksoy, K.; Can, F.; Palaoglu, E.; Ergonul, O. Rapid Molecular Detection of Gastrointestinal Pathogens and Its Role in Antimicrobial Stewardship. J. Clin. Microbiol. 2018, 56, e00148-18. [Google Scholar] [CrossRef] [Green Version]
- Rand, K.H.; Tremblay, E.E.; Hoidal, M.; Fisher, L.B.; Grau, K.R.; Karst, S.M. Multiplex gastrointestinal pathogen panels: Implications for infection control. Diagn. Microbiol. Infect. Dis. 2015, 82, 154–157. [Google Scholar] [CrossRef]
- Machiels, J.D.; Cremers, A.J.H.; van Bergen-Verkuyten, M.; Paardekoper-Strijbosch, S.J.M.; Frijns, K.C.J.; Wertheim, H.F.L.; Rahamat-Langendoen, J.; Melchers, W.J.G. Impact of the BioFire FilmArray gastrointestinal panel on patient care and infection control. PLoS ONE 2020, 15, e0228596. [Google Scholar] [CrossRef]
- Halligan, E.; Edgeworth, J.; Bisnauthsing, K.; Bible, J.; Cliff, P.; Aarons, E.; Klein, J.; Patel, A.; Goldenberg, S. Multiplex molecular testing for management of infectious gastroenteritis in a hospital setting: A comparative diagnostic and clinical utility study. Clin. Microbiol. Infect. 2014, 20, O460–O467. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Distribution of causative pathogens in the study group by GIP. Sixty-one stool samples were found to be positive by the GIP for one or more pathogens. The distribution of the different detected pathogens is presented.
Figure 1.
Distribution of causative pathogens in the study group by GIP. Sixty-one stool samples were found to be positive by the GIP for one or more pathogens. The distribution of the different detected pathogens is presented.

Figure 2.
Coinfections detected in GIP-positive specimens. Among the 61 positive stool samples, 24 samples were positive for more than one pathogen (i.e., coinfection), with various combinations of pathogens, as presented in the graph.
Figure 2.
Coinfections detected in GIP-positive specimens. Among the 61 positive stool samples, 24 samples were positive for more than one pathogen (i.e., coinfection), with various combinations of pathogens, as presented in the graph.

Figure 3.
Distribution of causative pathogens in the study group according to age. The various causative agents of GIs distribute differently in distinct age groups, as presented in the graph.
Figure 3.
Distribution of causative pathogens in the study group according to age. The various causative agents of GIs distribute differently in distinct age groups, as presented in the graph.


{kind=link}
{kind=link}
{kind=link}
Table 1.
General demographic and clinical data of study participants.
| Characteristics | GIP− (N = 30) n, % | GIP+ (N = 61) n, % | Total (N = 91) n, % | p-Value |
|---|---|---|---|---|
| Gender, n (%) | 0.331 | |||
| Female Male | 18 (60) 12 (40) | 30 (49.2) 31 (50.8) | 48(52.7) 43 (47.3) | |
| Age (years) | <0.012 | |||
| Mean (SD) Range | 18.9 (27.4) 0–80.4 | 7.3 (15.8) 0–76.6 | 11.2 (20.6) 0–80.4 | |
| Ethnicity, n (%) | ||||
| Arab Jews | 13 (43.3) 17 (56.7) | 37 (60.7) 24 (39.3) | 50 (55) 41(46) | 0.118 |
| Vaccinated 1, n (%) | 1.000 | |||
| No Yes | 1 (3.3) 29 (96.7) | 2 (3.3) 58 (96.7) | 3 (3.3) 87 (96.7) | |
| Chronic Disease 2, n (%) | 0.775 | |||
| No Yes | 27 (90) 3 (10) | 56 (91.8) 5 (8.2) | 83 (91.2) 8 (8.8) |
1 Vaccinated refers to vaccination with the routinely administered vaccines in Israel. 2 Chronic disease refers to chronic diseases the patient has, such as cancer.
Table 2.
Antibiotic status, length of stay and outcomes.
| Parameter | GIP− (N = 30) n, (%) | GIP+ (N = 61) n, (%) | Total (N = 91) n, (%) | p-Value |
|---|---|---|---|---|
| Antibiotic treatment prior test, n (%) | 0.599 | |||
| No | 11 (36.7) | 19 (31.1) | 30 (33.0) | |
| Yes | 19 (63.3) | 42 (68.9) | 61 (67.0) | |
| Antibiotic treatment after test, n (%) | ||||
| No | 19 (63.3) | 22 (36) | 41 (45) | 0.014 |
| Yes | 11 (36.7) | 39 (64) | 50 (55) | |
| Antibiotic change/discontinuation, n (%) | 0.203 | |||
| No | 15 (50) | 39 (64) | 54 (59.3) | |
| Yes | 15 (50) | 22 (36) | 37 (40.7) | |
| Time to sample (Days) | 0.055 | |||
| Mean (SD) | 1.3 (1.4) | 0.7 (1.2) | 0.9 (1.3) | |
| Range | 0.0–5.0 | 0.0–8.0 | 0.0–8.0 | |
| Time to discharge (Days) | 0.035 | |||
| Mean (SD) | 3.0 (4.5) | 1.5 (1.8) | 2.0 (3.0) | |
| Range | 0–18 | 0–13 | 0–18 | |
| Length of stay (Days) | 0.003 | |||
| Mean (SD) | 4.1 (4.8) | 2.0 (1.5) | 2.0 (3.0) | |
| Range | 0–21.0 | 0–8.0 | 0–18 | |
| Discharge due to GIP result, n (%) | 0.604 | |||
| No | 29 (96.7) | 60 (98.4) | 89 (97.8) | |
| Yes | 1 (3.3) | 1 (1.6) | 2 (2.2) | |
| Acute complications 1, n (%) | 0.152 | |||
| No | 29 (96.7) | 61 (100) | 90 (99) | |
| Yes | 1 (3.3) | 0 (0) | 1 (1) | |
| Treatment received on discharge, n (%) | 0.029 | |||
| No | 22 (73.3) | 30 (49.2) | 52 (57) | |
| Yes | 8 (26.7) | 31 (50.8) | 39 (43) | |
| Change in diagnosis following test, n (%) | 0.036 | |||
| No | 29(96.7) | 49(80.3) | 78 (85.7) | |
| Yes | 1 (3.3) | 12 (19.7) | 13 (14.3) |
1 Acute complications include dehydration, malabsorption, transient lactose intolerance, systemic infection, and sepsis.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Carmon, D.; Rohana, H.; Azrad, M.; Peretz, A. The Impact of a Positive Biofire® FilmArray® Gastrointestinal Panel Result on Clinical Management and Outcomes. Diagnostics 2023, 13, 1094. https://doi.org/10.3390/diagnostics13061094
AMA Style
Carmon D, Rohana H, Azrad M, Peretz A. The Impact of a Positive Biofire® FilmArray® Gastrointestinal Panel Result on Clinical Management and Outcomes. Diagnostics. 2023; 13(6):1094. https://doi.org/10.3390/diagnostics13061094
Chicago/Turabian StyleCarmon, David, Hanan Rohana, Maya Azrad, and Avi Peretz. 2023. "The Impact of a Positive Biofire® FilmArray® Gastrointestinal Panel Result on Clinical Management and Outcomes" Diagnostics 13, no. 6: 1094. https://doi.org/10.3390/diagnostics13061094
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.