Alarming and/or Alerting Device Effectiveness in Reducing Falls in Long-Term Care (LTC) Facilities? A Systematic Review

 , ,
, ,
Abstract
:1. Introduction
1.1. Background
1.2. Significance
1.3. Objectives
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Exclusion Criteria
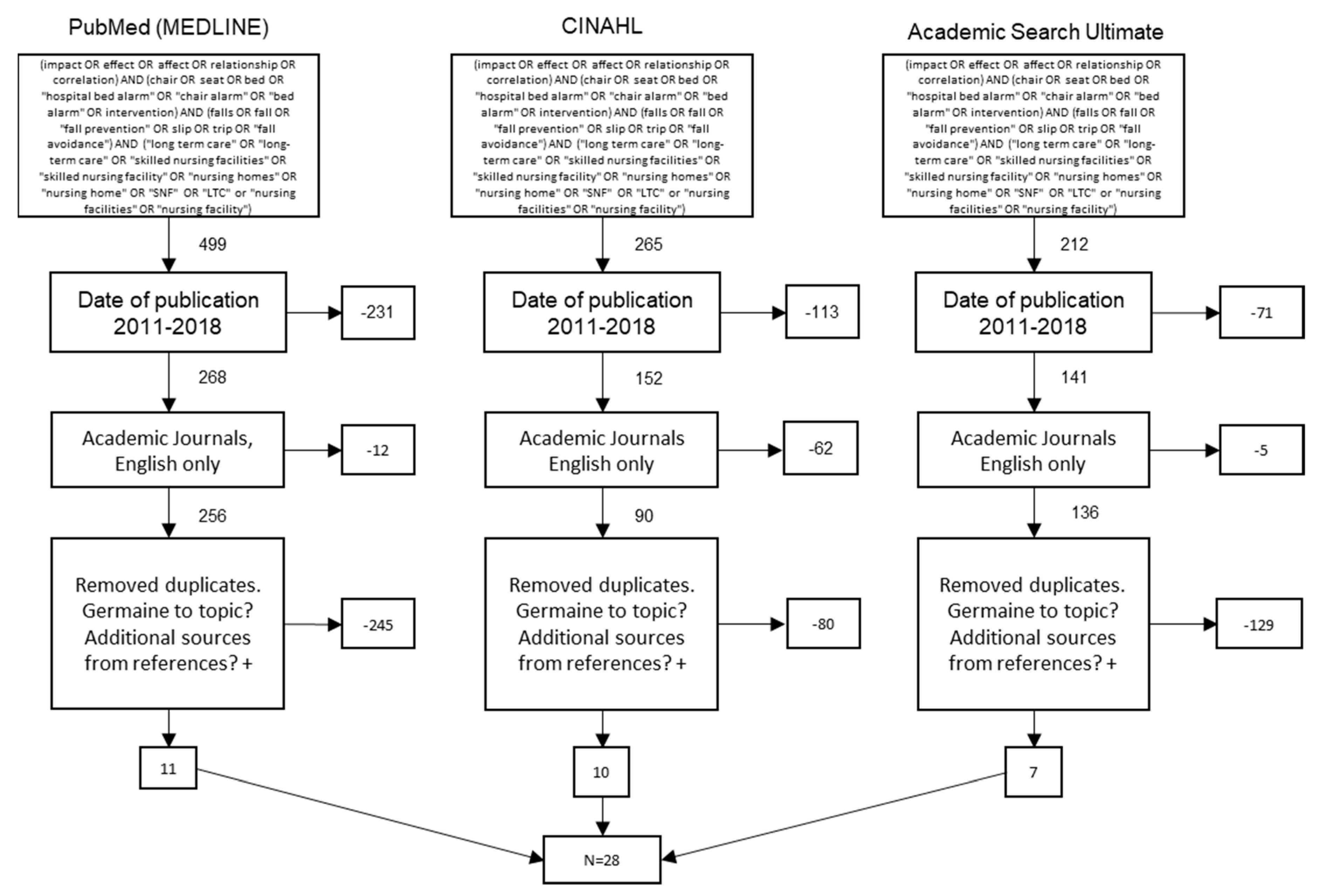
2.3. Study Selection
2.4. Data Analysis
3. Results
3.1. Facilitators
3.2. Barriers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Büchele, G.; Becker, C.; Cameron, I.; König, H.; Robinovitch, S.; Rapp, K. Predictors of serious consequences of falls in residential aged care: Analysis of more than 70,000 falls from residents of Bavarian nursing homes. J. Am. Med. Dir. Assoc. 2014, 15, 559–563. [Google Scholar] [CrossRef]
- Bergen, G.; Burns, E.; Stevens, M. Falls and fall injuries among adults aged ≥65 years—United States, 2014. Morb. Mortal. Wkly. Rep. 2016, 65, 938–983. [Google Scholar] [CrossRef] [PubMed]
- Fonad, E.; Emami, A.; Wahlin, T.; Winblad, B.; Sandmark, H. Falls in somatic and dementia wards at community care units. Scand. J. Caring Sci. 2009, 23, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Quigley, P.; Bulat, T.; Kurtzman, E.; Olney, R.; Powell-Cope, G.; Rubenstein, L. Clinical practice in long-term care: Fall prevention and injury protection for nursing home residents. J. Am. Med. Dir. Assoc. 2010, 11, 284–293. [Google Scholar] [CrossRef]
- Vlaeyen, E.; Coussement, J.; Leysens, G.; Van der Elst, E.; Delbaere, K.; Cambier, D.; Denhaerynck, K.; Goemaere, S.; Wertelaers, A.; Dobbels, F.; et al. Characteristics and effectiveness of fall prevention programs in nursing homes: A systematic review and meta-analysis of randomized controlled trials. J. Am. Geriatr. Soc. 2015, 63, 211–221. [Google Scholar] [CrossRef]
- Francisco Álvarez, B.; Borja d Jesús d Rosa, M.A.; Borja Sañudo, C.; Michael, E.R. Factors associated with the risk of falls of nursing home residents aged 80 or older. Rehabil. Nurs. J. 2016, 41, 16–25. [Google Scholar] [CrossRef]
- Crogan, N.; Dupler, A. Quality improvement in nursing homes: Testing of an alarm elimination program. J. Nurs. Care Qual. 2014, 29, 60–65. [Google Scholar] [CrossRef]
- Horn, S.; Hudak, S.; Barrett, R.; Cohen, L.; Reed, D.; Zimmerman, S. Interpersonal care processes, falls, and hospitalizations in green house and other nursing homes. Sr. Hous. Care J. 2016, 24, 31–46. [Google Scholar]
- Neyens, J.; van Haastregt, J.; Dijcks, B.; Martens, M.; van den Heuvel, W.; de Witte, L.P.; Schols, J. Effectiveness and implementation aspects of interventions for preventing falls in elderly people in long-term care facilities: A systematic review of RCTs. J. Am. Med. Dir. Assoc. 2011, 12, 410–425. [Google Scholar] [CrossRef] [PubMed]
- Wells, P. Preventing Falls in a Nursing Home. Doctoral Dissertation, A.T. Still University of Health Sciences, Kirksville, MO, USA, 2017. [Google Scholar]
- Capezuti, E.; Brush, B.; Lane, S.; Rabinowitz, H.; Secic, M. Bed-exit alarm effectiveness. Arch. Gerontol. Geriatr. 2009, 49, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Hilbe, J.; Schulc, E.; Linder, B.; Them, C. Development and alarm threshold evaluation of a side rail integrated sensor technology for the prevention of falls. Int. J. Med. Inform. 2010, 79, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Kosse, N.; Brands, K.; Bauer, J.; Hortobagyi, T.; Lamoth, C. Sensor technologies aiming at fall prevention in institutionalized old adults: A synthesis of current knowledge. Int. J. Med. Inform. 2013, 82, 743–752. [Google Scholar] [CrossRef]
- Powell-Cope, G.; Campbell, R.; Hahm, B.; Bulat, T.; Westphal, J. Sociotechnical probabilistic risk modeling to predict injurious falls in community living centers. J. Rehabil. Res. Dev. 2016, 53, 881–892. [Google Scholar] [CrossRef]
- Tzeng, H.M.; Prakash, A.; Brehob, M.; Anderson, A.; Devecsery, D.A.; Yin, C.Y. How feasible was a bed-height alert system? Clin. Nurs. Res. 2013, 22, 300–309. [Google Scholar] [CrossRef] [PubMed]
- Shorr, R.; Chandler, A.; Mion, L.; Waters, T.; Liu, M.; Daniels, M.J.; Kessler, L.A.; Miller, S.T. Effects of an intervention to increase bed alarm use to prevent falls in hospitalized residents: A cluster randomized trial. Ann. Intern. Med. 2012, 157, 692–699. [Google Scholar] [CrossRef]
- Wong Shee, A.; Phillips, B.; Hill, K.; Dodd, K. Feasibility, acceptability, and effectiveness of an electronic sensor bed/chair alarm in reducing falls in residents with cognitive impairment in a subacute ward. J. Nurs. Care Qual. 2014, 29, 253–262. [Google Scholar] [CrossRef]
- Coyle, R. Initiating and sustaining a fall prevention program. Nursing 2016, 46, 16–21. [Google Scholar] [CrossRef]
- Johnson, M.; Kelly, L.; Siric, K.; Tran, D.; Overs, B. Improving falls risk screening and prevention using an e-learning approach. J. Nurs. Manag. 2015, 23, 910–919. [Google Scholar] [CrossRef]
- Ranasinghe, D.; Shinmoto Torres, R.; Hill, K.; Visvanathan, R. Low cost and batteryless sensor-enabled radio frequency identification tag based approaches to identify resident bed entry and exit posture transitions. Gait Posture 2014, 39, 118–123. [Google Scholar] [CrossRef] [PubMed]
- Subermaniam, K.; Welfred, R.; Subramanian, P.; Chinna, K.; Ibrahim, F.; Mohktar, M.; Tian, M. The effectiveness of a wireless modular bed absence sensor device for fall prevention among older inpatients. Front. Public Health 2016, 4, 292. [Google Scholar] [CrossRef]
- Barker, A.; Morello, R.; Ayton, D.; Hill, K.; Brand, C.; Livingston, P.M.; Botti, M. Acceptability of the 6-PACK falls prevention program: A pre-implementation study in hospitals participating in a cluster randomized controlled trial. PLoS ONE 2017, 12, e0172005. [Google Scholar] [CrossRef]
- Bressler, K.; Redfern, R.; Brown, M. Elimination of position-change alarms in an Alzheimer’s and dementia long-term care facility. Am. J. Alzheimers Dis. Other Dement. 2011, 26, 599–605. [Google Scholar] [CrossRef]
- Cangany, M.; Back, D.; Hamilton-Kelly, T.; Altman, M.; Lacey, S. Bedside nurses leading the way for falls prevention: An evidence-based approach. Crit. Care Nurse 2015, 35, 82–84. [Google Scholar] [CrossRef] [PubMed]
- Chu, R. Preventing in-resident falls: The nurse’s pivotal role. Nursing 2017, 47, 25–30. [Google Scholar] [CrossRef]
- Horton, K. Falls in older people: The place of telemonitoring in rehabilitation. J. Rehabil. Res. Dev. 2008, 45, 1183–1194. [Google Scholar] [CrossRef]
- Lach, H.; Parsons, J. Impact of fear of falling in long term care: An integrative review. J. Am. Med. Dir. Assoc. 2013, 14, 573–577. [Google Scholar] [CrossRef] [PubMed]
- Sahota, O.; Drummond, A.; Kendrick, D.; Grainge, M.; Vass, C.; Avis, M. REFINE (Reducing Falls in In-resident Elderly) using bed and bedside chair pressure sensors linked to radio-pagers in acute hospital care: A randomised controlled trial. Age Ageing 2014, 43, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Vandenberg, A.; van Beijnum, B.; Overdevest, V.; Capezuti, E.; Johnson, I. US and Dutch nurse experiences with fall prevention technology within nursing home environment and workflow: A qualitative study. Geriatr. Nurs. 2017, 38, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Vassallo, M.; Wilkinson, C.; Stockdale, R.; Malik, N.; Baker, R.; Allen, S. Attitudes to restraint for the prevention of falls in hospital. Gerontology 2005, 51, 66–70. [Google Scholar] [CrossRef]
- Holmes, D.; Teresi, J.; Ramirez, M.; Eimicke, J.; Ellis, J.; Kong, J.; Orzechowska, L.; Silver, S. An evaluation of a monitoring system intervention: Falls, injuries, and affect in nursing homes. Clin. Nurs. Res. 2007, 16, 317–335. [Google Scholar] [CrossRef]
- Nitz, J.; Cyarto, E.; Andrews, S.; Fearn, M.; Fu, S.; Haines, T.; Haralambous, B.; Hill, K.; Hunt, S.; Lea, E.; et al. Outcomes from the implementation of a facility-specific evidence-based falls prevention intervention program in residential aged care. Geriatr. Nurs. 2012, 3, 341–350. [Google Scholar] [CrossRef] [PubMed]
- Torres, R.; Visvanathan, R.; Hoskins, S.; van den Hengel, A.; Ranasinghe, D. Effectiveness of a batteryless and wireless wearable sensor system for identifying bed and chair exits in healthy older people. Sensors 2016, 16, 546. [Google Scholar] [CrossRef] [PubMed]
- Wagner, J.; Mazurek, P.; Miękina, A.; Morawski, R.; Jacobsen, F.; Sudmann, T.T.; Børsheim, I.T.; Øvsthus, K.; Ciamulski, T. Comparison of two techniques for monitoring of human movements. Measurement 2017, 111, 420–431. [Google Scholar] [CrossRef]
- Wickramasinghe, A.; Ranasinghe, D.; Fumeaux, C.; Hill, K.; Visvanathan, R. Sequence learning with passive RFID sensors for real-time bed-egress recognition in older people. IEEE J. Biomed. Health Inform. 2017, 21, 917–929. [Google Scholar] [CrossRef]
- Hamm, J.; Money, A.; Atwal, A.; Paraskevopoulos, I. Fall prevention intervention technologies: A conceptual framework and survey of the state of the art. J. Biomed. Inform. 2016, 59, 319–345. [Google Scholar] [CrossRef] [PubMed]
- Nazir, A.; Mueller, C.; Perkins, A.; Arling, G. Falls and nursing home residents with cognitive impairment: New insights into quality measures and interventions. J. Am. Med. Dir. Assoc. 2012, 13, 819.e1–819.e6. [Google Scholar] [CrossRef]


{kind=link}
| Facilitators | Occurrences | Sum | % |
|---|---|---|---|
| Proper implementation of alarms improves care | [7,11,12,18,22,23,24,25] *, [16,17,28,29] | 17 | 29.80% |
| Technology improvements have increased alarm efficacy | [11,14,17] *, [12,13,15,16,20,21] | 16 | 28.10% |
| Proper implementation of alarms reduces fall risk | [15,32] *, [17,19,28,34,35] | 10 | 17.50% |
| Improved resident quality of life | [17,31], [26] * | 6 | 10.50% |
| Resident education about falls is important | [18,36] | 2 | 3.50% |
| Proper implementation of alarms improves alarm efficacy | [33] * | 2 | 3.50% |
| Improved care for residents with cognitive impairment with alarms | [27] | 1 | 1.80% |
| Staff in favor of alarms | [15] | 1 | 1.80% |
| Staff interaction with residents reduces fall risk | [21] | 1 | 1.80% |
| Staff training in alarm use | [19] | 1 | 1.80% |
| Total | 57 | 100% |
| Barriers | Occurrences | Sum | % |
|---|---|---|---|
| Ineffective as standalone intervention | [16,21,22,23,24,28] *, [12,13,15,19,25,27,30,31,32,36] | 23 | 37.70% |
| Alarm fatigue by caregiver | [17,22,23,26,34], [14,16,21,33] * | 12 | 19.70% |
| Difficult to implement properly | [7,12,14,15,16,18,28,37] | 8 | 13.10% |
| Expensive to implement | [16,18,28,33,35] | 5 | 8.20% |
| Increased staff burden | [15,18,22,29] | 4 | 6.60% |
| Alarm noise annoyance | [11,17,23] | 3 | 4.90% |
| Noise of alarms startles residents | [23] *, [11] | 3 | 4.90% |
| Resident reluctance | [26] * | 3 | 4.90% |
| Total | 61 | 100% |
| Summary of Facilitators | Summary of Barriers |
|---|---|
| Nurses perceived bed/chair alarms as a useful way to prevent resident falls. | Alarms must be consistently monitored and kept in working order. |
| Alarm systems which send signals directly to caregivers for immediate action are more effective in use. | Concerns exist when alarms are used on residents who are isolated from others, or if there are too many alarms in use in one area. |
| Bed alarms as part of a comprehensive fall prevention plan reduce falls. | Alarms alone do not reduce fall rates. |
| The use of infrared beam detectors along with alarms can promote the timely activation of the alarm. | Alarms can startle residents, causing negative effects from this reaction, and could potentially cause a fall. These loud sounds may cause a flight response in residents. |
| Tailoring the alarm type to resident characteristics can improve alarm performance and ultimately reduce the risk of falls and related injuries. | Alarms can be viewed as loud and burdensome to other residents because of their environmental impact. |
| Alarms using dual pressure sensors plus infrared beam detectors were more accurate than only pressure sensitive alarms in identifying bed-exiting. | Equipment malfunctions associated with medical technology can increase workload for nurses. |
| Fall prevention initiatives and activities must be in the forefront of all activities in the facility for the best effectiveness. | Bed and chair alarms must be implemented correctly to reduce fall rates. Otherwise, they could be contributors. |
| Resident education about fall prevention and safety awareness can also be an effective method at reducing falls. | False alarms can be burdensome on staff and residents and can contribute to "alarm fatigue" by staff members. |
| Focus on resident self-assessment and feedback regarding fall risk can assist in reducing falls. | Devices became a “nuisance” to residents because of their functionality and application. |
| Use of monitoring system can have a positive impact on resident quality of life. | |
| Residents with a fall risk can have a greater sense of security when using alarming systems. | Residents may be reluctant to wear alarms because they do not want to inconvenience others or lose their independence. |
| Residents who wore their fall detector felt more confident and independent and reported that devices improved their safety and decreased their fear of falling. | No consistent evidence that current sensor technology reduces fall rates |
| Bed-exit alarms used with confused and agitated residents may have helped reduce falls. | Those who consider alarming-device restraints perceive these devices to contribute to a lower quality of life for residents and a potential source of additional injuries. |
| Bed height alerting systems can also have a positive impact upon reducing resident falls. | Residents are often able to disconnect the alarms on their own, rendering them useless. |
| Interventions such as a falls risk flag in the records/on beds, additional supervision when the resident is mobilizing or in the bathroom, keeping areas clear of hazards, and use of chair/bed alarms can reduce falls. | Cost effectiveness of alarms and alarming systems is a concern. |
| Reducing the number of unassisted transfers through a modest improvement in response time to alarms can positively affect fall numbers. | Alarm signals may occur after residents had already fallen because they fell immediately on exiting the bed or chair. |
| Coworkers aware of and assisting with alarm devices decreased the noncompliance rates resident alarms from 50 to 30 percent. | |
| Reduce false positives by using alarm systems that allow for adjusting sensitivities. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mileski, M.; Brooks, M.; Topinka, J.B.; Hamilton, G.; Land, C.; Mitchell, T.; Mosley, B.; McClay, R. Alarming and/or Alerting Device Effectiveness in Reducing Falls in Long-Term Care (LTC) Facilities? A Systematic Review. Healthcare 2019, 7, 51. https://doi.org/10.3390/healthcare7010051
Mileski M, Brooks M, Topinka JB, Hamilton G, Land C, Mitchell T, Mosley B, McClay R. Alarming and/or Alerting Device Effectiveness in Reducing Falls in Long-Term Care (LTC) Facilities? A Systematic Review. Healthcare. 2019; 7(1):51. https://doi.org/10.3390/healthcare7010051
Chicago/Turabian StyleMileski, Michael, Matthew Brooks, Joseph Baar Topinka, Guy Hamilton, Cleatus Land, Traci Mitchell, Brandy Mosley, and Rebecca McClay. 2019. "Alarming and/or Alerting Device Effectiveness in Reducing Falls in Long-Term Care (LTC) Facilities? A Systematic Review" Healthcare 7, no. 1: 51. https://doi.org/10.3390/healthcare7010051