
Primary Health Care System Strengthening Project in Sri Lanka: Status and Challenges with Human Resources, Information Systems, Drugs and Laboratory Services
 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Setting
2.2.1. General Setting
2.2.2. Specific Setting
Healthcare System in Sri Lanka
PSSP Project
Empanelment of the Population
Trained Human Resources
Essential Drugs and Drug Supply Chain Management
Laboratory Services
Health Management Information System (HMIS)
2.3. Study Population
2.3.1. Quantitative Component
2.3.2. Qualitative Component
2.4. Data Collection, Study Variables, Data Source and Study Tools
2.4.1. Quantitative Component
2.4.2. Qualitative Component
2.5. Data Analysis
2.5.1. Quantitative Component
2.5.2. Qualitative Component
3. Results
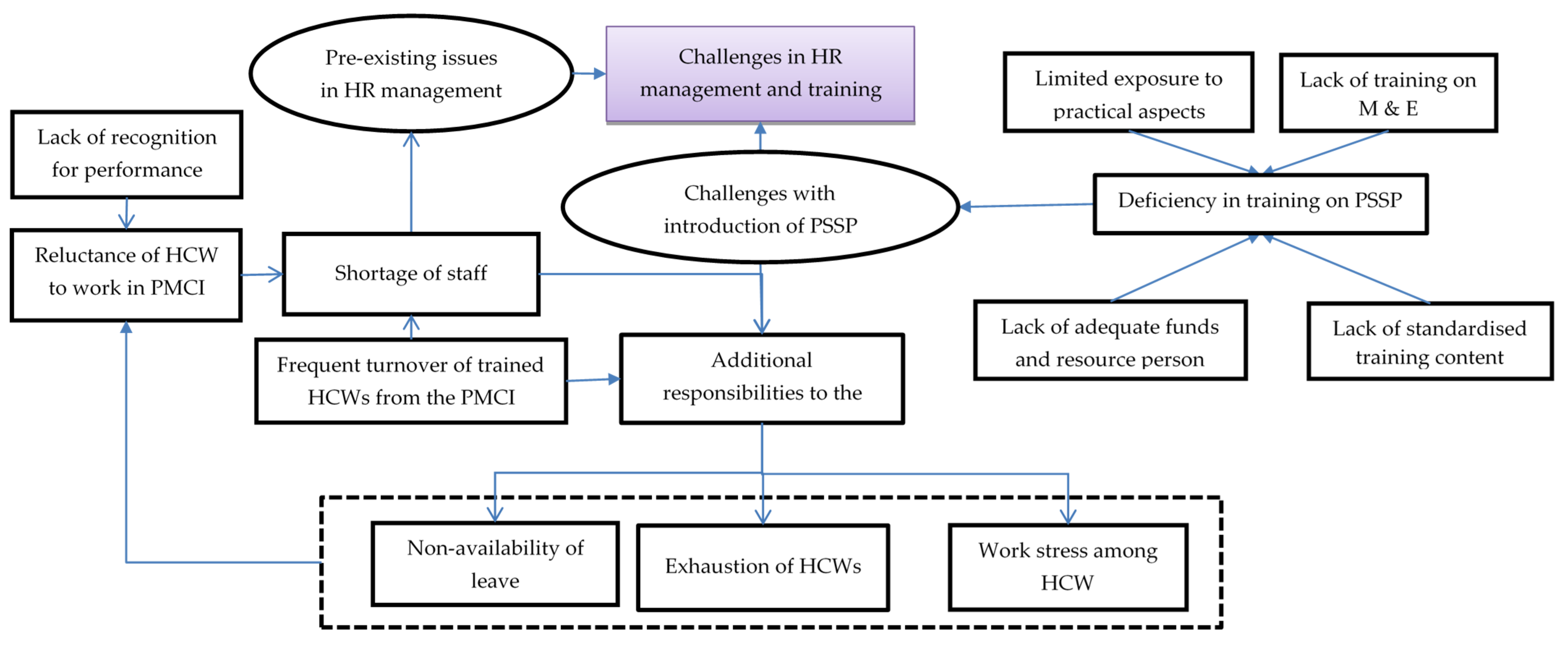
3.1. Human Resource and Training
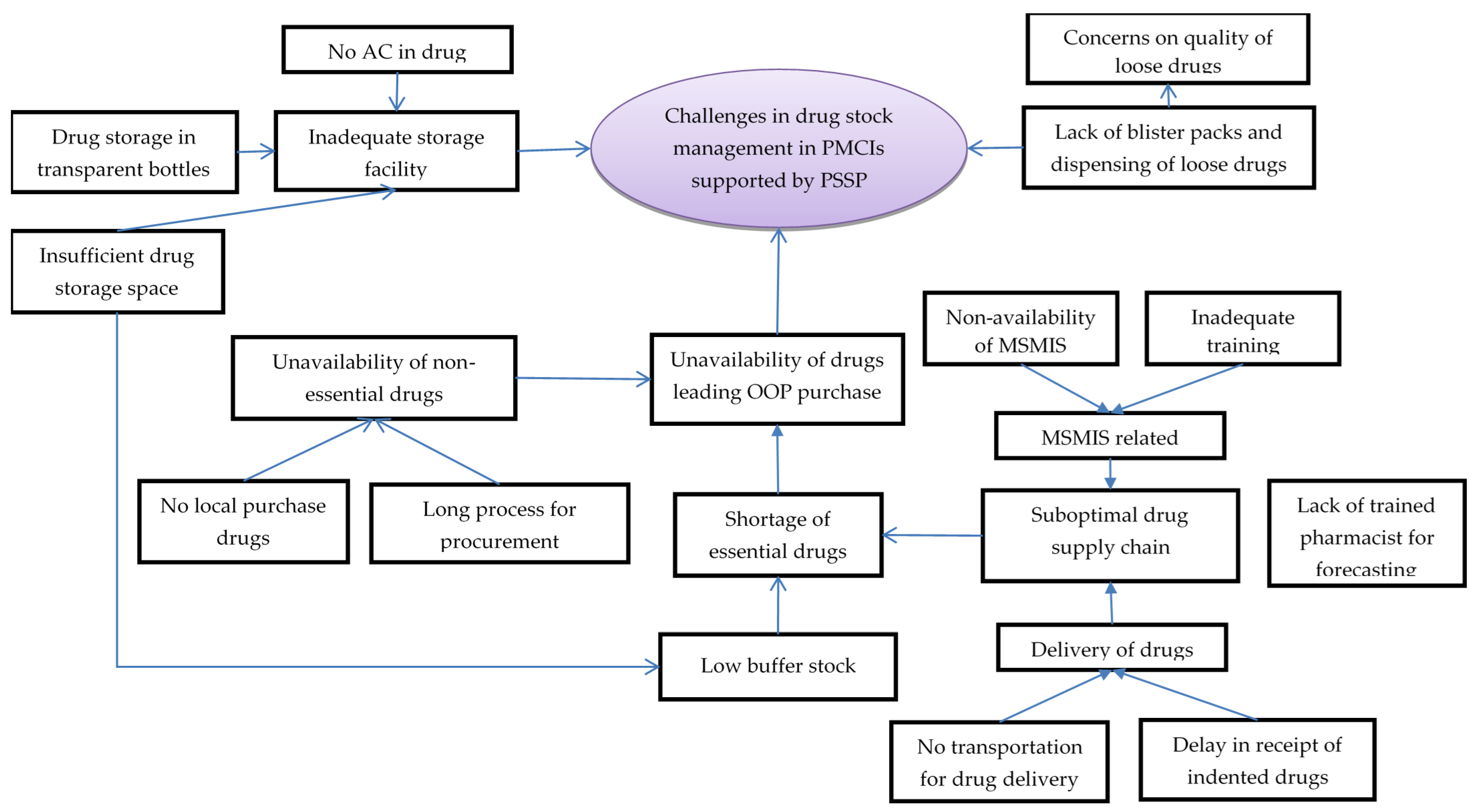
3.2. Essential Drugs and Supply Chain Management
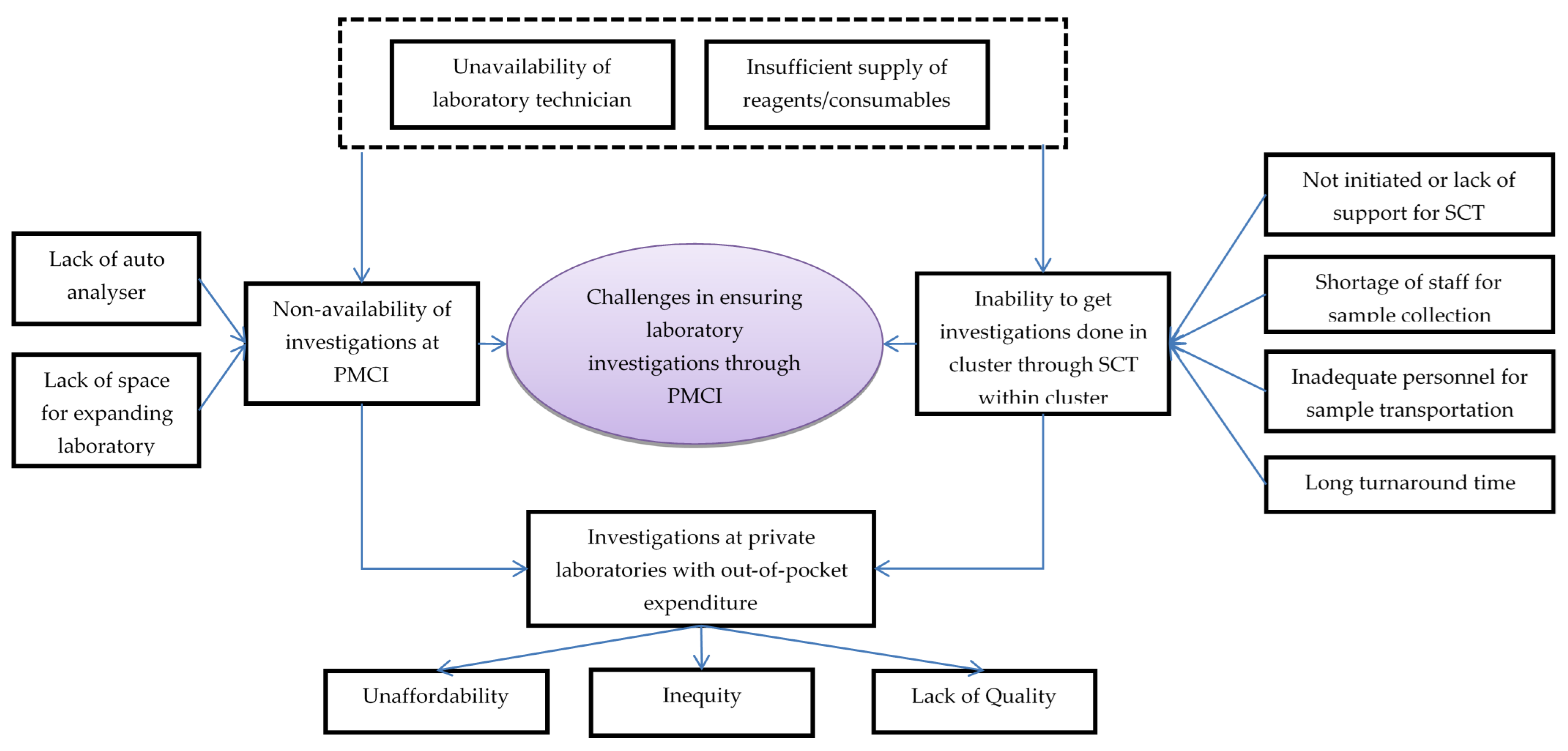
3.3. Laboratory Services
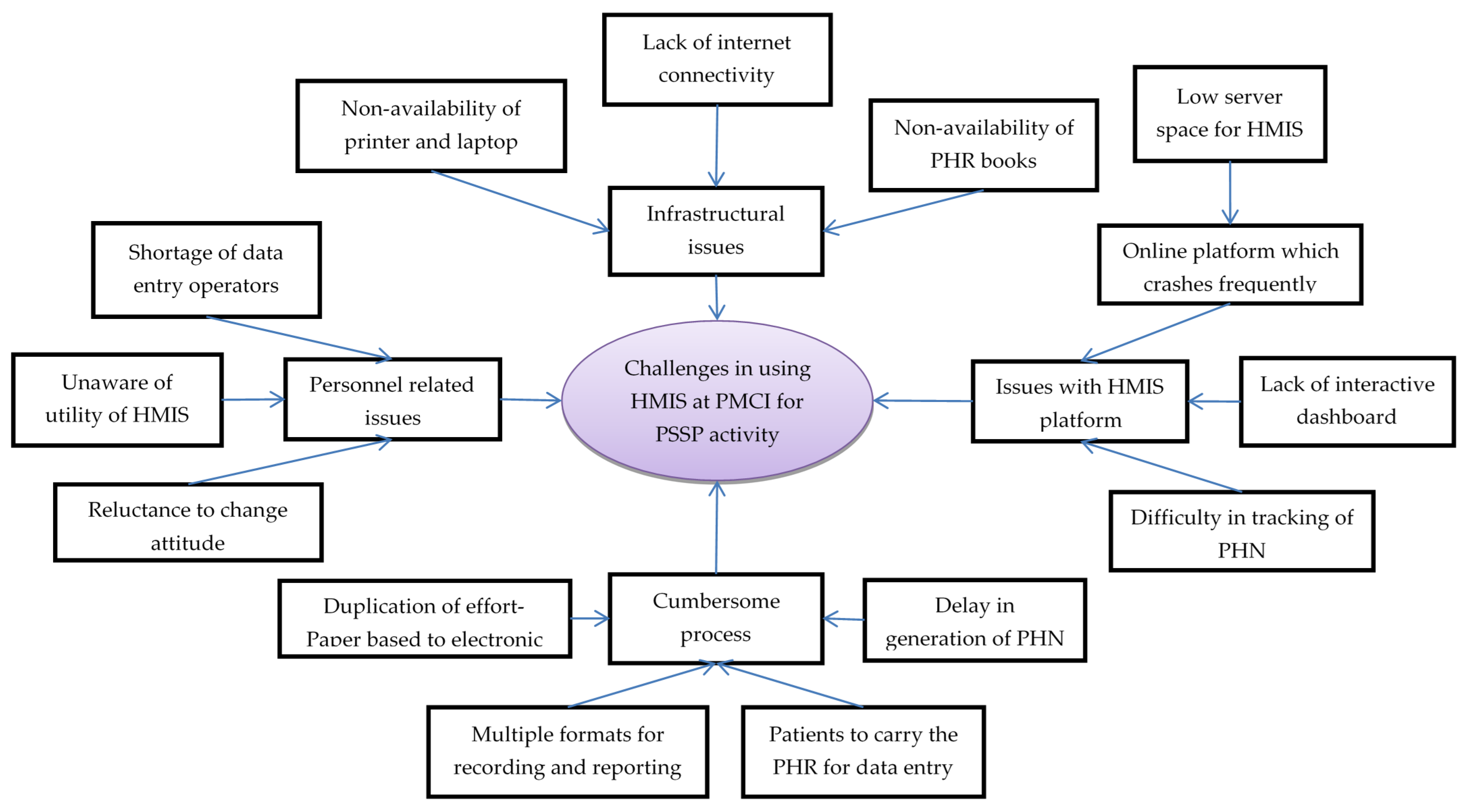
3.4. Health Management Information System (HMIS)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
List of Abbreviation
| Abbreviation | Definition |
| DALY | Disability Adjusted Life Year |
| DH | Divisional Hospital |
| DLI | Disbursement-Linked Indicator |
| GIS | Geographic Information System |
| GN | Grama Niladhari |
| HIMS | Health Information Management System |
| HLC | Health Lifestyle Centre |
| LMIC | Low-and-middle income country |
| MoH | Medical Office of Health |
| MOH | Ministry of Health |
| NCD | Non-communicable disease |
| OOPE | Out-of-Pocket Expenditure |
| PEN | Package of Essential NCD interventions for primary care |
| PHC | Primary Health Care |
| PHN | Personal Health Number |
| PHR | Personal Health Records |
| PMCI | Primary Medical Care Institution |
| PMCU | Primary Medical Care Units |
| PMU | Project Monitoring Unit |
| POCT | Point Of Care Test |
| PSSP | Primary Health Care System Strengthening Project |
| UHC | Universal Health Coverage |
| UN | United Nations |
| WHO | World Health Organization |
References
- World Health Organization (WHO). Noncommunicable Diseases—Fact Sheet. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 6 January 2021).
- World Health Organization (WHO). The Top 10 Causes of Death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 6 January 2021).
- GBD 2017 Causes of Death Collaborators. Global, Regional, and National Age-Sex-Specific Mortality for 282 Causes of Death in 195 Countries and Territories, 1980–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef] [Green Version]
- World Economic Programme; World Health Organization (WHO). From Burden to “Best Buys”: Reducing the Economic Impact of Non-Communicable Diseases in Low- and Middle-Income Countries; World Health Organization (WHO): Geneva, Switzerland, 2011. [Google Scholar]
- Samb, B.; Desai, N.; Nishtar, S.; Mendis, S.; Bekedam, H.; Wright, A.; Hsu, J.; Martiniuk, A.; Celletti, F.; Patel, K.; et al. Prevention and Management of Chronic Disease: A Litmus Test for Health-Systems Strengthening in Low-Income and Middle-Income Countries. Lancet 2010, 376, 1785–1797. [Google Scholar] [CrossRef]
- World Health Organization. Global Action Plan for the Prevention and Control of NCDs 2013–2020; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Pan American Health Organization (PAHO), World Health Organization (WHO). Third United Nations High-Level Meeting on NCDs. Available online: http://www3.paho.org/hq/index.php?option=com_content&view=article&id=14416:un-general-assembly-third-high-level-meeting-ncds-2018&Itemid=0&lang=en#gsc.tab=0 (accessed on 6 January 2021).
- Beaglehole, R.; Bonita, R.; Horton, R.; Adams, C.; Alleyne, G.; Asaria, P.; Baugh, V.; Bekedam, H.; Billo, N.; Casswell, S.; et al. Priority Actions for the Non-Communicable Disease Crisis. Lancet 2011, 377, 1438–1447. [Google Scholar] [CrossRef]
- Varghese, C.; Nongkynrih, B.; Onakpoya, I.; McCall, M.; Barkley, S.; Collins, T.E. Better Health and Wellbeing for Billion More People: Integrating Non-Communicable Diseases in Primary Care. BMJ 2019, 364, l327. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Package of Essential Noncommunicable (PEN) Disease Interventions for Primary Health Care in Low-Resource Settings; World Health Organization (WHO): Geneva, Switzerland, 2010. [Google Scholar]
- Leslie, H.H.; Spiegelman, D.; Zhoub, X.; Kruka, M.E. Service Readiness of Health Facilities in Bangladesh, Haiti, Kenya, Malawi, Namibia, Nepal, Rwanda, Senegal, Uganda and the United Republic of Tanzania. Bull. World Health Organ. 2017, 95, 738–748. [Google Scholar] [CrossRef]
- Huque, R.; Nasreen, S.; Ahmed, F.; Hicks, J.P.; Walley, J.; Newell, J.N.; Elsey, H. Integrating a Diabetes and Hypertension Case Management Package within Primary Health Care: A Mixed Methods Feasibility Study in Bangladesh. BMC Health Serv. Res. 2018, 18, 811. [Google Scholar] [CrossRef] [Green Version]
- Hyon, C.S.; Nam, K.Y.; Sun, H.C.; Garg, R.; Shrestha, S.M.; Ok, K.U.; Kumar, R. Package of Essential Noncommunicable Disease (PEN) Interventions in Primary Health-Care Settings in the Democratic People’s Republic of Korea: A Feasibility Study. WHO South-East Asia J. Public Health 2017, 6, 69–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wangchuk, D.; Virdi, N.; Garg, R.; Mendis, S.; Nair, N.; Wangchuk, D.; Kumar, R. Package of Essential Noncommunicable Disease (PEN) Interventions in Primary Health-Care Settings of Bhutan: A Performance Assessment Study. WHO South-East Asia J. Public Health 2014, 3, 154. [Google Scholar] [CrossRef] [Green Version]
- Aye, L.L.; Tripathy, J.P.; Maung Maung, T.; Oo, M.M.; Nwe, M.L.; Thu, H.M.M.; Ko, K.; Kaung, K.K. Experiences from the Pilot Implementation of the Package of Essential Non-Communicable Disease Interventions (PEN) in Myanmar, 2017–2018: A Mixed Methods Study. PLoS ONE 2020, 15, e0229081. [Google Scholar] [CrossRef] [Green Version]
- Kontsevaya, A.; Farrington, J. Implementation of a Package of Essential Noncommunicable (PEN) Disease Interventions in Kyrgyzstan: Evaluation of Effects and Costs in Bishkek after One Year; World Health Organization (WHO): Copenhagen, Denmark, 2017. [Google Scholar]
- Tesema, A.G.; Ajisegiri, W.S.; Abimbola, S.; Balane, C.; Kengne, A.P.; Shiferaw, F.; Dangou, J.-M.; Narasimhan, P.; Joshi, R.; Peiris, D. How Well Are Non-Communicable Disease Services Being Integrated into Primary Health Care in Africa: A Review of Progress against World Health Organization’s African Regional Targets. PLoS ONE 2020, 15, e0240984. [Google Scholar] [CrossRef]
- Mendis, S.; Al Bashir, I.; Dissanayake, L.; Varghese, C.; Fadhil, I.; Marhe, E. Gaps in Capacity in Primary Care in Low-Resource Settings for Implementation of Essential Noncommunicable Disease Interventions. Int. J. Hypertens. 2012, 2012, 584041. [Google Scholar] [CrossRef] [PubMed]
- Allen, L.; Nicholson, B.; Yeung, B.; Goiana-da-Silva, F. Implementation of Non-Communicable Disease Policies: A Geopolitical Analysis of 151 Countries. Lancet Glob. Health 2020, 8, e50–e58. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Service Availability and Readiness Assessment (SARA)—An Annual Monitoring System for Service Delivery Reference Manual; World Health Organization (WHO): Geneva, Switzerland, 2015. [Google Scholar]
- Institute for Health Metrics and Evaluation. GBD Results Tool—GHDx. Available online: http://ghdx.healthdata.org/gbd-results-tool (accessed on 6 January 2021).
- Senaratne, R.; Mendis, S. Prevention and Control of Noncommunicable Diseases: Think Globally—Act Locally; Lessons from Sri Lanka; Ministry of Health, Nutrition and Indigenous Medicine: Colombo, Sri Lanka, 2018.
- Ministry of Health Nutrition and Indigenous Medicine Department of Census and Statistics. Service Availability and Readiness Assessment Sri Lanka 2017; Ministry of Health, Nutrition and Indigenous Medicine: Colombo, Sri Lanka, 2018.
- Ministry of Health Nutrition and Indigenous Medicine. Reorganising Primary Health Care in Sri Lanka—Preserving Our Progress, Preparing Our Future; Ministry of Health, Nutrition and Indigenous Medicine: Colombo, Sri Lanka, 2017.
- World Health Organization (WHO). Colombo Declaration: Strengthening Health Systems to Accelerate Delivery of Noncommunicable Diseases Services at the Primary Health Care Level. In Proceedings of the Sixty-Ninth Session of the WHO Regional Committee for South-East Asia 2016, Colombo, Sri Lanka, 5–9 September 2016; World Health Organization (WHO): New Delhi, India, 2016. [Google Scholar]
- World Health Organization (WHO). Strengthening Health Systems to Accelerate Delivery of Noncommunicable Diseases Services at the Primary Health Care Leve—A One-Year Progress Review of the Implementation of the 2016 Colombo Declaration on NCDs; World Health Organization (WHO): New Delhi, India, 2017. [Google Scholar]
- Ministry of Health Nutrition and Indigenous Medicine. Road Map for the Primary Healthcare System Strengthening Project (PSSP); Ministry of Health, Nutrition and Indigenous Medicine: Colombo, Sri Lanka, 2019.
- The World Bank; Health Nutrition and Population Global Practice. Project Appraisal Document: Primary Health Care System Strengthening Project; The World Bank: Washington, DC, USA, 2018. [Google Scholar]
- Ministry of Health Nutrition and Indigenous Medicine. Guidelines for Operationalizing Primary Medical Care Services in Sri Lanka; Ministry of Health, Nutrition and Indigenous Medicine: Colombo, Sri Lanka, 2019.
- Creswell, J.; Plano Clark, V. Designing and Conducting Mixed Methods Research, 2nd ed.; Sage Publications Ltd.: London, UK, 2010. [Google Scholar]
- The World Bank. Sri Lanka—Data. Available online: https://data.worldbank.org/country/sri-lanka?view=chart (accessed on 6 January 2021).
- Government of Sri Lanka. List of Codes for the Administrative Divisions of Sri Lanka. 2001. Available online: https://web.archive.org/web/20110519151751/http://www.statistics.gov.lk/GNcode/introduction.pdf (accessed on 6 January 2021).
- Govindaraj, R.; Navaratne, K.; Cavagnero, E.; Seshadri, S.R. Health Care in Sri Lanka: What Can the Private Health Sector Offer; The World Bank: Washington, DC, USA, 2014. [Google Scholar]
- Ministry of Health. Summary of Government Hospitals. Available online: http://www.health.gov.lk/moh_final/english/others.php?pid=92 (accessed on 7 January 2021).
- DeJonckheere, M.; Vaughn, L.M. Semistructured Interviewing in Primary Care Research: A Balance of Relationship and Rigour. Fam. Med. Community Health 2019, 7, e000057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated Criteria for Reporting Qualitative Research (COREQ): A 32-Item Checklist for Interviews and Focus Groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Mijovic, H.; McKnight, J.; English, M. What Does the Literature Tell Us about Health Workers’ Experiences of Task-Shifting Projects in Sub-Saharan Africa? A Systematic, Qualitative Review. J. Clin. Nurs. 2016, 25, 2083–2100. [Google Scholar] [CrossRef] [Green Version]
- Hurst, K. Primary and Community Care Workforce Planning and Development. J. Adv. Nurs. 2006, 55, 757–769. [Google Scholar] [CrossRef]
- Bourgeault, I.L.; Chamberland-Rowe, C.; Simkin, S. Co-Developing an Integrated Primary Care Workforce Planning Approach at a Regional Level: Overarching Framework and Guiding Principles. Hum. Resour. Health 2021, 19, 87. [Google Scholar] [CrossRef]
- Aytona, M.G.; Politico, M.R.; McManus, L.; Ronquillo, K.; Okech, M. Determining Staffing Standards for Primary Care Services Using Workload Indicators of Staffing Needs in the Philippines. Hum. Resour. Health 2022, 19, 129. [Google Scholar] [CrossRef]
- Maleki, M.; Mardani, A.; Vaismoradi, M. Insecure Employment Contracts during the COVID-19 Pandemic and the Need for Participation in Policy Making. Int. J. Environ. Res. Public Health 2021, 18, 12548. [Google Scholar] [CrossRef]
- Steinmetz, S.; Vries, D.H.D.; Tijdens, K.G. Should I Stay or Should I Go? The Impact of Working Time and Wages on Retention in the Health Workforce. Hum. Resour. Health 2014, 12, 23. [Google Scholar] [CrossRef]
- Kaplan, R.L.; Burgess, T.E. The Impending Crisis. J. Microbiol. Biol. Educ. 2010, 11, 140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, K. The Laboratory Workforce Shortage Demands New Solutions—AACC.Org. Available online: https://www.aacc.org/cln/articles/2015/november/the-laboratory-workforce-shortage-demands-new-solutions (accessed on 19 April 2022).
- Strain, A.K.; Sullivan, M.M. Strengthening Laboratory Partnerships, Enhancing Recruitment, and Improving Through Training and Outreach Activities: The Minnesota. Public Health Rep. 2019, 134, 11S–15S. [Google Scholar] [CrossRef] [PubMed]
- Harb, R.; Kachimanga, C.; Bangura, M.; Kanawa, S.; Stratton, C.W.; Milner, D.A.; Eichbaum, Q. Providing Laboratory Medicine Training in a Low-Resource Setting: Lessons Learned From a Recent Experience in Sierra Leone. Am. J. Clin. Pathol. 2021, 155, 473. [Google Scholar] [CrossRef] [PubMed]
- Motta, L.A.; Shephard, M.D.S.; Brink, J.; Lawson, S.; Rheeder, P. Point-of-Care Testing Improves Diabetes Management in a Primary Care Clinic in South Africa. Prim. Care Diabetes 2017, 11, 248–253. [Google Scholar] [CrossRef] [PubMed]
- El-Osta, A.; Woringer, M.; Pizzo, E.; Verhoef, T.; Dickie, C.; Ni, M.Z.; Huddy, J.R.; Soljak, M.; Hanna, G.B.; Majeed, A. Does Use of Point-of-Care Testing Improve Cost-Effectiveness of the NHS Health Check Programme in the Primary Care Setting? A Cost-Minimisation Analysis. BMJ Open 2017, 7, e015494. [Google Scholar] [CrossRef] [Green Version]
- Laurence, C.O.; Gialamas, A.; Bubner, T.; Yelland, L.; Willson, K.; Ryan, P.; Beilby, J. Patient Satisfaction with Point-of-Care Testing in General Practice. Br. J. Gen. Pract. 2010, 60, 166–171. [Google Scholar] [CrossRef] [Green Version]
- Weigl, B.H.; Neogi, T.; McGuire, H. Point-of-Care Diagnostics in Low-Resource Settings and Their Impact on Care in the Age of the Noncommunicable and Chronic Disease Epidemic. J. Lab. Autom. 2014, 19, 248–257. [Google Scholar] [CrossRef] [Green Version]
- Kuupiel, D.; Tlou, B.; Bawontuo, V.; Drain, P.K.; Mashamba-Thompson, T.P. Poor Supply Chain Management and Stock-Outs of Point-of-Care Diagnostic Tests in Upper East Region’s Primary Healthcare Clinics, Ghana. PLoS ONE 2019, 14, e0211498. [Google Scholar] [CrossRef]
- Nybo, M.; Cadamuro, J.; Cornes, M.P.; Gómez Rioja, R.; Grankvist, K. Sample Transportation—An Overview. Diagnosis 2019, 6, 39–43. [Google Scholar] [CrossRef]
- Cureau, F.V.; Bloch, K.V.; Henz, A.; Schaan, C.W.; Klein, C.H.; De Oliveira, C.L.; Giannini, D.T.; De Leon, E.B.; de Azevedo Abreu, G.; Telo, G.H.; et al. Challenges for Conducting Blood Collection and Biochemical Analysis in a Large Multicenter School-Based Study with Adolescents: Lessons from ERICA in Brazil. Cad. Saude Publica 2017, 33, e00122816. [Google Scholar] [CrossRef]
- Gebregergs, G.B.; Sinishaw, M.A.; Shiferaw, M.B.; Antife, T.; Assefa, M.; Fiseha, D.; Klinkenberg, E. Evaluation of the Postal Service for Referral of Specimen of Drug Resistance Tuberculosis in Amhara Region, Ethiopia; Mixed Method. Afr. Health Sci. 2021, 21, 619–627. [Google Scholar] [CrossRef] [PubMed]
- Zaman, F.A.; Aggarwal, S.; Pal, R.; Chatterjee, P.K.; Kiran, K.A.; Panda, S.; Sharma, U.; Bhattacharya, T. Exploratory Study on the Operational Issues Faced in Collection, Transportation, and Laboratory Testing Related to COVID-19 in Remote Areas of Selected EAG States of North East and East India. J. Fam. Med. Prim. Care 2021, 10, 1452. [Google Scholar] [CrossRef]
- Kebede, Y.; Fonjungo, P.N.; Tibesso, G.; Shrivastava, R.; Nkengasong, J.N.; Kenyon, T.; Kebede, A.; Gadde, R.; Ayana, G. Improved Specimen-Referral System and Increased Access to Quality Laboratory Services in Ethiopia: The Role of the Public-Private Partnership. J. Infect. Dis. 2016, 213 (Suppl. 2), S59–S64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kassambara, H.; Nana, M.L.; Samassa, F.; Traoré, M.D. Sample Transport Optimization: Mali Pilot Study. Health Secur. 2020, 18, S92–S97. [Google Scholar] [CrossRef] [Green Version]
- Dama, E.; Nikiema, A.; Nichols, K.; Bicaba, B.W.; Porgho, S.; Greco Koné, R.; Tarnagda, Z.; Cissé, A.; Ngendakumana, I.; Adjami, A.; et al. Designing and Piloting a Specimen Transport System in Burkina Faso. Health Secur. 2020, 18, S98–S104. [Google Scholar] [CrossRef] [Green Version]
- Semret, M.; Ndao, M.; Jacobs, J.; Yansouni, C.P. Point-of-Care and Point-of-“can”: Leveraging Reference-Laboratory Capacity for Integrated Diagnosis of Fever Syndromes in the Tropics. Clin. Microbiol. Infect. 2018, 24, 836–844. [Google Scholar] [CrossRef] [Green Version]
- Tran, D.N.; Bero, L.A. Barriers and Facilitators to the Quality Use of Essential Medicines for Maternal Health in Low–Resource Countries: An Ishikawa Framework. J. Glob. Health 2015, 5, 010406. [Google Scholar] [CrossRef] [Green Version]
- Shukar, S.; Zahoor, F.; Hayat, K.; Saeed, A.; Gillani, A.H.; Omer, S.; Hu, S.; Babar, Z.U.D.; Fang, Y.; Yang, C. Drug Shortage: Causes, Impact, and Mitigation Strategies. Front. Pharmacol. 2021, 12, 1772. [Google Scholar] [CrossRef]
- Conn, V.S.; Ruppar, T.M.; Chan, K.C.; Dunbar-Jacob, J.; Pepper, G.A.; De Geest, S. Packaging Interventions to Increase Medication Adherence: Systematic Review and Meta-Analysis. Curr. Med. Res. Opin. 2015, 31, 145. [Google Scholar] [CrossRef] [Green Version]
- Tummers, J.; Tekinerdogan, B.; Tobi, H.; Catal, C.; Schalk, B. Obstacles and Features of Health Information Systems: A Systematic Literature Review. Comput. Biol. Med. 2021, 137, 104785. [Google Scholar] [CrossRef]
- Afrizal, S.H.; Handayani, P.W.; Hidayanto, A.N.; Eryando, T.; Budiharsana, M.; Martha, E. Barriers and Challenges to Primary Health Care Information System (PHCIS) Adoption from Health Management Perspective: A Qualitative Study. Inform. Med. Unlocked 2019, 17, 100198. [Google Scholar] [CrossRef]
- Feyzabadi, V.Y.; Emami, M.; Mehrolhassani, M.H. Health Information System in Primary Health Care: The Challenges and Barriers from Local Providers’ Perspective of an Area in Iran. Int. J. Prev. Med. 2015, 6, 57. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name of the Essential Drug | Drugs Available, n (%) | Adequate Buffer Stock *, n (%) | Stock Outs in 2020, n (%) | Receipt of Drugs within a Month, n (%) |
|---|---|---|---|---|
| Cardiovascular medicines | ||||
| Anti-arrhythmic medicines | ||||
| Adrenaline tartrate (0.1%)—1 mL Ampoule | 9 (100.0) | 1 (11.1) | 0 (0.0) | 6 (85.7) a |
| Anti-thrombotic medicines | ||||
| Aspirin tablet 150 mg | 5 (55.6) | 1 (20.0) * | 1 (11.1) | 5 (100.0) b |
| Aspirin tablet 75 mg | 3 (33.3) | 3 (100.0) # | 1 (11.1) | 3 (100.0) # |
| Lipid-lowering agents | ||||
| Atorvastatin tablet 10 mg | 9 (100.0) | 8 (88.9) | 1 (11.1) | 8 (88.9) |
| Anti-anginal medicines | ||||
| Glyceryl trinitrate tablet 0.5 mg sublingual | 9 (100.0) | 5 (55.5) | 1 (11.1) | 7 (77.8) |
| Nifedipine slow release tablet 20 mg | 9 (100.0) | 7 (77.8) | 2 (22.2) | 7 (87.5) c |
| Anti-hypertensive drugs | ||||
| Atenolol tablet 50 mg | 9 (100.0) | 6 (66.7) | 1 (11.1) | 7 (77.8) |
| Enalapril maleate tablet 5 mg | 8 (88.9) | 7 (77.8) | 3 (33.3) | 8 (88.9) |
| Frusemide—Injection 20 mg in 2 mL Ampoule | 9 (100.0) | 2 (22.2) | 0 (0.0) | 8 (88.9) |
| Frusemide tablet 40 mg | 9 (100.0) | 5 (55.5) | 1 (11.1) | 8 (88.9) |
| Hydrochlorothiazide tablet 25 mg | 9 (100.0) | 8 (88.9) | 1 (11.1) | 8 (88.9) |
| Losartan tablet 50 mg | 9 (100.0) | 7 (77.8) | 1 (11.1) | 9 (100.0) |
| Medicine for diabetics (Oral hypoglycaemic) | ||||
| Gliclazide tablet 40 mg and 80 mg | 8 (88.9) | 8 (100.0) | 3 (33.3) | 8 (88.9) |
| Metformin tablet 500 mg | 9 (100.0) | 9 (100.0) | 2 (22.2) | 8 (88.9) |
| Anti-asthmatic medicines | ||||
| Salbutamol Respiratory solution 0.5%/10 mL | 8 (88.9) | 6 (66.7) | 0 (0.0) | 7 (87.5) d |
| Salbutamol 2 mg tablet | 9 (100.0) | 3 (33.3) | 0 (0.0) | 8 (88.9) |
| Salbutamol 4 mg tablet | 0 (0.0) | NA ‡ | 0 (0.0) | NA ‡ |
| Theophylline Slow released tablet 125 mg | 8 (88.9) | 4 (44.4) | 1 (11.1) | 8 (88.9) |
| Name Laboratory/Diagnostic Services | Available through PMCI n (%) | Available at the PMCI n (%) | Availed at Apex Laboratories in the Cluster n (%) | Sample Collection Facilities for Specimens Sent to Apex Laboratories (%) a |
|---|---|---|---|---|
| Blood Glucose | 9 (100.0) | 7 (77.8) | 2 (22.2) | 1 (50.0) |
| HbA1C | 0 (0.0) | 0 (0.0) | 0 (0.0) | - |
| Total Cholesterol | 9 (100.0) | 7 (77.8) | 2 (22.2) | 1 (50.0) |
| Lipid Profile | 2 (22.2) | 2 (100.0) | 0 (0.0) | - |
| Serum Creatinine | 7 (77.8) | 4 (57.1) | 3 (42.9) | 2 (66.7) |
| Urine for glucose | 6 (66.7) | 6 (100.0) | 0 (0.0) | - |
| Urine for ketone bodies | 2 (22.2) | 2 (100.0) | 0 (0.0) | - |
| UACR | 1 (11.1) | 1 (100.0) | 0 (0.0) | - |
| OGTT | 6 (66.7) | 5 (83.3) | 1 (16.7) | 1 (100.0) |
| PAP-Smear | 1 (11.1) | 0 (0.0) | 1 (100) | 1 (100.0) |
| ALT/AST | 4 (44.4) | 4 (100.0) | 0 (0.0) | - |
| Complete Blood Count | 8 (88.9) | 6 (75.0) | 2 (25.0) | 2 (100.0) |
| AFB stain for TB | 2 (22.2) | 1 (50.0) | 1 (50.0) | 1 (100.0) |
| HIV | 3 (33.3) | 0 (0.0) | 3 (100.0) | 3 (100.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thekkur, P.; Fernando, M.; Nair, D.; Kumar, A.M.V.; Satyanarayana, S.; Chandraratne, N.; Chandrasiri, A.; Attygalle, D.E.; Higashi, H.; Bandara, J.; et al. Primary Health Care System Strengthening Project in Sri Lanka: Status and Challenges with Human Resources, Information Systems, Drugs and Laboratory Services. Healthcare 2022, 10, 2251. https://doi.org/10.3390/healthcare10112251
Thekkur P, Fernando M, Nair D, Kumar AMV, Satyanarayana S, Chandraratne N, Chandrasiri A, Attygalle DE, Higashi H, Bandara J, et al. Primary Health Care System Strengthening Project in Sri Lanka: Status and Challenges with Human Resources, Information Systems, Drugs and Laboratory Services. Healthcare. 2022; 10(11):2251. https://doi.org/10.3390/healthcare10112251
Chicago/Turabian StyleThekkur, Pruthu, Manoj Fernando, Divya Nair, Ajay M. V. Kumar, Srinath Satyanarayana, Nadeeka Chandraratne, Amila Chandrasiri, Deepika Eranjanie Attygalle, Hideki Higashi, Jayasundara Bandara, and et al. 2022. "Primary Health Care System Strengthening Project in Sri Lanka: Status and Challenges with Human Resources, Information Systems, Drugs and Laboratory Services" Healthcare 10, no. 11: 2251. https://doi.org/10.3390/healthcare10112251