
Personalized Diet in Obesity: A Quasi-Experimental Study on Fat Mass and Fat-Free Mass Changes

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. First Consultation
2.3. Second Consultation
- A 7-day menu [38] (pp. 145–147). Details about it are displayed in Section 2.3.1.
- Recommendations to initiate the method: cooking time of food; quantity of food with the use of food scrapers and ladles to make a single meal in the family home, recommending the weighing of meat, fish, and potatoes; advice on the use of oil or other fats for the consumption of raw or cooked foods; encouraging the consumption of vegetables and fruits; time between meals of around three hours [38] (pp. 148–150).
- Food equivalents/substitution table, which is a document in which foods are presented in groups that are interchangeable among themselves because they are equivalent in size or weight, in addition, they have a similar nutritional composition.
- A food survey to record intake, if they were unable to take a meal on any of the days, and the alternative option decided upon [38,39] (p. 137). In this document, the dietary intake was recorded for 7 days of the week and 5 meals of the day (breakfast, morning snack, lunch, afternoon snack, and dinner). It was asked what was consumed and the amount, the type of liquid consumed at these meals (water, soft drinks, juices, alcoholic beverages, etc.), and whether these meals were eaten alone or in company.
2.3.1. Personalized Diet
2.4. Third and Subsequent Consultations
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Subjects
3.2. Changes in Body Composition
3.3. Odds Ratio Analysis
4. Discussion
- ✓
- ✓
- In Spain, there is a need to improve eating habits, due to deviation in caloric profile and in macronutrients in adults [7]. The use of personalized diet will help to improve adherence to interventions, and behavioral support will help to remove barriers that limit lifestyle changes in overweight subjects [8,9,10,11].
- ✓
- The monitoring of body composition changes and realistic planning of body weight changes are an important part of follow-up in an intervention in overweight subjects [13,14,15]. Given that clinical change in fat mass is an underexplored area, the concept of clinically significant body weight change is extrapolated in this study [8,16,17,18,19,20,21,22,23]. In the analysis of fat-free mass changes, its decrease was considered as a non-recommendable change due to contributing to the prognosis of metabolic syndrome [29,30]. The analysis of fat and fat-free mass index provides added information to the fat and fat-free mass data; therefore, they are variables that should be used in interventions of this type [31,32] (p. 381).
- ✓
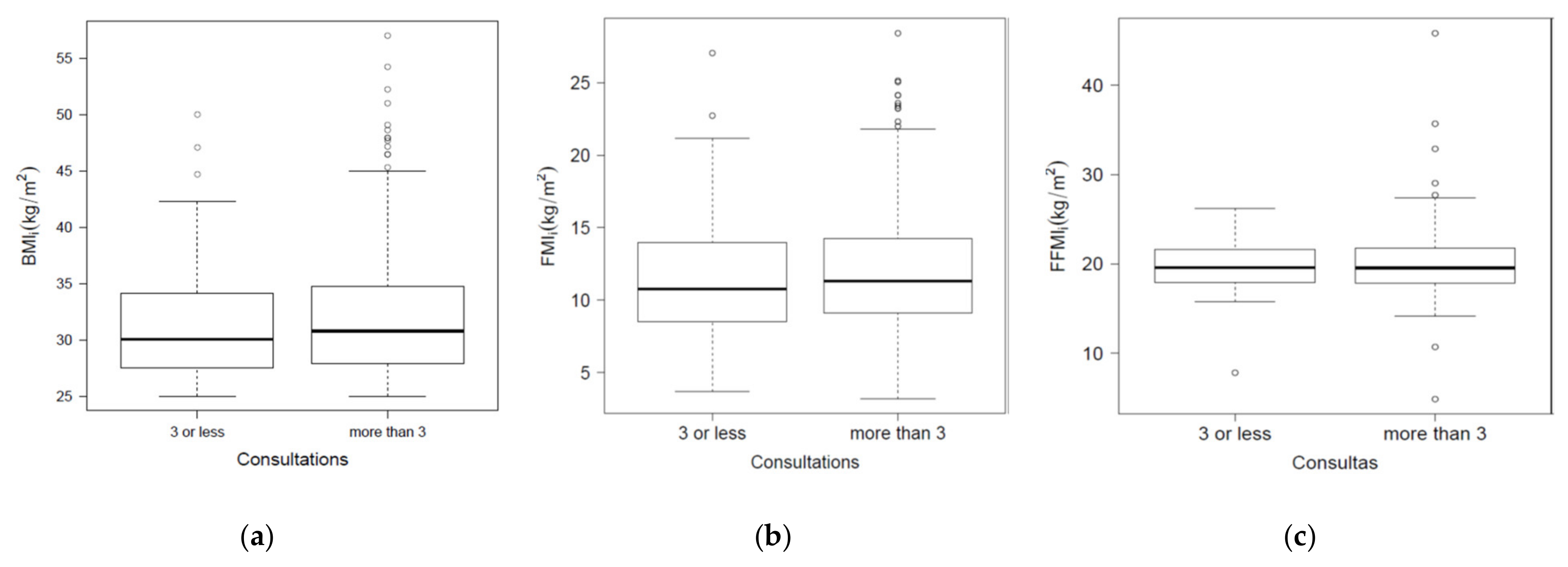
- The main differences between the study presented here and those related to it that are previously reported are the following [37,45,47]: the bioimpedance measurement protocol was included; this is the first time that the analysis was carried out according to the groups attending the consultation (Table 1, Table 2 and Table 3); a comparison was made by different age groups and subjects ≤ 25 years were evaluated; two groups of subjects were designed according to the FFM variable (Table 1 and Table 3); to date, no studies of this type have been found in Spain, where the following variables are analyzed (Table 2 and Figure 1a–c): FMI, FFMI, FMIf–i, and FFMIf–i.
- i.
- Fat and fat-free mass analysis: their indices will provide greater accuracy for diagnosis in early consultations versus BMI (Figure 1a–c).
- ii.
- Monitoring body composition changes: fat mass and fat-free mass should be recorded (Table 2), then some options should be proposed to improve adherence to the diet and obtain clinically significant changes in fat mass and recommended fat-free mass (Table 1 and Table 3):
- a.
- Promote attendance to the dietitian’s office for a period of ≥6 weeks, especially in men and those over 65 years of age with overweight and obesity (Table 1).
- b.
- Being part of a dynamic learning process divided into several periods will enable the subject to know where he/she currently stands in the intervention (initiation, improvement, and maintenance).
- c.
- Use of a hypocaloric and balanced diet: with an energy restriction of 500–1000 Kcal × day−1; an intake of 45–55% carbohydrates, 25–35% total fat, and 15–25% protein.
- d.
- The complementary recommendations used will allow the subject to know how to incorporate the indicated changes in his/her day-to-day life.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Tzanetakou, I.P.; Katsilambros, N.L.; Benetos, A.; Mikhailidis, D.P.; Perrea, D.N. “Is obesity linked to aging?”: Adipose tissue and the role of telomeres. Ageing Res. Rev. 2012, 11, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Frasca, D.; Blomberg, B.B.; Paganelli, R. Aging, Obesity, and Inflammatory Age-Related Diseases. Front Immunol. 2017, 8, 1745. [Google Scholar] [CrossRef]
- NCD Risk Factor Collaboration (NCD-RisC). Trends in adult body-mass index in 200 countries from 1975 to 2014: A pooled analysis of 1698 population-based measurement studies with 19.2 million participants. Lancet 2016, 387, 1377–1396. [Google Scholar] [CrossRef] [Green Version]
- Ministerio de Sanidad, Consumo y Bienestar Social. Encuesta Nacional de Salud. España 2018. Available online: https://www.mscbs.gob.es/estadEstudios/estadisticas/encuestaNacional/encuestaNac2017/ENSE2017_notatecnica.pdf (accessed on 1 July 2021).
- Ministerio de Sanidad, Servicios Sociales e Igualdad y el Instituto Nacional de Estadística. Encuesta Nacional de Salud de España (ENSE), Metodología. 2017. Available online: https://www.mscbs.gob.es/estadEstudios/estadisticas/encuestaNacional/encuestaNac2017/ENSE17_Metodologia.pdf (accessed on 1 July 2021).
- Hernáez, Á.; Zomeño, M.D.; Dégano, I.R.; Pérez-Fernández, S.; Goday, A.; Vila, J.; Civeira, F.; Moure, R.; Marrugat, J. Excess Weight in Spain: Current Situation, Projections for 2030, and Estimated Direct Extra Cost for the Spanish Health System. Rev. Esp. Cardiol. 2019, 72, 916–924, (In English, Spanish). [Google Scholar] [CrossRef]
- Agencia Española de Alimentación y Nutrición. Encuesta ENALIA 2. Encuesta Nacional de Alimentación en Población Adulta, Mayores y Embarazadas. 2016. Available online: https://www.aesan.gob.es/AECOSAN/web/seguridad_alimentaria/subdetalle/enalia_2.htm#4 (accessed on 8 May 2021).
- Bray, G.A.; Heisel, W.E.; Afshin, A.; Jensen, M.D.; Dietz, W.H.; Long, M.; Kushner, R.F.; Daniels, S.R.; Wadden, T.A.; Tsai, A.G.; et al. The Science of Obesity Management: An Endocrine Society Scientific Statement. Endocr. Rev. 2018, 39, 79–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Horn, L. A diet by any other name is still about energy. JAMA 2014, 312, 900–901. [Google Scholar] [CrossRef] [PubMed]
- Garvey, W.T.; Mechanick, J.I.; Brett, E.M.; Garber, A.J.; Hurley, D.L.; Jastreboff, A.M.; Nadolsky, K.; Pessah-Pollack, R.; Plodkowski, R. American Association of Clinical Endocrinologist and American College of Endocrinology comprehensive Clinical Practice Guidelines for Medical Care of Patients with obesity. Endocr. Pract. 2016, 22, 1–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacLean, P.S.; Wing, R.R.; Davidson, T.; Epstein, L.; Goodpaster, B.; Hall, K.D.; Levin, B.E.; Perri, M.G.; Rolls, B.J.; Rosenbaum, M.; et al. NIH working group report: Innovative research to improve maintenance of weight loss. Obesity 2015, 23, 7–15. [Google Scholar] [CrossRef]
- Munt, A.E.; Partridge, S.R.; Allman-Farinelli, M. The barriers and enablers of healthy eating among young adults: A missing piece of the obesity puzzle: A scoping review. Obes. Rev. 2017, 8, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Albert Pérez, E.; Poveda González, M.; Martínez-Espinosa, R.M.; Molina Vila, M.D.; Reig García-Galbis, M. Practical Guidance for Interventions in Adults with Metabolic Syndrome: Diet and Exercise vs. Changes in Body Composition. Int. J. Environ. Res. Public Health 2019, 16, 3481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burgess, E.; Hassmén, P.; Pumpa, K.L. Determinants of adherence to lifestyle intervention in adults with obesity: A systematic review. Clin. Obes. 2017, 7, 123–135. [Google Scholar] [CrossRef] [PubMed]
- Yackobovitch-Gavan, M.; Steinberg, D.M.; Endevelt, R.; Benyamini, Y. Factors associated with dropout in a group weight-loss programme: A longitudinal investigation. J. Hum. Nutr. Diet. 2015, 28, 33–40. [Google Scholar] [CrossRef]
- Ryan, D.; Heaner, M. Guidelines (2013) for managing overweight and obesity in adults: Preface to the full report. Obesity 2014, 22, S1–S3. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, J.; Whybrow, S.; Teixeira, P.; Blundell, J.; Lawton, C.; Westenhoefer, J.; Engel, D.; Shepherd, R.; McConnon, A.; Gilbert, P.; et al. Problems in identifying predictors and correlates of weight loss and maintenance: Implications for weight control therapies based on behaviour change. Obes. Rev. 2011, 12, 688–708. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. 4. Lifestyle Management. Diabetes Care 2017, 40, 33–43. [Google Scholar] [CrossRef] [Green Version]
- Yumuk, V.; Tsigos, C.; Fried, M.; Schindler, K.; Busetto, L.; Micic, D.; Toplak, H. European Guidelines for Obesity Management in Adults. Obes. Facts 2015, 8, 402–424. [Google Scholar] [CrossRef]
- Jensen, M.D.; Ryan, D.H. 2013 AHA/ACC/TOS Guideline for the management of overweight and obesity in adults. J. Am. Coll. Cardiol. 2014, 63, 2994–3000. [Google Scholar] [CrossRef] [Green Version]
- Obesity: Preventing and Managing the Global Epidemic. Report of a WHO Consultation (WHO Technical Report Series 894). Available online: https://apps.who.int/iris/handle/10665/42330?locale-attribute=es& (accessed on 4 May 2021).
- Brown, T.J.; O’Malley, C.; Blackshaw, J.; Coulton, V.; Tedstone, A.; Summerbell, C.; Ells, L.J. Exploring the evidence base for Tier 3 weight management interventions for adults: A systematic review. Clin. Obes. 2017, 7, 260–272. [Google Scholar] [CrossRef] [Green Version]
- Look AHEAD Research Group. Eight-year weight losses with an intensive lifestyle intervention: The look AHEAD study. Obesity 2014, 22, 5–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cava, E.; Yeat, N.C.; Mittendorfer, B. Preserving Healthy Muscle during Weight Loss. Adv. Nutr. 2017, 8, 511–519. [Google Scholar] [CrossRef] [Green Version]
- Batsis, J.A.; Villareal, D.T. Sarcopenic obesity in older adults: Aetiology, epidemiology and treatment strategies. Nat. Rev. Endocrinol. 2018, 14, 513–537. [Google Scholar] [CrossRef]
- Armani, A.; Berry, A.; Cirulli, F.; Caprio, M. Molecular mechanisms underlying metabolic syndrome: The expanding role of the adipocyte. FASEB J. 2017, 31, 4240–4255. [Google Scholar] [CrossRef]
- Pi-Sunyer, X. Changes in body composition and metabolic disease risk. Eur. J. Clin. Nutr. 2019, 73, 231–235. [Google Scholar] [CrossRef]
- Mechanick, J.I.; Hurley, D.L.; Garvey, W.T. Adiposity-based chronic disease as a new diagnostic term: The American Association of Clinical Endocrinologists and American College of Endocrinology Position Statement. Endocr. Pract. 2017, 23, 372–378. [Google Scholar] [CrossRef] [Green Version]
- Zibellini, J.; Seimon, R.V.; Lee, C.M.; Gibson, A.A.; Hsu, M.S.; Sainsbury, A. Effect of diet-induced weight loss on muscle strength in adults with overweight or obesity—A systematic review and meta-analysis of clinical trials. Obes. Rev. 2016, 17, 647–663. [Google Scholar] [CrossRef]
- Bosy-Westphal, A.; Müller, M.J. Identification of skeletal muscle mass depletion across age and BMI groups in health and disease—There is need for a unified definition. Int. J. Obes. 2015, 39, 379–386. [Google Scholar] [CrossRef] [PubMed]
- Pourshahidi, L.K.; Wallace, J.M.; Mulhern, M.S.; Horigan, G.; Strain, J.J.; McSorley, E.M.; Magee, P.J.; Bonham, M.P.; Livingstone, M.B. Indices of adiposity as predictors of cardiometabolic risk and inflammation in young adults. J. Hum. Nutr. Diet 2016, 29, 26–37. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.; Ma, F.; Lou, H.; Liu, Y. The utility of fat mass index vs. body mass index and percentage of body fat in the screening of metabolic syndrome. BMC Public Health 2013, 13, 629. [Google Scholar] [CrossRef] [Green Version]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The International Committee of Biomedical Journal Editors (ICMJE). Recommendations for the Preparation, Presentation, Editing and Publication of Academic Papers in Medical Journal. 2017. Available online: http://www.icmje.org/icmje-recommendations.pdf (accessed on 1 July 2021).
- Ruiz, E.; Ávila, J.M.; Valero, T.; Del Pozo, S.; Rodriguez, P.; Aranceta-Bartrina, J.; Gil, A.; González-Gross, M.; Ortega, R.M.; Serra-Majem, L.; et al. Macronutrient Distribution and Dietary Sources in the Spanish Population: Findings from the ANIBES Study. Nutrients 2016, 8, 177. [Google Scholar] [CrossRef]
- Salas-Salvadó, J.; Rubio, M.A.; Barbany, M.; Moreno, B.; Grupo Colaborativo de la SEEDO. SEEDO 2007 Consensus for the evaluation of overweight and obesity and the establishment of therapeutic intervention criteria. Med. Clin. 2007, 128, 184–200. [Google Scholar] [CrossRef]
- Reig García-Galbis, M. The management of qualitative and quantitative dietary treatment for overweight and obesity: Methodology and a new perspective on individualised assessment. Nutr. Hosp. 2015, 32, 2019–2029. [Google Scholar] [CrossRef] [Green Version]
- Reig García-Galbis, M. La Eficacia de Una Educación Nutricional Como Método en la Pérdida de Peso. Ph.D. Thesis, Universidad de Alicante, Alicante, Spain, 2013. Available online: https://rua.ua.es/dspace/bitstream/10045/28416/1/Tesis_Reig_Garcia-Galbis.pdf (accessed on 30 May 2021).
- Rizo Baeza, M.M. Hábitos nutricionales de Los Escolares y Adolescentes de la Comarca del Alacanti. Ph.D. Thesis, Universidad de Alicante, Alicante, Spain, 2003. [Google Scholar]
- Madden, A.M.; Smith, S. Body composition and morphological assessment of nutritional status in adults: A review of anthropometric variables. J. Hum. Nutr. Diet. 2016, 29, 7–25. [Google Scholar] [CrossRef] [PubMed]
- Müller, M.J.; Braun, W.; Pourhassan, M.; Geisler, C.; Bosy-Westphal, A. Application of standards and models in body composition analysis. Proc. Nutr. Soc. 2016, 75, 181–187. [Google Scholar] [CrossRef] [Green Version]
- Hume, P.; Marfell-Jones, M. The importance of accurate site location for skinfold measurement. J. Sports Sci. 2008, 26, 1333–1340. [Google Scholar] [CrossRef] [PubMed]
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gómez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.-C.; Pirlich, M.; et al. Bioelectrical impedance analysis-part II: Utilization in clinical practice. Clin. Nutr. 2004, 23, 1430–1453. [Google Scholar] [CrossRef] [PubMed]
- Pancorbo, A.E.; Pancorbo, E.L. Actividad Física en la Prevención Y Tratamiento de la Enfermedad Cardiometabólica. La Dosis de Ejercicio Cardiosaludable. 2011, pp. 165–194. Available online: https://fundadeps.org/recursos/Actividad-fisica-en-la-prevencion-y-tratamiento-de-la-enfermedad-cardiometabolica-La-dosis-de-ejercicio-cardiosaludable/ (accessed on 30 May 2021).
- Reig García-Galbis, M.; Rizo Baeza, M.; Cortés Castell, E. Indicators of success in the dietary management of overweight and obesity: Weight, body fat loss and quality. Nutr. Hosp. 2015, 32, 1009–1016. [Google Scholar] [CrossRef] [Green Version]
- Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.r-project.org/ (accessed on 30 May 2021).
- Reig García-Galbis, M.; Cortés Castell, E.; Rizo Baeza, M.; Gutiérrez Hervás, A. The variability in adherence to dietary treatment and quality of weight loss: Overweight and obesity. Nutr. Hosp. 2015, 31, 2020–2027. [Google Scholar] [CrossRef] [Green Version]
- Larsen, T.M.; Dalskov, S.; van Baak, M.; Jebb, S.; Kafatos, A.; Pfeiffer, A.; Martinez, J.A.; Handjieva-Darlenska, T.; Kuneå¡ovã¡, M.; Holst, C.; et al. The Diet, Obesity and Genes (Diogenes) Dietary Study in eight European countries—A comprehensive design for long-term intervention. Obes. Rev. 2010, 11, 76–91. [Google Scholar] [CrossRef] [PubMed]
- Frühbeck, G.; Busetto, L.; Dicker, D.; Yumuk, V.; Goossens, G.H.; Hebebrand, J.; Halford, J.G.C.; Farpour-Lambert, N.J.; Blaak, E.E.; Woodward, E.; et al. The ABCD of Obesity: An EASO Position Statement on a Diagnostic Term with Clinical and Scientific Implications. Obes. Facts 2019, 12, 131–136. [Google Scholar] [CrossRef]
- Varkevisser, R.D.M.; van Stralen, M.M.; Kroeze, W.; Ket, J.C.F.; Steenhuis, I.H.M. Determinants of weight loss maintenance: A systematic review. Obes. Rev. 2019, 20, 171–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnston, B.C.; Kanters, S.; Bandayrel, K.; Wu, P.; Naji, F.; Siemieniuk, R.A.; Ball, G.D.; Busse, J.W.; Thorlund, K.; Guyatt, G.; et al. Comparison of weight loss among named diet programs in overweight and obese adults: A meta-analysis. JAMA 2014, 312, 923–933. [Google Scholar] [CrossRef] [PubMed]
- Jäger, R.; Kerksick, C.M.; Campbell, B.I.; Cribb, P.J.; Wells, S.D.; Skwiat, T.M.; Purpura, M.; Ziegenfuss, T.N.; Ferrando, A.A.; Arent, S.M.; et al. International Society of Sports Nutrition Position Stand: Protein and exercise. J. Int. Soc. Sports Nutr. 2017, 14, 20. [Google Scholar] [CrossRef] [Green Version]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef]
- De Toro-Martín, J.; Arsenault, B.J.; Després, J.P.; Vohl, M.C. Precision Nutrition: A Review of Personalized Nutritional Approaches for the Prevention and Management of Metabolic Syndrome. Nutrients 2017, 9, 913. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Categories | Subcategories | Participants n (%) | ≤3 Consultation Attendance (n: 121) | Attendance to >3 Consultations (n: 470) |
|---|---|---|---|---|
| Sex | Male | 188 (32%) | 44 (36%) | 144 (31%) |
| Female | 403 (68%) | 77 (64%) | 326 (69%) | |
| Age | 19–64 years old | 553 (94%) | 116 (96%) | 437 (93%) |
| ≥65 years old | 38 (6%) | 5 (4%) | 33 (7%) | |
| BMI | Obesity | 330 (56%) | 59 (49%) | 272 (58%) |
| Overweight | 261 (44%) | 62 (51%) | 199 (42%) | |
| Clinically significant changes | Change ≥ 5% in body weight and fat mass | 313 (53%) | 15 (12%) | 298 (63%) |
| Change < 5% in body weight and ≥5% fat mass | 156 (26%) | 41 (34%) | 115 (24%) | |
| Clinically non-significant changes | Change ≥ 5% in body weight and <5% fat mass | 11 (2%) | 1 (1%) | 10 (2%) |
| <5% change in body weight and fat mass | 111 (19%) | 64 (53%) | 47 (10%) | |
| Recommended changes | Change in FFM ≥ 0% | 530 (90%) | 97 (80%) | 433 (92%) |
| Not-recommended changes | FFM change < 0% | 61 (10%) | 24 (20%) | 37 (8%) |
| Parameters | Min | Med | Max | Mean (SD) (n: 591) | ≤3 Consultation Attendance (n: 121) | Attendance to >3 Consultations (n: 470) | KW Statistic (p-Value) |
|---|---|---|---|---|---|---|---|
| Age (years old) | 19 | 42 | 86 | 43.43 (13.96) | 40.74 (14.38) | 44.12 (13.78) | −2.321 (0.021) |
| BMIi (kg/m2) | 25 | 30.67 | 57.01 | 31.75 (5.24) | 31.28 (5.01) | 31.88 (5.29) | −1.166 (0.245) |
| BWi (kg) | 58.6 | 83.6 | 166.7 | 85.38 (15.87) | 84.67 (13.82) | 85.56 (16.37) | −0.612 (0.541) |
| FMi (kg) | 8.9 | 29.7 | 74.8 | 31.22 (9.98) | 30.29 (9.97) | 31.46 (9.97) | −1.155 (0.249) |
| (%) | 12.36 | 37.19 | 82.93 | 36.4 (8.28) | 35.64 (9.21) | 36.59 (8.02) | −1.045 (0.298) |
| FMIi (kg/m2) | 3.19 | 11.13 | 28.42 | 11.76 (4.03) | 11.4 (4.29) | 11.85 (3.95) | −1.046 (0.297) |
| FFMi (kg) | 15.4 | 50 | 134 | 54.16 (11.89) | 54.38 (11.18) | 54.1 (12.07) | 0.239 (0.812) |
| (%) | 17.07 | 62.81 | 87.64 | 63.6 (8.28) | 64.36 (9.21) | 63.41 (8.02) | 1.045 (0.298) |
| FFMIi (kg/m2) | 4.86 | 19.59 | 45.83 | 20 (3.06) | 19.87 (2.7) | 20.03 (3.15) | −0.54 (0.59) |
| Number of consultations | 2 | 6 | 42 | 6.9 (4.42) | 2.6 (0.49) | 8.01 (4.31) | |
| BMIf–i (kg/m2) | −9.65 | −1.72 | 1.84 | −2.05 (1.62) | −0.73 (0.69) | −2.39 (1.62) | 16.959 (<0.001) |
| BWf–i (kg) | −32.4 | − 4.6 | 4.9 | −5.53 (4.51) | −1.93 (1.78) | −6.45 (4.53) | 17.112 (<0.001) |
| (%) | −29.81 | −5.59 | 4.91 | −6.42 (4.79) | −2.35 (2.14) | −7.46 (4.73) | 17.475 (<0.001) |
| FMf–i (kg) | −25.1 | −3.9 | 1.9 | −4.76 (4.15) | −1.63 (1.71) | −5.56 (4.21) | 15.809 (<0.001) |
| (%) | −72.13 | −13.04 | 7.39 | −15.8 (13.1) | −6 (6.24) | −18.33 (13.22) | 14.806 (<0.001) |
| FMIf–i (kg/m2) | −8.58 | −1.46 | 0.72 | −1.75 (1.5) | −0.61 (0.64) | −2.05 (1.51) | 15.752 (<0.001) |
| FFMf–i (kg) | −9.8 | −0.8 | 17.2 | −0.77 (2.63) | −0.3 (1.56) | −0.89 (2.83) | 3.082 (0.002) |
| (%) | −3 | 2.7 | 23.97 | 3.5 (3.61) | 1.2 (1.73) | 4.1 (3.73) | −12.451 (<0.001) |
| FFMIf–i (kg/m2) | −3.96 | −0.3 | 6.47 | − 0.29 (0.95) | −0.12 (0.57) | − 0.33 (1.02) | 3.074 (0.002) |
| ≤3 Consultation Attendance vs. Attend to >3 Consultations | ||||
|---|---|---|---|---|
| Categories | Subcategories | OR | 95% CI | p |
| Sex | Male vs. female | 1.294 | 0.846–1.960 | 0.229 |
| Age | 19–64 years old vs. ≥65 years old | 1.752 | 0.729–5.205 | 0.254 |
| BMI | Overweight vs. obesity | 1.431 | 0.959–2.139 | 0.078 |
| Clinically significant changes vs. Clinically non-significant changes | Change ≥ 5% in body weight and fat mass vs. <5% change in body weight and fat mass | 27.052 | 14.611–52.979 | <0.0001 |
| Change < 5% in body weight and ≥5% fat mass vs. <5% change in body weight and fat mass | 3.819 | 2.287–6.463 | <0.0001 | |
| Comparison of clinically insignificant changes | Change ≥ 5% in body weight and <5% fat mass vs. <5% change in body weight and fat mass | 13.617 | 2.482–254.218 | 0.0143 |
| Not recommended changes vs. Recommended changes | FFM change < 0% vs. Change in FFM ≥ 0% | 2.896 | 1.640–5.03 | 0.0002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Galbis, M.R.; Gallardo, D.I.; Martínez-Espinosa, R.M.; Soto-Méndez, M.J. Personalized Diet in Obesity: A Quasi-Experimental Study on Fat Mass and Fat-Free Mass Changes. Healthcare 2021, 9, 1101. https://doi.org/10.3390/healthcare9091101
García-Galbis MR, Gallardo DI, Martínez-Espinosa RM, Soto-Méndez MJ. Personalized Diet in Obesity: A Quasi-Experimental Study on Fat Mass and Fat-Free Mass Changes. Healthcare. 2021; 9(9):1101. https://doi.org/10.3390/healthcare9091101
Chicago/Turabian StyleGarcía-Galbis, Manuel Reig, Diego I. Gallardo, Rosa María Martínez-Espinosa, and María José Soto-Méndez. 2021. "Personalized Diet in Obesity: A Quasi-Experimental Study on Fat Mass and Fat-Free Mass Changes" Healthcare 9, no. 9: 1101. https://doi.org/10.3390/healthcare9091101