
Diving into Health: A Mixed Methods Study on the Impact of Scuba Diving in People with Physical Impairments
 , ,
, ,
Abstract
:1. Introduction
Research Questions and Hypotheses
2. Materials and Methods
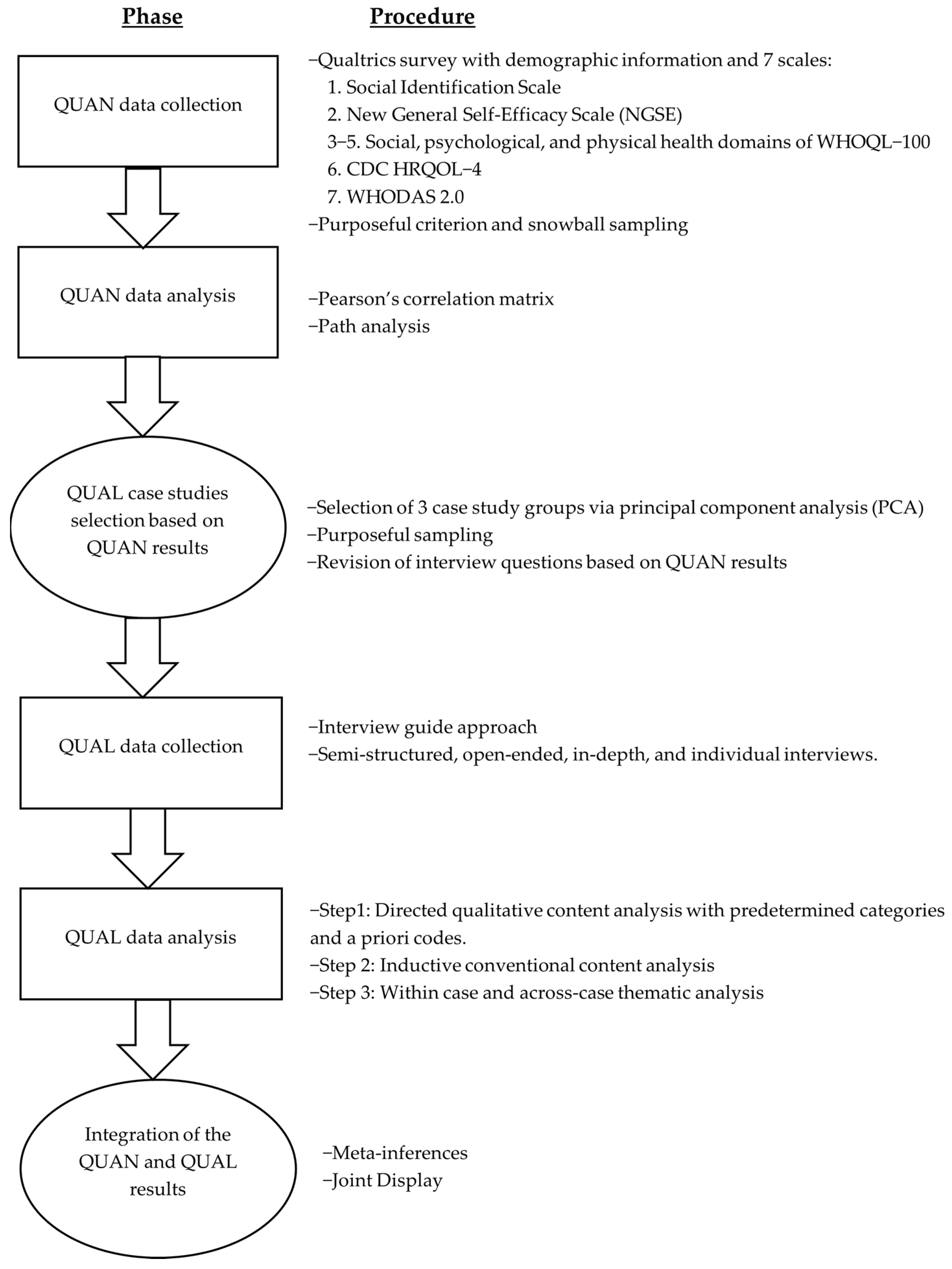
2.1. Design
2.2. Sampling and Recruitment
2.3. Phase One: Quantitative Phase
2.3.1. Quantitative Variables and Data Collection
2.3.2. Quantitative Data Analysis
2.4. Phase Two: Qualitative Phase
2.4.1. Qualitative Data Collection
2.4.2. Qualitative Data Analysis
2.5. Mixing of Quantitative and Qualitative Data
3. Results
3.1. Quantitative Results
3.1.1. Participants
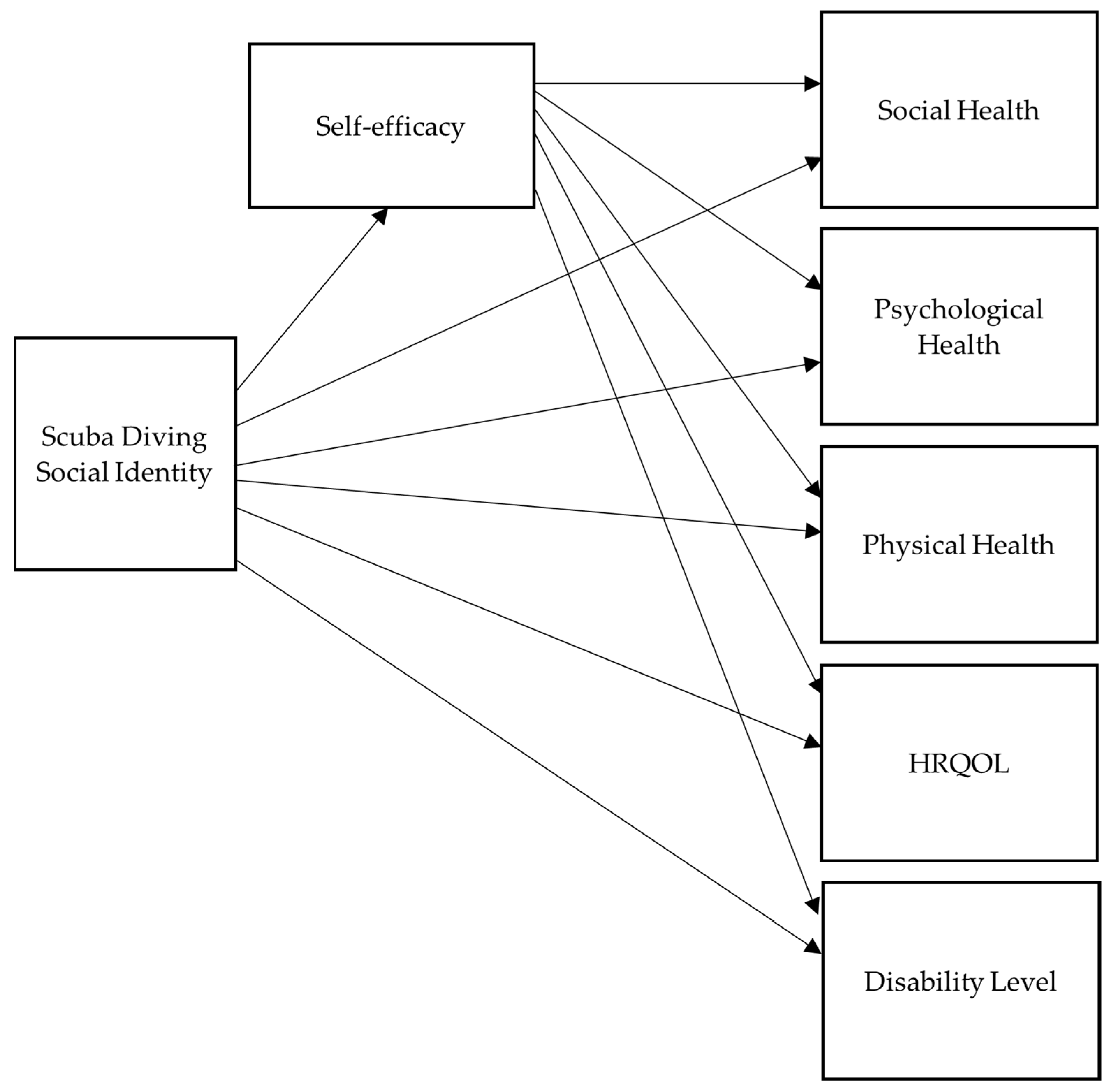
3.1.2. Test of Model
3.2. Qualitative Results
3.2.1. Participants
3.2.2. Qualitative Themes
In addition to a sense of belonging, the participants narrated that their scuba diving identity provides them with meaning and purpose. Robin shared “I think (scuba) it’s who I am, so it’s very extremely important…it’s given me a sense of purpose now.” To illustrate how scuba gives them purpose, Nat explained “It is an important part of my life…I’m advocating for other vets (veterans) to get out there…I want to not only be able to do more myself, but to bring up those others who can’t, and bring them along.Diving is a universal language, so even if you’re dealing with divers and there’s a language barrier, there’s still a common language that you share. And it ingratiates you with them, because you have shared experiences and it makes things easier, like we always identify as a group in some way.
Marion and Devin shared the following stories on how scuba diving has helped with relaxation, reducing their symptomatology of anxiety, depression, and PTSD:Self-esteem has improved because I’ve changed a lot from I can’t to I can. It actually made me love who I am as a person. For a long time I didn’t, because I can’t play basketball anymore, football out, frisbee, football is out, golf…I used to play softball…I was my kid’s soccer coach and trying to run after the ball and I’m eating it, so I mean, a lot of the world above the water is very negative for me. But then when I introduced the water, it made me very positive towards who I could be…because my activities in the water, now has made it to where I feel better about myself. It increased my self-esteem.
Honestly, I could say if I was not as active as a scuba diver, my depression and everything probably would have taken over, and just ruined my life….everybody’s always like…what does scuba diving do for you? and I’m like, well, it does a lot because a lot of people don’t understand when you’re underwater, the world just disappears, it’s a whole other world underwater, you don’t have all the busyness, you don’t have highway traffic, you don’t have the negative of the world. When you’re underwater, it’s freeing, it’s soothing…when I hear my bubbles while I’m diving and everything, it’s just calming.Devin
I’m able to take the stresses of everyday life, the military life, the PTSD, and scuba diving is a way to let that out, to let that release, to let that become a different person. Mentally, it saved my life. Scuba diving has, it is kind of emotional to put it in words for me, but it has been able to…pull me off the edge. When I’m in the water, nobody’s threatening me, I don’t have to worry about killing-attack, or the PTSD, becoming overwhelmed with the noises…it has been kind of like a saving grace for me…it’s a sense of safety for me, so mentally it has greatly improved my ability to deal with my disabilities.Marion
Addressing sleep, Robin shared “I have an extreme hard time sleeping, I’ve got to take medicine to try to sleep at night. And noticing after diving, I’ll feel a whole lot better, I’ll be able to sleep, I don’t have to take medicine.”Muscle spasms can be painful, and diving helps to release, relax the muscles and loosen the legs, so there’s not as many spasms and it’s not as painful. The pain and the spasticity in my legs and arms almost goes to zero under the water…And after I dive, I’m, you know, several hours of relief.
Alex shared how they felt more confident about earning more scuba certifications. Similarly, Terry described, “You build a lot of confidence in learning the skill and then executing the skill in a high stakes environment…I see myself as more confident individual because I’m able to do new things and take on new challenges.”(Scuba diving) It’s a challenge, and each time I can get in and do it, it helps me realize that you know, even though I’m injured, I can still get out and do these things, so it helps me say, you know, -hey, I’m doing good, I’m doing better; I can do this-. I may need a little help, but I can still do it…it probably has given me more confidence because, -hey I can do this-, and so I see myself as able to do more. And so, I can be more of an overcomer.
For me the quality life is what I’m looking for and scuba diving helps my quality of life, and like what we talked about, emotionally, physically, and then like I said, you have other aspects, like social jumps into it or recreational…it’s really neat that you can find something that has all of those. I used to be a wrestler and a boxer and it was all physical, I can’t do those as much anymore, but now, I can do something that helps my every day to day life trying to, and it may not help me all the time…when I’m not diving, but it will help me when I’m diving, and it may not help me physically when I’m not diving but it helps me emotionally or socially.
3.3. Mixed Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jesus, T.S.; Landry, M.D.; Hoenig, H. Global Need for Physical Rehabilitation: Systematic Analysis from the Global Burden of Disease Study 2017. Int. J. Environ. Res. Public Health 2019, 16, 980. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reichard, A.; Stolzle, H.; Fox, M.H. Health disparities among adults with physical disabilities or cognitive limitations compared to individuals with no disabilities in the United States. Disabil. Health J. 2011, 4, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Krahn, G.L.; Walker, D.K.; Correa-De-Araujo, R. Persons with Disabilities as an Unrecognized Health Disparity Population. Am. J. Public Health 2015, 105, S198–S206. [Google Scholar] [CrossRef] [PubMed]
- Zack, M. Health-Related Quality of Life-United States, 2006 and 2010. MMWR Surveill. Summ. 2013, 62, 105–111. Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/su6203a18.htm (accessed on 19 September 2022).
- Keramat, S.A.; Ahammed, B.; Mohammed, A.; Seidu, A.-A.; Farjana, F.; Hashmi, R.; Ahmad, K.; Haque, R.; Ahmed, S.; Ali, M.A.; et al. Disability, physical activity, and health-related quality of life in Australian adults: An investigation using 19 waves of a longitudinal cohort. PLoS ONE 2022, 17, e0268304. [Google Scholar] [CrossRef]
- Krops, L.A.; Jaarsma, E.A.; Dijkstra, P.U.; Geertzen, J.H.B.; Dekker, R. Health Related Quality of Life in a Dutch Rehabilitation Population: Reference Values and the Effect of Physical Activity. PLoS ONE 2017, 12, e0169169. [Google Scholar] [CrossRef] [Green Version]
- Lima-Castro, S.; Blanco, V.; Otero, P.; López, L.; Vázquez, F.L. Health-related quality of life among persons with physical disabilities: A systematic review and meta-analysis. Rev. Iberoam. Psicol. Salud 2020, 11, 82. [Google Scholar] [CrossRef]
- Jetten, J.; Haslam, S.A.; Cruwys, T.; Greenaway, K.H.; Haslam, C.; Steffens, N.K. Advancing the social identity approach to health and well-being: Progressing the social cure research agenda. Eur. J. Soc. Psychol. 2017, 47, 789–802. [Google Scholar] [CrossRef]
- Haslam, C.; Jetten, J.; Cruwys, T.; Dingle, G.A.; Haslam, S.A. The New Psychology of Health: Unlocking the Social Cure; Routledge: London, UK, 2018. [Google Scholar] [CrossRef]
- Haslam, S.A.; Jetten, J.; Postmes, T.; Haslam, C. Social Identity, Health and Well-Being: An Emerging Agenda for Applied Psychology. Appl. Psychol. 2009, 58, 1–23. [Google Scholar] [CrossRef]
- Engell, G.L. The need for a new medical model: A challenge for biomedicine. Sci. New Ser. 1977, 196, 129–136. [Google Scholar] [CrossRef]
- Haslam, S.A.; Haslam, C.; Jetten, J.; Cruwys, T.; Bentley, S. Group life shapes the psychology and biology of health: The case for a sociopsychobio model. Soc. Pers. Psychol. Compass 2019, 13, e12490. [Google Scholar] [CrossRef]
- Muldoon, O.T.; Walsh, R.S.; Curtain, M.; Crawley, L.; Kinsella, E.L. Social cure and social curse: Social identity resources and adjustment to acquired brain injury. Eur. J. Soc. Psychol. 2019, 49, 1272–1282. [Google Scholar] [CrossRef] [Green Version]
- Mertens, N.; Boen, F.; Steffens, N.K.; Haslam, S.A.; Bruner, M.; Barker, J.B.; Slater, M.J.; Fransen, K. Harnessing the power of ‘us’: A randomized wait-list controlled trial of the 5R shared leadership development program (5RS) in basketball teams. Psychol. Sport Exerc. 2021, 54, 101936. [Google Scholar] [CrossRef]
- Kinsella, E.L.; Muldoon, O.T.; Fortune, D.G.; Haslam, C. Collective influences on individual functioning: Multiple group memberships, self-regulation, and depression after acquired brain injury. Neuropsychol. Rehabil. 2018, 30, 1059–1073. [Google Scholar] [CrossRef]
- Tajfel, H.; Turner, J.C. An integrative theory of inergroup conflict. In The Social Psychology of Intergroup Relations; Austin, W.G., Worchel, S., Eds.; Brooks/Cole: Monterey, CA, USA, 1979; pp. 33–47. [Google Scholar]
- Willer, D.; Turner, J.C.; Hogg, M.A.; Oakes, P.J.; Reicher, S.D.; Wetherell, M.S. Rediscovering the Social Group: A Self-Categorization Theory; Blackwell: Hoboken, NJ, USA, 1987. [Google Scholar]
- Walker, G.J.; Kleiber, D.A.; Mannell, R.C. A Social Psychology of Leisure, 3rd ed.; Sagamore Venture: Champaign, IL, USA, 2019. [Google Scholar]
- Kleiber, D. Leisure Experience and Human Development: A Dialectical Interpretation (Lives in Context); Basic Books: New York, NY, USA, 1999. [Google Scholar]
- Kelly, J.R. Leisure Identities and Interactions; George Allen & Unwin Ltd.: Crows Nest, Australia, 1983. [Google Scholar]
- Naumann, K.; Kernot, J.; Parfitt, G.; Gower, B.; Winsor, A.; Davison, K. What are the effects of scuba diving-based interventions for clients with neurological disability, autism or intellectual disability? A systematic review. Diving Hyperb. Med. J. 2021, 51, 355–360. [Google Scholar] [CrossRef]
- Henrykowska, G.; Soin, J.; Siermontowski, P. Scuba Diving as a Form of Rehabilitation for People with Physical Disabilities. Int. J. Environ. Res. Public Health 2021, 18, 5678. [Google Scholar] [CrossRef] [PubMed]
- Aganovic, Z. Effects of scuba diving programmed classes on Bosnian war veterans with amputations. Int. J. Sport Exerc. Train. Sci. 2019, 5, 6–14. [Google Scholar] [CrossRef] [Green Version]
- Williamson, J.A.; McDonald, F.W.; Galligan, E.A.; Baker, P.G. Selection and training of disabled persons for scuba-diving: Medical and psychological aspects. Med. J. Aust. 1984, 141, 414–418. [Google Scholar] [CrossRef]
- Haydn, T.; Brenneis, C.; Schmutzhard, J.; Gerstenbrand, F.; Saltuan, L.; Schmutzhard, E. Scuba diving—A therapeutic option for patients with paraplegia. Neuropsychiatrie 2007, 21, 226–229. [Google Scholar]
- Novak, H.F.; Ladurner, G. Scuba diving as a rehabilitation approach in paraplegia. Rehabilitation 1999, 38, 181–184. [Google Scholar]
- Blumhorst, E.; Kono, S.; Cave, J. An Exploratory Study of Adaptive Scuba Diving’s Effects on Psychological Well-Being among Military Veterans. Ther. Recreat. J. 2020, 54, 173–189. [Google Scholar] [CrossRef]
- Morgan, A.; Sinclair, H.; Tan, A.; Thomas, E.; Castle, R. Can scuba diving offer therapeutic benefit to military veterans experiencing physical and psychological injuries as a result of combat? A service evaluation of Deptherapy UK. Disabil. Rehabil. 2019, 41, 2832–2840. [Google Scholar] [CrossRef] [PubMed]
- Beneton, F.; Michoud, G.; Coulange, M.; Laine, N.; Ramdani, C.; Borgnetta, M.; Breton, P.; Guieu, R.; Rostain, J.C.; Trousselard, M. Recreational Diving Practice for Stress Management: An Exploratory Trial. Front. Psychol. 2017, 8, 2193. [Google Scholar] [CrossRef] [Green Version]
- Cracknell, D.; White, M.P.; Pahl, S.; Nichols, W.J.; Depledge, M.H. Marine Biota and Psychological Well-Being: A preliminary examination of dose–response effects in an aquarium setting. Environ. Behav. 2016, 48, 1242–1269. [Google Scholar] [CrossRef] [PubMed]
- Graczyk, D. Diving and autonomic cardiovascular system regulation in persons with paraplegia. Med. Rehabil. 2010, 14, 17–21. [Google Scholar]
- Carin-Levy, G.; Jones, D. Psychosocial aspects of scuba diving for people with physical disabilities: An occupational science perspective. Can. J. Occup. Ther. 2007, 74, 6–14. [Google Scholar] [CrossRef]
- Madorsky, J.G.; Madorsky, A.G. Scuba diving: Taking the wheelchair out of wheelchair sports. Arch. Phys. Med. Rehabil. 1988, 69, 215–218. [Google Scholar]
- Boyd, L.A. Scuba provides expression. J. Rehabil. 1972, 38, 21. [Google Scholar]
- Dimmock, K. Finding comfort in adventure: Experiences of recreational SCUBA divers. Leis. Stud. 2009, 28, 279–295. [Google Scholar] [CrossRef]
- Creswell, J.W.; Plano Clark, V.L. Designing and Conducting Mixed Methods Research, 3rd ed.; SAGE: London, UK, 2018. [Google Scholar]
- Chmiliar, L. Multiple-Case Designs. In Encyclopedia of Case Study Research; Mills, A.J., Durepos, G., Wiebe, E., Eds.; SAGE: London, UK, 2010; pp. 582–584. [Google Scholar] [CrossRef]
- Teddlie, C.; Yu, F. Mixed methods sampling: A typology journal of mixed methods research. J. Mix. Methods Res. 2007, 1, 77–100. [Google Scholar] [CrossRef]
- Collins, K.M.T. Advanced Sampling Designs in Mixed Research: Current Practices and Emerging Trends in the Social and Behavioral Sciences. In SAGE Handbook of Mixed Methods in Social & Behavioral Research; Tashakkori, A., Teddlie, C., Eds.; SAGE Publications, Inc.: Thousands Oaks, CA, USA, 2015; pp. 353–378. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdi, H.; Williams, L.J. Principal component analysis. Wiley Interdiscip. Rev. Comput. Stat. 2010, 2, 433–459. [Google Scholar] [CrossRef]
- Qualtrics2020. Available online: https://www.qualtrics.com (accessed on 17 January 2021).
- Doosje, B.; Ellemers, N.; Spears, R. Perceived Intragroup Variability as a Function of Group Status and Identification. J. Exp. Soc. Psychol. 1995, 31, 410–436. [Google Scholar] [CrossRef]
- Chen, G.; Gully, S.M.; Eden, D. Validation of a New General Self-Efficacy Scale. Organ. Res. Methods 2001, 4, 62–83. [Google Scholar] [CrossRef] [Green Version]
- The World Health Organization Quality of Life Group. The World Health Organization quality of life assessment (WHOQOL): Development and general psychometric properties. Soc. Sci. Med. 1998, 46, 1569–1585. [Google Scholar] [CrossRef]
- World Health Organization. WHOQOL Manual. 2012. Available online: https://www.who.int/tools/whoqol (accessed on 26 June 2021).
- CDC. HRQOL Methods and Measures. 2018. Available online: https://www.cdc.gov/hrqol/methods.htm (accessed on 26 June 2021).
- CDC. Healthy Days Core Module (CDC HRQOL-4). 2018. Available online: https://www.cdc.gov/hrqol/hrqol14_measure.htm (accessed on 26 June 2021).
- R Core Team. A Language and Environment for Statistical Computing. 2021. Available online: https://www.r-project.org/ (accessed on 24 May 2021).
- Rosseel, Y. lavaan: AnRPackage for Structural Equation Modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef] [Green Version]
- Zoom Video Communications, Inc. Zoom. 2022. Available online: https://zoom.us/ (accessed on 20 October 2022).
- Turner, D.W. Qualitative Interview Design: A Practical Guide for Novice Investigators. Qual. Rep. 2010, 15, 754–760. [Google Scholar] [CrossRef]
- Hsieh, H.-F.; Shannon, S.E. Three Approaches to Qualitative Content Analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- Paterson, B. Within-case analysis. In Encyclopedia of Case Study Research; Mills, A., Durepos, G., Wiebe, E., Eds.; SAGE: Thousands Oaks, CA, USA, 2012; pp. 761–764. [Google Scholar] [CrossRef]
- Burns, J.M.C. Cross-case synthesis and analysis. In Encyclopedia of Case Study Research; Mills, A., Durepos, G., Wiebe, E., Eds.; SAGE: Thousands Oaks, CA, USA, 2012; pp. 265–267. [Google Scholar] [CrossRef]
- Creswell, J.W.; Poth, C.N. Qualitiative Inquiry & Research Design: Choosing among Five Approaches, 4th ed.; SAGE: Thousands Oaks, CA, USA, 2018. [Google Scholar]
- Creswell, J.W.; Creswell, J.D. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches, 5th ed.; SAGE: Thousands Oaks, CA, USA, 2018. [Google Scholar]
- Häusser, J.A.; Junker, N.M.; van Dick, R. The how and the when of the social cure: A conceptual model of group- and individual-level mechanisms linking social identity to health and well-being. Eur. J. Soc. Psychol. 2020, 50, 721–732. [Google Scholar] [CrossRef]
- Steffens, N.K.; La Rue, C.J.; Haslam, C.; Walter, Z.C.; Cruwys, T.; Munt, K.A.; Haslam, S.A.; Jetten, J.; Tarrant, M. Social identification-building interventions to improve health: A systematic review and meta-analysis. Health Psychol. Rev. 2021, 15, 85–112. [Google Scholar] [CrossRef]
- Muldoon, O.T.; Haslam, S.A.; Haslam, C.; Cruwys, T.; Kearns, M.; Jetten, J. The social psychology of responses to trauma: Social identity pathways associated with divergent traumatic responses. Eur. Rev. Soc. Psychol. 2019, 30, 311–348. [Google Scholar] [CrossRef] [Green Version]
- Cheng, J.; Diamond, M. SCUBA Diving for Individuals with Disabilities. Am. J. Phys. Med. Rehabil. 2005, 84, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Walker, P.A.; Kampman, H. “It didn’t bring back the old me but helped me on the path to the new me”: Exploring posttraumatic growth in British veterans with PTSD. Disabil. Rehabil. 2021, 44, 7455–7463. [Google Scholar] [CrossRef] [PubMed]
- Henrykowska, G.; Soin, J.; Pleskacz, K.; Siermontowski, P. Influence of Scuba Diving on the Quality of Life of People with Physical Disabilities. Healthcare 2022, 10, 761. [Google Scholar] [CrossRef] [PubMed]
- Cameron, J.E.; Voth, J.; Jaglal, S.B.; Guilcher, S.J.T.; Hawker, G.; Salbach, N.M. “In this together”: Social identification predicts health outcomes (via self-efficacy) in a chronic disease self-management program. Soc. Sci. Med. 2018, 208, 172–179. [Google Scholar] [CrossRef] [PubMed]
- Benyon, K.; Hill, S.; Zadurian, N.; Mallen, C. Coping strategies and self-efficacy as predictors of outcome in osteoarthritis: A systematic review. Musculoskelet. Care 2010, 8, 224–236. [Google Scholar] [CrossRef]
- Jones, F.; Riazi, A. Self-efficacy and self-management after stroke: A systematic review. Disabil. Rehabil. 2011, 33, 797–810. [Google Scholar] [CrossRef]
- Mortenson, W.; Noreau, L.; Miller, W. The relationship between and predictors of quality of life after spinal cord injury at 3 and 15 months after discharge. Spinal Cord 2010, 48, 73–79. [Google Scholar] [CrossRef]
- Wilski, M.; Tasiemski, T. Illness perception, treatment beliefs, self-esteem, and self-efficacy as correlates of self-management in multiple sclerosis. Acta Neurol. Scand. 2016, 133, 338–345. [Google Scholar] [CrossRef]
- Van Diemen, T.; Crul, T.; van Nes, I.; Geertzen, J.H.; Post, M.W. Associations Between Self-Efficacy and Secondary Health Conditions in People Living With Spinal Cord Injury: A Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2017, 98, 2566–2577. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Calderon, J.; Meeus, M.; Struyf, F.; Luque-Suarez, A. The role of self-efficacy in pain intensity, function, psychological factors, health behaviors, and quality of life in people with rheumatoid arthritis: A systematic review. Physiother. Theory Pract. 2018, 36, 21–37. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Predetermined Category | A Priori Codes |
|---|---|
| Scuba diving social identity | Sense of belonging |
| Positive distinctiveness | |
| Emotional significance | |
| Social health | Personal relationships |
| Social support | |
| Sexual activity | |
| Psychological health | Bodily image and appearance |
| Positive vs. negative feelings | |
| Self-esteem | |
| Thinking, learning, memory, and concentration | |
| Physical health | Energy and fatigue |
| Pain and discomfort | |
| Sleep and rest |
| Characteristic | N | (%) |
|---|---|---|
| Impairment Category | ||
| Spinal Cord Injury | 20 | 25.6% |
| Acquired/Traumatic Brain Injury | 12 | 15.4% |
| Amputation or Limb Loss | 6 | 7.7% |
| Degenerative Disc Disease | 5 | 6.4% |
| Arthritis | 4 | 5.1% |
| Chronic Back Pain | 4 | 5.1% |
| Multiple Sclerosis | 4 | 5.1% |
| Fibromyalgia | 3 | 3.8% |
| Joint Reconstruction or Replacement | 3 | 3.8% |
| Sensory Impairment | 3 | 3.8% |
| Muscular Dystrophy | 2 | 2.6% |
| Spinal Stenosis | 2 | 2.6% |
| Amyotrophic Lateral Sclerosis | 1 | 1.28% |
| Cerebral Palsy | 1 | 1.28% |
| Clonus | 1 | 1.28% |
| De Quervain’s Syndrome | 1 | 1.28% |
| Lupus | 1 | 1.28% |
| Neuro-Sweet Disease | 1 | 1.28% |
| Poliomyelitis | 1 | 1.28% |
| Polymyositis | 1 | 1.28% |
| Scoliosis | 1 | 1.28% |
| Transverse Myelitis | 1 | 1.28% |
| Impairment Onset | ||
| As an adult (19+) | 63 | 80.8% |
| Before age 18 | 11 | 5.1% |
| Congenital | 4 | 14.1% |
| Gender | ||
| Male | 54 | 69.2% |
| Female | 24 | 30.8% |
| Non-binary/Third Gender | 0 | 0.0% |
| Race/Ethnicity | ||
| White | 63 | 80.8% |
| Hispanic or Latinx | 6 | 7.7% |
| Multiracial | 4 | 5.1% |
| Black or African American | 4 | 5.1% |
| American Indian or Alaskan Native | 1 | 1.3% |
| Age | ||
| 20–29 | 1 | 1.3% |
| 30–39 | 14 | 17.9% |
| 40–49 | 25 | 32.0% |
| 50–59 | 26 | 33.3% |
| 60–69 | 11 | 14.1% |
| 70–79 | 1 | 1.3% |
| Length of Scuba Diving Group Membership | ||
| <1 year | 4 | 5.1% |
| 1–3 years | 17 | 21.8% |
| 4–6 years | 19 | 24.3% |
| 7–9 years | 10 | 12.9% |
| 10+ years | 28 | 35.9% |
| Diving Level | ||
| Beginner | 13 | 16.7% |
| Intermediate | 24 | 30.7% |
| Advanced | 24 | 30.7% |
| Expert | 17 | 21.8% |
| Logged Dives per Year | ||
| 1–5 | 19 | 24.3% |
| 6–10 | 9 | 11.5% |
| 11–15 | 10 | 12.8% |
| 16–20 | 11 | 14.1% |
| 21–25 | 2 | 2.5% |
| 26–30 | 6 | 7.7% |
| >30 | 20 | 25.6% |
| NA | 1 | 1.3% |
| Variable | Mean | Median | SD |
|---|---|---|---|
| Scuba diving social identity | 6.07 | 7.00 | 1.41 |
| Self-efficacy | 3.98 | 4.00 | 0.72 |
| Social health | 59.74 | 58.33 | 19.98 |
| Psychological health | 64.51 | 63.75 | 18.46 |
| Physical health | 53.90 | 52.08 | 21.41 |
| HRQOL | 2.81 | 4.00 | 1.45 |
| Disability level | 13.84 | 12.00 | 8.85 |
| Path | z-Value | p |
|---|---|---|
| Scuba social identity to self-efficacy | 0.303 | 0.762 |
| Scuba social identity to social health | −1.032 | 0.302 |
| Scuba social identity to psychological health | −0.738 | 0.461 |
| Scuba social identity to physical health | −0.514 | 0.607 |
| Scuba social identity to HRQOL | −0.406 | 0.685 |
| Scuba social identity to disability level | −0.214 | 0.830 |
| Self-efficacy to social health | 4.790 | <0.001 |
| Self-efficacy to psychological health | 8.648 | <0.001 |
| Self-efficacy to physical health | 4.853 | <0.001 |
| Self-efficacy to HRQOL | 5.586 | <0.001 |
| Self-efficacy to disability level | −7.186 | <0.001 |
| Self-Efficacy | Scuba Diving Social Identity | |||
|---|---|---|---|---|
| r | p | r | p | |
| Social Health | 0.50 | <0.001 | −0.12 | 0.2171 |
| Psychological health | 0.70 | <0.001 | −0.07 | 0.5089 |
| Physical health | 0.45 | <0.001 | −0.04 | 0.7055 |
| HRQOL | 0.54 | <0.001 | −0.03 | 0.8132 |
| Disability level | −0.60 | <0.001 | −0.09 | 0.3739 |
| Self-efficacy | −0.01 | 0.8939 | ||
| Characteristic | n | (%) |
|---|---|---|
| Impairment Category | ||
| Spinal Cord Injury | 5 | 33.3% |
| Acquired/Traumatic Brain Injury | 3 | 20.0% |
| Chronic Back Pain | 2 | 13.3% |
| Arthritis | 1 | 6.7% |
| Fibromyalgia | 1 | 6.7% |
| Joint Reconstruction or Replacement | 1 | 6.7% |
| Muscular Dystrophy | 1 | 6.7% |
| Polymyositis | 1 | 6.7% |
| Impairment Onset | ||
| As an adult (age 19+) | 13 | 86.6% |
| Before age 18 | 1 | 6.7% |
| Congenital | 1 | 6.7% |
| Gender | ||
| Male | 12 | 80% |
| Female | 3 | 20% |
| Non-binary/Third Gender | 0 | 0.0% |
| Race/Ethnicity | ||
| White | 10 | 66.6% |
| Hispanic or Latinx | 2 | 13.3% |
| Multiracial | 2 | 13.3% |
| Black or African American | 1 | 6.7% |
| Age | ||
| 20–29 | 1 | 6.7% |
| 30–39 | 2 | 13.3% |
| 40–49 | 6 | 40.0% |
| 50–59 | 5 | 33.3% |
| 60–69 | 1 | 6.7% |
| Length of Scuba Diving Group Membership | ||
| <1 year | 1 | 6.7% |
| 1–3 years | 2 | 13.3% |
| 4–6 years | 3 | 20.0% |
| 7–9 years | 4 | 26.7% |
| 10+ years | 5 | 33.3% |
| Diving Level | ||
| Beginner | 1 | 6.7% |
| Intermediate | 7 | 46.6% |
| Advanced | 3 | 20.0% |
| Expert | 4 | 26.7% |
| Logged Dives per Year | ||
| 1–5 | 4 | 26.7% |
| 6–10 | 4 | 26.7% |
| 11–15 | 0 | 0.0% |
| 16–20 | 1 | 6.7% |
| 21–25 | 1 | 6.7% |
| 26–30 | 2 | 13.3% |
| >30 | 3 | 20.0% |
| Themes | *Freq. | Categories | *Freq. | Codes | *Freq. |
|---|---|---|---|---|---|
| Theme 1: Being a scuba diver is a positive social identity that provides me with a sense of belonging, meaning, and purpose. | 15 | Scuba diving social identity | 15 | Deductive | |
| Sense of belonging | 14 | ||||
| Positive distinctiveness | 11 | ||||
| Emotional significance | 14 | ||||
| Inductive | |||||
| Meaningful identity | 14 | ||||
| Purposeful identity | 14 | ||||
| Positive identity | 15 | ||||
| Theme 2: Scuba diving has contributed positively to my social health through enhanced social relationships and a community that provides me with social support. | 15 | Social health | 15 | Deductive | |
| Personal relationships | 14 | ||||
| Social support | 13 | ||||
| Sexual activity | 0 | ||||
| Inductive | |||||
| Community | 14 | ||||
| Theme 3: Scuba diving has contributed positively to my psychological health by enhancing self-esteem, positive feelings, and relaxation; and reducing symptoms of depression, anxiety, and/or post-traumatic stress disorder (PTSD). | 15 | Psychological health | 15 | Deductive | |
| Bodily image & appearance | 6 | ||||
| Positive feelings | 15 | ||||
| Self-esteem | 13 | ||||
| Thinking, learning, memory, and concentration | 7 | ||||
| Inductive | |||||
| Relaxation | 14 | ||||
| Anxiety and depression | 11 | ||||
| PTSD | 8 | ||||
| Theme 4: Scuba diving has contributed positively to my physical health by offering physical activity/exercise, better mobility, relief from physical pain, and better sleep | 15 | Physical health | 15 | Deductive | |
| Energy and fatigue | 14 | ||||
| Pain and discomfort | 12 | ||||
| Sleep and rest | 11 | ||||
| Inductive | |||||
| Physical activity/exercise | 14 | ||||
| Improved mobility | 11 | ||||
| Theme 5: Scuba diving has contributed positively to my self-efficacy by boosting my self-confidence. | 14 | Self-efficacy | 14 | Inductive | |
| Self-confidence | 13 | ||||
| Accomplishments & goals | 8 | ||||
| Theme 6: Scuba diving has contributed positively to the quality of my life. | 14 | Health-related quality of life | 12 | Inductive | |
| Positive influence on different life domains. | 14 |
| Dimension | QUAN Results | QUAL Results | Mixed-Methods Comparison |
|---|---|---|---|
| Influence of scuba diving social identity on self-efficacy | Scuba diving social identity does not influence self-efficacy (r = −0.01, p = 0.8939, β = 0.01, p = 0.762) | Themes 1 & 5 Scuba diving social identity influences self-efficacy | Discrepancy between quantitative and qualitative results |
| Influence of scuba diving social identity on social health | Scuba diving social identity does not influence social health (r = −0.12, p = 0.2171, β = −1.54, p = 0.302) | Themes 1 & 2 Scuba diving social identity influences social health | Discrepancy between quantitative and qualitative results |
| Influence of scuba diving social identity on psychological health | Scuba diving social identity does not influence psychological health (r = −0.07, p = 0.5089, β = −0.80, p = 0.461) | Themes 1 & 3 Scuba diving social identity influences psychological health | Discrepancy between quantitative and qualitative results |
| Influence of scuba diving social identity on physical health | Scuba diving social identity does not influence physical health (r = −0.04, p = 0.7055, β = −0.78, p = 0.607) | Themes 1 & 4 Scuba diving social identity influences physical health | Discrepancy between quantitative and qualitative results |
| Influence of scuba diving social identity on HRQOL | Scuba diving social identity does not influence HRQOL (r = −0.03, p = 0.8132, β = −0.04, p = 0.685) | Themes 1 & 6 Scuba diving social identity influences HRQOL | Discrepancy between quantitative and qualitative results |
| Influence of scuba diving social identity on disability level | Scuba diving social identity does not influence disability level (r = −0.09, p = 0.3729, β = −0.12, p = 0.830) | Themes 1, 2, 3, 4 Scuba diving social identity influences disability level | Discrepancy between quantitative and qualitative results |
| Quantitative Findings | Qualitative Findings | Meta-Inferences |
|---|---|---|
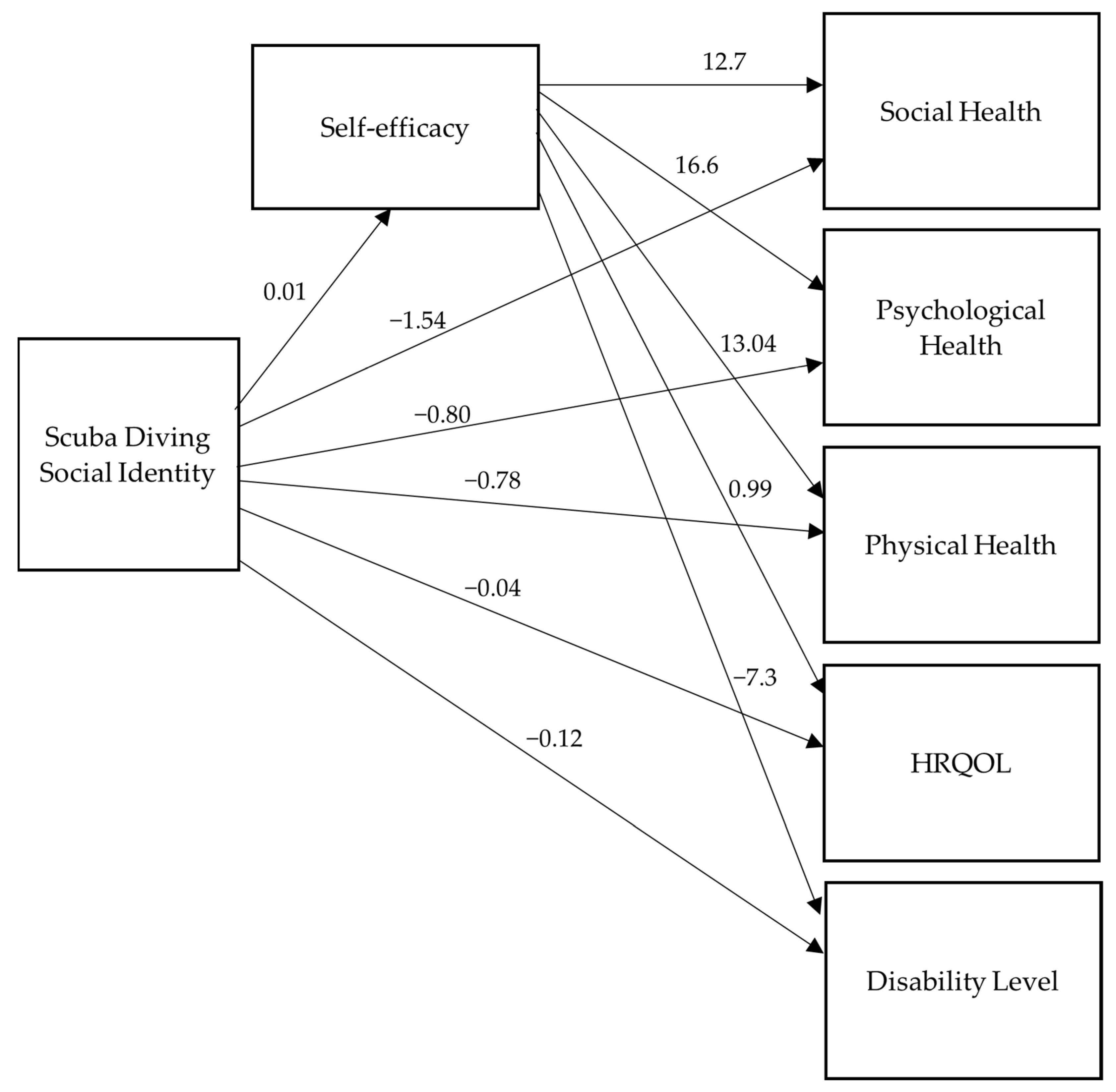
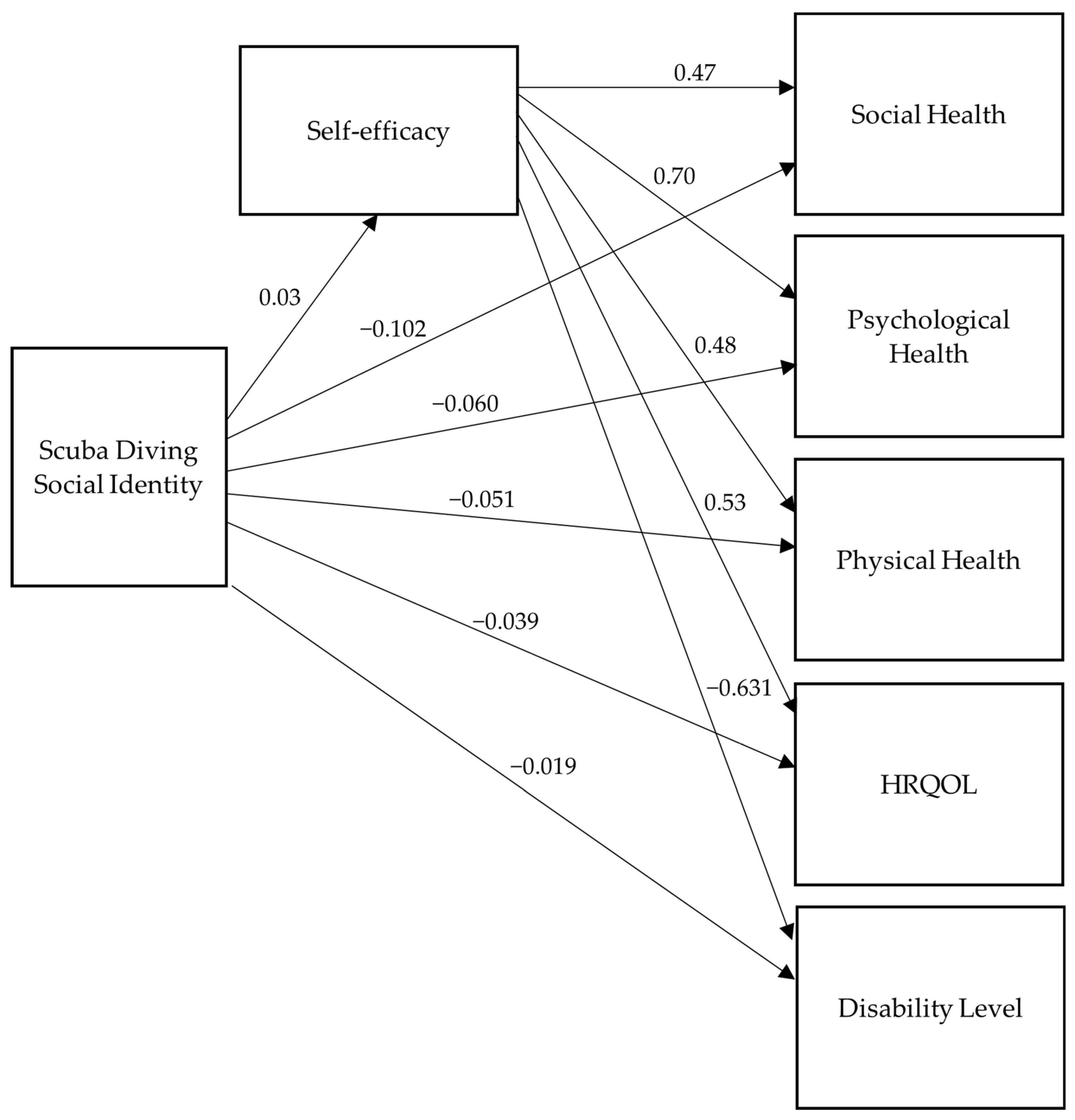
| Pearson’s correlation coefficients from the sample did not show any correlations between scuba diving social identity and social health (r = −0.12, p = 0.2171), psychological health (−0.07, p = 0.5089), physical health (r = −0.04, p = 0.7055), HRQOL (r = −0.03, p = −0.8132), disability level (r = −0.09, p = 0.3729), or self-efficacy (−0.01, p = 0.8939) The path analysis from the sample did not show scuba diving social identity as a predictor of social health (β= −1.54, p = 0.302), psychological health (β= −0.80, p = 0.461), physical health (β = −0.78, p = 0.607), HRQOL (β = −0.04, p = 0.685), or disability level (β = −0.12, p = 0.830) Pearson’s correlation coefficients from the sample showed strong positive correlations between self-efficacy and social health (r = 0.50, p = 0.000), psychological health (r = 0.70, p = 0.000), and HRQOL (r = 0.54, p = 0.000). Moderate positive correlations were found between self-efficacy and physical health (r = 0.45, p = 0.000). Additionally, there was a strong negative correlation between self-efficacy and disability level (r = −0.60, p = 0.000). The path analysis from the sample showed that self-efficacy significantly predicted social health (β = 12.71, p = 0.000), psychological health (β = 16.60, p = 0.000), physical health (β = 13.04, p = 0.000), HRQOL (β = 0.99, p = 0.000), and disability level (β = −7.37, p = 0.000) | Theme 1: Being a scuba diver is a positive social identity that provides me with a sense of belonging, meaning, and purpose. “I have a connection with other scuba divers, and with sea-related material like everyone in this community.” Alex “Scuba has had a huge impact on my life. I started scuba diving when I was 14. I got certified with my dad. And then, last year I got certified up to dive master and now, that’s actually what I do for a living…I’m a dive guide, like it’s really helped me.” Arden “One of my goals as part of my mission statement is to help other combat veterans reconnect to life through the outdoors. And one of my goals is to be able to pour into other combat veterans’ lives. I have been able to do that through scuba.” Briar Theme 2: Scuba diving has contributed positively to my social health through enhanced social relationships and a community that provides me with social support. “It helps you gain friendships, having camaraderie, the ability to meet new people, and when you find a group of people that have the same interest, it’s usually easier to become, have a friendship started. When I dive, I’m going to be in a pretty darn good mood, I’m pretty happy, so that helps you socially with your spouse, that helps you socially with your kids, or even friends.” Kim “Within the scuba diving community, everybody’s super supportive, it’s across the board, everybody respects you and you respect everybody, and it’s just a good community.” Devin “When I’m diving, I’m more, I guess you could say more friendlier to the others around me so, I’m more receptive to listening to people and I would open up some more.” Robin Theme 3: Scuba diving has contributed positively to my psychological health by enhancing self-esteem, positive feelings, and relaxation; and reducing symptoms of depression, anxiety, or post-traumatic stress disorder (PTSD). “Every time I get a new certification, it gives me more self-esteem, it gives me more pride.” Nat “You’re like there in the moment and enjoying it. For me, it becomes almost euphoric and there’s a high that exists for like a week after diving, where the decompression of doing the activity bleeds over into every aspect of my life in a positive way. More so, than other things that I do.” Terry “When I come out the water after diving, I’m not depressed, I’m not unhappy, I’m thrilled that I’m doing it, I know I’m in the place where I should be at. For us, for the PTSD and everything like that I think it’s one of the best therapies out there, the best medicine for this kind of a disease.” Robin Theme 4: Scuba diving has contributed positively to my physical health by offering physical activity or exercise, better mobility, relief from physical pain, and better sleep. “It helps me stay active…I wanted to lose weight when I started, when I first started receiving the training for the certification, and I was able to do it because it got me moving.” Sal “Scuba has helped decrease my pain…it physically makes me more tired, so I can sleep better and gets rid of my pain, so I can sleep better…it helps me stay more mobile. If I hurt, I don’t want to move. I get in the water, I don’t hurt, I move. Movement helps keep me active, scuba diving helps keep me active. Being active helps out my heart, my muscles, my joints.” Briar “I can feel like just the ability to move more fluidly in the water. Moving in those ways doesn’t hurt, so if it doesn’t hurt to move, mobility is improved, just hands down.” Terry Theme 5: Scuba diving has contributed positively to my self-efficacy by boosting my self-confidence. “Scuba has really deeply ignited confidence that was lost, it absolutely has influenced my self-confidence. Because of scuba diving, I did apply for a retreat and that’s not something I ever would have done, but scuba diving opened up that door for me to wanna go do that. As far as other things, I bike now, diving has helped me improve that to where now I can go bike riding.” Marion “It has influenced my confidence in that it goes back to that aspect of you know, if you can learn to do this, you can learn to do whatever else you come across in life.” Eli “It kind of goes back to you know, not knowing it’s possible, and now we know we can do this, let’s do more. After we dove a few times, my goal was to get 100 dives. When I hit 100 dives, I wanted to hit 200 dives. Now, I’m at 217; my next goal is 300.” Morgan Theme 6: Scuba diving has contributed positively to the quality of my life. “It’s expanded my life experiences, it’s expanded my social circle, and it’s given me an outdoor recreation activity that is new, and it’s something that I enjoy. It’s very much improved the quality of my life, very much.” Win “It influences me on my quality of life, my quality of life has improved because I’ve improved through my self-esteem because of being able to do different things with diving and learning.” Gael “Scuba is part of my life; it is a lifeline. It has influenced the quality of my life because it has left a positive influence, a positive striving influence, exciting influence, and lastly, it is something that I can do and enjoy.” Les | Data on social identity were not converged due to range restrictions on the quantitative strand on the scuba social identity variable. Range restrictions affect correlations and predictions, meaning the scuba diving social identity results for the correlation and path analyses may have underestimated the relationships between scuba social identity and the rest of the variables. The social identity approach to health, previous evidence on this theory, and the qualitative results support social identity as a predictor of health and HRQOL. Thus, we recommend future studies with individuals who have greater variability in their degree of scuba diving social identification. The quantitative results found self-efficacy as a strong predictor of social health, psychological health, physical health, HRQOL, and disability level among scuba divers with physical disabilities. The qualitative results indicated that participants perceived scuba diving to be a strong contributor to their self-efficacy; they attributed part of their enhanced self-efficacy to scuba diving. The qualitative results added meaningful insight and depth to the understanding of the dependent variables. The participants described scuba diving as a positive contributor to their social health, psychological health, physical health, and HRQOL. Further research on the mechanisms of scuba diving that may contribute to these outcomes would be worthwhile. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santiago Perez, T.; Crowe, B.M.; Rosopa, P.J.; Townsend, J.N.; Kaufman, M.R. Diving into Health: A Mixed Methods Study on the Impact of Scuba Diving in People with Physical Impairments. Healthcare 2023, 11, 984. https://doi.org/10.3390/healthcare11070984
Santiago Perez T, Crowe BM, Rosopa PJ, Townsend JN, Kaufman MR. Diving into Health: A Mixed Methods Study on the Impact of Scuba Diving in People with Physical Impairments. Healthcare. 2023; 11(7):984. https://doi.org/10.3390/healthcare11070984
Chicago/Turabian StyleSantiago Perez, Tania, Brandi M. Crowe, Patrick J. Rosopa, Jasmine N. Townsend, and Michael R. Kaufman. 2023. "Diving into Health: A Mixed Methods Study on the Impact of Scuba Diving in People with Physical Impairments" Healthcare 11, no. 7: 984. https://doi.org/10.3390/healthcare11070984