
Breast Cancer Diagnosis Using Extended-Wavelength–Diffuse Reflectance Spectroscopy (EW-DRS)—Proof of Concept in Ex Vivo Breast Specimens Using Machine Learning
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Recruitment
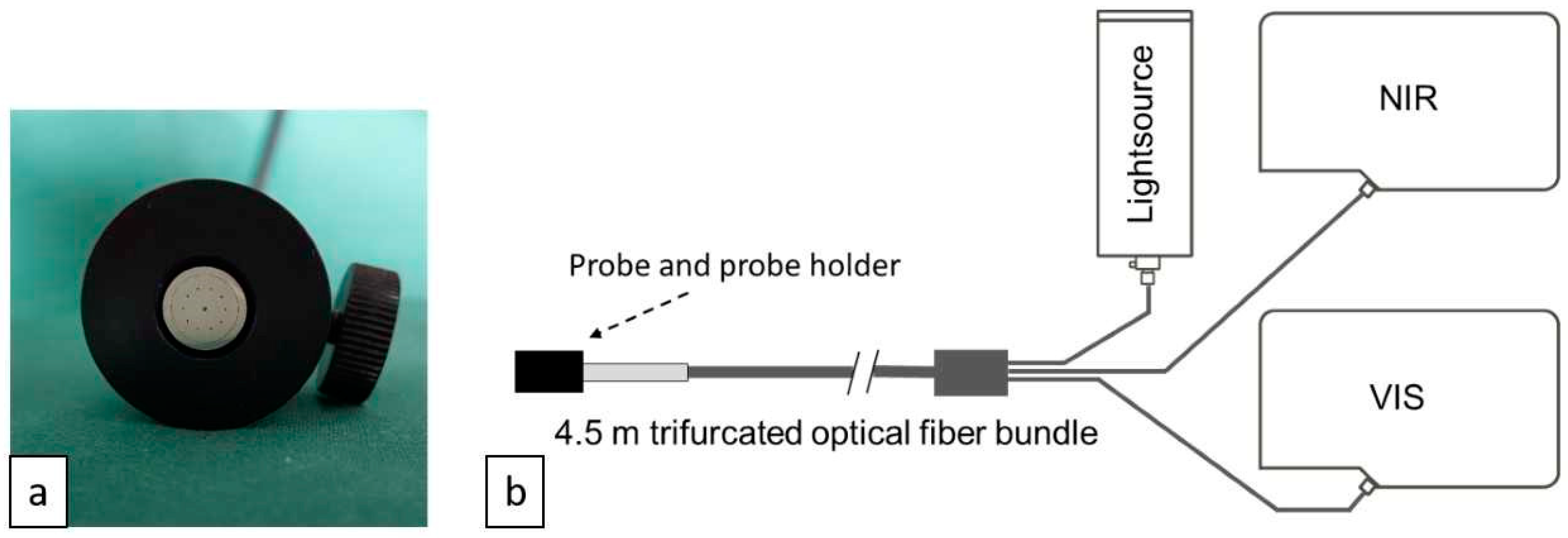
2.2. Instrumentation
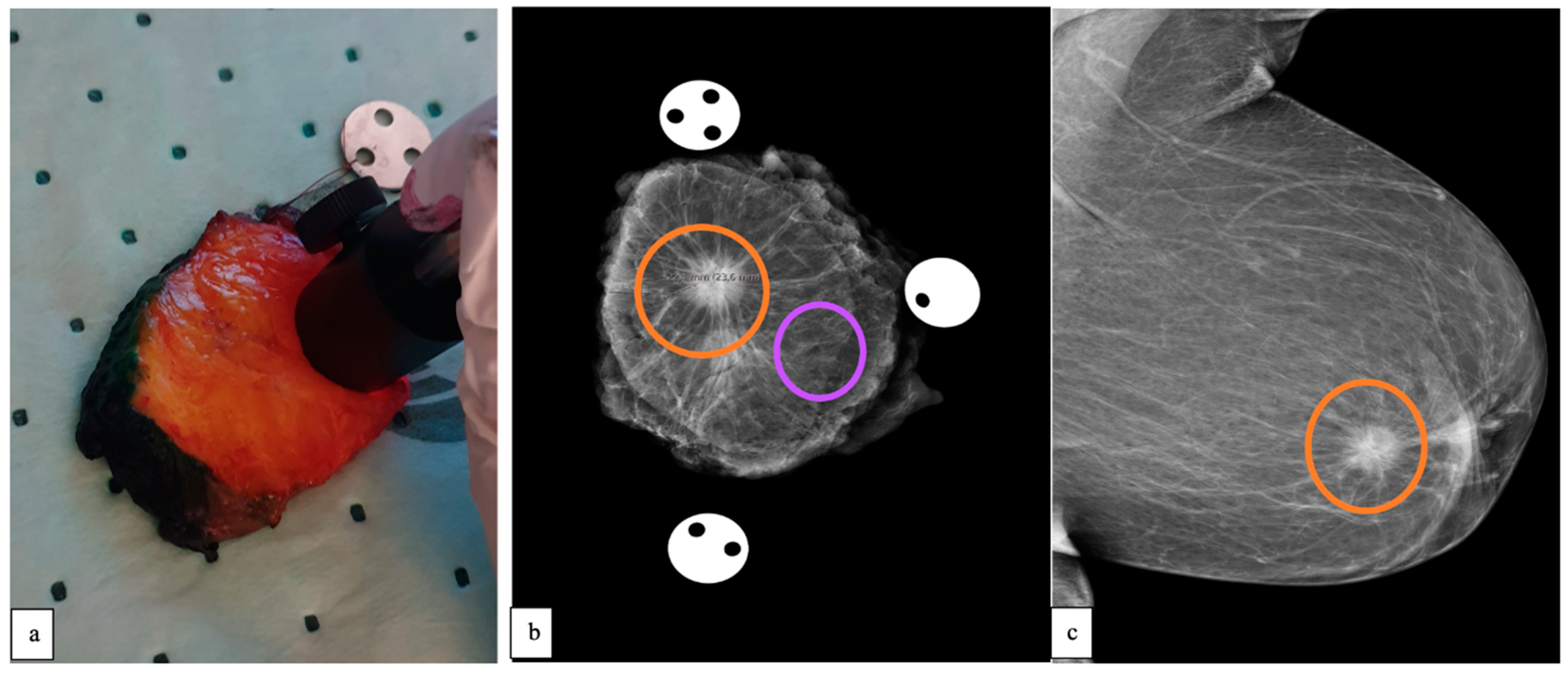
2.3. Data Collection
2.4. Histopathological Analysis
2.5. Multivariate Statistics and Machine Learning Discrimination Models
3. Results
3.1. Demographics
Pre-Operative Radiological Report
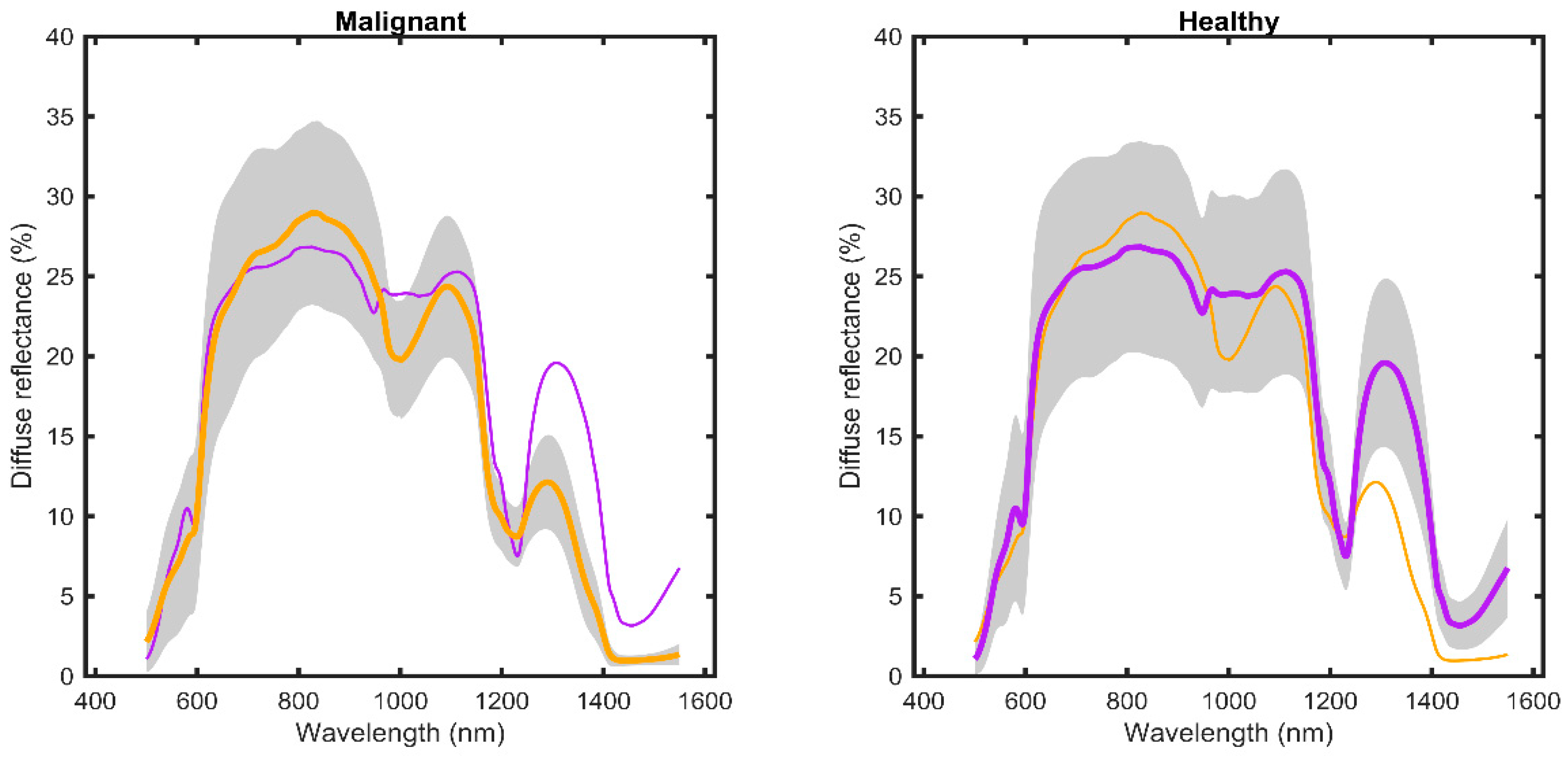
3.2. DRS Data
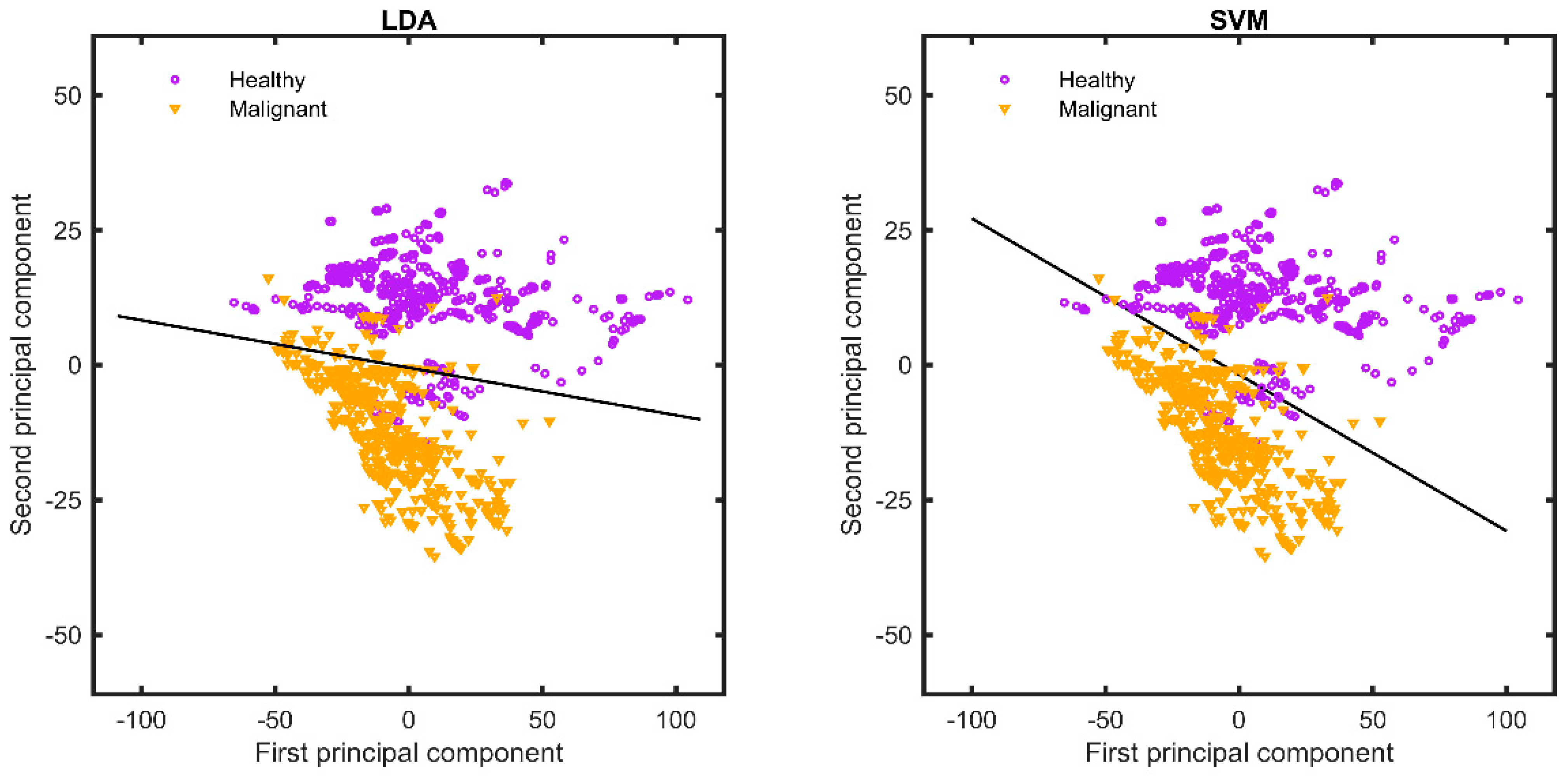
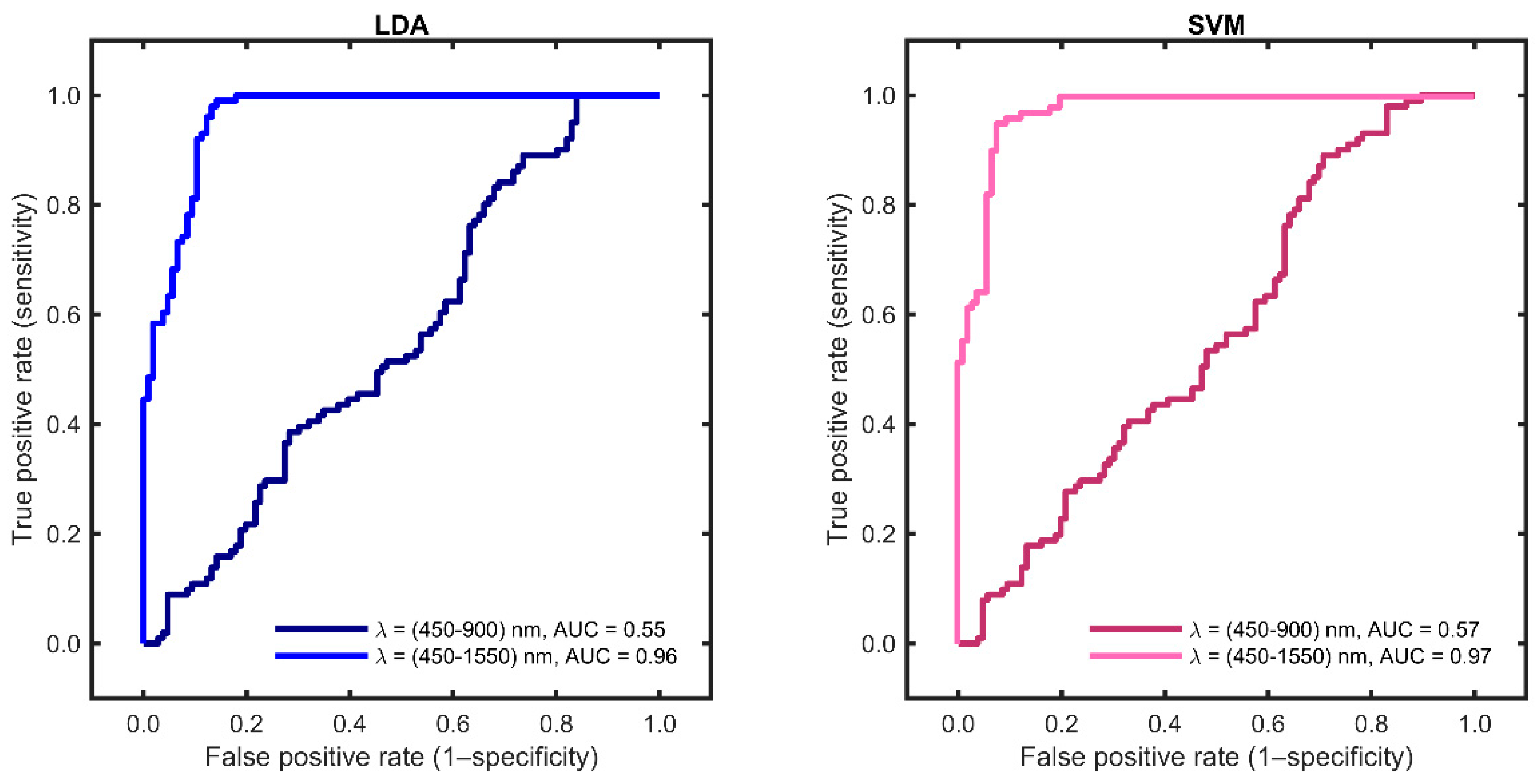
3.3. Machine Learning Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fakhri, N.; Chad, M.A.; Lahkim, M.; Houari, A.; Dehbi, H.; Belmouden, A.; El Kadmiri, N. Risk factors for breast cancer in women: An update review. Med. Oncol. 2022, 39, 197. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Olle Bergman, L.F.; Hont, G.; Johansson, E.; Ljungman, P. Cancer i Siffror 2018. Socialsyrelsen. 2018. Available online: https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/artikelkatalog/statistik/2018-6-10.pdf (accessed on 5 January 2022).
- Segnan, N.; Minozzi, S.; Ponti, A.; Bellisario, C.; Balduzzi, S.; González-Lorenzo, M.; Gianola, S.; Armaroli, P. Estimate of false-positive breast cancer diagnoses from accuracy studies: A systematic review. J. Clin. Pathol. 2017, 70, 282–294. [Google Scholar] [CrossRef] [PubMed]
- Taroni, P.; Quarto, G.; Pifferi, A.; Abbate, F.; Balestreri, N.; Menna, S.; Cassano, E.; Cubeddu, R. Breast tissue composition and its dependence on demographic risk factors for breast cancer: Non-invasive assessment by time domain diffuse optical spectroscopy. PLoS ONE 2015, 10, e0128941. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, I.; Huland, D.M.; Vermesh, O.; Frostig, H.E.; Tummers, W.S.; Gambhir, S.S. Photoacoustic clinical imaging. Photoacoustics 2019, 14, 77–98. [Google Scholar] [CrossRef] [PubMed]
- Evers, D.J.; Nachabe, R.; Peeters, M.-J.V.; van der Hage, J.A.; Oldenburg, H.S.; Rutgers, E.J.; Lucassen, G.W.; Hendriks, B.H.W.; Wesseling, J.; Ruers, T.J.M. Diffuse reflectance spectroscopy: Towards clinical application in breast cancer. Breast Cancer Res. Treat. 2012, 137, 155–165. [Google Scholar] [CrossRef]
- Shalaby, N.; Al-Ebraheem, A.; Le, D.; Cornacchi, S.; Fang, Q.; Farrell, T.; Lovrics, P.; Gohla, G.; Reid, S.; Hodgson, N.; et al. Time-resolved fluorescence (TRF) and diffuse reflectance spectroscopy (DRS) for margin analysis in breast cancer. Lasers Surg. Med. 2018, 50, 236–245. [Google Scholar] [CrossRef]
- de Boer, L.L.; Hendriks, B.H.W.; van Duijnhoven, F.; Peeters-Baas, M.-J.T.F.D.V.; Van de Vijver, K.; Loo, C.E.; Jóźwiak, K.; Sterenborg, H.J.C.M.; Ruers, T.J.M. Using DRS during breast conserving surgery: Identifying robust optical parameters and influence of inter-patient variation. Biomed. Opt. Express 2016, 7, 5188–5200. [Google Scholar] [CrossRef]
- de Boer, L.L.; Molenkamp, B.G.; Bydlon, T.M.; Hendriks, B.H.W.; Wesseling, J.; Sterenborg, H.J.C.M.; Ruers, T.J.M. Fat/water ratios measured with diffuse reflectance spectroscopy to detect breast tumor boundaries. Breast Cancer Res. Treat. 2015, 152, 509–518. [Google Scholar] [CrossRef]
- Kennedy, S.; Geradts, J.; Bydlon, T.; Brown, J.Q.; Gallagher, J.; Junker, M.; Barry, W.; Ramanujam, N.; Wilke, L. Optical breast cancer margin assessment: An observational study of the effects of tissue heterogeneity on optical contrast. Breast Cancer Res. 2010, 12, R91. [Google Scholar] [CrossRef]
- Taroni, P.; Paganoni, A.M.; Ieva, F.; Pifferi, A.; Quarto, G.; Abbate, F.; Cassano, E.; Cubeddu, R. Non-invasive optical estimate of tissue composition to differentiate malignant from benign breast lesions: A pilot study. Sci. Rep. 2017, 7, 40683. [Google Scholar] [CrossRef] [PubMed]
- Zhu, C.; Palmer, G.M.; Breslin, T.M.; Harter, J.M.; Ramanujam, N. Diagnosis of breast cancer using fluorescence and diffuse reflectance spectroscopy: A Monte-Carlo-model-based approach. J. Biomed. Opt. 2008, 13, 034015. [Google Scholar] [CrossRef] [PubMed]
- Nachabé, R.; Hendriks, B.H.W.; Desjardins, A.E.; van der Voort, M.; van der Mark, M.B.; Sterenborg, H.J.C.M. Estimation of lipid and water concentrations in scattering media with diffuse optical spectroscopy from 900 to 1600 nm. J. Biomed. Opt. 2010, 15, 037015. [Google Scholar] [CrossRef]
- Prabitha, V.G.; Suchetha, S.; Jayanthi, J.L.; Baiju, K.V.; Rema, P.; Anuraj, K.; Mathews, A.; Sebastian, P.; Subhash, N. Detection of cervical lesions by multivariate analysis of diffuse reflectance spectra: A clinical study. Lasers Med. Sci. 2016, 31, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Reistad, N.; Sturesson, C. Distinguishing tumor from healthy tissue in human liver ex vivo using machine learning and multivariate analysis of diffuse reflectance spectra. J. Biophotonics 2022, 15, e202200140. [Google Scholar] [CrossRef]
- Reistad, N.; Nilsson, J.H.; Bergenfeldt, M.; Rissler, P.; Sturesson, C. Intraoperative liver steatosis characterization using diffuse reflectance spectroscopy. HPB 2019, 21, 175–180. [Google Scholar] [CrossRef]
- Dahlstrand, U.; Sheikh, R.; Nguyen, C.D.; Hult, J.; Reistad, N.; Malmsjö, M. Identification of tumor margins using diffuse reflectance spectroscopy with an extended-wavelength spectrum in a porcine model. Ski. Res. Technol. 2018, 24, 667–671. [Google Scholar] [CrossRef]
- Bunke, J.; Sheikh, R.; Reistad, N.; Malmsjö, M. Extended-wavelength diffuse reflectance spectroscopy for a comprehensive view of blood perfusion and tissue response in human forearm skin. Microvasc. Res. 2019, 124, 1–5. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. J. Am. Coll. Dent. 2014, 81, 14–18. [Google Scholar]
- McClatchy, D.M., 3rd; Krishnaswamy, V.; Kanick, S.C.; Elliott, J.T.; Wells, W.A.; Barth, R.J.; Paulsen, K.D.; Pogue, B.W. Molecular dyes used for surgical specimen margin orientation allow for intraoperative optical assessment during breast conserving surgery. J. Biomed. Opt. 2015, 20, 040504. [Google Scholar] [CrossRef]
- Sickles, E.; D’Orsi, C.J.; Bassett, L.W. ACR BI-RADS® Mammography. In ACR BI-RADS® Atlas, Breast Imaging Reporting and Data System, 5th ed.; American College of Radiology: Reston, VA, USA, 2013. [Google Scholar]
- Hoon Tan, P.; Ellis, I.; Allison, K.; Brogi, E.; Fox, S.B.; Lakhani, S.; Lazar, A.J.; Morris, E.A.; Sahin, A.; Salgado, R.; et al. The 2019 World Health Organization classification of tumours of the breast. Histopathology 2020, 77, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Roggan, A.; Friebel, M.; Dörschel, K.; Hahn, A.; Müller, G. Optical Properties of Circulating Human Blood in the Wavelength Range 400–2500 nm. J. Biomed. Opt. 1999, 4, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Heijblom, M.; Piras, D.; van den Engh, F.M.; Van Der Schaaf, M.; Klaase, J.M.; Steenbergen, W.; Manohar, S. The state of the art in breast imaging using the Twente Photoacoustic Mammoscope: Results from 31 measurements on malignancies. Eur. Radiol. 2016, 26, 3874–3887. [Google Scholar] [CrossRef] [PubMed]
- Heijblom, M.; Piras, D.; Xia, W.; van Hespen, J.C.G.; Klaase, J.M.; van den Engh, F.M.; van Leeuwen, T.G.; Steenbergen, W.; Manohar, S. Visualizing breast cancer using the Twente photoacoustic mammoscope: What do we learn from twelve new patient measurements? Opt. Express 2012, 20, 11582–11597. [Google Scholar] [CrossRef] [PubMed]
- Randeberg, L.L. Diagnostic Applications of Diffuse Reflectance Spectroscopy 2005. Ph.D. Thesis, Norwegian University of Science and Technology, Trondheim, Norway, 2005. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient nr | Age | BMI | HRT | Breast Density, BI-RADS 5th Edi | Mammogram (MAM) Tumour Appearance, mm | MAM Size, mm | US Tumour Appearance, mm | US Size, mm | Breast Specimen | Histopathological Diagnosis |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 68 | 20.3 | No | B | Spiculated | 10 | Ill-defined, diffuse, hypoechoic | 10 | M | ILC |
| 2 | 84 | 30.5 | No | D | Partly ill-defined | 16 | Ill-defined, diffuse, hypoechoic | 13 | M | IDC |
| 3 | 70 | 29.8 | Yes | A | Indistinct, lobulated elongated | 25 | Hypoechoic | 25 | PM | IPC |
| 4 | 54 | 30.8 | No | A | Spiculated | 11 | Spiculated | 10 | PM | IDC |
| 5 | 56 | 29.4 | No | B | Ill-defined, diffuse | 15 | Ill-defined, diffuse, hypoechoic | 15 | PM | IDC |
| 6 | 66 | 28.7 | Yes | B | Ill-defined, diffuse | 15 | Ill-defined, diffuse, hypoechoic | 11 | PM | IDC |
| 7 | 52 | 27.9 | No | C | Spiculated, multifocal | 15 + 10 | Multifocal, ill-defined diffuse, hypoechoic | 20 | PM | IDC |
| 8 | 71 | 34.6 | No | A | Spiculated | 17 | Spiculated, hypoechoic | 15 | PM | ILC |
| 9 | 77 | 18.5 | No | D | Ill-defined, diffuse | * | Ill-defined, diffuse, hypoechoic | 30 | PM | IDC |
| 10 | 84 | 29.5 | No | A | Spiculated | 18 | Hypoechoic | 14 | PM | ILC |
| 11 | 57 | 34.3 | No | C | Multifocal | 45 | Multifocal, ill-defined diffuse, hypoechoic | 36 | M | ILC |
| 12 | 52 | 29.8 | No | B | Spiculated | 18 | Ill-defined, diffuse, hypoechoic | 15 | PM | IDC |
| 13 | 69 | 26.6 | No | A | Ill-defined, diffuse | 10 | Ill-defined, diffuse, hypoechoic | 10 | M | TC |
| 14 | 71 | 29.0 | No | B | Ill-defined, diffuse | 10 | Ill-defined, diffuse, hypoechoic | 8 | PM | TC |
| 15 | 73 | 25.1 | No | C | Partly ill-defined | 40 | Ill-defined, diffuse, hypoechoic | 40 | PM | ILC |
| 16 | 57 | 18.3 | No | D | Partly ill-defined | 12 | Ill-defined, diffuse, hypoechoic | 12 | PM | IDC |
| 17 | 56 | 32.0 | No | A | Calcification | 20 | Normal | * | PM | DCIS |
| 18 | 61 | 26.0 | No | C | Spiculated | 12 | Spiculated, hypoechoic | 12 | PM | ILC |
| 19 | 72 | 33.5 | No | C | Distortion | 50 | Ill-defined, diffuse, hypoechoic | 60 | M | ILC |
| 20 | 70 | 23.5 | No | B | Spiculated | 12 | Ill-defined, diffuse, hypoechoic | 12 | PM | IDC |
| 21 | 56 | 20.5 | No | D | Distortion | 12 | Ill-defined, diffuse, hypoechoic | 8 | PM | IDC |
| 22 | 61 | 21.0 | No | C | Partly ill-defined | 17 | Ill-defined, diffuse, hypoechoic | 17 | PM | IDC |
| 23 | 74 | 26.0 | No | B | Distortion | 10 | Ill-defined, diffuse, hypoechoic | 10 | PM | ILC |
| Breast Density, BI-RADS 5th Edi (n, %) | |
|---|---|
| A | 6 (26.1) |
| B | 7 (30.4) |
| C | 6 (26.1) |
| D | 4 (17.4) |
| Ultrasound tumour size (mm) | |
| Minimum | 10 |
| Maximum | 60 |
| Mean * | 18.3 |
| Mammography tumour size (mm) | |
| Minimum | 10 |
| Maximum | 50 |
| Mean * | 18.6 |
| Tissue | Number of Measurement Sites (n = 207) | Number of Optical Measurements (n = 1035) |
|---|---|---|
| Malignant | 101 | 505 |
| Healthy | 106 | 530 |
| Diagnostic Algorithm | Wavelength Ranges | SE | SP | CR | MCC |
|---|---|---|---|---|---|
| Nm | (%) | ||||
| LDA | 450–900 | 33 | 70 | 52 | 3 |
| 450–1550 | 92 | 90 | 91 | 82 | |
| SVM | 450–900 | 40 | 71 | 56 | 11 |
| 450–1550 | 94 | 91 | 92 | 85 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chaudhry, N.; Albinsson, J.; Cinthio, M.; Kröll, S.; Malmsjö, M.; Rydén, L.; Sheikh, R.; Reistad, N.; Zackrisson, S. Breast Cancer Diagnosis Using Extended-Wavelength–Diffuse Reflectance Spectroscopy (EW-DRS)—Proof of Concept in Ex Vivo Breast Specimens Using Machine Learning. Diagnostics 2023, 13, 3076. https://doi.org/10.3390/diagnostics13193076
Chaudhry N, Albinsson J, Cinthio M, Kröll S, Malmsjö M, Rydén L, Sheikh R, Reistad N, Zackrisson S. Breast Cancer Diagnosis Using Extended-Wavelength–Diffuse Reflectance Spectroscopy (EW-DRS)—Proof of Concept in Ex Vivo Breast Specimens Using Machine Learning. Diagnostics. 2023; 13(19):3076. https://doi.org/10.3390/diagnostics13193076
Chicago/Turabian StyleChaudhry, Nadia, John Albinsson, Magnus Cinthio, Stefan Kröll, Malin Malmsjö, Lisa Rydén, Rafi Sheikh, Nina Reistad, and Sophia Zackrisson. 2023. "Breast Cancer Diagnosis Using Extended-Wavelength–Diffuse Reflectance Spectroscopy (EW-DRS)—Proof of Concept in Ex Vivo Breast Specimens Using Machine Learning" Diagnostics 13, no. 19: 3076. https://doi.org/10.3390/diagnostics13193076