The Perimenopausal Fatigue Self-Management Scale Is Suitable for Evaluating Perimenopausal Taiwanese Women’s Vulnerability to Fatigue Syndrome


Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Subjects
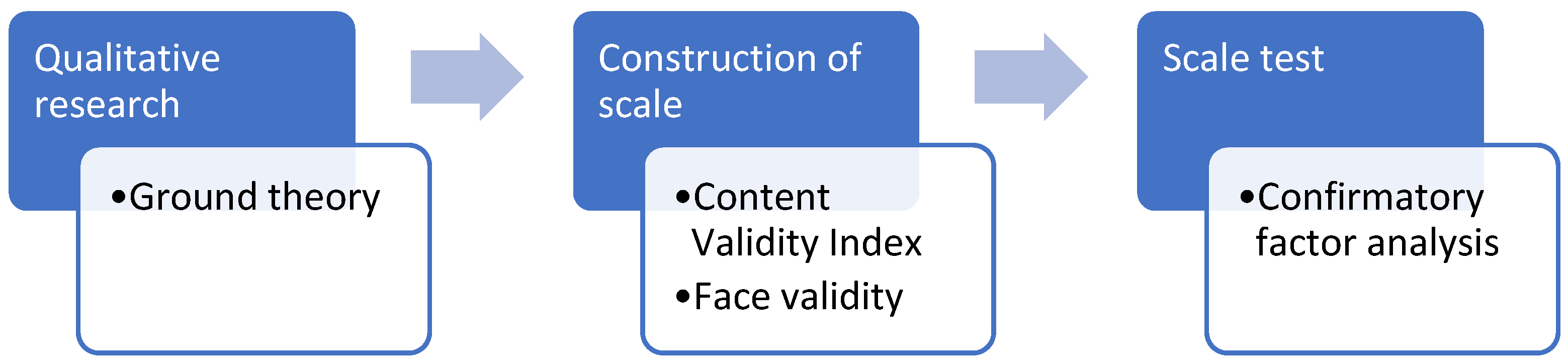
2.3. Development of the Perimenopausal Fatigue Self-Management Scale (P-MFSMS)
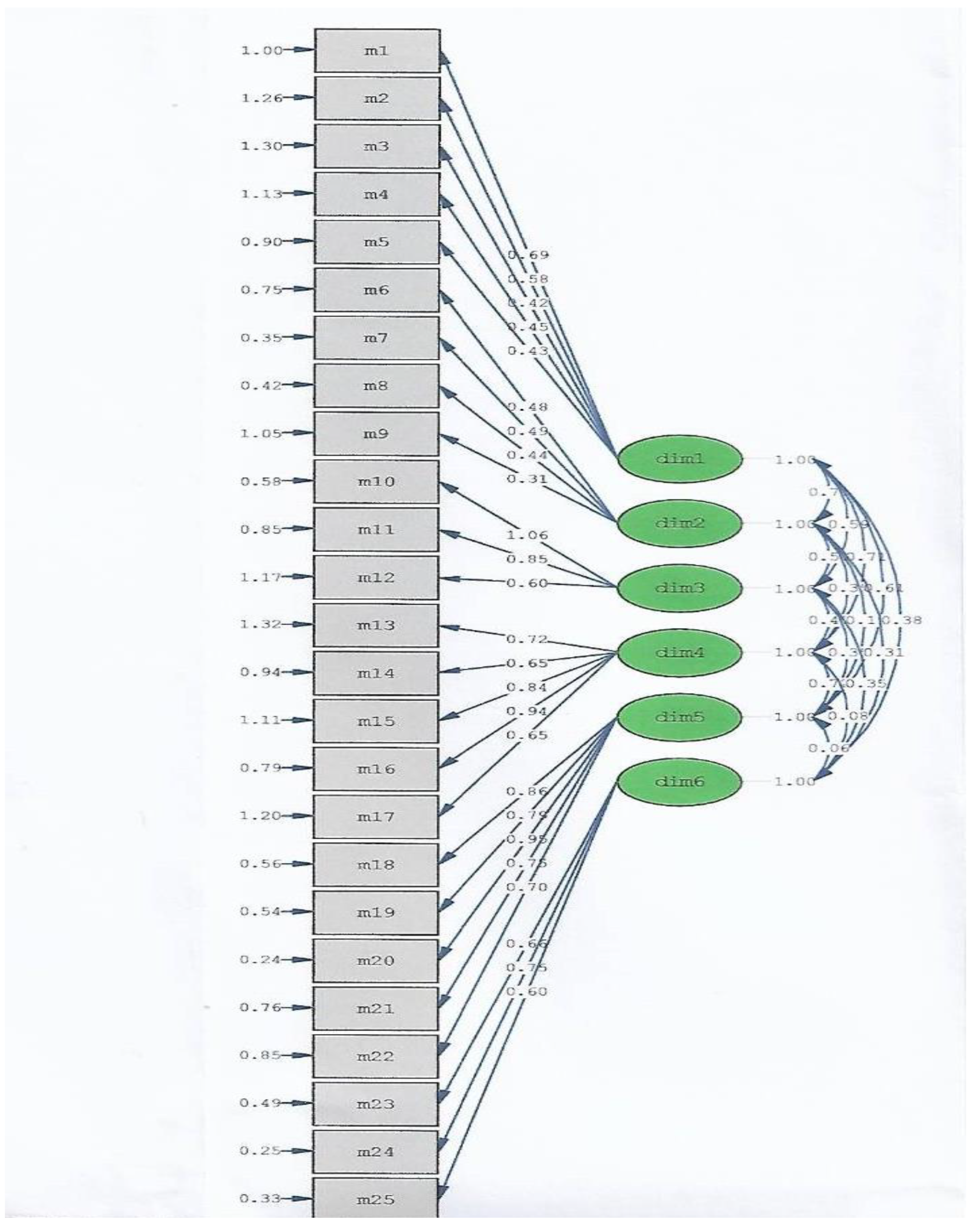
2.4. Analysis
3. Results
3.1. Demographics
3.2. The Perimenopausal Fatigue Self-Management Scale (P-MFSMS)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BMI | body mass index |
| CFS | chronic fatigue syndrome |
| CFI | Comparative Fit Index |
| CFA | confirmatory factor analysis |
| CVI | content validity index |
| DIF | differential item function |
| EFA | exploratory factor analysis |
| IFI | Incremental Fit Index |
| IRB | Institutional Review Board |
| KMO | Kaiser–Meyer–Olkin |
| MSA | measure of sampling adequacy |
| P-MFSMS | perimenopausal fatigue self-management scale |
| RMSEA | root mean square error of approximation |
| SD | standard deviation |
| SE | Standard error |
| TLI | Tucker–Lewis Index |
References
- Boneva, R.S.; Lin, J.M.S.; Unger, E.R. Early menopause and other gynecologic risk indicators for chronic fatigue syndrome in women. Menopause 2015, 22, 826–834. [Google Scholar] [CrossRef] [Green Version]
- Ali, A.M.; Ahmed, A.H.; Smail, L. Psychological climacteric symptoms and attitudes toward menopause among Emirati women. Int. J. Environ. Res. Public. Health 2020, 17, 5028. [Google Scholar] [CrossRef]
- Park, J.; Han, S.; Park, H. Effect of Schisandra Chinensis extract supplementation on quadriceps muscle strength and fatigue in adult women: A randomized, double-blind, placebo-controlled trial. Int. J. Environ. Res. Public. Health 2020, 17, 2475. [Google Scholar] [CrossRef] [Green Version]
- Taylor-Swanson, L.; Wong, A.E.; Pincus, D.; Butner, J.E.; Hahn-Holbrook, J.; Koithan, M.; Wann, K.; Woods, N.F. The dynamics of stress and fatigue across menopause: Attractors, coupling, and resilience. Menopause 2018, 25, 380–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, P.S.; Lee, C.L. Prevalence of symptoms and associated factors across menopause status in Taiwanese women. Menopause 2020, 28, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Chiu, H.H.; Wu, S.F.; Wang, P.H. The experience of menopausal women participating in weight management program: A pilot study. Taiwan J. Obstet. Gynecol. 2020, 59, 686–690. [Google Scholar] [CrossRef]
- Chang, C.; Chow, S.N.; Chen, F.L.; Chang, C.H. Menopausal symptoms reported by women in Taipei. Chin. J. Public. Health 1995, 14, 191–200, (In Chinese, English Abstract). [Google Scholar]
- Szu, L.Y.; Liu, C.F.; Sun, M.F.; Chou, P.C.; Huang, T.H.; Tseng, S.M.; Tsao, L.I. The effects of baduanjin sport on perimenopausal disturbances and bone mineral content among perimenopausal women. Chang Gung Nurs. 2012, 23, 1–13. [Google Scholar]
- Hall, M.N.; Leach, L.; Kynerd, R. Clinical inquiries. In menopausal women, does fatigue indicate disease? J. Fam. Pract. 2005, 54, 895–896. [Google Scholar]
- Lo, H.Y.; Lee, S. The influence of climacteric symptoms on self-efficacy in health behavior. Chung Shan Med. J. 2006, 17, 153–168. [Google Scholar]
- Huang, H.M.; Chao, H.T.; Lin, K.C.; Cheng, S.Y.; Liao, Y.M. Menopausal symptoms and factors related to quality life among a sample of women 45–60 years of age. New Taipei J. Nurs. 2010, 12, 7–20, (In Chinese, English Abstract). [Google Scholar]
- Hsiang, C.Y.; Lee, J.Z.; Cheng, S.Y. The effect of symptom distress, resilience and family support on health status of menopausal women. New Taipei J. Nurs. 2014, 16, 31–41, (In Chinese, English Abstract). [Google Scholar]
- Du, L.; Xu, B.; Huang, C.; Zhu, L.; He, N. Menopausal symptoms and perimenopausal healthcare-seeking behavior in women aged 40-60 years: A community-based cross-sectional survey in Shanghai, China. Int. J. Environ. Res. Public Health 2020, 17, 2640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mikolasek, M.; Witt, C.M.; Barth, J. Effects and implementation of a mindfulness and relaxation App for patients with cancer: Mixed methods feasibility study. JMIR Cancer 2021, 7, e16785. [Google Scholar] [CrossRef]
- Oliver, A.; Galiana, L.; Simone, G.; Tomás, J.M.; Arena, F.; Linzitto, J.; Grance, G.; Sansó, N. Palliative care professionals’ inner lives: Cross-cultural application of the awareness model of self-care. Healthcare 2021, 9, 81. [Google Scholar] [CrossRef] [PubMed]
- Koo, M.M.; Swann, R.; McPhail, S.; Abel, G.A.; Elliss-Brookes, L.; Rubin, G.P.; Lyratzopoulos, G. Presenting symptoms of cancer and stage at diagnosis: Evidence from a cross-sectional, population-based study. Lancet Oncol. 2020, 21, 73–79. [Google Scholar] [CrossRef] [Green Version]
- Whicker, M.; Black, J.; Altwerger, G.; Menderes, G.; Feinberg, J.; Ratner, E. Management of sexuality, intimacy, and menopause symptoms in patients with ovarian cancer. Am. J. Obstet. Gynecol. 2017, 217, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Lyu, X.; Liu, Y.; Yu, H.; Mi, M.; Shang, L.; Zhong, Y.; Xie, D. Development and validation of a risk perception scale of medical help-seeking behavior in Chinese adults. Ann. Transl. Med. 2020, 8, 1352. [Google Scholar] [CrossRef]
- Ahmad, N.F.D.; Ren Jye, A.K.; Zulkifli, Z.; Bujang, M.A. The development and validation of job satisfaction questionnaire for health workforce. Malays. J. Med. Sci. 2020, 27, 128–143. [Google Scholar]
- Abdullah, N.; Kueh, Y.C.; Kuan, G.; Wong, M.S.; Yahaya, F.H.; Lee, Y.Y. Validity and reliability of the newly developed Malay-language health belief of bloating (HB-Bloat) scale. Int. J. Environ. Res. Public. Health 2020, 17, 2773. [Google Scholar] [CrossRef] [Green Version]
- Davis, S.R.; Lambrinoudaki, I.; Lumsden, M.; Mishra, G.D.; Pal, L.; Rees, M.; Santoro, N.; Simoncini, T. Menopause. Nat. Rev. Dis. Primers 2015, 1, 15004. [Google Scholar] [CrossRef]
- Jane, F.M.; Davis, S.R. A practitioner’s toolkit for managing the menopause. Climacteric 2014, 17, 564–579. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, M.; Raval, A.P. The peri-menopause in a woman’s life: A systemic inflammatory phase that enables later neurodegenerative disease. J. Neuroinflam. 2020, 17, 317. [Google Scholar] [CrossRef]
- André, N.; Agbangla, N.F. Are barriers the same whether I want to start or maintain exercise? A narrative review on healthy older adults. Int. J. Environ. Res. Public. Health 2020, 17, 6247. [Google Scholar] [CrossRef]
- Bartlett, M.S. The goodness of fit of a single hypothetical discriminant function in the case of several groups. Ann. Eugen. 1951, 16, 199–214. [Google Scholar] [CrossRef]
- Bentler, P.M.; Bonett, D.G. Significance tests and goodness-of –fit in the analysis of covariance structures. Psychlogical. Bull. 1980, 88, 588–606. [Google Scholar] [CrossRef]
- de Barros Ahrens, R.; da Silva Lirani, L.; de Francisco, A.C. Construct validity and reliability of the work environment assessment instrument WE-10. Int. J. Environ. Res. Public Health 2020, 17, 7364. [Google Scholar] [CrossRef] [PubMed]
- Li, D.J.; Kao, W.T.; Shieh, V.; Chou, F.H.; Lo, H.A. Development and Implementation of Societal Influences Survey Questionnaire (SISQ) for Peoples during COVID-19 Pandemic: A Validity and Reliability Analysis. Int. J. Environ. Res. Public Health 2020, 17, 6246. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.; Ham, Y.H.; Han, K.; Ryu, E. Knowing in nurses’ belief and attitude about patient activation: A validation of the Korean clinician support for patient activation measure using rasch analysis. Healthcare 2020, 8, 571. [Google Scholar] [CrossRef]
- Martins, M.A.; Neves, A.N.; Moss, T.; Martins, W.H.; Pereira, G.V.; Pessôa, K.V.O.; Silva, M.H.D.; de Abreu, L.C. Psychometric validation of the Brazilian Portuguese version of the Derriford Appearance Scale-24 (DAS-24) for people living with HIV/AIDS. Healthcare 2020, 8, 569. [Google Scholar] [CrossRef] [PubMed]
- Hee, O.C. Validity and reliability of the Customer-Oriented Behaviour Scale in the health Tourism Hospitals in Malaysia. Inter. J. Caring Sci. 2014, 7, 771–775. [Google Scholar]
- Bland, J.; Altman, D. Statistics notes: Cronbach’s alpha. BMJ 1997, 314, 275. [Google Scholar] [CrossRef] [Green Version]
- Tavakol, M.; Dennick, R. Making sense of Cronbach’s alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef]
- Bujang, M.A.; Omar, E.D.; Baharum, N.A. A review on sample size determination for Cronbach’s alpha test: A simple guide for researchers. Malays. J. Med. Sci. 2018, 25, 85–99. [Google Scholar] [CrossRef] [PubMed]
- Corrêa, J.É.; Turrioni, J.B.; Mello, C.H.P.; Santos, A.C.O.; da Silva, C.E.S.; de Almeida, F.A. Development of a system measurement model of the Brazilian hospital accreditation system. Int. J. Environ. Res. Public. Health 2018, 15, 2520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, J.M.; Hsu, C.Y.; Tsai, L.Y.; Tsay, S.L. Translation and validation of Taiwan Chinese version of the self-regulation questionnaire for gynecologic cancer survivors. Taiwan. J. Obstet. Gynecol. 2019, 58, 614–620. [Google Scholar] [CrossRef] [PubMed]
- Liao, H.C.; Wang, Y.H. Development and validation of a Chinese version of a professional identity scale for healthcare students and professionals. Healthcare 2020, 8, 451. [Google Scholar] [CrossRef] [PubMed]
- Gajda, M.; Szemik, S.; Sedlaczek, K.; Kowalska, M. The reliability and compatibility of the paper and electronic versions of the POLLEK cohort study questionnaire. Healthcare 2020, 8, 438. [Google Scholar] [CrossRef]
- Jeng, C.J.; Hou, M.F.; Liu, H.Y.; Wang, L.R.; Chen, J.J. Construction of an integrated sexual function questionnaire for women with breast cancer. Taiwan J. Obstet. Gynecol. 2020, 59, 534–540. [Google Scholar] [CrossRef]
- Kim, J.; Heo, S.; Hong, S.W.; Kim, H.; Jung, A.; An, M.; Shim, J. Psychometric testing of the Korean version of the attitudes toward the advance directives in low-income chronically ill older adults. Healthcare 2020, 8, 62. [Google Scholar] [CrossRef] [Green Version]
- Hou, G.; Fang, Z.; Cao, W.; Shi, Y.; Xu, X.; Han, M.; Dong, J. Development and validation of a diabetes mellitus treatment adherence scale. Diabetes Res. Clin. Pract. 2020, 172, 108629. [Google Scholar] [CrossRef] [PubMed]
- Choe, K.; Ryu, E.; Kim, S. Feasibility of the schizophrenia hope scale-9: A psychometric study. Int. J. Environ. Res. Public Health 2020, 17, 8635. [Google Scholar] [CrossRef] [PubMed]
- González-Cabrera, M.; Ortega-Martínez, A.R.; Martínez-Galiano, J.M.; Hernández-Martínez, A.; Parra-Anguita, L.; Frías-Osuna, A. Design and validation of a questionnaire on communicating bad news in nursing: A pilot study. Int. J. Environ. Res. Public Health 2020, 17, 457. [Google Scholar] [CrossRef] [Green Version]
- Vidal-Alaball, J.; Flores Mateo, G.; Garcia Domingo, J.L.; Marín Gomez, X.; Sauch Valmaña, G.; Ruiz-Comellas, A.; López Seguí, F.; García Cuyàs, F. Validation of a short questionnaire to assess healthcare professionals’ perceptions of asynchronous telemedicine services: The catalan version of the health optimum telemedicine acceptance questionnaire. Int. J. Environ. Res. Public Health 2020, 17, 2202. [Google Scholar] [CrossRef] [Green Version]
- Hasan, S.I.; Mohd Hairi, F.; Amer Nordin, A.S.; Danaee, M. Development and validation of an evaluation tool to measure the effectiveness of a smoking cessation training among healthcare providers in Malaysia: The providers’ smoking cessation training evaluation (ProSCiTE). Int. J. Environ. Res. Public Health 2019, 16, 4297. [Google Scholar] [CrossRef] [Green Version]
- Figueroa, R.; Gago, C.M.; Beckerman-Hsu, J.; Aftosmes-Tobio, A.; Yu, X.; Davison, K.K.; Jurkowski, J.J. Development and validation of a parental health-related empowerment scale with low-income parents. Int. J. Environ. Res. Public Health 2020, 17, 8645. [Google Scholar] [CrossRef] [PubMed]
- Macias-Velasquez, S.; Baez-Lopez, Y.; Maldonado-Macías, A.A.; Limon-Romero, J.; Tlapa, D. Burnout syndrome in middle and senior management in the industrial manufacturing sector of Mexico. Int. J. Environ. Res. Public Health 2019, 16, 1467. [Google Scholar] [CrossRef] [Green Version]
- MacCallum, R.; Browne, M.; Sugawara, H. Power analysis and determination of sample size for covariancestructure modeling. Psychol. Methods 1996, 1, 130–149. [Google Scholar] [CrossRef]
- Soeken, K.L. Validity of Measures, 3th ed.; Springer: New York, NY, USA, 2005; pp. 154–189. [Google Scholar]
- Jones, R.N. Differential item functioning and its relevance to epidemiology. Curr. Epidemiol. Rep. 2019, 6, 174–183. [Google Scholar] [CrossRef] [PubMed]
- Lundgren-Nilsson, Å.; Tennant, A.; Jakobsson, S.; Simrén, M.; Taft, C.; Dencker, A. Validation of fatigue impact scale with various item sets—A Rasch analysis. Disabil. Rehabil. 2019, 41, 840–846. [Google Scholar] [CrossRef] [Green Version]
- Thomas, S.; Kersten, P.; Thomas, P.W. The Multiple Sclerosis-Fatigue Self- Efficacy (MS-FSE) scale: Initial validation. Clin. Rehabil. 2015, 29, 376–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.; Lang, J.; Xuan, L.; Li, X.; Zhang, L. The effect of health literacy and self-management efficacy on the health-related quality of life of hypertensive patients in a western rural area of China: A cross-sectional study. Int. J. Equity. Health 2017, 16, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.; Fu, G.; Liang, F.; Wei, J.; He, J.; Bai, J. Symptoms, hope, self-management behaviors, and quality of life among Chinese preoperative patient with symptomatic valvular heart diseases. J. Transcult. Nurs. 2020, 31, 284–293. [Google Scholar] [CrossRef]
- Lou, Y.; Yates, P.; McCarthy, A.; Wang, H. Fatigue self-management: A survey of Chinese cancer patients undergoing chemotherapy. J. Clin. Nurs. 2013, 22, 1053–1065. [Google Scholar] [CrossRef]
- Kamp, K.J.; Weaver, K.R.; Sherwin, L.B.; Barney, P.; Hwang, S.K.; Yang, P.L.; Burr, R.L.; Cain, K.C.; Heitkemper, M.M. Effects of a comprehensive self-management intervention on extraintestinal symptoms among patients with IBS. J. Psychosom. Res. 2019, 126, 109821. [Google Scholar] [CrossRef]
- Baussard, L.; Carayol, M.; Porro, B.; Baguet, F.; Cousson-Gelie, F. Fatigue in cancer patients: Development and validation of a short form of the Multidimensional Fatigue Inventory (MFI-10). Eur. J. Oncol. Nurs. 2018, 36, 62–67. [Google Scholar] [CrossRef]
- O’Regan, P.; Hegarty, J. The importance of self-care for fatigue amongst patients undergoing chemotherapy for primary cancer. Eur. J. Oncol. Nurs. 2017, 28, 47–55. [Google Scholar] [CrossRef]
- Yancey, J.R.; Thomas, S.M. Chronic fatigue syndrome: Diagnosis and treatment. Am. Fam. Physician 2012, 86, 741–746. [Google Scholar] [PubMed]
- Cahill, C.A. Differential diagnosis of fatigue in women. J. Obstet. Gynecol. Neonatal. Nurs. 1999, 28, 81–86. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Qualitative Categories |
|---|
| 1. Strive to maintain work energy and efficiency |
| 2. Seek self-help from medical resources |
| 3. Strive to maintain normal operation of the family |
| 4. Make time for activities or exercise in busy life |
| 5. Slow down or adjust lifestyle |
| 6. Frustration |
| Ways of Dealing with Fatigue | Method | Effectiveness | ||||
|---|---|---|---|---|---|---|
| No | Yes | 25% | 50% | 75% | 100% | |
| Strive to maintain work energy and efficiency | ||||||
| 1. You have temporarily left your work and not thought of other things to give yourself a break. | 0 | 1 | 1 | 2 | 3 | 4 |
| 2. You have drunk coffee to refresh yourself. | 0 | 1 | 1 | 2 | 3 | 4 |
| 3. You have kept yourself busy. | 0 | 1 | 1 | 2 | 3 | 4 |
| 4. You have canceled a scheduled plan or arrangement. | 0 | 1 | 1 | 2 | 3 | 4 |
| 5. You have consulted people who have gone through menopause. | 0 | 1 | 1 | 2 | 3 | 4 |
| Seek self-help from medical resources | ||||||
| 6. You have turned to traditional Chinese medicine to treat fatigue. | 0 | 1 | 1 | 2 | 3 | 4 |
| 7. You have sought psychological counseling. | 0 | 1 | 1 | 2 | 3 | 4 |
| 8. You have used Western medicine to supply hormone supplements. | 0 | 1 | 1 | 2 | 3 | 4 |
| 9. You have used healthy foods or other alternative therapies. | 0 | 1 | 1 | 2 | 3 | 4 |
| Strive to maintain normal operation of the family | ||||||
| 10. You have asked your family to share the housework. | 0 | 1 | 1 | 2 | 3 | 4 |
| 11. You have asked your family to help buy daily necessities. | 0 | 1 | 1 | 2 | 3 | 4 |
| 12. You have relieved discomfort through a body massage and other methods. | 0 | 1 | 1 | 2 | 3 | 4 |
| Make time for activities or exercise in busy life | ||||||
| 13. You have found partners to participate in activities. | 0 | 1 | 1 | 2 | 3 | 4 |
| 14. You have arranged simple and non-time-consuming activities, such as getting up and drinking water from time to time. | 0 | 1 | 1 | 2 | 3 | 4 |
| 15. You have found time to exercise to increase your physical fitness. | 0 | 1 | 1 | 2 | 3 | 4 |
| 16. You have listened to music to relax. | 0 | 1 | 1 | 2 | 3 | 4 |
| 17. You have meditated or sat still. | 0 | 1 | 1 | 2 | 3 | 4 |
| Slow down or adjust lifestyle | ||||||
| 18. You have lived with these fatigue symptoms or discomfort. | 0 | 1 | 1 | 2 | 3 | 4 |
| 19. You have endured fatigue. | 0 | 1 | 1 | 2 | 3 | 4 |
| 20. You can bear these fatigue experiences. | 0 | 1 | 1 | 2 | 3 | 4 |
| 21. For fatigue, you have adjusted your future lifestyle. | 0 | 1 | 1 | 2 | 3 | 4 |
| 22. For fatigue, you have shared your management experiences with others. | 0 | 1 | 1 | 2 | 3 | 4 |
| Frustration | ||||||
| 23. You feel helpless about fatigue. | 0 | 1 | 1 | 2 | 3 | 4 |
| 24. You feel angry about fatigue. | 0 | 1 | 1 | 2 | 3 | 4 |
| 25. You have closed yourself to fatigue. | 0 | 1 | 1 | 2 | 3 | 4 |
| Variables | n | (%) | |
|---|---|---|---|
| Age (years) | 51.28 ± 4.64 | ||
| Body mass index (kg/m2) | 23.07 ± 3.04 | ||
| Marital status | Single | 26 | (11.8) |
| Married | 167 | (75.9) | |
| Divorced | 18 | (8.2) | |
| Widowed | 9 | (4.1) | |
| Education | Elementary school or below | 4 | (1.9) |
| Junior high school | 4 | (1.8) | |
| Senior high school | 60 | (27.3) | |
| College or university | 115 | (52.3) | |
| Graduate school or above | 37 | (16.8) | |
| Career | No paid salary | 43 | (19.6) |
| With paid salary | 176 | (80.4) | |
| Family type | Nuclear family | 178 | (81.3) |
| Stem family | 35 | (16.0) | |
| Extended family | 6 | (2.7) | |
| None | 212 | (96.4) | |
| Yes | 8 | (3.6) | |
| Menstruation status * | Perimenopause | 99 | (45.0) |
| Menopause | 111 | (55.0) | |
| Regular exercise ** | None | 141 | (64.1) |
| Yes | 79 | (35.9) | |
| Chronic disease | None | 167 | (75.9) |
| Hypertension | 25 | (11.4) | |
| Diabetes | 13 | (5.9) | |
| Renal disease | 1 | (0.5) | |
| Other | 20 | (9.1) |
| (Yes) | 25% | 50% | 75% | 100% | M | |
|---|---|---|---|---|---|---|
| Items in the Perimenopausal Fatigue Self-Management Scale | n (%) | n (%) | n (%) | n (%) | n (%) | (SD) |
| Strive for maintaining work energy and efficiency | ||||||
| 173 (78.6) | 40 (23.1) | 68 (39.3) | 50 (28.9) | 15 (8.7) | 2.2 (0.9) |
| 168 (76.4) | 39 (23.2) | 64 (38.1) | 47 (28.0) | 18 (10.7) | 2.3 (0.9) |
| 116 (52.7) | 41 (35.3) | 33 (28.4) | 38 (32.8) | 4 (3.4) | 2.0 (0.9) |
| 114 (51.8) | 46 (40.4) | 42 (36.8) | 18 (15.8) | 8 (7.0) | 1.9 (0.9) |
| 102 (46.4) | 49 (48.0) | 33 (32.4) | 17 (16.7) | 3 (2.9) | 1.8 (0.8) |
| Seek self-help from medical resources | ||||||
| 67 (30.5) | 25 (37.3) | 27 (40.3) | 12 (17.9) | 3 (4.5) | 1.9 (0.9) |
| 29 (13.2) | 11 (37.9) | 10 (34.5) | 5 (17.2) | 3 (10.3) | 2.0 (1.0) |
| 32 (14.5) | 11 (34.4) | 14 (43.8) | 4 (12.5) | 3 (9.4) | 2.0 (0.9) |
| 106 (48.2) | 45 (42.5) | 38 (35.8) | 21 (19.8) | 2 (1.9) | 1.8 (0.8) |
| Strive to maintain the normal operation of the family | ||||||
| 146 (66.4) | 43 (59.5) | 48 (32.9) | 40 (27.4) | 15 (10.3) | 2.2 (1.0) |
| 117 (53.2) | 39 (33.3) | 38 (32.5) | 31 (26.5) | 9 (7.7) | 2.1 (1.0) |
| 172 (78.2) | 40 (23.3) | 60 (34.9) | 58 (33.7) | 14 (8.1) | 2.3 (0.9) |
| Make time for activities or exercise in busy life | ||||||
| 128 (58.2) | 24 (18.8) | 48 (37.5) | 42 (32.8) | 14 (10.9) | 2.4 (0.9) |
| 151 (68.6) | 55 (36.4) | 49 (32.5) | 4 (28.5) | 4 (2.6) | 2.0 (0.9) |
| 166 (75.5) | 39 (23.5) | 52 (31.3) | 49 (29.5) | 26 (15.7) | 2.4 (1.0) |
| 182 (82.7) | 38 (20.9) | 61 (33.5) | 52 (28.6) | 31 (17.0) | 2.4 (1.0) |
| 96 (43.6) | 27 (28.1) | 33 (34.4) | 25 (26.0) | 11 (11.5) | 2.2 (1.0) |
| Slow down or adjust lifestyle | ||||||
| 182 (82.7) | 59 (32.4) | 71 (39.0) | 38 (20.9) | 14 (7.7) | 2.0 (0.9) |
| 185 (84.1) | 63 (34.1) | 67 (36.2) | 48 (25.9) | 7 (3.8) | 2.0 (0.9) |
| 197 (89.5) | 63 (32.0) | 74 (37.6) | 47 (23.9) | 13 (6.6) | 2.1 (0.9) |
| 178 (80.9) | 49 (27.5) | 70 (39.3) | 48 (27.0) | 11 (6.2) | 2.1 (0.9) |
| 165 (75.0) | 53 (32.1) | 68 (41.2) | 34 (20.6) | 10 (6.1) | 2.0 (0.9) |
| Frustration | ||||||
| 82 (37.3) | 41 (50.0) | 28 (34.1) | 10 (12.2) | 3 (3.7) | 1.7 (0.8) |
| 72 (32.7) | 38 (52.8) | 22 (30.6) | 11 (15.3) | 1 (1.4) | 1.7 (0.8) |
| 54 (24.5) | 28 (51.9) | 16 (29.6) | 9 (16.7) | 1 (1.9) | 1.7 (0.8) |
| Item | Person Class | Person Class | DIF Contrast | DIF SE | Rush–Welch | |
|---|---|---|---|---|---|---|
| t | p-Value | |||||
| m1 | Perimenopause | Menopause | −0.18 | 0.12 | −1.44 | 0.1509 |
| m2 | Perimenopause | Menopause | 0.10 | 0.12 | 0.84 | 0.4022 |
| m3 | Perimenopause | Menopause | 0.11 | 0.13 | 0.81 | 0.4178 |
| m4 | Perimenopause | Menopause | 0.07 | 0.14 | 0.49 | 0.6233 |
| m5 | Perimenopause | Menopause | 0.27 | 0.15 | 1.82 | 0.0704 |
| m6 | Perimenopause | Menopause | 0 | 0.17 | 0 | 1.0000 |
| m7 | Perimenopause | Menopause | 0.51 | 0.26 | 1.95 | 0.0527 |
| m8 | Perimenopause | Menopause | 0.42 | 0.25 | 1.71 | 0.0898 |
| m9 | Perimenopause | Menopause | −0.19 | 0.14 | −1.33 | 0.1847 |
| m10 | Perimenopause | Menopause | −0.13 | 0.13 | −1 | 0.3192 |
| m11 | Perimenopause | Menopause | 0.11 | 0.13 | 0.82 | 0.4112 |
| m12 | Perimenopause | Menopause | −0.15 | 0.12 | −1.22 | 0.2254 |
| m13 | Perimenopause | Menopause | 0 | 0.13 | 0 | 1.000 |
| m14 | Perimenopause | Menopause | −0.07 | 0.13 | −0.56 | 0.573 |
| m15 | Perimenopause | Menopause | 0.19 | 0.12 | 1.51 | 0.132 |
| m16 | Perimenopause | Menopause | 0.05 | 0.13 | 0.38 | 0.705 |
| m17 | Perimenopause | Menopause | 0.19 | 0.14 | 1.35 | 0.1787 |
| m18 | Perimenopause | Menopause | 0.07 | 0.12 | 0.58 | 0.5622 |
| m19 | Perimenopause | Menopause | −0.18 | 0.12 | −1.41 | 0.1609 |
| m20 | Perimenopause | Menopause | 0 | 0.12 | 0 | 1.000 |
| m21 | Perimenopause | Menopause | −0.15 | 0.12 | −1.2 | 0.2298 |
| m22 | Perimenopause | Menopause | −0.07 | 0.13 | −0.56 | 0.5728 |
| m23 | Perimenopause | Menopause | −0.02 | 0.16 | −0.13 | 0.9002 |
| m24 | Perimenopause | Menopause | −0.13 | 0.17 | −0.74 | 0.463 |
| m25 | Perimenopause | Menopause | −0.18 | 0.19 | −0.95 | 0.3418 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiu, H.-H.; Tsao, L.-I.; Liu, C.-Y.; Lu, Y.-Y.; Shih, W.-M.; Wang, P.-H. The Perimenopausal Fatigue Self-Management Scale Is Suitable for Evaluating Perimenopausal Taiwanese Women’s Vulnerability to Fatigue Syndrome. Healthcare 2021, 9, 336. https://doi.org/10.3390/healthcare9030336
Chiu H-H, Tsao L-I, Liu C-Y, Lu Y-Y, Shih W-M, Wang P-H. The Perimenopausal Fatigue Self-Management Scale Is Suitable for Evaluating Perimenopausal Taiwanese Women’s Vulnerability to Fatigue Syndrome. Healthcare. 2021; 9(3):336. https://doi.org/10.3390/healthcare9030336
Chicago/Turabian StyleChiu, Hsiao-Hui, Lee-Ing Tsao, Chieh-Yu Liu, Yu-Ying Lu, Whei-Mei Shih, and Peng-Hui Wang. 2021. "The Perimenopausal Fatigue Self-Management Scale Is Suitable for Evaluating Perimenopausal Taiwanese Women’s Vulnerability to Fatigue Syndrome" Healthcare 9, no. 3: 336. https://doi.org/10.3390/healthcare9030336