
Effect of Indoor Temperature on Physical Performance in Older Adults during Days with Normal Temperature and Heat Waves

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects and Design
2.2. Assessment Protocol
2.3. Repetitive Assessments
2.3.1. Climate Condition
2.3.2. Physical Performance:
2.4. Descriptive Measures
2.5. Statistics
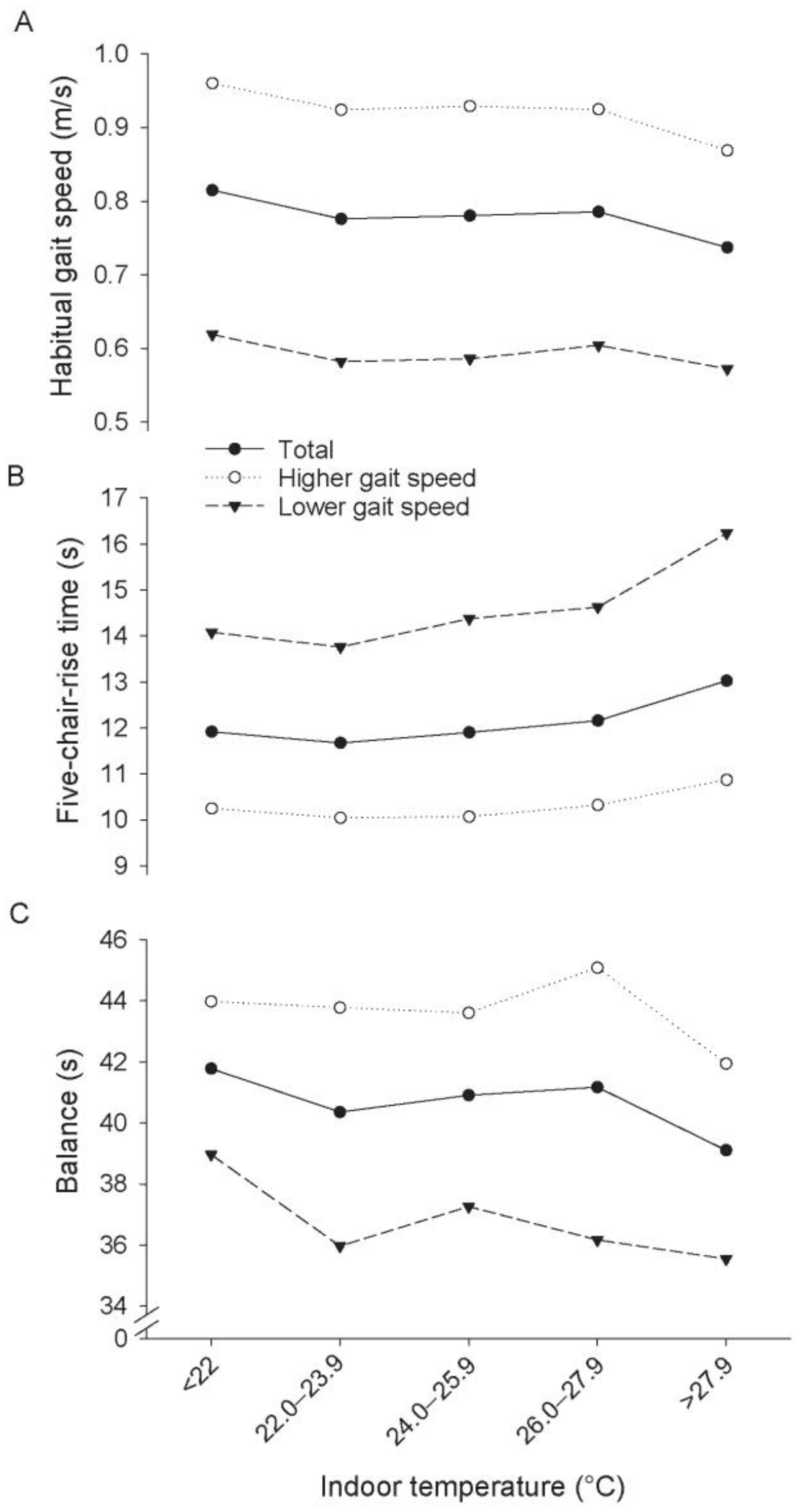
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Baccini, M.; Kosatsky, T.; Biggeri, A. Impact of summer heat on urban population mortality in Europe during the 1990s: An evaluation of years of life lost adjusted for harvesting. PLoS ONE 2013, 8, e69638. [Google Scholar] [CrossRef] [PubMed]
- Klenk, J.; Becker, C.; Rapp, K. Heat-related mortality in residents of nursing homes. Age Ageing 2010, 39, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, R.; Le Tertre, A.; Schwartz, J.; Gotway, C.A.; Daley, W.R.; Rubin, C.H. The effect of the 1995 heat wave in Chicago on all-cause and cause-specific mortality. Am. J. Public Health 2007, 97 (Suppl. 1), 158–162. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Sun, Q.; Zhou, X.; Li, X.; Yang, M.; Yu, A.; Geng, F. Heat wave impact on mortality in Pudong New Area, China in 2013. Sci. Total Environ. 2014, 493, 789–794. [Google Scholar] [CrossRef] [PubMed]
- Bunker, A.; Wildenhain, J.; Vandenbergh, A.; Henschke, N.; Rocklöv, J.; Hajat, S.; Sauerborn, R. Effects of Air Temperature on Climate-Sensitive Mortality and Morbidity Outcomes in the Elderly; a Systematic Review and Meta-analysis of Epidemiological Evidence. EBiolMedicine 2016, 6, 258–268. [Google Scholar] [CrossRef] [PubMed]
- Wardekker, J.A.; de Jong, A.; van Bree, L.; Turkenburg, W.C.; van der Sluijs, J.P. Health risks of climate change: An assessment of uncertainties and its implications for adaptation policies. Environ. Health 2012, 11, 67. [Google Scholar] [CrossRef] [PubMed]
- Van Loenhout, J.F.; le Grand, A.; Duijm, F.; Greven, F.; Vink, N.M.; Hoek, G.; Zuurbier, M. The effect of high indoor temperatures on self-perceived health of elderly persons. Environ. Res. 2015, 146, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Barnett, A.G.; Sans, S.; Salomaa, V.; Kuulasmaa, K.; Dobson, A.J.; WHO MONICA Project. The effect of temperature on systolic blood pressure. Blood Press. Monit. 2007, 12, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-M.; Kim, S.; Cheong, H.-K.; Ahn, B.; Choi, K. Effects of heat wave on body temperature and blood pressure in the poor and elderly. Environ. Health Toxicol. 2012, 27, e2012013. [Google Scholar] [CrossRef] [PubMed]
- Flouris, A.D.; Schlader, Z.J. Human behavioral thermoregulation during exercise in the heat. Scand. J. Med. Sci. Sports 2015, 25 (Suppl. 1), 52–64. [Google Scholar] [CrossRef] [PubMed]
- Galloway, S.D.; Maughan, R.J. Effects of ambient temperature on the capacity to perform prolonged cycle exercise in man. Med. Sci. Sports Exerc. 1997, 29, 1240–1249. [Google Scholar] [CrossRef] [PubMed]
- Maughan, R.J. Distance running in hot environments: A thermal challenge to the elite runner. Scand. J. Med. Sci. Sports 2010, 20 (Suppl. 3), 95–102. [Google Scholar] [CrossRef] [PubMed]
- Sawka, M.N.; Leon, L.R.; Montain, S.J.; Sonna, L.A. Integrated physiological mechanisms of exercise performance, adaptation, and maladaptation to heat stress. Compr. Physiol. 2011, 1, 1883–1928. [Google Scholar] [PubMed]
- Stotz, A.; Rapp, K.; Oksa, J.; Skelton, D.A.; Beyer, N.; Klenk, J.; Becker, C.; Lindemann, U. Effect of a brief heat exposure on blood pressure and physical performance of older women living in the community—A pilot-study. Int. J. Environ. Res. Public Health 2014, 11, 12623–12631. [Google Scholar] [CrossRef] [PubMed]
- Asmussen, E.; Boje, O. Body temperature and capacity for work. Acta Physiol. Scand. 1945, 10, 1–22. [Google Scholar] [CrossRef]
- Middleton, A.; Fulk, G.D.; Herter, T.M.; Beets, M.W.; Donley, J.; Fritz, S.L. Self-Selected and Maximal Walking Speeds Provide Greater Insight Into Fall Status Than Walking Speed Reserve Among Community-Dwelling Older Adults. Am. J. Phys. Med. Rehabil. 2016, 95, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Buatois, S.; Miljkovic, D.; Manckoundia, P.; Gueguen, R.; Miget, P.; Vançon, G.; Perrin, P.; Benetos, A. Five times sit to stand test is a predictor of recurrent falls in healthy community-living subjects aged 65 and older. J. Am. Geriatr. Soc. 2008, 56, 1575–1577. [Google Scholar] [CrossRef] [PubMed]
- Muir, S.W.; Berg, K.; Chesworth, B.; Klar, N.; Speechley, M. Quantifying the magnitude of risk for balance impairment on falls in community-dwelling older adults: A systematic review and meta-analysis. J. Clin. Epidemiol. 2010, 63, 389–406. [Google Scholar] [CrossRef] [PubMed]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef] [PubMed]
- Groll, D.L.; To, T.; Bombardier, C.; Wright, J.G. The development of a comorbidity index with physical function as the outcome. J. Clin. Epidemiol. 2005, 58, 595–602. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Schoon, Y.; Bongers, K.; Van Kempen, J.; Melis, R.; Olde Rikkert, M. Gait speed as a test for monitoring frailty in community-dwelling older people has the highest diagnostic value compared to step length and chair rise time. Eur. J. Phys. Rehabil. Med. 2014, 50, 693–701. [Google Scholar] [PubMed]
- Katzman, R.; Brown, T.; Fuld, P.; Peck, A.; Schechter, R.; Schimmel, H. Validation of a short Orientation-Memory-Concentration Test of cognitive impairment. Am. J. Psychiatry 1983, 140, 734–739. [Google Scholar] [PubMed]
- Klenk, J.; Buchele, G.; Rapp, K.; Franke, S.; Peter, R. Walking on sunshine: Effect of weather conditions on physical activity in older people. J. Epidemiol. Community Health 2012, 66, 474–476. [Google Scholar] [CrossRef] [PubMed]
- Gillespie, L.D.; Robertson, M.C.; Gillespie, W.J.; Sherrington, C.; Gates, S.; Clemson, L.M.; Lamb, S.E. Interventions for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2012, 9, CD007146. [Google Scholar]
- Tansey, E.A.; Johnson, C.D. Recent advances in thermoregulation. Adv. Physiol. Educ. 2015, 39, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Xu, Y.J.; Zhang, Y.H.; Yan, Q.H.; Song, X.L.; Xie, H.Y.; Luo, Y.; Rutherford, S.; Chu, C.; Lin, H.L.; et al. Associations between risk perception, spontaneous adaptation behavior to heat waves and heatstroke in Guangdong province, China. BMC Public Health 2013, 13, 913. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Habitual Gait Speed | |||
|---|---|---|---|
| Total (n = 81) | Low * (n = 35) | High * (n = 46) | |
| Female, n (%) | 68 (84) | 28 (80) | 40 (87) |
| Age (years), mean (SD) | 80.9 (6.53) | 81.6 (7.42) | 80.4 (5.79) |
| Body height (cm), mean (SD) | 158.7 (8.13) | 157.5 (8.85) | 159.5 (7.56) |
| Body Mass Index (kg/m2), mean (SD) | 27.9 (4.75) | 27.9 (4.16) | 28.0 (5.18) |
| SOMC score (0–28), mean (SD) | 3.51 (3.17) | 3.41 (2.46) | 3.58 (3.62) |
| Co-morbidity score (0–18), mean (SD) | 4.15 (2.33) | 5.18 (2.07) | 3.39 (2.25) |
| Respiratory diseases, n (%) ** | 16 (20) | 6 (17) | 10 (22) |
| Cardiovascular diseases, n (%) ** | 33 (41) | 19 (54) | 14 (30) |
| Drugs (n), mean (SD) | 4.85 (3.45) | 6.11 (3.50) | 3.89 (3.11) |
| Frailty score (0–5), mean (SD) | 1.37 (1.08) | 2.14 (0.94) | 0.78 (0.76) |
| Non-frail, n (%) | 18 (22) | 0 (0) | 18 (39) |
| Pre-frail, n (%) | 52 (64) | 25 (71) | 27 (59) |
| Frail, n (%) | 11 (14) | 10 (29) | 1 (2) |
| Habitual gait speed (m/s), mean (SD) | 0.76 (0.25) | 0.53 (0.12) | 0.92 (0.20) |
| Balance (s), mean (SD) | 40.5 (7.94) | 36.6 (8.25) | 43.2 (6.55) |
| Five-chair-rise time (s), mean (SD) | 11.3 (3.42) | 13.2 (3.54) | 10.1 (2.76) |
| Total number of measurements, n | 538 | 223 | 315 |
| Number of measurements during a heat wave, n | 111 | 45 | 66 |
| Physical Performance; Group of Participants | n/Obs | Mean Change of Functional Performance Per 10 °C Increase of Indoor Temperature with 95% CI † | Mean Difference of Functional Performance between Heatwaves and Normal Days * with 95% CI † |
|---|---|---|---|
| Gait speed (m/s); all adults | 81/537 | −0.074 (−0.113; −0.034) | −0.041 (−0.065; −0.018) |
| Gait speed (m/s); adults with initially higher gait speed | 46/315 | −0.087 (−0.136; −0.038) | −0.062 (−0.092; −0.032) |
| Gait speed (m/s); adults with initially lower gait speed | 35/222 | −0.044 (−0.109; 0.021) | −0.010 (−0.048; 0.027) |
| Chair-rise (s); all adults | 81/514 | 1.15 (0.58; 1.73) | 0.90 (0.55; 1.24) |
| Chair-rise (s); adults with initially higher gait speed | 46/313 | 0.67 (0.12; 1.23) | 0.57 (0.23; 0.90) |
| Chair-rise (s); adults with initially lower gait speed | 35/201 | 2.03 (0.79; 3.28) | 1.44 (0.72; 2.16) |
| Balance (s); all adults | 81/538 | −1.69 (−3.56; 0.182) | −1.11 (−2.24; 0.01) |
| Balance (s); adults with initially higher gait speed | 46/315 | −0.18 (−2.33; 1.98) | −0.93 (−2.27; 0.41) |
| Balance (s); adults with initially lower gait speed | 35/223 | −3.92 (−7.31; −0.52) | −1.36 (−3.33; 0.61) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lindemann, U.; Stotz, A.; Beyer, N.; Oksa, J.; Skelton, D.A.; Becker, C.; Rapp, K.; Klenk, J. Effect of Indoor Temperature on Physical Performance in Older Adults during Days with Normal Temperature and Heat Waves. Int. J. Environ. Res. Public Health 2017, 14, 186. https://doi.org/10.3390/ijerph14020186
Lindemann U, Stotz A, Beyer N, Oksa J, Skelton DA, Becker C, Rapp K, Klenk J. Effect of Indoor Temperature on Physical Performance in Older Adults during Days with Normal Temperature and Heat Waves. International Journal of Environmental Research and Public Health. 2017; 14(2):186. https://doi.org/10.3390/ijerph14020186
Chicago/Turabian StyleLindemann, Ulrich, Anja Stotz, Nina Beyer, Juha Oksa, Dawn A. Skelton, Clemens Becker, Kilian Rapp, and Jochen Klenk. 2017. "Effect of Indoor Temperature on Physical Performance in Older Adults during Days with Normal Temperature and Heat Waves" International Journal of Environmental Research and Public Health 14, no. 2: 186. https://doi.org/10.3390/ijerph14020186