Genetic Variants Affecting Anti-VEGF Drug Response in Polypoidal Choroidal Vasculopathy Patients: A Systematic Review and Meta-Analysis

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
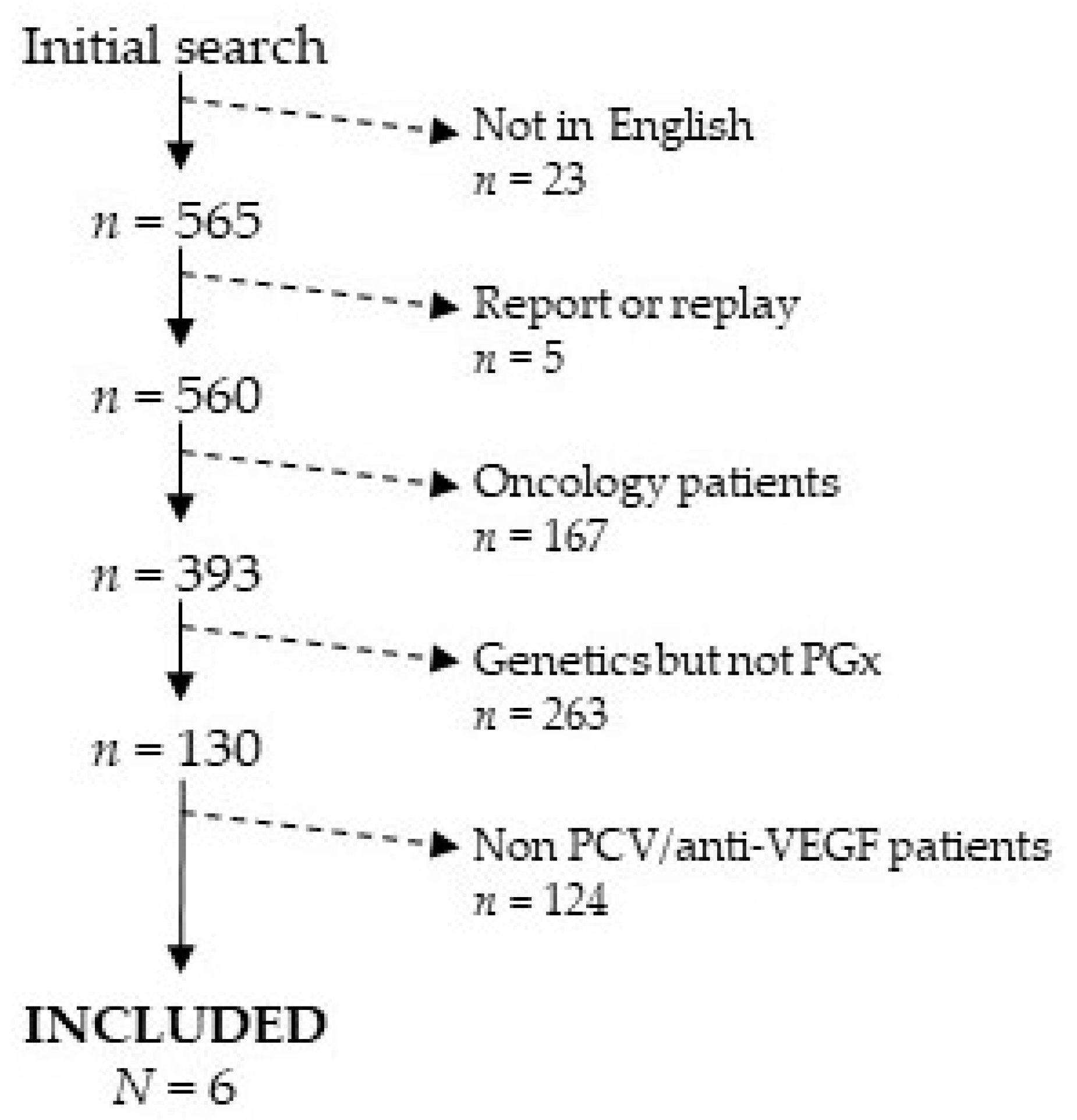
2.1. Search Strategy and Inclusion/Exclusion Criteria
- Manuscripts studying genetic variants affecting anti-VEGF drug response in oncology patients were excluded.
- Manuscripts published in journals not indexed in Journal Citation Reports (JCR) were excluded.
- Manuscripts regarding genetic variants related to the illness and not related to anti-VEGF drug response were excluded.
- Manuscripts studying the association of genetic variants with response to anti-VEGF drugs in non-PCV patients (only) were excluded.
- Manuscripts written in English (only) were included.
- Manuscripts studying the association of genetic variants with patients′ response to anti-VEGF drugs in PCV patients were included.
2.2. Data Extraction and Quality Assessment
2.3. Data Analysis
3. Results
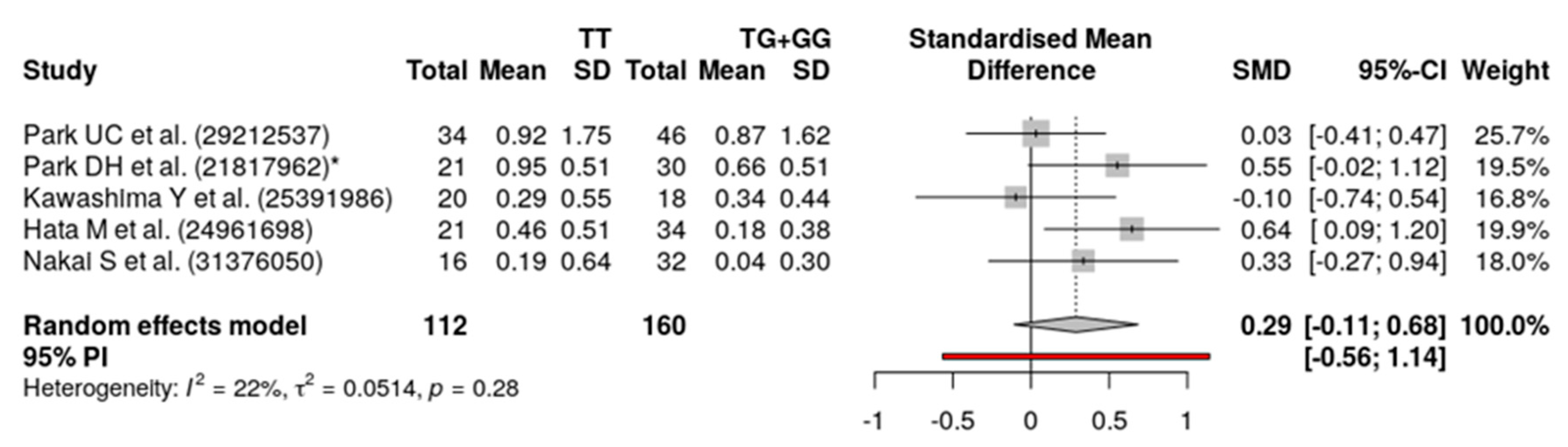
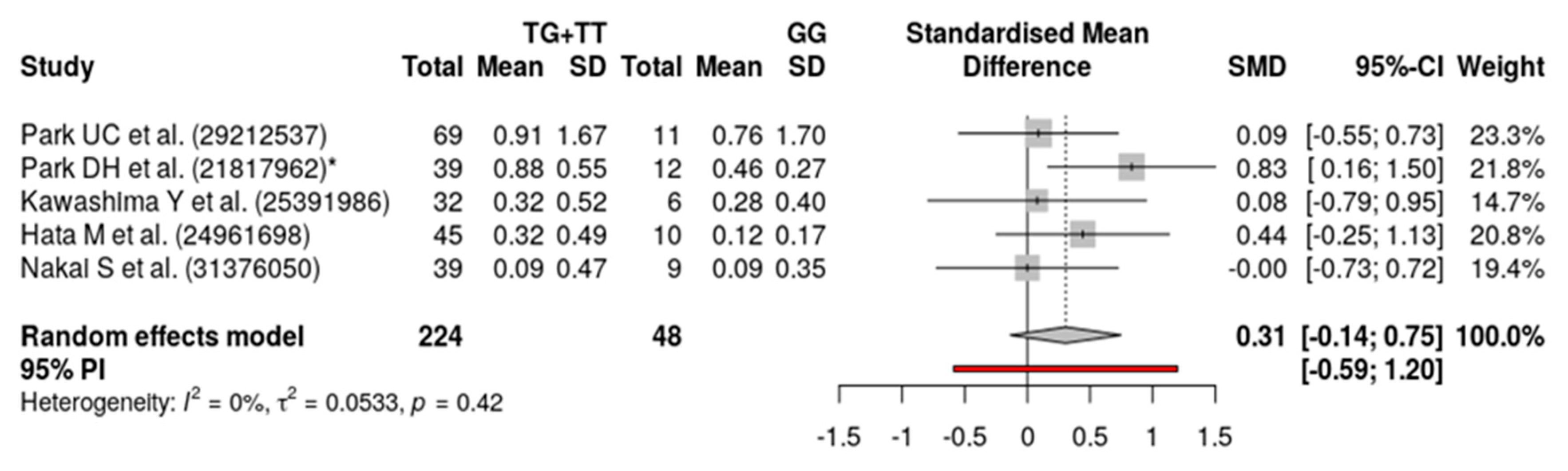
Meta-Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Grossniklaus, H.E.; Green, W.R. Choroidal neovascularization. Am. J. Ophthalmol. 2004, 137, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Spaide, R.F. Choriocapillaris flow features follow a power law distribution: Implications for characterization and mechanisms of disease progression. Am. J. Ophthalmol. 2016, 170, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Honda, S.; Matsumiya, W.; Negi, A. Polypoidal choroidal vasculopathy: Clinical features and genetic predisposition. Ophthalmologica 2014, 231, 59–74. [Google Scholar] [CrossRef] [PubMed]
- Laude, A.; Cackett, P.D.; Vithana, E.N.; Yeo, I.Y.; Wong, D.; Koh, A.H.; Wong, T.Y.; Aung, T. Polypoidal choroidal vasculopathy and neovascular age-related macular degeneration: Same or different disease? Prog. Retin. Eye Res. 2010, 29, 19–29. [Google Scholar] [CrossRef]
- Yannuzzi, L.A.; Sorenson, J.; Spaide, R.F.; Lipson, B. Idiopathic polypoidal choroidal vasculopathy (IPCV). Retina 2012, 32 (Suppl. 1), 1–8. [Google Scholar] [CrossRef]
- Imamura, Y.; Engelbert, M.; Iida, T.; Freund, K.B.; Yannuzzi, L.A. Polypoidal choroidal vasculopathy: A review. Surv. Ophthalmol. 2010, 55, 501–515. [Google Scholar] [CrossRef]
- Nakashizuka, H.; Mitsumata, M.; Okisaka, S.; Shimada, H.; Kawamura, A.; Mori, R.; Yuzawa, M. Clinicopathologic findings in polypoidal choroidal vasculopathy. Investig. Opthalmol. Vis. Sci. 2008, 49, 4729–4737. [Google Scholar] [CrossRef] [Green Version]
- Uyama, M.; Wada, M.; Nagai, Y.; Matsubara, T.; Matsunaga, H.; Fukushima, I.; Takahashi, K.; Matsumura, M. Polypoidal choroidal vasculopathy: Natural history. Am. J. Ophthalmol. 2002, 133, 639–648. [Google Scholar] [CrossRef]
- Matsumiya, W.; Honda, S.; Kusuhara, S.; Tsukahara, Y.; Negi, A. Effectiveness of intravitreal ranibizumab in exudative age-related macular degeneration (AMD): Comparison between typical neovascular AMD and polypoidal choroidal vasculopathy over a 1 year follow-up. BMC Ophthalmol. 2013, 13, 10. [Google Scholar] [CrossRef] [Green Version]
- Hikichi, T.; Higuchi, M.; Matsushita, T.; Kosaka, S.; Matsushita, R.; Takami, K.; Ohtsuka, H.; Kitamei, H.; Shioya, S. Results of 2 years of treatment with as-needed ranibizumab reinjection for polypoidal choroidal vasculopathy. Br. J. Ophthalmol. 2013, 97, 617–621. [Google Scholar] [CrossRef]
- Hikichi, T.; Ohtsuka, H.; Higuchi, M.; Matsushita, T.; Ariga, H.; Kosaka, S.; Matsushita, R.; Takami, K. Improvement of angiographic findings of polypoidal choroidal vasculopathy after intravitreal injection of ranibizumab monthly for 3 months. Am. J. Ophthalmol. 2010, 150, 674–682.e1. [Google Scholar] [CrossRef] [PubMed]
- Koh, A.; Lee, W.K.; Chen, L.J.; Chen, S.J.; Hashad, Y.; Kim, H.; Lai, T.Y.; Pilz, S.; Ruamviboonsuk, P.; Tokaji, E.; et al. EVEREST study: Efficacy and safety of verteporfin photodynamic therapy in combination with ranibizumab or alone versus ranibizumab monotherapy in patients with symptomatic macular polypoidal choroidal vasculopathy. Retina 2012, 32, 1453–1464. [Google Scholar] [CrossRef] [PubMed]
- Kokame, G.T.; Yeung, L.; Lai, J.C. Continuous anti-VEGF treatment with ranibizumab for polypoidal choroidal vasculopathy: 6-month results. Br. J. Ophthalmol. 2010, 94, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Tsujikawa, A.; Ooto, S.; Yamashiro, K.; Tamura, H.; Otani, A.; Yoshimura, N. Treatment of polypoidal choroidal vasculopathy by intravitreal injection of bevacizumab. Jpn. J. Ophthalmol. 2010, 54, 310–319. [Google Scholar] [CrossRef] [Green Version]
- Tano, Y. Guidelines for PDT in Japan. Ophthalmology 2008, 115, 585. [Google Scholar] [CrossRef]
- Gomi, F.; Ohji, M.; Sayanagi, K.; Sawa, M.; Sakaguchi, H.; Oshima, Y.; Ikuno, Y.; Tano, Y. One-year outcomes of photodynamic therapy in age-related macular degeneration and polypoidal choroidal vasculopathy in Japanese patients. Ophthalmology 2008, 115, 141–146. [Google Scholar] [CrossRef]
- Stangos, A.N.; Gandhi, J.S.; Nair-Sahni, J.; Heimann, H.; Pournaras, C.J.; Harding, S.P. Polypoidal choroidal vasculopathy masquerading as neovascular age-related macular degeneration refractory to ranibizumab. Am. J. Ophthalmol. 2010, 150, 666–673. [Google Scholar] [CrossRef]
- Rouvas, A.A.; Papakostas, T.D.; Ntouraki, A.; Douvali, M.; Vergados, I.; Ladas, I.D. Photodynamic therapy, ranibizumab, and ranibizumab with photodynamic therapy for the treatment of polypoidal choroidal vasculopathy. Retina 2011, 31, 464–474. [Google Scholar] [CrossRef]
- Cho, H.J.; Koh, K.M.; Kim, H.S.; Lee, T.G.; Kim, C.G.; Kim, J.W. Anti-vascular endothelial growth factor monotherapy in the treatment of submacular hemorrhage secondary to polypoidal choroidal vasculopathy. Am. J. Ophthalmol. 2013, 156, 524–531.e1. [Google Scholar] [CrossRef]
- Kokame, G.T.; Yeung, L.; Teramoto, K.; Lai, J.C.; Wee, R. Polypoidal choroidal vasculopathy exudation and hemorrhage: Results of monthly ranibizumab therapy at one year. Ophthalmologica 2014, 231, 94–102. [Google Scholar] [CrossRef]
- Whirl-Carrillo, M.; McDonagh, E.M.; Hebert, J.M.; Gong, L.; Sangkuhl, K.; Thorn, C.F.; Altman, R.B.; Klein, T.E. Pharmacogenomics knowledge for personalized medicine. Clin. Pharmacol. Ther. 2012, 92, 414–417. [Google Scholar] [CrossRef] [PubMed]
- Hautamäki, A.; Kivioja, J.; Seitsonen, S.; Savolainen, E.-R.; Liinamaa, M.J.; Luoma, A.; Jarvela, I.; Immonen, I. The IL-8, VEGF, and CFH polymorphisms and bevacizumab in age-related macular degeneration. Ophthalmology 2014, 121, 973–974.e2. [Google Scholar] [CrossRef] [PubMed]
- Lazzeri, S.; Figus, M.; Orlandi, P.; Fioravanti, A.; Di Desidero, T.; Agosta, E.; Sartini, M.S.; Posarelli, C.; Nardi, M.; Danesi, R.; et al. VEGF-Apolymorphisms predict short-term functional response to intravitreal ranibizumab in exudative age-related macular degeneration. Pharmacogenomics 2013, 14, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Abedi, F.; Wickremasinghe, S.; Richardson, A.J.; Makalic, E.; Schmidt, D.F.; Sandhu, S.S.; Baird, P.N.; Guymer, R. Variants in the VEGFA gene and treatment outcome after anti-VEGF treatment for neovascular age-related macular degeneration. Ophthalmology 2013, 120, 115–121. [Google Scholar] [CrossRef]
- Smailhodzic, D.; Muether, P.S.; Chen, J.; Kwestro, A.; Zhang, A.Y.; Omar, A.; Van De Ven, J.P.; Keunen, J.E.; Kirchhof, B.; Hoyng, C.B.; et al. Cumulative effect of risk alleles in CFH, ARMS2, and VEGFA on the response to ranibizumab treatment in age-related macular degeneration. Ophthalmology 2012, 119, 2304–2311. [Google Scholar] [CrossRef]
- Medina, F.M.C.; Da Motta, A.A.L.; Takahashi, W.Y.; Carricondo, P.C.; Motta, M.M.D.S.; Melo, M.B.; Vasconcellos, J.P.C. Pharmacogenetic effect of complement factor H gene polymorphism in response to the initial intravitreal injection of bevacizumab for wet age-related macular degeneration. Ophthalmic Res. 2015, 54, 169–174. [Google Scholar] [CrossRef]
- Brantley, M.A., Jr.; Edelstein, S.L.; King, J.M.; Plotzke, M.R.; Apte, R.S.; Kymes, S.M.; Shiels, A. Association of complement factor H and LOC387715 genotypes with response of exudative age-related macular degeneration to photodynamic therapy. Eye 2008, 23, 626–631. [Google Scholar] [CrossRef] [Green Version]
- Lorés-Motta, L.; Van Asten, F.; Muether, P.S.; Smailhodzic, D.; Groenewoud, J.M.; Omar, A.; Chen, J.; Koenekoop, R.K.; Fauser, S.; Hoyng, C.B.; et al. A genetic variant in NRP1 is associated with worse response to ranibizumab treatment in neovascular age-related macular degeneration. Pharm. Genom. 2016, 26, 20–27. [Google Scholar] [CrossRef] [Green Version]
- Tian, J.; Qin, X.; Fang, K.; Chen, Q.; Hou, J.; Li, J.; Yu, W.; Chen, D.; Hu, Y.; Li, X. Association of genetic polymorphisms with response to bevacizumab for neovascular age-related macular degeneration in the Chinese population. Pharmacogenomics 2012, 13, 779–787. [Google Scholar] [CrossRef]
- Chen, G.; Tzekov, R.; Li, W.; Jiang, F.; Mao, S.; Tong, Y. Pharmacogenetics of complement factor H Y402H polymorphism and treatment of neovascular AMD with anti-VEGF agents: A meta-analysis. Sci. Rep. 2015, 5, 14517. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.-L.; Chen, C.; Wang, Y.-X.; Tong, Y.; Fang, X.-L.; Li, L.; Wang, Z.-Y. Association between polymorphism rs11200638 in the HTRA1 gene and the response to anti-VEGF treatment of exudative AMD: A meta-analysis. BMC Ophthalmol. 2017, 17, 97. [Google Scholar] [CrossRef] [Green Version]
- Hu, Z.; Xie, P.; Ding, Y.; Yuan, D.; Liu, Q. Association between variants A69S in ARMS2 gene and response to treatment of exudative AMD: A meta-analysis. Br. J. Ophthalmol. 2015, 99, 593–598. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.; Shea, B.; O’connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2011. [Google Scholar]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, U.C.; Shin, J.Y.; Chung, H.; Yu, H.G. Association of ARMS2 genotype with response to anti-vascular endothelial growth factor treatment in polypoidal choroidal vasculopathy. BMC Ophthalmol. 2017, 17, 241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, D.H.; Kim, I.T. LOC387715/HTRA1 variants and the response to combined photodynamic therapy with intravitreal bevacizumab for polypoidal choroidal vasculopathy. Retina 2012, 32, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Kawashima, Y.; Oishi, A.; Tsujikawa, A.; Yamashiro, K.; Miyake, M.; Ueda-Arakawa, N.; Yoshikawa, M.; Takahashi, A.; Yoshimura, N. Effects of aflibercept for ranibizumab-resistant neovascular age-related macular degeneration and polypoidal choroidal vasculopathy. Graefe’s Arch. Clin. Exp. Ophthalmol. 2015, 253, 1471–1477. [Google Scholar] [CrossRef]
- Hata, M.; Tsujikawa, A.; Miyake, M.; Yamashiro, K.; Ooto, S.; Oishi, A.; Nakanishi, H.; Takahashi, A.; Yoshimura, N. Two-year visual outcome of ranibizumab in typical neovascular age-related macular degeneration and polypoidal choroidal vasculopathy. Graefe’s Arch. Clin. Exp. Ophthalmol. 2015, 253, 221–227. [Google Scholar] [CrossRef]
- Hata, M.; Tsujikawa, A.; Miyake, M.; Yamashiro, K.; Ooto, S.; Oishi, A.; Nakata, I.; Takahashi, A.; Yoshimura, N. Two-year visual outcome of polypoidal choroidal vasculopathy treated with photodynamic therapy combined with intravitreal injections of ranibizumab. Graefe’s Arch. Clin. Exp. Ophthalmol. 2015, 253, 189–197. [Google Scholar] [CrossRef]
- Nakai, S.; Matsumiya, W.; Miki, A.; Honda, S.; Nakamura, M. Association of an age-related maculopathy susceptibility 2 gene variant with the 12-month outcomes of intravitreal aflibercept combined with photodynamic therapy for polypoidal choroidal vasculopathy. Jpn. J. Ophthalmol. 2019, 63, 389–395. [Google Scholar] [CrossRef]
- Yamashiro, K.; Hosoda, Y.; Miyake, M.; Ooto, S.; Tsujikawa, A. Characteristics of pachychoroid diseases and age-related macular degeneration: Multimodal imaging and genetic backgrounds. J. Clin. Med. 2020, 9, 2034. [Google Scholar] [CrossRef]
- Dansingani, K.K.; Perlee, L.T.; Hamon, S.; Lee, M.; Shah, V.P.; Spaide, R.F.; Sorenson, J.; Klancnik, J.M.; Yannuzzi, L.A.; Barbazetto, I.A.; et al. Risk alleles associated with neovascularization in a pachychoroid phenotype. Ophthalmology 2016, 123, 2628–2630. [Google Scholar] [CrossRef] [PubMed]
- Yoneyama, S.; Sakurada, Y.; Kikushima, W.; Sugiyama, A.; Matsubara, M.; Fukuda, Y.; Tanabe, N.; Parikh, R.; Mabuchi, F.; Kashiwagi, K.; et al. Genetic factors associated with response to as-needed aflibercept therapy for typical neovascular age-related macular degeneration and polypoidal choroidal vasculopathy. Sci. Rep. 2020, 10, 7188. [Google Scholar] [CrossRef] [PubMed]
- Rondanelli, M.; Melzi d’Eril, G.V.; Anesi, A.; Ferrari, E. Altered oxidative stress in healthy old subjects. Aging 1997, 9, 221–223. [Google Scholar] [CrossRef] [PubMed]
- Johnson, L.V.; Leitner, W.P.; Staples, M.K.; Anderson, D.H. Complement activation and inflammatory processes in Drusen formation and age related macular degeneration. Exp. Eye Res. 2001, 73, 887–896. [Google Scholar] [CrossRef]
- Despriet, D.D.G.; Klaver, C.C.W.; Witteman, J.C.M.; Bergen, A.A.B.; Kardys, I.; De Maat, M.P.M.; Boekhoorn, S.S.; Vingerling, J.R.; Hofman, A.; Oostra, B.A.; et al. Complement factor H polymorphism, complement activators, and risk of age-related macular degeneration. JAMA 2006, 296, 301–309. [Google Scholar] [CrossRef] [Green Version]
- Lambert, N.G.; Elshelmani, H.; Singh, M.K.; Mansergh, F.C.; Wride, M.A.; Padilla, M.; Keegan, D.; Hogg, R.E.; Ambati, B.K. Risk factors and biomarkers of age-related macular degeneration. Prog. Retin. Eye Res. 2016, 54, 64–102. [Google Scholar] [CrossRef] [Green Version]
- Micklisch, S.; Lin, Y.; Jacob, S.; Karlstetter, M.; Dannhausen, K.; Dasari, P.; von der Heide, M.; Dahse, H.; Schmölz, L.; Grassmann, F.; et al. Age-related macular degeneration associated polymorphism rs10490924 in ARMS2 results in deficiency of a complement activator. J. Neuroinflamm. 2017, 14, 4. [Google Scholar] [CrossRef] [Green Version]
- Valverde-Megías, A.; Veganzones-de-Castro, S.; Donate-López, J.; Maestro-de-Las-Casas, M.L.; Megías-Fresno, A.; García-Feijoo, J. ARMS2 A69S polymorphism is associated with the number of ranibizumab injections needed for exudative age-related macular degeneration in a pro re nata regimen during 4 years of follow-up. Graefe’s Arch. Clin. Exp. Ophthalmol. 2017, 255, 2091–2098. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Ref SNP (rs) | Gene | Drug | Type | Pathology |
|---|---|---|---|---|
| rs4073 | CXCL8 | bevacizumab | Efficacy | Macular Degeneration |
| rs699947 | VEGFA | ranibizumab | Efficacy | Macular Degeneration |
| rs3025000 | VEGFA | bevacizumab, ranibizumab | Efficacy | Macular Degeneration |
| rs2070296 | NRP1 | ranibizumab | Efficacy | Macular Degeneration |
| rs10490924 | ARMS2 | bevacizumab | Efficacy | Macular Degeneration |
| rs1061170 | CFH | bevacizumab | Dosage | Macular Degeneration |
| rs1061170 | CFH | bevacizumab, ranibizumab | Efficacy | Macular Degeneration |
| rs833069 | VEGFA | ranibizumab | Efficacy | Macular Degeneration |
| rs11200638 | HTRA1 | bevacizumab, ranibizumab | Efficacy | Macular Degeneration |
| rs1061170 | CFH | photodynamic therapy | Efficacy | Macular Degeneration |
| rs5985 | F13A1 | photodynamic therapy | Efficacy | Choroidal Neovascularization |
| rs2010963 | VGFA | bevacizumab, pegaptanib, ranibizumab | Efficacy | Choroidal Neovascularization |
| Author | Ref SNP (rs) | Gene | SNP (Location) | MAF | Genotype mm/Mm/MM | Origin | Treatment | Patients | Follow-Up (Months) |
|---|---|---|---|---|---|---|---|---|---|
| Park UC et al. [35] | rs800292 | CFH | I62V | 0.290 | 4/46/45 | Korea | Ranibizumab or bevacizumab | PCV | 12 |
| rs1061170 | CFH | Y402H | 0.080 | 1/13/81 | Korea | Ranibizumab or bevacizumab | PCV | 12 | |
| rs9332739 | C2 | E318D | 0.019 | 1/1/93 | Korea | Ranibizumab or bevacizumab | PCV | 12 | |
| rs641153 | CFB | R32Q | 0.081 | 0/14/79 | Korea | Ranibizumab or bevacizumab | PCV | 12 | |
| rs429608 | SKIV2L | 3493G/A | 0.088 | 1/13/80 | Korea | Ranibizumab or bevacizumab | PCV | 12 | |
| rs699947 | VEGFA | C-2578A | 0.281 | 10/39/45 | Korea | Ranibizumab or bevacizumab | PCV | 12 | |
| rs3025039 | VEGFA | C936T | 0.247 | 6/36/53 | Korea | Ranibizumab or bevacizumab | PCV | 12 | |
| rs10490924 | ARMS2 | A69S | 0.375 | 12/40/42 | Korea | Ranibizumab or bevacizumab | PCV | 12 | |
| rs11200638 | HTRA1 | -625A/G | 0.370 | 12/41/42 | Korea | Ranibizumab or bevacizumab | PCV | 12 | |
| rs1136287 | PEDF | Met72Thr | 0.488 | 23/50/22 | Korea | Ranibizumab or bevacizumab | PCV | 12 | |
| Park DH et al. [36] | rs10490924 | ARMS2 | A69S | 0.412 | 12/18/21 | Korea | Bevacizumab + PDT | PCV | 12 |
| rs11200638 | HTRA1 | -625A/G | 0.382 | 10/19/22 | Korea | Bevacizumab + PDT | PCV | 12 | |
| Kawashima Y et al. [37] | rs10490924 | ARMS2 | A69S | 0.316 | 6/12/20 | Japan | 1st Ranibizumab; 2nd Aflibercept | PCV or nAMD | 6 |
| rs800292 | CFH | I62V | 0.184 | 2/10/26 | Japan | 1st Ranibizumab; 2nd Aflibercept | PCV or nAMD | 6 | |
| rs1061170 | CFH | Y402H | 0.145 | 1/9/28 | Japan | 1st Ranibizumab; 2nd Aflibercept | PCV or nAMD | 6 | |
| Hata M et al. [38] | rs10490924 | ARMS2 | A69S | 0.400 | 17/43/45 | Japan | Ranibizumab | PCV or nAMD | 24 |
| rs800292 | CFH | I62V | 0.246 | 7/38/61 | Japan | Ranibizumab | PCV or nAMD | 24 | |
| Hata M et al. [39] | rs10490924 | ARMS2 | A69S | 0.338 | 10/32/35 | Japan | Ranibizumab + PDT | PCV | 24 |
| rs800292 | CFH | I62V | 0.316 | 10/28/38 | Japan | Ranibizumab + PDT | PCV | 24 | |
| Nakai S et al. [40] | rs10490924 | ARMS2 | A69S | 0.427 | 9/23/16 | Japan | Aflibercept + PDT | PCV | 12 |
| Study | n | Gene | Change | Related Endpoint | p-Value |
|---|---|---|---|---|---|
| Park UC et al. * [35] | 81 | CFH | I62V | BCVA (Early Treatment Diabetic Retinopathy Study) | 0.039 |
| Total Foveal Thickness change | 0.255 | ||||
| Pigment Epithelium Detachment (PED) regression on OCT | 0.079 | ||||
| 81 | CFH | Y402H | BCVA (Early Treatment Diabetic Retinopathy Study) | 0.043 | |
| Total Foveal Thickness change | 0.551 | ||||
| Pigment Epithelium Detachment (PED) regression on OCT | 0.133 | ||||
| 80 | ARMS2 | A69S | BCVA (Early Treatment Diabetic Retinopathy Study) | 0.338 | |
| Total Foveal Thickness change | 0.212 | ||||
| Pigment Epithelium Detachment (PED) regression on OCT | 0.004 | ||||
| 81 | HTRA1 | -625A/G | BCVA (Early Treatment Diabetic Retinopathy Study) | 0.615 | |
| Total Foveal Thickness change | 0.276 | ||||
| Pigment Epithelium Detachment (PED) regression on OCT | 0.014 | ||||
| Park DH et al. [36] | 51 | ARMS2 | A69S | FA-GLD | 0.004 |
| ICGA-GLD | 0.972 | ||||
| Complete absence of leakage by FA | 0.04 | ||||
| Complete polyp regression by ICGA | 0.006 | ||||
| BCVA (Snellen visual acuity) | 0.034 | ||||
| 51 | HTRA1 | -625A/G | FA-GLD | 0.009 | |
| ICGA-GLD | 0.937 | ||||
| Complete absence of leakage by FA | 0.019 | ||||
| Complete polyp regression by ICGA | 0.002 | ||||
| BCVA (Snellen visual acuity) | 0.022 | ||||
| Kawashima Y et al. † [37] | 38 | ARMS2 | A69S | Visual acuity change (Landolt chart) | 0.91 |
| 38 | CFH | I62V | Visual acuity change (Landolt chart) | 0.44 | |
| 38 | CFH | Y402H | Visual acuity change (Landolt chart) | 0.24 | |
| Hata M et al. [38] | 70 | ARMS2 | A69S | BCVA (Landolt chart) | 0.942 |
| 70 | CFH | I62V | BCVA (Landolt chart) | 0.352 | |
| Hata M et al. [39] | 77 | ARMS2 | A69S | BCVA (Landolt chart) at 12 months/24 months | 0.957/0.048 |
| 76 | CFH | I62V | BCVA (Landolt chart) at 12 months/24 months | 0.439/0.664 | |
| Nakai S et al. [40] | 48 | ARMS2 | A69S | BCVA | 0.235 |
| Central Retinal Thickness | 0.381 | ||||
| Subfoveal Choroidal thickness | 0.133 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Díaz-Villamarín, X.; Blánquez-Martínez, D.; Pozo-Agundo, A.; Pérez-Gutiérrez, A.M.; Muñoz-Ávila, J.I.; Antúnez-Rodríguez, A.; Fernández-Gómez, A.E.; García-Navas, P.; Martínez-González, L.J.; Dávila-Fajardo, C.L. Genetic Variants Affecting Anti-VEGF Drug Response in Polypoidal Choroidal Vasculopathy Patients: A Systematic Review and Meta-Analysis. Genes 2020, 11, 1335. https://doi.org/10.3390/genes11111335
Díaz-Villamarín X, Blánquez-Martínez D, Pozo-Agundo A, Pérez-Gutiérrez AM, Muñoz-Ávila JI, Antúnez-Rodríguez A, Fernández-Gómez AE, García-Navas P, Martínez-González LJ, Dávila-Fajardo CL. Genetic Variants Affecting Anti-VEGF Drug Response in Polypoidal Choroidal Vasculopathy Patients: A Systematic Review and Meta-Analysis. Genes. 2020; 11(11):1335. https://doi.org/10.3390/genes11111335
Chicago/Turabian StyleDíaz-Villamarín, Xando, David Blánquez-Martínez, Ana Pozo-Agundo, Ana María Pérez-Gutiérrez, José Ignacio Muñoz-Ávila, Alba Antúnez-Rodríguez, Ana Estefanía Fernández-Gómez, Paloma García-Navas, Luis Javier Martínez-González, and Cristina Lucía Dávila-Fajardo. 2020. "Genetic Variants Affecting Anti-VEGF Drug Response in Polypoidal Choroidal Vasculopathy Patients: A Systematic Review and Meta-Analysis" Genes 11, no. 11: 1335. https://doi.org/10.3390/genes11111335