Frailty Confers High Mortality Risk across Different Populations: Evidence from an Overview of Systematic Reviews and Meta-Analyses

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy and Study Selection
2.2. Selection Criteria
2.3. Data Extraction
2.4. Quality Assessment
2.5. Data Synthesis
3. Results
3.1. Characteristics of Included Studies
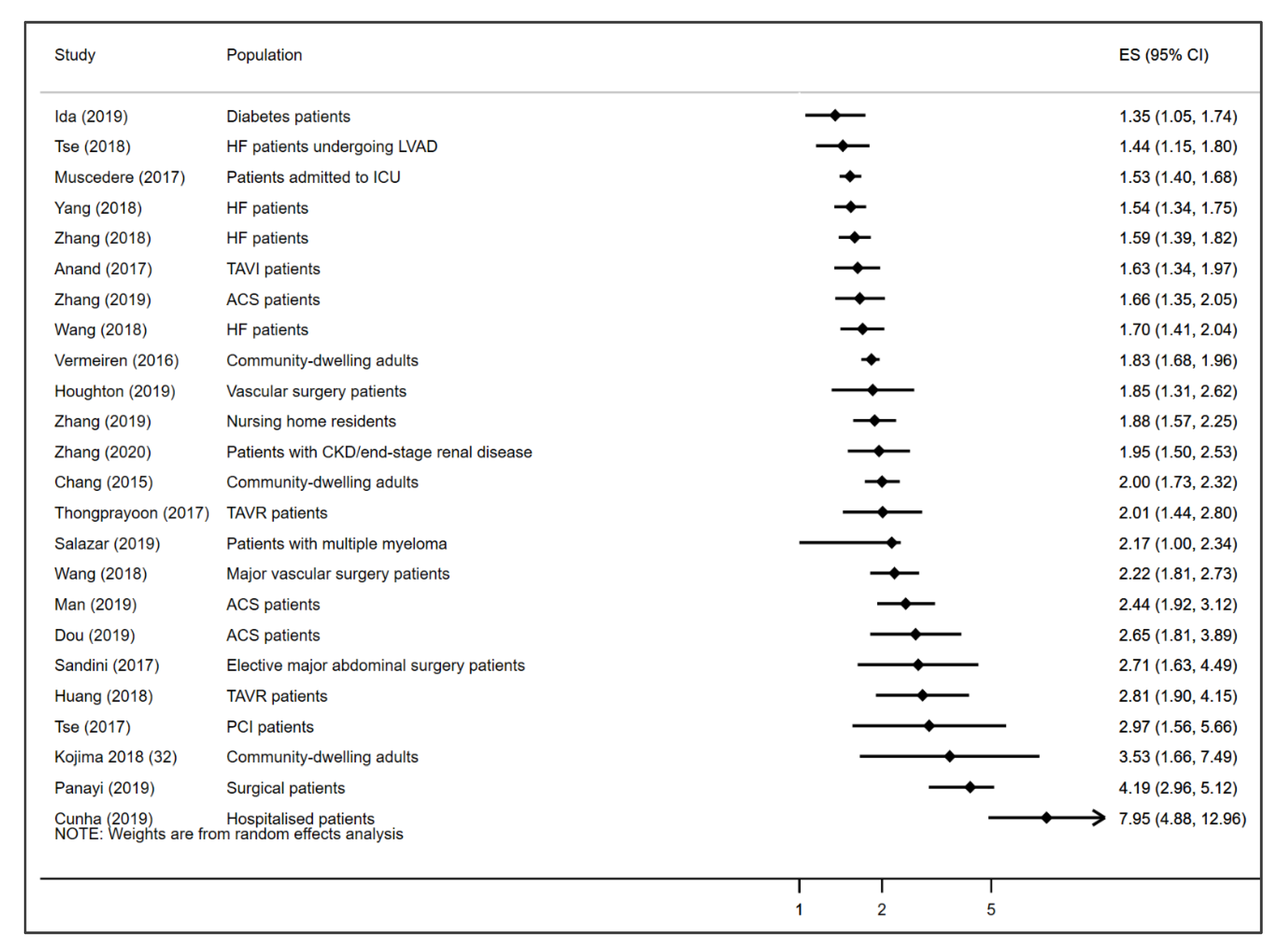
3.2. Association Between Frailty and All-Cause Mortality
3.3. Association between Pre-Frailty and All-Cause Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Xue, Q.L. The frailty syndrome: Definition and natural history. Clin. Geriatr. Med. 2011, 27, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clegg, A.; Young, J. The frailty syndrome. Clin. Med. 2011, 11, 72–75. [Google Scholar] [CrossRef] [PubMed]
- Ofori-Asenso, R.; Chin, K.L.; Mazidi, M.; Zomer, E.; Ilomaki, J.; Zullo, A.R.; Gasevic, D.; Ademi, Z.; Korhonen, M.J.; LoGiudice, D.; et al. Global Incidence of Frailty and Prefrailty Among Community-Dwelling Older Adults: A Systematic Review and Meta-analysis. JAMA Netw. Open 2019, 2, e198398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collard, R.M.; Boter, H.; Schoevers, R.A.; Oude Voshaar, R.C. Prevalence of frailty in community-dwelling older persons: A systematic review. J. Amer. Geriatr. Soc. 2012, 60, 1487–1492. [Google Scholar] [CrossRef] [PubMed]
- Hewitt, J.; Long, S.; Carter, B.; Bach, S.; McCarthy, K.; Clegg, A. The prevalence of frailty and its association with clinical outcomes in general surgery: A systematic review and meta-analysis. Age Ageing 2018, 47, 793–800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Handforth, C.; Clegg, A.; Young, C.; Simpkins, S.; Seymour, M.T.; Selby, P.J.; Young, J. The prevalence and outcomes of frailty in older cancer patients: A systematic review. Ann. Oncol 2015, 26, 1091–1101. [Google Scholar] [CrossRef]
- Kojima, G. Prevalence of Frailty in Nursing Homes: A Systematic Review and Meta-Analysis. J. Am. Med. Dir. Assoc. 2015, 16, 940–945. [Google Scholar] [CrossRef]
- Kojima, G. Frailty as a predictor of hospitalisation among community-dwelling older people: A systematic review and meta-analysis. J. Epidemiol. Community Health 2016, 70, 722–729. [Google Scholar] [CrossRef]
- Kojima, G. Frailty as a predictor of disabilities among community-dwelling older people: A systematic review and meta-analysis. Disabil. Rehabilit. 2017, 39, 1897–1908. [Google Scholar] [CrossRef]
- Cheng, M.H.; Chang, S.F. Frailty as a Risk Factor for Falls among Community Dwelling People: Evidence from a Meta-Analysis. J. Nurs. Scholarsh. 2017, 49, 529–536. [Google Scholar] [CrossRef]
- Kojima, G. Frailty significantly increases the risk of fractures among middle-aged and older people. Evid. Based Nurs. 2017, 20, 119–120. [Google Scholar] [CrossRef] [PubMed]
- Persico, I.; Cesari, M.; Morandi, A.; Haas, J.; Mazzola, P.; Zambon, A.; Annoni, G.; Bellelli, G. Frailty and Delirium in Older Adults: A Systematic Review and Meta-Analysis of the Literature. J. Am. Geriatr. Soc. 2018, 66, 2022–2030. [Google Scholar] [CrossRef] [PubMed]
- Kojima, G. Frailty as a Predictor of Nursing Home Placement Among Community-Dwelling Older Adults: A Systematic Review and Meta-analysis. J. Geriatr. Phys. Ther. 2018, 41, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Bock, J.O.; Konig, H.H.; Brenner, H.; Haefeli, W.E.; Quinzler, R.; Matschinger, H.; Saum, K.U.; Schottkerm, B.; Heider, D. Associations of frailty with health care costs—Results of the ESTHER cohort study. BMC Health Serv. Res. 2016, 16, 128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kojima, G. Frailty as a Predictor of Emergency Department Utilization among Community-Dwelling Older People: A Systematic Review and Meta-Analysis. J. Am. Med. Dir. Assoc. 2019, 20, 103–105. [Google Scholar] [CrossRef] [PubMed]
- Kojima, G. Increased healthcare costs associated with frailty among community-dwelling older people: A systematic review and meta-analysis. Arch. Gerontol. Geriatr. 2019, 84, 103898. [Google Scholar] [CrossRef]
- Klein, B.E.; Klein, R.; Knudtson, M.D.; Lee, K.E. Frailty morbidity and survival. Arch. Gerontol. Geriatr. 2005, 41, 141–149. [Google Scholar] [CrossRef]
- Ensrud, K.E.; Ewing, S.K.; Cawthon, P.M.; Fink, H.A.; Taylor, B.C.; Cauley, J.A.; Dam, T.T.; Marshall, L.M.; Orwoll, E.S.; Cummings, S.R.; et al. A comparison of frailty indexes for the prediction of falls, disability, fractures, and mortality in older men. J. Am. Geriatr. Soc. 2009, 57, 492–498. [Google Scholar] [CrossRef] [Green Version]
- Mousa, A.; Savva, G.M.; Mitnitski, A.; Rockwood, K.; Jagger, C.; Brayne, C.; Matthews, F.E. Is frailty a stable predictor of mortality across time? Evidence from the Cognitive Function and Ageing Studies. Age Ageing 2018, 47, 721–727. [Google Scholar] [CrossRef] [Green Version]
- Shamliyan, T.; Talley, K.M.; Ramakrishnan, R.; Kane, R.L. Association of frailty with survival: A systematic literature review. Ageing Res. Rev. 2013, 12, 719–736. [Google Scholar] [CrossRef]
- De Lepeleire, J.; Iliffe, S.; Mann, E.; Degryse, J.M. A Frailty: An emerging concept for general practice. Br. J. Gen. Pract. 2009, 59, e177–e182. [Google Scholar] [CrossRef] [PubMed]
- Fielding, R.A. A Summary of the Biological Basis of Frailty; Karger Publishers: Basel, Switzerland, 2015; pp. 41–44. [Google Scholar]
- Bergman, H.; Ferrucci, L.; Guralnik, J.; Hogan, D.B.; Hummel, S.; Karunananthan, S.; Wolfson, C. Frailty: An emerging research and clinical paradigm—Issues and controversies. J. Gerontol. Biol. Sci. Med. Sci. 2007, 62, 731–737. [Google Scholar] [CrossRef] [PubMed]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Fougère, B.; Morley, J.E. Weight loss is a major cause of frailty. J. Nutr. Health Aging 2017, 21, 933–935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Group P: Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.; Green, S. Cochrane Handbook of Systematic Reviews of Interventions; John Wiley and Sons, Ltd: Hoboken, NJ, USA, 2005. [Google Scholar]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [Green Version]
- Lopez-Plaza, B.; Bermejo, L.M.; Santurino, C.; Cavero-Redondo, I.; Alvarez-Bueno, C.; Gomez-Candela, C. Milk and Dairy Product Consumption and Prostate Cancer Risk and Mortality: An Overview of Systematic Reviews and Meta-analyses. Adv. Nutr. 2019, 10, S212–S223. [Google Scholar] [CrossRef]
- Alvarez-Bueno, C.; Cavero-Redondo, I.; Martinez-Vizcaino, V.; Sotos-Prieto, M.; Ruiz, J.R.; Gil, A. Effects of Milk and Dairy Product Consumption on Type 2 Diabetes: Overview of Systematic Reviews and Meta-Analyses. Adv. Nutr. 2019, 10, S154–S163. [Google Scholar] [CrossRef]
- Poole, R.; Kennedy, O.J.; Roderick, P.; Fallowfield, J.A.; Hayes, P.C.; Parkes, J. Coffee consumption and health: Umbrella review of meta-analyses of multiple health outcomes. BMJ 2017, 359, j5024. [Google Scholar] [CrossRef] [Green Version]
- Anand, A.; Harley, C.; Visvanathan, A.; Shah, A.S.V.; Cowell, J.; MacLullich, A.; Shenkin, S.; Mills, N.L. The relationship between preoperative frailty and outcomes following transcatheter aortic valve implantation: A systematic review and meta-analysis. Eur. Heart J. Qual. Care Clin. Outcomes 2017, 3, 123–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, L.; Zhou, X.; Yang, X.; Yu, H.; Baltatu, O.C. The impact of preoperative frailty status on outcomes after transcatheter aortic valve replacement: An update of systematic review and meta-analysis. Medicine 2018, 97, e13475. [Google Scholar] [CrossRef]
- Ida, S.; Kaneko, R.; Imataka, K.; Murata, K. Relationship between frailty and mortality, hospitalization, and cardiovascular diseases in diabetes: A systematic review and meta-analysis. Cardiovasc. Diabetol. 2019, 18, 81. [Google Scholar] [CrossRef] [PubMed]
- Kojima, G. Frailty Defined by FRAIL Scale as a Predictor of Mortality: A Systematic Review and Meta-analysis. J. Am. Med. Dir. Assoc. 2018, 19, 480–483. [Google Scholar] [CrossRef] [PubMed]
- Man, C.; Xiang, S.; Fan, Y. Frailty for predicting all-cause mortality in elderly acute coronary syndrome patients: A meta-analysis. Ageing Res. Rev. 2019, 52, 1–6. [Google Scholar] [CrossRef]
- Muscedere, J.; Waters, B.; Varambally, A.; Bagshaw, S.M.; Boyd, J.G.; Maslove, D.; Sibley, S.; Rockwood, K. The impact of frailty on intensive care unit outcomes: A systematic review and meta-analysis. Intensive Care Med. 2017, 43, 1105–1122. [Google Scholar] [CrossRef] [Green Version]
- Panayi, A.C.; COrkaby, A.R.; Sakthivel, D.; Endo, Y.; Varon, D.; Roh, D.; Orgill, D.P.; Neppl, R.L.; Javedan, H.; Bhasin, S.; et al. Impact of frailty on outcomes in surgical patients: A systematic review and meta-analysis. Am. J. Surg. 2019, 218, 393–400. [Google Scholar] [CrossRef]
- Salazar, A.S.; Recinos, L.M.; Mian, H.S.; Stoll, C.; Simon, L.E.; Sekhon, S.; Colditz, G.A.; Wildes, T.M. Geriatric Assessment and Frailty Scores Predict Mortality in Myeloma: Systematic Review and Meta-analysis. Clin. Lymphoma Myeloma Leuk. 2019, 19, 488. [Google Scholar] [CrossRef]
- Sandini, M.; Pinotti, E.; Persico, I.; Picone, D.; Bellelli, G.; Gianotti, L. Systematic review and meta-analysis of frailty as a predictor of morbidity and mortality after major abdominal surgery. BJS Open 2017, 1, 128–137. [Google Scholar] [CrossRef]
- Shu-Fang, C.; Pei-Ling, L. Frail phenotype and mortality prediction: A systematic review and meta-analysis of prospective cohort studies. Int. J. Nurs. Stud. 2015, 52, 1362–1374. [Google Scholar]
- Thongprayoon, C.; Cheungpasitporn, W.; Thamcharoen, N.; Ungprasert, P.; Kittanamongkolchai, W.; Mao, M.A.; Sakhuja, A.; Greason, K.L.; Kashani, K. Association of frailty status with acute kidney injury and mortality after transcatheter aortic valve replacement: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0177157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tse, G.; Gong, M.; Nunez, J.; Sanchis, J.; Li, G.; Ali-Hasan-Al-Saegh, S.; Wong, W.T.; Wong, S.H.; Wu, W.K.K.; Bazoukis, G.; et al. Frailty and Mortality Outcomes After Percutaneous Coronary Intervention: A Systematic Review and Meta-Analysis. J. Am. Med. Dir. Assoc. 2017, 18, 1097-e1. [Google Scholar] [CrossRef] [PubMed]
- Tse, G.; Gong, M.Q.; Wong, S.H.; Wu, W.K.K.; Bazoukis, G.; Lampropoulos, K.; Wong, W.T.; Xia, Y.L.; Wong, M.C.S.; Liu, T.; et al. Frailty and Clinical Outcomes in Advanced Heart Failure Patients Undergoing Left Ventricular Assist Device Implantation: A Systematic Review and Meta-analysis. J. Am. Med. Dir. Assoc. 2018, 19, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Vermeiren, S.; Vella-Azzopardi, R.; Beckwee, D.; Habbig, A.-K.; Scafoglieri, A.; Jansen, B.; Bautmans, I. Gerontopole Brussels Study g: Frailty and the Prediction of Negative Health Outcomes: A Meta-Analysis. J. Am. Med. Dir. Assoc 2016, 17, 1163-e1. [Google Scholar] [CrossRef]
- Wang, J.; Zou, Y.; Zhao, J.; Schneider, D.B.; Yang, Y.; Ma, Y.; Huang, B.; Yuan, D. The Impact of Frailty on Outcomes of Elderly Patients After Major Vascular Surgery: A Systematic Review and Meta-analysis. Eur. J. Vasc. Endovasc. Surg. 2018, 56, 591–602. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Zhou, C.; Li, Y.; Li, H.; Cao, Q.; Li, F. Prognostic Value of Frailty for Older Patients with Heart Failure: A Systematic Review and Meta-Analysis of Prospective Studies. BioMed Res. Int. 2018, 2018, 1–9. [Google Scholar] [CrossRef]
- Yang, X.; Lupón, J.; Vidán, M.T.; Ferguson, C.; Gastelurrutia, P.; Newton, P.J.; Macdonald, P.S.; Bueno, H.; Bayés-Genís, A.; Woo, J.; et al. Impact of Frailty on Mortality and Hospitalization in Chronic Heart Failure: A Systematic Review and Meta-Analysis. J. Am. Hear. Assoc. 2018, 7, e008251. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Dou, Q.; Zhang, W.; Wang, C.; Xie, X.; Yang, Y.; Zeng, Y. Frailty as a Predictor of All-Cause Mortality Among Older Nursing Home Residents: A Systematic Review and Meta-analysis. J. Am. Med Dir. Assoc. 2019, 20, 657–663. [Google Scholar] [CrossRef]
- Zhang, Y.; Yuan, M.; Gong, M.; Li, G.; Liu, T.; Tse, G. Associations Between Prefrailty or Frailty Components and Clinical Outcomes in Heart Failure: A Follow-up Meta-analysis. J. Am. Med Dir. Assoc. 2019, 20, 509–510. [Google Scholar] [CrossRef]
- Zhang, Y.P.; Yuan, M.; Gong, M.Q.; Tse, G.; Li, G.P.; Liu, T. Frailty and Clinical Outcomes in Heart Failure: A Systematic Review and Meta-analysis. J. Am. Med. Dir. Assoc. 2018, 19, 1003–1008. [Google Scholar] [CrossRef]
- Dou, Q.; Wang, W.; Wang, H.; Ma, Y.; Hai, S.; Lin, X.; Liu, Y.; Zhang, X.; Wu, J.; Dong, B. Prognostic value of frailty in elderly patients with acute coronary syndrome: A systematic review and meta-analysis. BMC Geriat. 2019, 19, 222. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Ma, Y.; Lin, F.; Zhao, J.; Xiong, J. Frailty and mortality among patients with chronic kidney disease and end-stage renal disease: A systematic review and meta-analysis. Int. Urol. Nephrol. 2020, 52, 363–370. [Google Scholar] [CrossRef]
- Houghton, J.S.M.; Nickinson, A.T.O.; Morton, A.J.; Nduwayo, S.; Pepper, C.J.; Rayt, H.S.; Gray, L.J.; Conroy, S.P.; Haunton, V.J.; Sayers, R.D. Frailty Factors and Outcomes in Vascular Surgery Patients. Ann. Surg. 2019. [Google Scholar] [CrossRef] [PubMed]
- Cunha, A.I.L.; Veronese, N.; Borges, S.D.M.; Ricci, N.A. Frailty as a predictor of adverse outcomes in hospitalized older adults: A systematic review and meta-analysis. Ageing Res. Rev. 2019, 56, 100960. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Meng, H.; Chen, Q.; Wang, X.; Zou, J.; Hao, Q.; Yang, M.; Wu, J. Is frailty a prognostic factor for adverse outcomes in older patients with acute coronary syndrome? Aging Clin. Exp. Res. 2019, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Fedarko, N.S. The Biology of Aging and Frailty. Clin. Geriatr. Med. 2011, 27, 27–37. [Google Scholar] [CrossRef] [Green Version]
- Morley, J.E. Frailty: diagnosis and management. J. Nutr. Health Aging 2011, 15, 667–670. [Google Scholar] [CrossRef] [Green Version]
- Sternberg, S.A.; Karunananthan, S.; Bergman, H.; Clarfield, A.M.; Schwartz, A.W. The Identification of Frailty: A Systematic Literature Review. J. Am. Geriatr. Soc. 2011, 59, 2129–2138. [Google Scholar] [CrossRef]
- Ambagtsheer, R.C.; Beilby, J.J.; Visvanathan, R.; Dent, E.; Yu, S.; Braunack-Mayer, A.J. Should we screen for frailty in primary care settings? A fresh perspective on the frailty evidence base: A narrative review. Prev. Med. 2019, 119, 63–69. [Google Scholar] [CrossRef]
- Rockwood, K.; Abeysundera, M.J.; Mitnitski, A. How should we grade frailty in nursing home patients? J. Am. Med Dir. Assoc. 2007, 8, 595–603. [Google Scholar] [CrossRef]
- Searle, S.D.; Mitnitski, A.; Gahbauer, E.A.; Gill, T.M.; Rockwood, K. A standard procedure for creating a frailty index. BMC Geriatr. 2008, 8, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vetrano, D.L.; Palmer, K.; Marengoni, A.; Marzetti, E.; Lattanzio, F.; Roller-Wirnsberger, R.; Samaniego, L.L.; Rodriguez-Mañas, L.; Bernabei, R.; Onder, G.; et al. Frailty and Multimorbidity: A Systematic Review and Meta-analysis. J. Gerontol. Ser. A Boil. Sci. Med Sci. 2018, 74, 659–666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanlon, P.; Nicholl, B.I.; Jani, B.D.; Lee, D.; McQueenie, R.; Mair, F.S. Frailty and pre-frailty in middle-aged and older adults and its association with multimorbidity and mortality: A prospective analysis of 493 737 UK Biobank participants. Lancet Public Heal. 2018, 3, e323–e332. [Google Scholar] [CrossRef]
- Gale, C.R.; Westbury, L.; Cooper, C. Social isolation and loneliness as risk factors for the progression of frailty: The English Longitudinal Study of Ageing. Age Ageing 2017, 47, 392–397. [Google Scholar] [CrossRef] [Green Version]
- Feng, Z.; Lugtenberg, M.; Franse, C.; Fang, X.; Hu, S.; Jin, C.; Raat, H. Risk factors and protective factors associated with incident or increase of frailty among community-dwelling older adults: A systematic review of longitudinal studies. PLoS ONE 2017, 12, e0178383. [Google Scholar] [CrossRef] [Green Version]
- Ofori-Asenso, R.; Chin, K.L.; Mazidi, M.; Zomer, E.; Ilomaki, J.; Ademi, Z.; Bell, J.S.; Liew, D. Natural Regression of Frailty Among Community-Dwelling Older Adults: A Systematic Review and Meta-Analysis. Gerontologist 2019. [Google Scholar] [CrossRef]
- Kojima, G.; Taniguchi, Y.; Iliffe, S.; Jivraj, S.; Walters, K. Transitions between frailty states among community-dwelling older people: A systematic review and meta-analysis. Ageing Res. Rev. 2019, 50, 81–88. [Google Scholar] [CrossRef]
- Puts, M.T.E.; Toubasi, S.; Andrew, M.K.; Ashe, M.C.; Ploeg, J.; Atkinson, E.; Ayala, A.P.; Roy, A.; Rodriguez-Monforte, M.; Bergman, H.; et al. Interventions to prevent or reduce the level of frailty in community-dwelling older adults: a scoping review of the literature and international policies. Age Ageing 2017, 46, 383–392. [Google Scholar] [CrossRef] [Green Version]
- Apostolo, J.; Cooke, R.; Bobrowicz-Campos, E.; Santana, S.; Marcucci, M.; Cano, A.; Vollenbroek-Hutten, M.; Germini, F.; D’Avanzo, B.; Gwyther, H.; et al. Effectiveness of interventions to prevent pre-frailty and frailty progression in older adults: A systematic review. JBI Database System Rev. Implement. Rep. 2018, 16, 140–232. [Google Scholar] [CrossRef]
- Travers, J.; Romero-Ortuno, R.; Bailey, J.; Cooney, M.T. Delaying and reversing frailty: A systematic review of primary care interventions. Br. J. Gen. Pract. 2019, 69, e61–e69. [Google Scholar] [CrossRef]
- Gordon, E.H.; Peel, N.; Samanta, M.; Theou, O.; Howlett, S.E.; Hubbard, R.E. Sex differences in frailty: A systematic review and meta-analysis. Exp. Gerontol. 2017, 89, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Hubbard, R.E. Sex Differences in Frailty. Interdiscip. Top. Gerontol. Geriatr. 2015, 41, 41–53. [Google Scholar] [PubMed]
- Franse, C.; Van Grieken, A.; Qin, L.; Melis, R.J.F.; Rietjens, J.A.C.; Raat, H. Socioeconomic inequalities in frailty and frailty components among community-dwelling older citizens. PLoS ONE 2017, 12, e0187946. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Author | Databases Searched | Search Period | No. of Studies Pooled | Population/Setting | Age | % Women | Countries of Included Studies | Follow up Duration | Total Sample (% Frail) | Exposures Assessed | Pre-Defined Frailty Measurement Criteria | Frailty Mortality HR/RRs (95% CI) | Model used | I2 | AMSTAR Quality Rating |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Anand et al. [33] | Medline, Embase and Cinahl | 1 January 2000 to 1 June 2015 | 7 | TAVI patients | Mean age: 81–86 y | 48–66% | Switzerland, Canada, Germany, Netherlands, Italy, USA | >30 days | 3159 (23.2%) | Frailty | Any | 1.63 (1.34–1.97) a | RE | 66.0% | Moderate |
| Huang et al. [34] | PubMed, Embase and Cochrane library | Inception to January 2018 | 10 | TAVR patients | NR | NR | USA, Poland, Germany, Spain, Japan, Switzerland | >6 months | 2992 (32.5%) | Frailty | Any | 2.81 (1.90–4.15) b | RE | 84.0% | Moderate |
| Ida et al. [35] | Medline, Cochrane central and Clinicaltrials.gov | Inception to 1 December 2018 | 4 (Frail vs. non-frail) 2 (pre-frail vs. non-frail) | Patients with diabetes | Mean age: 56–76 y | 46–67% | Italy, USA, Spain, Taiwan | 3–12 y | 563,761 (NR) | Frailty, Pre-frailty | Any | Frailty: 1.35 (1.05–1.74) a Pre-frailty: 1.09 (1.01–1.17) a | RE | 92.0% (Frailty) 89.0% (Pre-frailty) | Moderate |
| Kojima et al. [36] | Embase, Scopus, Medline, Cinahl PsycINFO and Google scholar | Inception to March 2018 | 3 | Community-dwelling middle-aged and older adults | Mean age: ≥59.9 y | 0–53.4% | UK, Mexico, Italy, Belgium, Denmark, France, Greece, Italy, Netherlands, Spain, Sweden, Switzerland | 2.4–4.3 y | 9273 (NR) | Frailty, Pre-frailty | FRAIL scale | Frailty: 3.53 (1.66–7.49) a** Pre-frailty: 1.75 (1.14–2.70) a | RE | 79.0% (Frailty) 64.0% (Pre-frailty) | Moderate |
| Man et al. [37] | PubMed and Embase | Inception to October 1 2018 | 5 (Frailty) 3 (Pre-frailty) | Patients with ACS | ≥65 y | 32.8–48.9 | Canada, Spain, France, Sweden | ≥12 months | 1270 (38.4%) | Frailty, Pre-frailty | Any | Frailty: 2.44 (1.92–3.12) a Pre-frailty:1.65 (1.01–2.69) a | FE | 0.0% (Frailty), 0.0% (pre-frailty) | Critically low |
| Muscedere et al. [38] | Cochrane central, Medline, Embase, PubMed, Cinahl and Clinicaltrials.gov | Inception to April 2017 | 6 | Patients admitted to the ICU | Mean age: 57.1–84.0 y | NR | USA, Canada, Turkey, France | >6 months | 2484 (42.8%) | Frailty | Any | 1.53 (1.40–1.68) b | RE | 0.0% | Moderate |
| Panayi et al. [39] | PubMed and Cochrane central | Inception to 1 January 2018 | 11 | Surgical patients (All surgeries) | NR | NR | USA, Canada | NR | 523,598 (70.7%) | Frailty | Modified frailty index (mFI) | 4.19 (2.96–5.12) b | RE | 91.0% | Moderate |
| Salazar et al. [40] | Medline, Embase, Scopus, Cochrane Database of Systematic Reviews, Cochrane Central, and Clinicaltrials.gov | Inception to August 2018 | 3 | Patients with multiple myeloma | Median age: 58–74 | NR | Italy, Czech Republic, Netherlands, China, Germany | 13–28 months | 1622 (NR) | Frailty | Any | 2.17 (1.00–2.34) a | RE | 33.7% | Critically low |
| Sandini et al. [41] | Medline, Embase, PubMed, Cochrane and Scopus libraries | 1990 to January 2017 | 8 | Elective major abdominal surgery patients | NR | NR | USA, Korea, Norway, Netherlands | Up to 1 y | 16,825 (NR) | Frailty | Any | 2.71 (1.63–4.49) a | RE | 88.3% | Moderate |
| Shu-Fang et al. [42] | Medline and CINAHL databases and the Cochrane Library | January 2001 to July 2014 | 11 | Community-dwelling older adults | ≥65 y | NR | France, Spain, USA, Israel, Finland | 1.5–10 y | 35538 (NR) | Frailty, Pre-frailty | Fried (CHS) criteria | Frailty:2.00 (1.73–2.32) a Pre-frailty: 1.34 (1.26–1.41) a | RE | 61.7% (Frailty) 0.0% (Pre-frailty) | Moderate |
| Thongprayoon et al. [43] | Medline, Embase, the Cochrane Central Register of Controlled Trials, and the Cochrane Database of Systematic Reviews | Inception to November 2016 | 8 | TAVR patients | NR | NR | USA, Germany, France | NR | 10,498 (NR) | Frailty | Any | 2.01 (1.44–2.80) b | RE | 58.0% | Moderate |
| Tse et al. [44] | PubMed and EMBASE | Inception to July 23 2017 | 8 | Patients who have undergone PCI | Mean age 69 y | 32 | Spain, Indonesia, UK, Japan, USA | Mean 2.5 y | 2332 (NR) | Frailty | Any | 2.97 (1.56–5.66) a | RE | 79.0% | Low |
| Tse et al. [45] | PubMed and Embase | Inception to September 11, 2017 | 7 | Advanced Heart Failure Patients Undergoing Left Ventricular Assist Device Implantation | Mean age 48–69 y | 20.8 | Mean 13 months | 2942 (13.5%) | Frailty | Any | 1.44 (1.15–1.80) a | FE | 0.0% | Moderate | |
| Vermeiren et al. [46] | PubMed, Web of Knowledge and PsycINFO | Inception to January 2016 | 17 | Community-dwelling older adults | ≥65 y | NR | USA, France, Spain, Cuba, Dominican Republic, Venezuela, Mexico, Peru, India, China, Italy, Finland | 10–120 months | 150,763 (NR) | Frailty | Any | 1.83 (1.68–1.98) a/b | n.s | 98.0% | Low |
| Wang et al. [47] | Medline, Embase, Cochrane, Scopus | Inception to September 2017 | 9 | Patients who have undergone major vascular surgery | Mean age ≥59.1 y | NR | Canada, USA, Japan | 1–8.4 y | 1957 (35.5%) | Frailty | Any | 2.22 (1.81–2.73) a | RE | 0.0% | Moderate |
| Wang et al. [48] | PubMed, Embase, Cochrane, Web of science | Inception to November 8 2017 | 6 | Patients with heart failure | Mean age: 82.6 y | 17.6 | USA, Italy, Spain | >30 days | 1747 (53.0%) | Frailty | Any | 1.70 (1.41–2.04) a | FE | 0.0% | Low |
| Yang et al. [49] | Medline, Embase, Cochrane Central | January 1966 to March 2018 | 8 | Patients with chronic heart failure | Mean age: 73.4 y | 40.1 | USA, Italy, Australia, Spain | NR | 2645 (50.7%) | Frailty | Any | 1.54 (1.34–1.75) a | RE | 0.0% | Moderate |
| Zhang et al. [50] | Medline, Embase, Cochrane Central | Inception to October 2018 | 14 | Nursing home residents | Mean age:84.9 | 72.1 | France, Spain, Canada, Belgium, USA, Japan, Poland, China, Australia | 0.5–9 y | 9076 (53.9%) | Frailty | Any | 1.88 (1.57–2.25) a | RE | 47.8% | Moderate |
| Zhang et al. [51] | Medline, Embase, Cochrane Central | Inception to October 2018 | 3 | Heart failure patients | NR | NR | USA, Spain | NR | NR | Frailty | Any | Pre-frailty: 1.51 (0.99–2.31) a | RE | 0.0% | Critically low |
| Zhang et al. [52] | PubMed and Embase | Inception to December 3 2017 | 20 | Patients with heart failure | Mean age: 79.9 y | 11.1–60.9 | USA, Spain, Italy, Australia, Canada, UK, Hong Kong | 0.5–12 y | 17201 (9.2–76%) | Frailty | Any | 1.59 (1.39–1.82) a | RE | 55.0% | Low |
| Dou et al. [53] | PubMed and Embase | Inception to July 1 2018 | 7 | Patients with ACS | ≥65 y | NR | Spain, France, Sweden, Canada, Japan, South Africa, Scandinavia, India, East Asia, Australia, New Zealand | In hospital to 56.4 months | 6658 (12.3%) | Frailty | Any | Frailty: 2.65 (1.81–3.89) a Pre-frailty: 1.41 (1.19–1.66) a | RE | 60.2% (Frailty) 0.0% (Pre-frailty) | Low |
| Zhang et al. [54] | PubMed, Web of Science, Embase and Cochrane Central databases | Inception to June 2019 | 11 | Patients with CKD or end-stage renal disease | Mean age: >45.0 y | USA, South Korea, India | 1–17 y | 127037 (7.9–82.0%) | Frailty | Fried (CHS) | 1.95 (1.50–2.53) a | RE | 82.0% | Low | |
| Houghton et al. [55] | Cinahl, PsycInfo, and Scopus | inception to September, 2018 | 9 | Vascular surgery patients | NR | USA, Japan, UK | NR | 2904 | Frailty | Any | 1.85 (1.31–2.62) a | RE | 74.0% | Low | |
| Cunha et al. [56] | PubMed, Embase, Web of Science, Lilacs, Cinahl, PsycInfo and Google Scholar | Inception to March 2019 | 4 (Frailty); 3 (Pre-frailty) | Hospitalized patients | NR | NR | 7–12 months | 2119 (86.6%) | Frailty, Pre-frailty | Any | Frailty: 7.95 (4.88–12.96)a, Pre-frailty: 3.65 (1.41–9.43) a | RE | 0.0% (Frailty), 28.0% (pre-frailty) | Moderate | |
| Zhang et al. [57] | Medline, Embase, and Cochrane Central | Inception to December 2018 | Patients with ACS | NR | NR | 15–60 Months | 4665 (12.8%) | Frailty | Any | 1.66 (1.35–2.05) a | FE | 11.0% | Low |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ofori-Asenso, R.; Chin, K.L.; Sahle, B.W.; Mazidi, M.; Zullo, A.R.; Liew, D. Frailty Confers High Mortality Risk across Different Populations: Evidence from an Overview of Systematic Reviews and Meta-Analyses. Geriatrics 2020, 5, 17. https://doi.org/10.3390/geriatrics5010017
Ofori-Asenso R, Chin KL, Sahle BW, Mazidi M, Zullo AR, Liew D. Frailty Confers High Mortality Risk across Different Populations: Evidence from an Overview of Systematic Reviews and Meta-Analyses. Geriatrics. 2020; 5(1):17. https://doi.org/10.3390/geriatrics5010017
Chicago/Turabian StyleOfori-Asenso, Richard, Ken Lee Chin, Berhe W. Sahle, Mohsen Mazidi, Andrew R. Zullo, and Danny Liew. 2020. "Frailty Confers High Mortality Risk across Different Populations: Evidence from an Overview of Systematic Reviews and Meta-Analyses" Geriatrics 5, no. 1: 17. https://doi.org/10.3390/geriatrics5010017