
The Initial ATA Risk Classification, but Not the AJCC/TNM Stage, Predicts the Persistence or Relapse of Differentiated Thyroid Cancer in Long-Term Surveillance

 ,
,  , ,
, ,  and
and 
Abstract
:1. Introduction
2. Patients and Methods
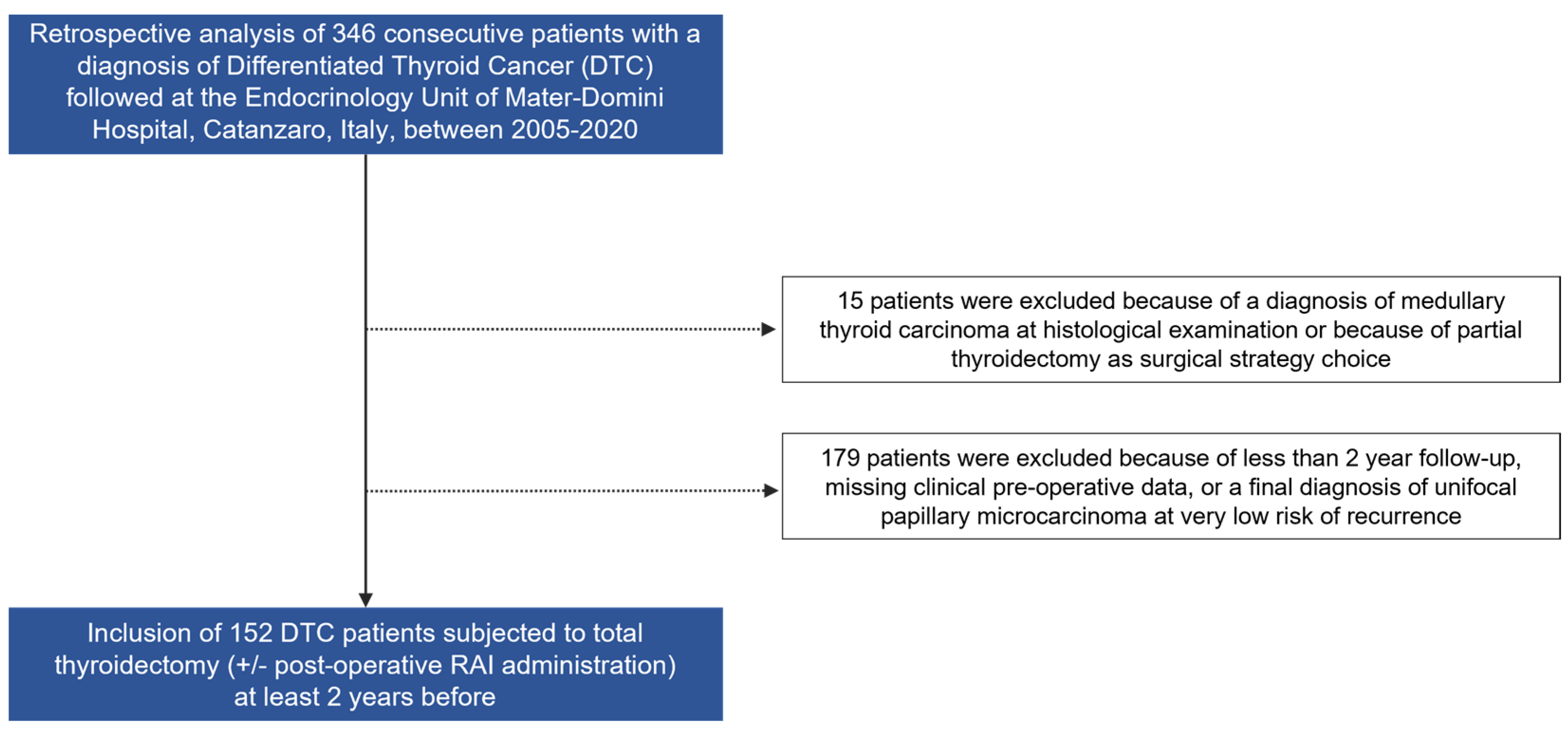
2.1. Study Participants
2.2. Outcome Assessment
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Participants and Prevalence Proportion of Persistence or Relapse of DTC
3.2. Outcome Assessments by ATA Risk Classification System and Other Prognostic Factors
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Giuliano, S.; Mirabelli, M.; Chiefari, E.; Vergine, M.; Gervasi, R.; Brunetti, F.S.; Innaro, N.; Donato, G.; Aversa, A.; Brunetti, A. Malignancy Analyses of Thyroid Nodules in Patients Subjected to Surgery with Cytological- and Ultrasound-Based Risk Stratification Systems. Endocrines 2020, 1, 102–118. [Google Scholar] [CrossRef]
- Kim, S.J.; Myong, J.P.; Suh, H.; Lee, K.E.; Youn, Y.K. Optimal Cutoff Age for Predicting Mortality Associated with Differentiated Thyroid Cancer. PLoS ONE 2015, 10, e0130848. [Google Scholar] [CrossRef]
- Van Den Heede, K.; Tolley, N.S.; Di Marco, A.N.; Palazzo, F.F. Differentiated Thyroid Cancer: A Health Economic Review. Cancers 2021, 13, 2253. [Google Scholar] [CrossRef] [PubMed]
- Arrigoni, G.; Crosetti, E.; Freddi, M.; Piovesan, A.; Rossetto Giaccherino, R.; Succo, G.; Palestini, N. Comparison between 2015 ATA guidelines and Italian Consensus for DTC management. A commented report. Acta Otorhinolaryngol. Ital. 2022, 42, 41–54. [Google Scholar] [CrossRef] [PubMed]
- Lamartina, L.; Handkiewicz-Junak, D. Follow-up of low risk thyroid cancer patients: Can we stop follow-up after 5 years of complete remission? Eur. J. Endocrinol. 2020, 182, D1–D16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manzardo, O.A.; Cellini, M.; Indirli, R.; Dolci, A.; Colombo, P.; Carrone, F.; Lavezzi, E.; Mantovani, G.; Mazziotti, G.; Arosio, M.; et al. TNM 8th edition in thyroid cancer staging: Is there an improvement in predicting recurrence? Endocr.-Relat. Cancer 2020, 27, 325–336. [Google Scholar] [CrossRef]
- Kloos, R.T.; Mazzaferri, E.L. A single recombinant human thyrotropin-stimulated serum thyroglobulin measurement predicts differentiated thyroid carcinoma metastases three to five years later. J. Clin. Endocrinol. Metab. 2005, 90, 5047–5057. [Google Scholar] [CrossRef] [Green Version]
- Kim, T.H.; Kim, Y.N.; Kim, H.I.; Park, S.Y.; Choe, J.H.; Kim, J.H.; Kim, J.S.; Oh, Y.L.; Hahn, S.Y.; Shin, J.H.; et al. Prognostic value of the eighth edition AJCC TNM classification for differentiated thyroid carcinoma. Oral Oncol. 2017, 71, 81–86. [Google Scholar] [CrossRef]
- Ge, M.H.; Cao, J.; Wang, J.Y.; Huang, Y.Q.; Lan, X.B.; Yu, B.; Wen, Q.L.; Cai, X.J. Nomograms predicting disease-specific regional recurrence and distant recurrence of papillary thyroid carcinoma following partial or total thyroidectomy. Medicine 2017, 96, e7575. [Google Scholar] [CrossRef]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [Green Version]
- Pacini, F.; Basolo, F.; Bellantone, R.; Boni, G.; Cannizzaro, M.A.; De Palma, M.; Durante, C.; Elisei, R.; Fadda, G.; Frasoldati, A.; et al. Italian consensus on diagnosis and treatment of differentiated thyroid cancer: Joint statements of six Italian societies. J. Endocrinol. Investig. 2018, 41, 849–876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baloch, Z.W.; Asa, S.L.; Barletta, J.A.; Ghossein, R.A.; Juhlin, C.C.; Jung, C.K.; LiVolsi, V.A.; Papotti, M.G.; Sobrinho-Simões, M.; Tallini, G.; et al. Overview of the 2022 WHO Classification of Thyroid Neoplasms. Endocr. Pathol. 2022, 33, 27–63. [Google Scholar] [CrossRef] [PubMed]
- Mukhtar, N.; Aljamei, H.; Aljomaiah, A.; Moria, Y.; Alzahrani, A.S. Natural Course of the American Thyroid Association Response to Therapy Statuses (Dynamic Risk Stratification) in Differentiated Thyroid Cancer. Eur. Thyroid J. 2020, 10, 198–207. [Google Scholar] [CrossRef] [PubMed]
- Zahedi, A.; Bondaz, L.; Rajaraman, M.; Leslie, W.D.; Jefford, C.; Young, J.E.; Pathak, K.A.; Bureau, Y.; Rachinsky, I.; Badreddine, M.; et al. Risk for Thyroid Cancer Recurrence Is Higher in Men Than in Women Independent of Disease Stage at Presentation. Thyroid 2020, 30, 871–877. [Google Scholar] [CrossRef]
- Shah, S.; Boucai, L. Effect of Age on Response to Therapy and Mortality in Patients with Thyroid Cancer at High Risk of Recurrence. J. Clin. Endocrinol. Metab. 2018, 103, 689–697. [Google Scholar] [CrossRef]
- Cooper, D.S. Radioiodine for Low-Risk Thyroid Cancer-the Swinging Pendulum. N. Engl. J. Med. 2022, 386, 990–991. [Google Scholar] [CrossRef]
- Leboulleux, S.; Bournaud, C.; Chougnet, C.N.; Zerdoud, S.; Al Ghuzlan, A.; Catargi, B.; Do Cao, C.; Kelly, A.; Barge, M.L.; Lacroix, L.; et al. Thyroidectomy without Radioiodine in Patients with Low-Risk Thyroid Cancer. N. Engl. J. Med. 2022, 386, 923–932. [Google Scholar] [CrossRef]
- Alzahrani, A.S.; Albalawi, L.; Mazi, S.; Mukhtar, N.; Aljamei, H.; Moria, Y.; Elsayed, T.; Amer, L.; Alanazi, F.; Alnasser, L.; et al. How Does The AJCC/TNM Staging System Eighth Edition Perform in Thyroid Cancer at A Major Middle Eastern Medical Center? Endocr. Pract. 2021, 27, 607–613. [Google Scholar] [CrossRef]
- Pitoia, F.; Jerkovich, F. Dynamic risk assessment in patients with differentiated thyroid cancer. Endocr. Relat. Cancer 2019, 26, R553–R566. [Google Scholar] [CrossRef]
- Grani, G.; Zatelli, M.C.; Alfò, M.; Montesano, T.; Torlontano, M.; Morelli, S.; Deandrea, M.; Antonelli, A.; Francese, C.; Ceresini, G.; et al. Real-World Performance of the American Thyroid Association Risk Estimates in Predicting 1-Year Differentiated Thyroid Cancer Outcomes: A Prospective Multicenter Study of 2000 Patients. Thyroid 2021, 31, 264–271. [Google Scholar] [CrossRef]
- Lamartina, L.; Durante, C.; Lucisano, G.; Bellantone, R.; Lombardi, C.P.; Pontecorvi, A.; Arvat, E.; Felicetti, F.; Zatelli, M.C.; Rossi, R.; et al. Are Evidence-Based Guidelines Reflected in Clinical Practice? An Analysis of Prospectively Collected Data of the Italian Thyroid Cancer Observatory. Thyroid 2017, 27, 1490–1497. [Google Scholar] [CrossRef] [PubMed]
- Lamartina, L.; Durante, C.; Filetti, S.; Cooper, D.S. Low-risk differentiated thyroid cancer and radioiodine remnant ablation: A systematic review of the literature. J. Clin. Endocrinol. Metab. 2015, 100, 1748–1761. [Google Scholar] [CrossRef] [PubMed]
- Maggiore, R.; Perticone, F.; Mari, G.; Pasquali, R.; Bosi, E.; Scavini, M.; Lanzi, R.; Rosati, R. Impact of the 8th Edition of the AJCC-TNM Staging System on Estimated Cancer-Specific Survival in Patients Aged 45-54 Years at Diagnosis with Differentiated Thyroid Carcinoma: A Single Center Report. Int. J. Endocrinol. 2021, 2021, 8820364. [Google Scholar] [CrossRef]
- Casella, C.; Ministrini, S.; Galani, A.; Mastriale, F.; Cappelli, C.; Portolani, N. The New TNM Staging System for Thyroid Cancer and the Risk of Disease Downstaging. Front. Endocrinol. 2018, 9, 541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thewjitcharoen, Y.; Chatchomchuan, W.; Karndumri, K.; Porramatikul, S.; Krittiyawong, S.; Wanothayaroj, E.; Butadej, S.; Nakasatien, S.; Veerasomboonsin, V.; Kanchanapituk, A.; et al. Impacts of the American Joint Committee on Cancer (AJCC) 8th edition tumor, node, metastasis (TNM) staging system on outcomes of differentiated thyroid cancer in Thai patients. Heliyon 2021, 7, e06624. [Google Scholar] [CrossRef]
- Tocci, V.; Mirabelli, M.; Giuliano, S.; Chiefari, E.; Hagelskjær Knudsen, J.; Kvistgaard, H.; La Torre, D.; Aversa, A.; Foti, D.P.; Hvarregaard Christensen, J.; et al. A Partial Phenotype of adFNDI Related to the Signal Peptide c.55G>A Variant of the AVP Gene. Endocrines 2021, 2, 37–43. [Google Scholar] [CrossRef]
- Rachinsky, I.; Rajaraman, M.; Leslie, W.D.; Zahedi, A.; Jefford, C.; McGibbon, A.; Young, J.E.; Pathak, K.A.; Badreddine, M.; De Brabandere, S.; et al. Regional Variation across Canadian Centers in Radioiodine Administration for Thyroid Remnant Ablation in Well-Differentiated Thyroid Cancer Diagnosed in 2000–2010. J. Thyroid Res. 2016, 2016, 2867916. [Google Scholar] [CrossRef]


{kind=link}
| Clinical and Pathological Characteristics | N (%) or Mean ± SD (Range) |
|---|---|
| Female gender, N | 123 (80.9) |
| Age at DTC diagnosis, yr | 43 ± 14 (33–52) |
| Follow-up duration, yr | 9.0 ± 6.2 |
| Post-operative RAI administration, N | 131 (86.1) |
| Multifocality, N | 33 (21.7) |
| Lymph node metastases, N | 28 (18.4) |
| Maximum tumor size, mm | 25 ± 12.7 (15–30) |
| PTC histology, N Aggressive subtypes * | 139 (92.1) 25 (17.9) |
| FTC histology, N | 7 (4.6) |
| OCA histology, N | 6 (3.9) |
| Angioinvasion, N | 16 (10.5) |
| Extrathyroidal extension, N Microscopic | 34 (22.3) 30 (88.2) |
| Initial risk category, N | |
| AJCC/TNM 7th Edition | |
| Stage I Stage II Stage III Stage Iva Stage IVb Stage IVc | 108 (71.0) 19 (12.5) 19 (12.5) 5 (3.3) 0 (0) 1 (0.7) |
| AJCC/TNM 8th Edition | |
| Stage I Stage II Stage III Stage IV Stage IVb | 136 (89.5) 14 (9.2) 1 (0.7) 0 (0) 1 (0.7) |
| ATA risk classification | |
| Low Intermediate High | 82 (53.9) 60 (39.5) 10 (6.6) |
| Disease Status | N (%) |
|---|---|
| No evidence of disease | 133 (87.5) |
| Persistence or relapse of disease (neck US or biochemical testing) | 19 (12.5) |
| ATA Risk Classification | Patients with Persistent or Recurrent Disease, N (%) | OR (95%CI) | p-Value |
|---|---|---|---|
| Low | 5 (6.1) | Reference | - |
| Intermediate | 10 (16.7) | 2.722 (0.842–8.800) | 0.094 |
| High | 4 (40.0) | 9.223 (1.792–47.465) | 0.008 |
| ATA Risk Classification | Patients Subjected to RAI, N (%) | Risk of Persistence or Relapse of DTC with RAI, N (%) | Risk of Persistence or Relapse of DTC without RAI, N (%) | p-Value |
|---|---|---|---|---|
| Low | 65 (79.2) | 4/65 (6.2) | 1/15 (6.7) | 1.000 |
| Intermediate | 56 (93.4) | 10/56 (17.8) | 0/2 (0.0) | 1.000 |
| High | 10 (100) | 4/10 (40) | n.a. | n.a. |
| AJCC/TNM 7th Edition | Patients with Persistent or Recurrent Disease, N (%) | OR (95%CI) | p-Value | AJCC/TNM 8th Edition | Patients with Persistent or Recurrent Disease, N (%) | OR (95%CI) | p-Value |
|---|---|---|---|---|---|---|---|
| Stage I-II | 13 (10.3) | Reference | - | Stage I–II | 18 (12.0) | Reference | - |
| Stage III-IV | 6 (24.0) | 2.745 (0.930–8.103) | 0.068 | Stage III–IV | 1 (50.0) | 7.3 (0.439–122.443) | 0.165 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giuliano, S.; Mirabelli, M.; Chiefari, E.; Tocci, V.; Donnici, A.; Iuliano, S.; Salatino, A.; Foti, D.P.; Aversa, A.; Brunetti, A. The Initial ATA Risk Classification, but Not the AJCC/TNM Stage, Predicts the Persistence or Relapse of Differentiated Thyroid Cancer in Long-Term Surveillance. Endocrines 2022, 3, 512-521. https://doi.org/10.3390/endocrines3030041
Giuliano S, Mirabelli M, Chiefari E, Tocci V, Donnici A, Iuliano S, Salatino A, Foti DP, Aversa A, Brunetti A. The Initial ATA Risk Classification, but Not the AJCC/TNM Stage, Predicts the Persistence or Relapse of Differentiated Thyroid Cancer in Long-Term Surveillance. Endocrines. 2022; 3(3):512-521. https://doi.org/10.3390/endocrines3030041
Chicago/Turabian StyleGiuliano, Stefania, Maria Mirabelli, Eusebio Chiefari, Vera Tocci, Alessandra Donnici, Stefano Iuliano, Alessandro Salatino, Daniela Patrizia Foti, Antonio Aversa, and Antonio Brunetti. 2022. "The Initial ATA Risk Classification, but Not the AJCC/TNM Stage, Predicts the Persistence or Relapse of Differentiated Thyroid Cancer in Long-Term Surveillance" Endocrines 3, no. 3: 512-521. https://doi.org/10.3390/endocrines3030041