
Analysis of Mobile App-Based Mental Health Solutions for College Students: A Rapid Review


Department of Industrial and Management Systems Engineering, Benjamin M. Statler College of Engineering and Mineral Resources, West Virginia University, Morgantown, WV 26506, USA
*
Author to whom correspondence should be addressed.
Healthcare 2023, 11(2), 272; https://doi.org/10.3390/healthcare11020272
Submission received: 28 December 2022
/
Revised: 12 January 2023
/
Accepted: 13 January 2023
/
Published: 16 January 2023
Abstract
:Background: College students are one of the most susceptible age groups to mental health problems. With the growing popularity of mobile health (mHealth), there is an increasing need to investigate its implications for mental health solutions. This review evaluates mHealth interventions for addressing mental health problems among college students. Methods: An online database search was conducted. Articles were required to focus on the impact of mHealth intervention on student mental health. Fifteen of the 487 articles, initially pulled from the search query, were included in the review. Results: The review identified three primary aspects of mental health: depression, anxiety, and stress. Research that found statistically significant improvements following mHealth intervention involved study durations between four and eight weeks, daily app use, guided lessons using cognitive behavioral therapy, acceptance and commitment therapy, and meditation. The review’s findings show that future work must address the concern of digital divide, gender and sex differences, and have larger sample sizes. Conclusions: There is potential to improve depressive symptoms and other similar mental health problems among college students via mobile app interventions. However, actions must be taken to improve barriers to communication and better reach the younger generations.
1. Introduction
Mental health can be defined as one’s condition regarding psychological, emotional, and social well-being. Instability of the mind can impact one’s thoughts, feelings, and actions [1]; thus, resulting challenges are expected. One of the most common mental health conditions is depression. The illness is recognized by a consistently low mood, loss of interest, and other debilitating emotions. Approximately 3.8% of the world is affected by depression. It is estimated that 20% of children and adolescents worldwide have some mental health problem, making it a global health concern [2].
Adolescents and young adults are a high risk for depression. According to the United States 2019 National Health Interview Survey, the highest rates of adult de-pression occurred among 18 to 29 year old (21% of participants had depressive symptoms) [2]. It is also reported that one in every five individuals experienced an episode by age 25 [3]. Within this age range falls a particular group of interest: college students. College students are known to be subject to high-stress environments, new experiences, and changing expectations during their education. In turn, they are particularly vulnerable to mental health challenges. It is estimated that one in every three college freshmen has mental health issues [4], and an estimated 9% of all students have depressive symptoms [5]. Unfortunately, public perception of mental illness is still recovering from barriers and past stigmatization. Whether or not people seek help, standard treatments are not always accessible; 95.6% of U.S. adults reported a barrier to mental healthcare access (the most critical link being affordability) [6]. Those affected often fail to recognize the severity of their conditions or fear being judged. College students are not immune to these barriers, typically being too embarrassed to seek treatment or wanting to work through their issues [7]. These beliefs can limit populations seeking traditional mental health treatments and pose challenges to awareness.
Mobile health (mHealth) technology has been growing in popularity to minimize some barriers to traditional mental healthcare [8,9]. The technology is unique for utilizing the increasing accessibility of mobile devices in the form of diagnostic apps, remote monitoring apps, mindfulness apps, text and video communication apps, and more. The technology has dramatically improved access to resources and treatment options across many populations. Young people and students are more likely to own and utilize mHealth apps. It is now timely and essential to evaluate the impact of mHealth treatments on students’ mental health.
In this study, we review the current research and successful techniques regarding mobile app mental health solutions for college students. The study will focus on depression and the ability of mobile apps to identify depressed students, present effective treatments for mental illness, and successfully rehabilitate users.
2. Materials and Methods
We leveraged the rapid review approach and analyzed information retrieved from PubMed and IEEE Xplore databases. Rapid reviews efficiently inform specific clinical or policy decisions promptly without losing much important information that may be expected from a comprehensive review. However, rapid reviews, although not exhaustive, should not be viewed as inherently inferior to full systematic reviews [10]. This approach is best suited for capturing timely information about fast-growing topics [8]. Synthesizing a standard systematic review, which is best suited to assess well-established topics, typically takes significant time to evaluate and analyze at least ten years of literature; therefore, fails to capture emerging issues. A rapid review speeds up the systematic review process by omitting stages of the systematic review making it less rigorous and precise [8,9].
2.1. Search Query
The keywords used to search for the papers were “students”, “mental health”, and “mobile” or “app”. The query used for students was: “student’s” [All Fields] OR “students” [MeSH Terms] OR “students” [All Fields] OR “student” [All Fields] OR “students” [All Fields]. The query used for mental health was: “mental health” [MeSH Terms] OR (“mental” [All Fields] AND “health” [All Fields]) OR “mental health” [All Fields]. The query used for mobile was: “mobile” [All Fields] OR “mobiles” [All Fields] OR “app” [All Fields].
2.2. Selection Criteria
Studies that tested for mental health problems related to depression were considered for evaluation. We considered studies that implemented a mobile app to improve depressive symptoms in young adults. Articles had to have focused on improving students’ mental health or the young adult populations using mHealth intervention. Note that the articles had to analyze the intervention’s impact, not just its feasibility. Articles older than five years were also removed from evaluation. The review included only articles published in English; the country of origin was not restricted. Apart from the desired information, the search resulted in many articles regarding mobile phone addiction and related issues, which were removed from the review.
Abstracts and, eventually, full articles were reviewed for their acceptability of the nature of this review. Two graduate students independently reviewed and coded the papers achieving an inter-reliability of 0.83. A third senior researcher then resolved the conflicts.
2.3. Coding and Data Extraction
Selected articles were categorized by country of origin, name of the app used, app’s accessibility (whether the app was accessible to the public or only to study participants), app methodology (the method of impacting the mental health of the users), intervention method (the mode via which the apps communicated with users), frequency of app use, duration of intervention, number of participants, participant dropout rate, participant gender, and ethnicity. We also captured the different mental health aspects analyzed by the studies and identified successful interventions where significant improvements were made.
3. Results
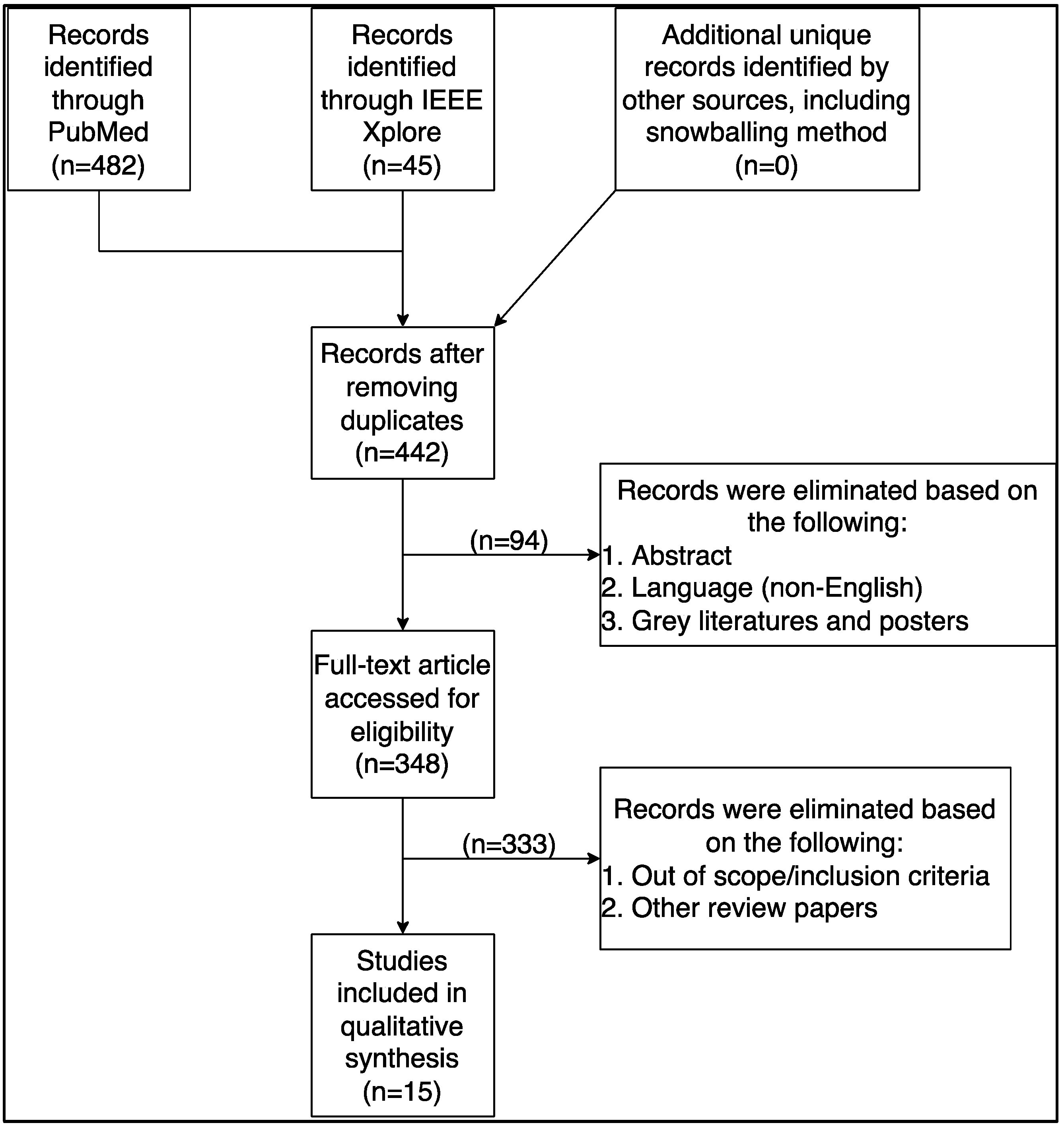
The search query yielded 487 (PubMed = 442, IEEE Xplore = 54) articles, of which articles published in the last five years were kept. Older articles or articles published in foreign languages were also excluded (n = 94). Review articles, conference abstracts, posters, opinion papers, letters to editors, editorials, book chapters, and other grey literature were excluded (n = 27). Others (n = 368) did not match our inclusion criteria and were excluded. Fifteen articles matched the inclusion criteria and were analyzed in this study. Figure 1 illustrates the review process.
As shown in Table 1, these studies were performed in developed nations across seven different countries, of which one was a multinational study [11], and one did not report their location [12]. Most studies were done in the United States of America [13,14,15,16,17] (n = 5), followed by Germany [18,19,20] (n = 3). The following countries are based on only one study each: Canada [21], Japan [22], Scotland [23], South Korea [24], and Sweden [25]. As shown in Table 1, all studies had significantly more female participants than male or other genders. On average, 72% of subjects identified as female in the evaluated studies. Half of the studies (50%) published the racial demographics of their subjects, of which 47% of the studies had minority representation in their participant pool. The studies had varying dropout rates that could be based on several factors. One study maintained all participants from baseline to completion [14]. Conversely, in another study, dropout rates reached 34% [23]. The studies averaged a 13% reduction from the baseline participant population to the final remarks.
3.1. Mobile App for Mental Health
As shown in Table 2, thirteen different apps were used across the fifteen studies. Most of the apps evaluated were available for public use before the study. [13,14,15,17,18,19,21,23] The other apps were created for their respective studies and await validation before seeking more widespread audiences [11,12,16,20,22,24,25]. The Calm app [15,23] and the StudiCare Stress app [11,20] were used by two studies, respectively. Other apps used by different studies included the ACT Daily app, [14] Balloon app, [19] DeStressify app [21], IntelliCare for College Students app [16], K-CESD-R Mobile App app [24], MCT & More app [18], Mental app [22], Metric Wire app [12], mHealth Positive Psychology Multicomponent Program app [25], Nod app [13], and Stop, Breathe and Think app [17]. Most apps leveraged a combination of methodologies to deliver diagnosis and treatment. The most common strategies were meditation and mindfulness [12,13,15,17,18,19,20,21,23] (n = 8), cognitive behavioral therapy [12,13,15,18,20,23] (n = 5), acceptance and commitment therapy [14,18,20] (n = 3), metacognitive training [18,19] (n = 2), and positive psychology [13,25] (n = 2). Other strategies enacted included varying kinds of surveys and emotion regulation strategies. The apps delivered these strategies via different means of presentations. Most apps (n = 9) used traditional guided exercises and lessons to impart their knowledge to users [11,14,15,16,17,18,19,20,21,23,25]. Other apps used combinations of virtual workshops, reflections, and self-monitoring [12,13,22,24]. The StudiCare Stress app and ACT Daily app used chatbots to interact with users and guide them through lessons. All apps used questionnaires and surveys to gauge user feelings.
Participants of the different studies were asked to use their respective apps for varying degrees of time. The most common assignment revolved around using the app once daily. This could be one prompt, one session, or one exercise daily, usually taking about ten minutes to complete [15,16,17,19,23,24,25]. Few studies required the participants to use the app once or twice every week [11,20]. Other studies required participants to use the app multiple times a day [12,14]; Some studies also left the frequency of interaction entirely up to users [13,22]. The most common intervention length was four weeks [13,17,18,21] and eight weeks [12,15,16,19]. The most extended intervention lasted ten weeks, [25] while the shortest lasted one week [23]. Post-evaluation follow-ups were noted in eight studies [11,13,14,15,20,21,23,25].
3.2. Mental Health Attributes and Assessment
Table 3 shows the three primary and five secondary attributes of mental ailments evaluated across different studies (primary: depression, anxiety, and stress; secondary: sleep quality, self-image, burnout, perception of quality of life, and general health). These attributes were selected in this review because of their relevance to depressive symptoms and frequency of use. The mental health attributes (themes) were noted at face value and reflected the studies’ definitions.
Twelve studies in this review tested the effectiveness of their app on the depression [11,12,13,14,16,17,18,20,21,22,24,25]. Six of those twelve studies found significant improvements in their participants’ symptoms before and after the intervention [11,12,14,18,20,25]. Two studies found no effective results but indications of substantial potential developments in the future [16,24]. Ten tested the effectiveness of their app in improving anxiety [11,12,13,14,16,17,20,21,24,25]. Of those ten studies, seven found significant improvements in their participants’ symptoms from before to after intervention [11,12,14,17,20,21,25]. Seven in this review tested the effectiveness of their app on stress [11,14,15,16,19,20,21]. Of those seven studies, six found significant improvements in their participants’ symptoms from before to after intervention [11,14,15,16,19,20]. Three studies tested the effectiveness of their app on sleep quality [13,15,21]. Of those three studies, one found significant improvements in their participants’ symptoms from before to after intervention [15]. Four studies tested the effectiveness of their app on self-image [11,15,18,20], of which three found significant improvements in their participants’ symptoms from before to after intervention [11,15,18]. Two studies tested the effectiveness of their app on burnout and found significant improvements in their participants’ symptoms from before to after intervention [11,20]. Three studies tested their app’s effectiveness on the perception of quality of life [18,19,21], of which one found significant improvements in their participants’ symptoms from before to after intervention [21]. Five studies tested the effectiveness of their app on general health and found significant improvements in their participants’ symptoms from before to after intervention [17,20,22,23,25].
Table 4 summarizes all the validated scales used by different studies to evaluate various aspects of mental health. Stress was measured using (a) Presenteeism Scale for Students (PSS) and (b) Depression, Anxiety, and Stress Scale (DASS). Depression was measured using the following eight different validated scales: (a) Center for Epidemiological Studies Depression Scale (CES-D), (b) Hospital Anxiety Depression Scale (HADS), (c) Patient Health Questionnaire (PHQ), (d) Quick Inventory for Depressive Symptomatology Self Report (QIDS-SR), (e) Montgomery-Asberg Depression Rating Scale (MADRS), (f) Hamilton Depression Rating Scale (HAM-D), (g) Ecological Momentary Assessment (EMA), and (h) DASS. Anxiety was measured using the following seven validated scales: (a) Spielberger State-Train Anxiety Inventory, (b) HADS, (c) Generalized Anxiety Disorder Scale (GAD), (d) Mini Social Phobia Inventory (MSPI), (e) Hamilton Anxiety Rating Scale (HAM-A), (f) EMA, and (g) DASS.
4. Discussion
4.1. Main Findings
Our review indicates a lack of studies evaluating the effectiveness of mHealth on students’ mental health problems and identified only fifteen published research. Since mHealth is rapidly increasing in popularity and the feasibility of such interventions is well accepted, the amount of data proving the best implementation method is underwhelming. There is a significant gap in overall research on the validity of mental health-based mobile apps.
When aiming to improve depression, cognitive behavioral therapy, acceptance and commitment therapy, mindfulness, positive psychology, and emotion regulation strategies were effective. Our review indicates that self-reflection is generally ineffective in addressing anxiety issues, meaning anxious participants may prefer to follow lessons than revisit past trauma. We also noted that longer intervention times (at least seven weeks) were most effective, meaning a more prolonged exposure to the app may help improve mental health conditions. Consistent and regular mindfulness practices via the mHealth app effectively improved the sleep quality of study participants across multiple studies. In improving the perception of self-image, guided lessons via mHealth apps were effective. Looking at burnout, improvements most often result in more extended intervention periods. The impact of mHealth on students’ general health perception was successful, where all five studies analyzed for the factor noted significant improvements in participants.
Our review noted a wide variety of interventions design across different studies, implying a need for further research to standardize the approach for optimal outcomes. In our review, the ideal setting for successfully improving the mental health of college students via mobile apps includes the following: one daily prompt averaging about 10 min; delivery via traditional guided exercises and lessons; content based on cognitive behavior therapy, acceptance and commitment therapy, and meditation; interventions lasting four to eight weeks with a follow-up.
4.2. Digital Divide
All fifteen studies identified in this review were conducted in high-income or developed nations, indicating the need for evaluating mHealth’s effectiveness on underserved and vulnerable populations across low-and-middle-income countries (LMICs). Compared to most other mobile technology, smartphones have penetrated and reached many rural and underserved regions across the globe, augmenting the potential of mHealth to improve access to affordable healthcare [26,27]. For many in LMICs, smartphones are often the only way to connect to the internet and access information and services, including healthcare. Unfortunately, mHealth and other mobile-based apps, instead of bridging the digital divide in healthcare, are contributing to the problem [28]. The digital divide results in unequal access to digital technology, resulting in inequality around access to resources, including healthcare services.
It must be understood that digital interventions must be user-centered, i.e., the technology interface, usability, and intervention design should cater to the end users’ needs. That being said, a mobile app designed and evaluated on a particular stratum of the population in a developed nation will not yield similar outcomes if implemented in underserved societies in a low-income country. Therefore, future studies should evaluate mHealth apps on a more diverse user across LMICs.
4.3. Gender Disparity and Sample Size
Sex and gender differences are often overlooked in research design. Our review identified a skewed representation of both. Unlike most other studies where female underrepresentation has been an issue [29], our review identified the underrepresentation of males. This oversight hinders the generalizability of research findings and their applicability to clinical practice. Future research must work to close gaps in equal sex and gender representation.
We also noted heterogeneity in the sample across all studies. Future studies should prepare bigger sample sizes to obtain generalizable outcomes and compensate for high dropout rates. A dropout rate in any research is the percentage of participants who do not complete the research task due to the study duration, lack of interest, technical difficulties, poor design, or insufficient compensation. As noted in our review, studies have faced a dropout rate of up to 50%. Dropout in research typically diminishes the validity of results, as completers may differ from people who drop out [30]. It may also result in a biased sample. Therefore, standardization must be made to inform the optimal sample size and diversity required to obtain feasible research validity.
4.4. Recommendations
Several actions could be taken to improve the acceptance and effectiveness of mHealth interventions among students:
Integrate mHealth interventions and not impose: To ensure the sustainability and effectiveness of mHealth interventions, it is essential to integrate them into the current lifestyle of students (study participants) and to work with them (and family) to ensure that interventions are aligned with their priorities and needs. It is also essential to consider human factors while designing the study and catering the comprehensive technology to meet students’ needs. Using the Test of Attentional and Interpersonal Style questionnaire [31], researchers should determine the information architecture to match user preference.
Ensure that mHealth interventions are culturally and linguistically appropriate: To ensure the adoption and effectiveness of mHealth interventions, it is essential to ensure that interventions are culturally and linguistically appropriate. Although international students are fluent in English, having multiple language choices built into the app would drastically change how they perceive the technology. However, studies should ensure that different languages retain common meanings and semantics.
Conduct ongoing evaluation and monitoring of mHealth interventions: It is essential to conduct ongoing evaluation and monitoring to identify and address any challenges or issues that may arise. This could involve using various evaluation and monitoring tools, such as surveys, focus groups, and data analysis.
Implement strong privacy and security measures: To ensure the privacy and confidentiality of personal and health information, it is essential to implement strong privacy and security measures for mHealth interventions [32]. This could involve implementing secure data storage and transmission systems and developing policies and procedures to protect personal and health information. More importantly, the student must be aware of the strengths of the security system.
4.5. Limitations
This study encompasses publications that matched our inclusion criteria. Therefore, the review is limited to relevant studies published in English between January 2017 and September 2022.
5. Conclusions
With the introduction and growing popularity of mHealth solutions, there has been a rise in the use of mobile apps to combat mental health problems. Our review shows mHealth’s potential to improve depressive symptoms and other similar mental health problems among college students. However, actions must be taken to improve barriers to communication and better reach the younger generations in healthcare. Besides, concerns such as digital divide, and unequal sex and gender representation, can hinder the growth, generalizability, effectiveness, and overall acceptance of mHealth for mental health.
Author Contributions
A.C. conceptualized the study, participated in the review process, and manuscript writing; A.K. participated in the review process and manuscript writing; H.S. participated in manuscript writing; Y.S. participated in manuscript writing and review. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Galderisi, S.; Heinz, A.; Kastrup, M.; Beezhold, J.; Sartorius, N. Toward a New Definition of Mental Health. World Psychiatry 2015, 14, 231–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. World Mental Health Report: Transforming Mental Health for All; WHO: Geneva, Switzerland, 2022; p. 296. [Google Scholar]
- Villarroel, M.A.; Terlizzi, E.P. Symptoms of Depression among Adults: United States, 2019. NCHS Data Brief 2020, 1–8. [Google Scholar]
- Pedrelli, P.; Nyer, M.; Yeung, A.; Zulauf, C.; Wilens, T. College Students: Mental Health Problems and Treatment Considerations. Acad. Psychiatry 2015, 39, 503–511. [Google Scholar] [CrossRef] [Green Version]
- Bruffaerts, R.; Mortier, P.; Kiekens, G.; Auerbach, R.P.; Cuijpers, P.; Demyttenaere, K.; Green, J.G.; Nock, M.K.; Kessler, R.C. Mental health problems in college freshmen: Prevalence and academic functioning. J. Affect. Disord. 2018, 225, 97–103. [Google Scholar] [CrossRef] [Green Version]
- Eisenberg, D.; Hunt, J.; Speer, N. Mental health in American colleges and universities: Variation across student subgroups and across campuses. J. Nerv. Ment. Dis. 2013, 201, 60–67. [Google Scholar] [CrossRef]
- Coombs, N.C.; Meriwether, W.E.; Caringi, J.; Newcomer, S.R. Barriers to healthcare access among U.S. adults with mental health challenges: A population-based study. SSM Popul. Health 2021, 15, 100847. [Google Scholar] [CrossRef] [PubMed]
- Ebert, D.D.; Mortier, P.; Kaehlke, F.; Bruffaerts, R.; Baumeister, H.; Auerbach, R.P.; Alonso, J.; Vilagut, G.; Martínez, K.I.; Lochner, C.; et al. Barriers of mental health treatment utilization among first-year college students: First cross-national results from the WHO World Mental Health International College Student Initiative. Int. J. Methods Psychiatr. Res. 2019, 28, e1782. [Google Scholar] [CrossRef] [Green Version]
- Chandrashekar, P. Do mental health mobile apps work: Evidence and recommendations for designing high-efficacy mental health mobile apps. Mhealth 2018, 4, 6. [Google Scholar] [CrossRef] [Green Version]
- Watt, A.; Cameron, A.; Sturm, L.; Lathlean, T.; Babidge, W.; Blamey, S.; Facey, K.; Hailey, D.; Norderhaug, I.; Maddern, G. Rapid versus full systematic reviews: Validity in clinical practice? ANZ J. Surg. 2008, 78, 1037–1040. [Google Scholar] [CrossRef]
- Harrer, M.; Apolinário-Hagen, J.; Fritsche, L.; Salewski, C.; Zarski, A.-C.; Lehr, D.; Baumeister, H.; Cuijpers, P.; Ebert, D.D. Effect of an internet- and app-based stress intervention compared to online psychoeducation in university students with depressive symptoms: Results of a randomized controlled trial. Internet Interv. 2021, 24, 100374. [Google Scholar] [CrossRef]
- Kleiman, E.M.; Bentley, K.H.; Wacha-Montes, A.; Taylor, M.E.; Lozy, O.; Conti, K.; Reese Mayer, W. A Pilot Implementation-Effectiveness Trial of a Single-Session Telehealth Workshop and Smartphone-Based Cognitive Behavioral Intervention for Managing Emotions Among College Students. Behav. Ther. 2022, 53, 1024–1036. [Google Scholar] [CrossRef] [PubMed]
- Bruehlman-Senecal, E.; Hook, C.J.; Pfeifer, J.H.; FitzGerald, C.; Davis, B.; Delucchi, K.L.; Haritatos, J.; Ramo, D.E. Smartphone App to Address Loneliness Among College Students: Pilot Randomized Controlled Trial. JMIR Ment. Health 2020, 7, e21496. [Google Scholar] [CrossRef] [PubMed]
- Haeger, J.A.; Davis, C.H.; Levin, M.E. Utilizing ACT daily as a self-guided app for clients waiting for services at a college counseling center: A pilot study. J. Am. Coll. Health 2022, 70, 742–749. [Google Scholar] [CrossRef] [PubMed]
- Huberty, J.; Green, J.; Glissmann, C.; Larkey, L.; Puzia, M.; Lee, C. Efficacy of the Mindfulness Meditation Mobile App “Calm” to Reduce Stress Among College Students: Randomized Controlled Trial. JMIR Mhealth Uhealth 2019, 7, e14273. [Google Scholar] [CrossRef] [Green Version]
- Lattie, E.; Cohen, K.A.; Winquist, N.; Mohr, D.C. Examining an App-Based Mental Health Self-Care Program, IntelliCare for College Students: Single-Arm Pilot Study. JMIR Ment. Health 2020, 7, e21075. [Google Scholar] [CrossRef]
- Levin, M.E.; Hicks, E.T.; Krafft, J. Pilot evaluation of the stop, breathe & think mindfulness app for student clients on a college counseling center waitlist. J. Am. Coll. Health 2022, 70, 165–173. [Google Scholar] [CrossRef] [Green Version]
- Bruhns, A.; Lüdtke, T.; Moritz, S.; Bücker, L. A Mobile-Based Intervention to Increase Self-esteem in Students with Depressive Symptoms: Randomized Controlled Trial. JMIR Mhealth Uhealth 2021, 9, e26498. [Google Scholar] [CrossRef]
- Schulte-Frankenfeld, P.M.; Trautwein, F.M. App-based mindfulness meditation reduces perceived stress and improves self-regulation in working university students: A randomised controlled trial. Appl. Psychol. Health Well Being 2022, 14, 1151–1171. [Google Scholar] [CrossRef]
- Harrer, M.; Adam, S.H.; Fleischmann, R.J.; Baumeister, H.; Auerbach, R.; Bruffaerts, R.; Cuijpers, P.; Kessler, R.C.; Berking, M.; Lehr, D.; et al. Effectiveness of an Internet- and App-Based Intervention for College Students with Elevated Stress: Randomized Controlled Trial. J. Med. Internet Res. 2018, 20, e136. [Google Scholar] [CrossRef] [Green Version]
- Lee, R.A.; Jung, M.E. Evaluation of an mHealth App (DeStressify) on University Students’ Mental Health: Pilot Trial. JMIR Ment. Health 2018, 5, e2. [Google Scholar] [CrossRef]
- Kajitani, K.; Higashijima, I.; Kaneko, K.; Matsushita, T.; Fukumori, H.; Kim, D. Short-term effect of a smartphone application on the mental health of university students: A pilot study using a user-centered design self-monitoring application for mental health. PLoS ONE 2020, 15, e0239592. [Google Scholar] [CrossRef] [PubMed]
- Clarke, J.; Draper, S. Intermittent mindfulness practice can be beneficial, and daily practice can be harmful. An in depth, mixed methods study of the “Calm” app’s (mostly positive) effects. Internet Interv. 2020, 19, 100293. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.; Park, J.Y.; Joung, D.; Jhung, K. Response Time as an Implicit Self-Schema Indicator for Depression among Undergraduate Students: Preliminary Findings From a Mobile App-Based Depression Assessment. JMIR Mhealth Uhealth 2019, 7, e14657. [Google Scholar] [CrossRef]
- Bendtsen, M.; Müssener, U.; Linderoth, C.; Thomas, K. A Mobile Health Intervention for Mental Health Promotion among University Students: Randomized Controlled Trial. JMIR Mhealth Uhealth 2020, 8, e17208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choudhury, A.; Choudhury, M. Mobile for Mothers mHealth Intervention to Augment Maternal Health Awareness and Behavior of Pregnant Women in Tribal Societies: Randomized Quasi-Controlled Study. JMIR Mhealth Uhealth 2022, 10, e38368. [Google Scholar] [CrossRef]
- Wallis, L.; Blessing, P.; Dalwai, M.; Shin, S.D. Integrating mHealth at point of care in low- and middle-income settings: The system perspective. Glob. Health Action 2017, 10, 1327686. [Google Scholar] [CrossRef] [Green Version]
- Cao, L.; Chongsuvivatwong, V.; McNeil, E.B. The Sociodemographic Digital Divide in Mobile Health App Use Among Clients at Outpatient Departments in Inner Mongolia, China: Cross-sectional Survey Study. JMIR Hum. Factors 2022, 9, e36962. [Google Scholar] [CrossRef]
- Källander, K.; Tibenderana, J.K.; Akpogheneta, O.J.; Strachan, D.L.; Hill, Z.; ten Asbroek, A.H.A.; Conteh, L.; Kirkwood, B.R.; Meek, S.R. Mobile Health (mHealth) Approaches and Lessons for Increased Performance and Retention of Community Health Workers in Low- and Middle-Income Countries: A Review. J. Med. Internet Res. 2013, 15, e17. [Google Scholar] [CrossRef]
- Bell, M.L.; Kenward, M.G.; Fairclough, D.L.; Horton, N.J. Differential dropout and bias in randomised controlled trials: When it matters and when it may not. BMJ 2013, 346, e8668. [Google Scholar] [CrossRef] [Green Version]
- Nideffer, R.M. Test of attentional and interpersonal style. J. Personal. Soc. Psychol. 1976, 34, 394. [Google Scholar] [CrossRef]
- Koh, J.; Tng, G.Y.Q.; Hartanto, A. Potential and Pitfalls of Mobile Mental Health Apps in Traditional Treatment: An Umbrella Review. J. Pers. Med. 2022, 12, 1376. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The rapid review selection process.


{kind=link}
Table 1.
Study and participant characteristics.
| Location | Intervention | Follow-Up | Participants at Baseline | Dropout Rate | Female | Minority Race |
|---|---|---|---|---|---|---|
| Weeks | Weeks | n | % | n (%) | % | |
| [15] USA | 8 | 4 | 88 | 0 | 79 (88) | 39 |
| [20] Multinational | 7 | 5 | 150 | 30 | 112 (75) | Na |
| [25] Sweden | 10 | 2 | 654 | 48 | 510 (78) | Na |
| [16] USA | 8 | None | 21 | 1 | 17 (81) | 28 |
| [21] Canada | 4 | 4 | 206 | 21 | 103 (63) | 21 |
| [18] Germany | 4 | None | 400 | 34 | 357 (89) | Na |
| [19] Germany | 8 | None | 99 | 35 | 67 (68) | Na |
| [22] Japan | 2 | None | 68 | 16 | 17 (30) | Na |
| [13] USA | 4 | 4 | 221 | 5 | 131 (59) | 47 |
| [11] Germany | 7 | 5 | 200 | 24 | 170 (85) | Na |
| [24] South Korea | 2 | None | 70 | 7 | 33 (51) | Na |
| [23] Scotland | 1 | 2 | 269 | 50 | 218 (81) | 16 |
| [17] USA | 4 | None | 23 | 30 | 16 (100) | 0 |
| [12] Unidentified | 8 | None | 222 | 20 | 138 (78) | 67 |
| [14] USA | 2 | 2 | 11 | 0 | 9 (82) | 9 |
Na: not available.
Table 2.
mHealth apps used by different studies.
| Name of the App | Access to the App | Methodology of the App | Intervention Delivery Approach | Frequency of App Use |
|---|---|---|---|---|
| [15] Calm | Public | Meditation, CBT | TGE | 10 min Daily |
| [20] StudiCare Stress | Participants | CBT and Mindfulness, Emotions, Acceptance | TGE, e-Coach (chatbot) | Two weekly modules |
| [25] mHealth PPMP | Participants | Positive Psychology | Text Messages, TGE | 10 min Daily |
| [16] IntelliCare for College Students | Participants | Cognitive Restructuring, Behavioral Activation | Mood Rating and Journal, Symptom Check, Lessons, and Resources | 1 Text daily |
| [21] DeStressify | Public | Mindfulness | TGE | 5 days/week) |
| [18] MCT & More | Public | CBT, Mindfulness, ACT, Metacognitive Training | TGE | 3–10 min daily |
| [19] Balloon | Public | MCT, Mindfulness, and Meditation | TGE | 10 min daily |
| [22] Mental App | Participants | Focus on Diagnosis Rather Than Treatment | Self-Monitoring, Self-Screening, and Referrals | Not defined |
| [13] Nod | Public | Positive Psychology, Mindfulness, CBT | Social Challenges, Reflections, and Written Testimonials | Not defined |
| [11] StudiCare | Participants | ERS | TGE | 1 weekly module |
| [24] K-CESD-R Mobile App | Participants | K-CESD-R Surveys | K-CESD-R Surveys | 1 session daily |
| [23] Calm | Public | Meditation, CBT | TGE | 10 min daily |
| [17] Stop, Breathe, and Think | Public | Meditation | TGE, Meditation and Emotional Check-Ins | 1 prompt daily |
| [12] MetricWire | Study | Mindfulness, Cognitive Flexibility, ERS | Therapeutic Workshop Skills | 4 prompts daily |
| [14] ACT Daily | Public | ACT | Coaching Sessions | 3 questionnaires daily |
ACT: Acceptance and Commitment Therapy; CBT: Cognitive Behavioral Therapy. TGE: Tradi-tional Guided Exercises; PPMP: Positive Psychology Multicomponent Program. ERS: Emotional Regulation Strategies.
Table 3.
Study outcomes.
| Mental Health Factors (Primary) | Other Factors Related to Mental Health (Secondary) | |||||||
|---|---|---|---|---|---|---|---|---|
| Study | Depression | Anxiety | Stress | Sleep Quality | Self-Image | Burnout | Quality of Life | General Health |
| [15] | Y * | Y * | Y * | |||||
| [20] | Y * | Y * | Y * | Y | Y * | Y * | ||
| [25] | Y * | Y * | Y * | |||||
| [16] | Y | Y | Y * | |||||
| [21] | Y | Y * | Y | Y | Y * | |||
| [18] | Y * | Y * | Y | |||||
| [19] | Y * | Y | ||||||
| [22] | Y | Y * | ||||||
| [13] | Y | Y | Y | |||||
| [11] | Y * | Y * | Y * | Y * | Y * | |||
| [24] | Y | Y | ||||||
| [23] | Y | |||||||
| [17] | Y | Y * | Y * | |||||
| [12] | Y * | Y * | ||||||
| [14] | Y * | Y * | Y * | |||||
* Significant improvement after mHealth intervention. Y: factors measured by different studies.
Table 4.
Validated scales used in different studies to evaluate various attributes of mental health.
Table 4.
Validated scales used in different studies to evaluate various attributes of mental health.
| Study | Validated Scales Used by Different Studies to Measure Different Mental Health Factor |
|---|---|
| Mental Health and Related Factor (Scales Used) | |
| [15] | Stress (PSS), Mindfulness (FFMQ), Self-Compassion (SCS-SF), Sleep Quality (PROMIS), Binge Drinking (YRBS), Physical Activity Participation (YRBS), Healthy Eating (YRBS) |
| [20] | Stress (PSS), Depression (CES-D), Anxiety (STAI), General Well-Being (WHO-5), Emotional Exhaustion (MBI-S), Dysfunctional Perfectionism (RAPS), Resilience (CD-RISC), Self-Compassion (SCS), Self-Esteem (RSES), Work Impairment (WIS), Academic Self-Efficacy (ASES), Academic Worrying (AWQ) |
| [25] | Mental Health and Well Being (MHC-SF), Depression (HADS), Anxiety (HADS) |
| [16] | Depression (PHQ), Anxiety (GAD), Anxiety Literacy (ALQ), Depression Literacy (DLQ), Knowledge and Beliefs About Services (KBSS), Cognitive and Behavioral Response to Stress (CB-RSS) |
| [21] | Stress (PSS), Anxiety (STAI), Depression (QIDS-SR), Sleep Quality (PSQI), Quality of Life (RAND-HS), Work Productivity (WPAI) |
| [18] | Depression (PHQ), Self-Esteem (RSES), Quality of Life (WHOQOL-BREF), Attitude Towards Psychological Online Interventions (APOI), Patient Therapy Expectation and Evaluation (PATHEV), Negative Effects of Psychotherapy (INEP) |
| [19] | Stress (PSS), Self-Regulation (SRS), Life Satisfaction and Happiness (QAH), Mindfulness (FMI), Emotional Regulation (ERQ), Social Desirability (SEA) |
| [22] | Public Stigma (LSS), Depression (CES-D), General Health (GHQ) |
| [13] | Loneliness (UCLA), Anxiety (GAD), Depression (PHQ), Social Anxiety (MSPI), Sleep Quality (PSQI), Perceived Social Support (CIT), Campus Belonging (SERUQ), Social Adjustment to College (SACQ), Intention to Return to College (NSSE) |
| [11] | Depression (CES-D), Behavioral Activation for Depression (BADS), Stress (PSS), Anxiety (STAD), Worrying (AWQ), Emotional Exhaustion (MBI-S), Work Impairment (WIS), Work Output (WOS), Work Cutback (PS-S), College Self-Efficacy (CSED), Resilience (CD-RISC), Emotion Regulation Competencies (SEK), Self-Compassion (SCS-D), Self-Esteem (RSES), Negative Beliefs About Stress (BASS), Positive Beliefs About Stress (BASS), Controllability Beliefs About Stress (BASS) |
| [24] | Depression (PHQ, CES-D, QIDS-SR, MADRS, HAM-D), Anxiety (HAM-A), Severity of Illness (CGI-S), Neuropsychiatric Interview (MINI) |
| [23] | Mindfulness (FFMQ), Generalized Self-Efficacy (GSE), Mental Well-Being (SWEMWBS) |
| [17] | Positive Mental Health (CCAPS, MHC-SF), Mindfulness (FFMQ), Values Progress (V.Q.) |
| [12] | Depression (EMA), Anxiety (EMA) |
| [14] | Depression (DASS), Anxiety (DASS), Stress (DASS), Psychological Inflexibility (AAQ), Cognitive Fusion (CFQ), Mindfulness (PHLMS), Valued Living (V.Q.), Emotional Self-Awareness (ESAS) |
AAQ: Acceptance and Action Questionnaire; ALQ: Anxiety Literacy Questionnaire; APOL: Attitude Towards Psychological Online Interventions; ASES: Academic Self-Efficacy Scale; AWO: Academic Worrying Questionnaire; BADS: Behavioral Activation for Depression Scale; BASS: Beliefs About Stress Scale; CB-RSS: Cognitive and Behavioral Response to Stress Scale; CCAPS: Counseling Center Assessment of Psychological Symptoms; CD-RISC: Connor-Davidson Resilience Scale Short Form; CES-D: Center for Epidemiological Studies’ Depression Scale; CPQ: Cognitive Fusion Questionnaire; CGI-S: Clinical Global Impressions Severity of Illness Scale; CIT: Comprehensive Inventory for Thriving; CSEI: College Self-Efficacy Inventory; DASS: Depression, Anxiety, and Stress Scale; DLQ: Depression Literacy Questionnaire; EMA-SI: Ecological Momentary Assessment Suicidal Ideation Questions; EMA: Ecological Momentary Assessment; ERQ: Emotion Regulation Questionnaire; ESAS: Emotional Self-Awareness Scale; FFMQ: Five Factor Mindfulness Questionnaire; FMI: Freiburg Mindfulness Inventory; GAD: Generalized Anxiety Disorder Scale; GHQ: General Health Questionnaire; GSE: Generalized Self Efficacy Scale; HADS: Hospital Anxiety Depression Scale; HAM-A: Hamilton Anxiety Rating Scale; HAM-D: Hamilton Depression Rating Scale; INEP: Inventory for Assessing Negative Effects of Psychotherapy; INQ: Interpersonal Needs Questionnaire; KBSS: Knowledge and Beliefs about Services Scale; LSS: Link Stigma Scale; MADRS; Montgomery-Asberg Depression Rating Scale; MBI-S: Maslach Burnout Inventory Student Version; MHC-SF: Mental Health Continuum Short Form; MINI: Mini-Intonational Neuropsychiatric Interview; MSPL: Mini Social Phobia Inventory; NSSE: National Survey for Student Engagement; PANAS: Positive and Negative Affect Schedule Scale; PATHEV: Patient Questionnaire on Therapy Expectation and Evaluation; PHLMS: Philadelphia Mindfulness Scale; PHQ: Patient Health Questionnaire; PIL: Purpose in Life Seale; PROMIS: Patient-Reported Outcomes Measurement Information System; PS-S: Presenteeism Scale for Students; PSQI: Pittsburg Sleep Quality Index; PSS: Perceived Stress Scale; QAH: Questionnaire for the Assessment of Happiness; QIDS-SR: Quick Inventory of Depressive Symptomatology Self-Report; RAND-HS: RAND Health Survey; RAPS: Revised Almost Perfect Scale; RSES: Rosenberg Self-Esteem Scale; SACQ: Student Adaptation to College Questionnaire; SCS-D: Self-Compassion Scale; SCS-SF: Self-Compassion Scale Short Form; SEA: Short Form Scale to Detect False Self-Representation; SEK: Assessment of Emotional Regulation Skills; SERUQ: Student Experiences in the Research University Questionnaire; SRS: Self-Regulation Scale; SWEMWBS: Short Warwick-Edinburgh Mental Well-Being Scale; UCLA: UCLA Loneliness Questionnaire; V.Q.: Valuing Questionnaire; WHO-5: WHO Well-Being Index; WHOQOL-BREF: World Health Organization Quality of Life Abbreviated Version; WIS: Work Impairment Scale; WOS: Work Output Scale; WPAL: Work Productivity and Activity Impairment Questionnaire; YRBS: Youth Risk Behavior Surveillance Survey.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Choudhury, A.; Kuehn, A.; Shamszare, H.; Shahsavar, Y. Analysis of Mobile App-Based Mental Health Solutions for College Students: A Rapid Review. Healthcare 2023, 11, 272. https://doi.org/10.3390/healthcare11020272
AMA Style
Choudhury A, Kuehn A, Shamszare H, Shahsavar Y. Analysis of Mobile App-Based Mental Health Solutions for College Students: A Rapid Review. Healthcare. 2023; 11(2):272. https://doi.org/10.3390/healthcare11020272
Chicago/Turabian StyleChoudhury, Avishek, Annabella Kuehn, Hamid Shamszare, and Yeganeh Shahsavar. 2023. "Analysis of Mobile App-Based Mental Health Solutions for College Students: A Rapid Review" Healthcare 11, no. 2: 272. https://doi.org/10.3390/healthcare11020272
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.