Association between Serum 25-Hydroxy Vitamin D Levels and the Prevalence of Adult-Onset Asthma


Abstract
:1. Introduction
2. Materials and Methods
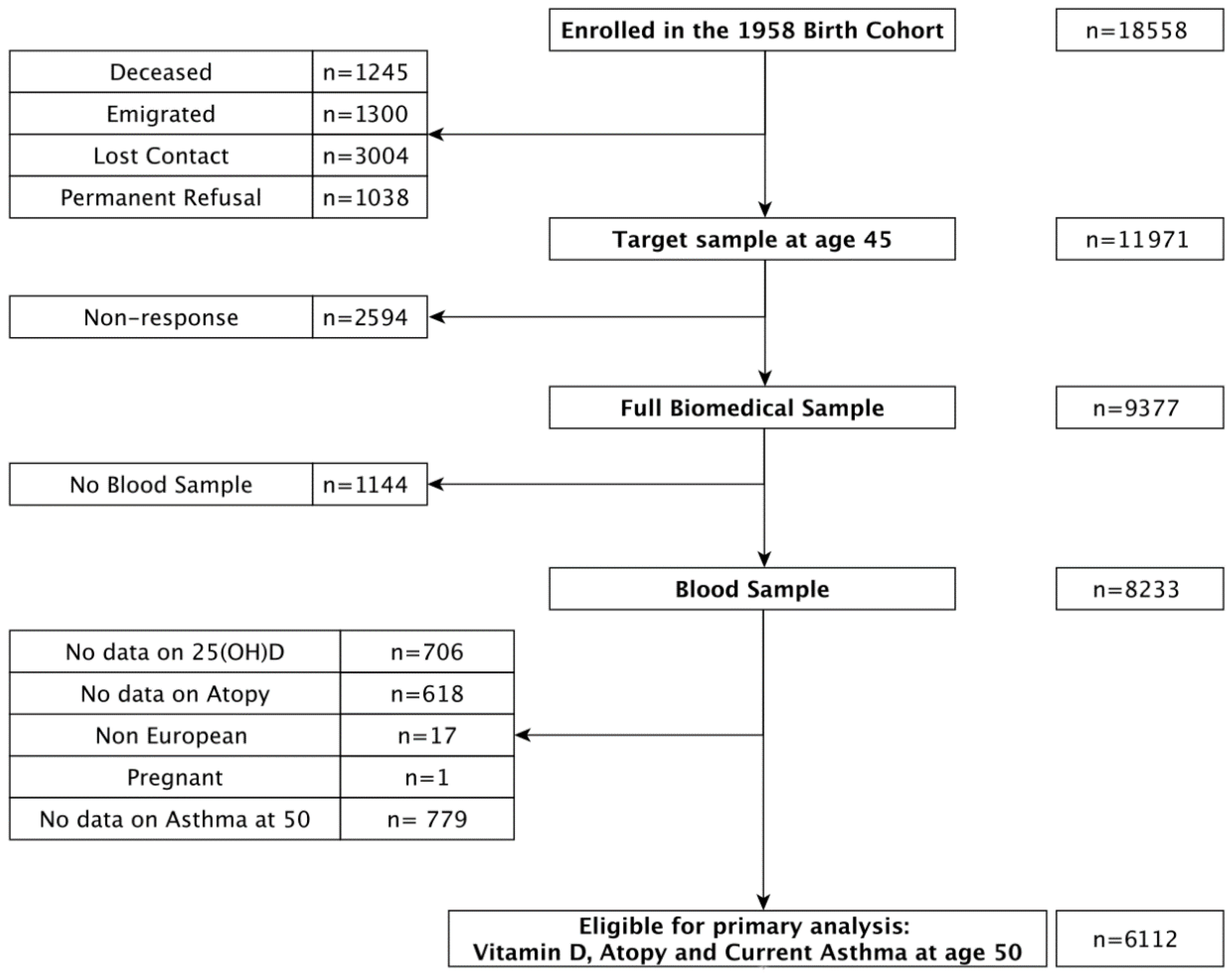
2.1. Subjects and Sample
2.2. Biomedical Data at Age 44/45
2.3. Self-Reported Data at Age 42
2.4. Self-Reported Data at Age 44/45
2.5. Self-Reported Asthma Data
2.6. Operationalisation of 25(OH)D Level and Status
2.7. Operationalisation of Atopy Score and Categories
2.8. Statistical Analysis
3. Results
3.1. Descriptive Statistics
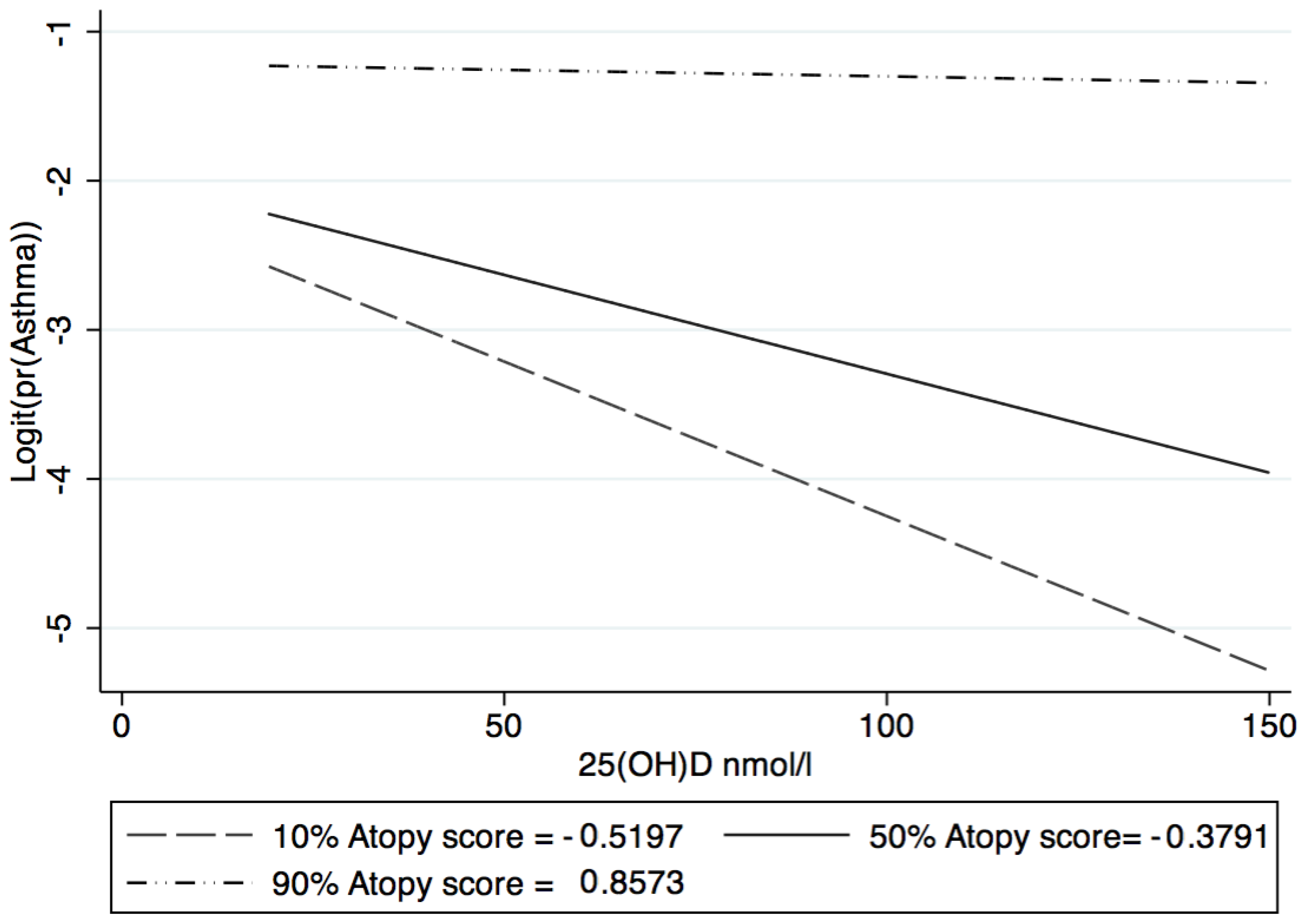
3.2. 25(OH)D and Atopy Interaction
3.3. Association between 25(OH)D and Asthma, by Atopy Category
4. Discussion
4.1. Main Findings
4.2. Strengths and Limitations
4.3. Relation to Previous Work
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- To, T.; Stanojevic, S.; Moores, G.; Gershon, A.S.; Bateman, E.D.; Cruz, A.A.; Boulet, L.P. Global asthma prevalence in adults: Findings from the cross-sectional world health survey. BMC Public Health 2012, 12, 204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Nijs, S.; Venekamp, L.; Bel, E.H. Adult-onset asthma: Is it really different? Eur. Respir. Rev. 2013, 22, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Lotvall, J.; Akdis, C.A.; Bacharier, L.B.; Bjermer, L.; Casale, T.B.; Custovic, A.; Lemanske, R.F.; Wardlaw, A.J.; Wenzel, S.E.; Greenberger, P.A. Asthma endotypes: A new approach to classification of disease entities within the asthma syndrome. J. Allergy Clin. Immun. 2011, 127, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Pearce, N.; Pekkanen, J.; Beasley, R. How much asthma is really attributable to atopy? Thorax 1999, 54, 268–272. [Google Scholar] [CrossRef] [PubMed]
- Anto, J.M.; Sunyer, J.; Basagana, X.; Garcia-Esteban, R.; Cerveri, I.; de Marco, R.; Heinrich, J.; Janson, C.; Jarvis, D.; Kogevinas, M.; et al. Risk factors of new-onset asthma in adults: A population-based international cohort study. Allergy 2010, 65, 1021–1030. [Google Scholar] [CrossRef] [PubMed]
- Vieth, R. Why “Vitamin D” is not a hormone, and not a synonym for 1,25-dihydroxy-vitamin D, its analogs or deltanoids. J. Steroid Biochem. Mol. Biol. 2004, 89–90, 571–573. [Google Scholar] [CrossRef] [PubMed]
- Baeke, F.; Takiishi, T.; Korf, H.; Gysemans, C.; Mathieu, C. Vitamin D: Modulator of the immune system. Curr. Opin. Pharmacol. 2010, 10, 482–496. [Google Scholar] [CrossRef] [PubMed]
- Berry, D.J.; Hesketh, K.; Power, C.; Hypponen, E. Vitamin D status has a linear association with seasonal infections and lung function in British adults. Br. J. Nutr. 2011, 106, 1433–1440. [Google Scholar] [CrossRef] [PubMed]
- Cantorna, M.T.; Snyder, L.; Lin, Y.D.; Yang, L.L. Vitamin D and 1,25(OH)(2)D Regulation of T cells. Nutrients 2015, 7, 3011–3021. [Google Scholar] [CrossRef] [PubMed]
- Scientific Advisory Commitee on Nutrition: Vitamin D and Health. 2016. Available online: https://bit.ly/2s6PsnC (accessed on 26 May 2018).
- National Osteoporosis Society. Vitamin D and Bone Health: A Practical Clinical Guideline for Patient Management; National Osteoporosis Society: Camerton, UK, 2013. [Google Scholar]
- Bischoff-Ferrari, H.A.; Giovannucci, E.; Willett, W.C.; Dietrich, T.; Dawson-Hughes, B. Estimation of optimal serum concentrations of 25-hydroxyvitamin D for multiple health outcomes. Am. J. Clin. Nutr. 2006, 84, 18–28. [Google Scholar] [CrossRef] [PubMed]
- Mai, X.M.; Langhammer, A.; Camargo, C.A., Jr.; Chen, Y. Serum 25-hydroxyvitamin D levels and incident asthma in adults: The HUNT Study. Am. J. Epidemiol. 2012, 176, 1169–1176. [Google Scholar] [CrossRef] [PubMed]
- Confino-Cohen, R.; Brufman, I.; Goldberg, A.; Feldman, B.S. Vitamin D, asthma prevalence and asthma exacerbations: A large adult population-based study. Allergy 2014, 69, 1673–1680. [Google Scholar] [CrossRef] [PubMed]
- De Groot, J.C.; van Roon, E.N.; Storm, H.; Veeger, N.J.; Zwinderman, A.H.; Hiemstra, P.S.; Bel, E.H.; ten Brinke, A. Vitamin D reduces eosinophilic airway inflammation in nonatopic asthma. J. Allergy Clin. Immunol. 2015, 135, 670–675.e673. [Google Scholar] [CrossRef] [PubMed]
- Power, C.; Elliott, J. Cohort profile: 1958 British birth cohort (National Child Development Study). Int. J. Epidemiol. 2006, 35, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Atherton, K.; Fuller, E.; Shepherd, P.; Strachan, D.P.; Power, C. Loss and representativeness in a biomedical survey at age 45 years: 1958 British birth cohort. J. Epidemiol. Commun. Health 2008, 62, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Hypponen, E.; Turner, S.; Cumberland, P.; Power, C.; Gibb, I. Serum 25-hydroxyvitamin D measurement in a large population survey with statistical harmonization of assay variation to an international standard. J. Clin. Endocrinol. Metab. 2007, 92, 4615–4622. [Google Scholar] [CrossRef] [PubMed]
- Pekkanen, J.; Lampi, J.; Genuneit, J.; Hartikainen, A.L.; Jarvelin, M.R. Analyzing atopic and non-atopic asthma. Eur. J. Epidemiol. 2012, 27, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Abramson, M.J.; Perret, J.L.; Dharmage, S.C.; McDonald, V.M.; McDonald, C.F. Distinguishing adult-onset asthma from COPD: A review and a new approach. Int. J. Chronic Obstr. Pulm. Dis. 2014, 9, 945–962. [Google Scholar] [CrossRef] [PubMed]
- Hirai, K.; Shirai, T.; Suzuki, M.; Akamatsu, T.; Suzuki, T.; Hayashi, I.; Yamamoto, A.; Akita, T.; Morita, S.; Asada, K.; et al. A clustering approach to identify and characterize the asthma and chronic obstructive pulmonary disease overlap phenotype. Clin. Exp. Allergy 2017, 47, 1374–1382. [Google Scholar] [CrossRef] [PubMed]
- Millen, A.E.; Bodnar, L.M. Vitamin D assessment in population-based studies: A review of the issues. Am. J. Clin. Nutr. 2008, 87, 1102S–1105S. [Google Scholar] [CrossRef] [PubMed]
- Oktaria, V.; Dharmage, S.C.; Burgess, J.A.; Simpson, J.A.; Morrison, S.; Giles, G.G.; Abramson, M.J.; Walters, E.H.; Matheson, M.C. Association between latitude and allergic diseases: A longitudinal study from childhood to middle-age. Ann. Allerg Asthma Immunol. 2013, 110, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Larose, T.L.; Langhammer, A.; Chen, Y.; Camargo, C.A., Jr.; Romundstad, P.; Mai, X.M. Serum 25-hydroxyvitamin D levels and lung function in adults with asthma: The HUNT Study. Eur. Respir. J. 2015, 45, 1019–1026. [Google Scholar] [CrossRef] [PubMed]
- Strina, A.; Barreto, M.L.; Cooper, P.J.; Rodrigues, L.C. Risk factors for non-atopic asthma/wheeze in children and adolescents: A systematic review. Emerg. Themes Epidemiol. 2014, 11, 5. [Google Scholar] [CrossRef] [PubMed]
- Osborne, N.J.; Ukoumunne, O.C.; Wake, M.; Allen, K.J. Prevalence of eczema and food allergy is associated with latitude in Australia. J. Allergy Clin. Immun. 2012, 129, 865–867. [Google Scholar] [CrossRef] [PubMed]
- Korn, S.; Hubner, M.; Jung, M.; Blettner, M.; Buhl, R. Severe and uncontrolled adult asthma is associated with vitamin D insufficiency and deficiency. Respir. Res. 2013, 14, 25. [Google Scholar] [CrossRef] [PubMed]
- Duijts, L. Fetal and infant origins of asthma. Eur. J. Epidemiol. 2012, 27, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, R.E.; Cullinan, P.; Fishwick, D.; Hoyle, J.; Warburton, C.J.; Strachan, D.P.; Butland, B.K.; Jarvis, D. Asthma and occupation in the 1958 birth cohort. Thorax 2013, 68, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Wortsman, J.; Matsuoka, L.Y.; Chen, T.C.; Lu, Z.; Holick, M.F. Decreased bioavailability of vitamin D in obesity. Am. J. Clin. Nutr. 2000, 72, 690–693. [Google Scholar] [CrossRef] [PubMed]
- Mason, C.; Xiao, L.; Imayama, I.; Duggan, C.R.; Bain, C.; Foster-Schubert, K.E.; Kong, A.; Campbell, K.L.; Wang, C.Y.; Neuhouser, M.L.; et al. Effects of weight loss on serum vitamin D in postmenopausal women. Am. J. Clin. Nutr. 2011, 94, 95–103. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Selected Characteristic at Age 45 | 25(OH)D (nmol/L) at Age 45 * | Atopy ** | Adulthood Asthma or Wheezy Bronchitis at Age 50 *** | |||
|---|---|---|---|---|---|---|
| Q1: Low | Q2: Moderate | Q3: High | No | Yes | ||
| Sex | ||||||
| Male | 50.1 (49.5–50.7) | 899 (37.6) | 1030 (33.0) | 915 (29.4) | 2598 (90.6) | 267 (9.3) |
| Female | 48.6 (48.0–49.2) | 1172 (30.4) | 974 (32.7) | 1110 (37.2) | 2564 (94.1) | 161 (5.9) |
| Socioeconomic Position at 42 | ||||||
| Professional/Managerial-Technical | 49.7 (49.0–50.3) | 842 (32.9) | 824 (32.2) | 893 (34.9) | 2200 (93.2) | 160 (6.7) |
| Skilled (non-manual) | 49.1 (48.1–50.2) | 471 (36.2) | 441 (33.9) | 389 (29.9) | 1096 (91.8) | 98 (8.2) |
| Skilled (manual) | 50.0 (48.8–51.3) | 373 (32.4) | 379 (33.0) | 398 (34.6) | 973 (92.8) | 75 (7.2) |
| Unskilled and others | 47.9 (46.8–49.0) | 320 (35.1) | 312 (34.2) | 280 (30.7) | 742 (90.1) | 82 (10.0) |
| NA | 178 (3) | |||||
| Socioeconomic Position at birth | ||||||
| Professional/Managerial-Technical | 49.8 (48.9–50.7) | 393 (32.7) | 395 (32.9) | 413 (34.4) | 1029 (93.1) | 76 (6.9) |
| Skilled (non-manual) | 51.4 (50.0–52.7) | 212 (34.5) | 199 (32.7) | 204 (33.2) | 534 (92.4) | 44 (7.6) |
| Skilled (manual) | 49.5 (48.9–50.1) | 1019 (34.4) | 968 (32.7) | 978 (33.0) | 2507 (92.5) | 202 (7.5) |
| Unskilled and others | 47.9 (47.0–48.8) | 409 (34.8) | 398 (33.9) | 1174 (31.3) | 974 (91.0) | 96 (8.9) |
| NA | 145 (2) | |||||
| Smoking status | ||||||
| Never | 50.1 (49.5–50.7) | 1026 (36.0) | 879 (30.8) | 946 (33.2) | 2446 (92.5) | 199 (7.5) |
| Ex-Smoker | 50.8 (50.0–51.6) | 551 (34.6) | 530 (33.3) | 511 (32.1) | 1339 (92.1) | 115 (7.9) |
| 1–19 a day | 48.4 (47.3–49.5) | 285 (29.1) | 358 (36.5) | 337 (34.4) | 828 (92.8) | 64 (7.2) |
| ≥20 a day | 44.0 (42.8–45.2) | 206 (30.8) | 235 (32.9) | 227 (34.0) | 541 (91.7) | 49 (8.3) |
| NA | 9 (0) | |||||
| Alcohol consumption | ||||||
| Not in the last 12 months | 44.3 (42.7–45.8) | 131 (36.8) | 122 (34.3) | 103 (28.9) | 293 (89.1) | 36 (10.9) |
| Once a month or less | 45.3 (44.3–46.4) | 314 (38.1) | 246 (30.0) | 264 (32.0) | 683 (89.9) | 77 (10.1) |
| 2–4 times a month | 49.6 (48.8–50.5) | 502 (38.0) | 420 (31.8) | 400 (30.3) | 1135 (93.5) | 79 (6.5) |
| 2–3 times a week | 51.1 (50.4–51.8) | 630 (31.5) | 678 (33.9) | 690 (34.5) | 1687 (92.1) | 145 (7.9) |
| Over 4 times a week | 50.3 (49.5–51.2) | 491 (31.0) | 533 (33.6) | 561 (35.4) | 1351 (93.8) | 90 (6.3) |
| NA | 15 (0) | |||||
| Region | ||||||
| Scotland | 44.0 (42.8–45.2) | 220 (36.1) | 192 (31.5) | 197 (32.4) | 513 (91.6) | 47 (8.4) |
| Northern England | 49.7 (48.9–50.5) | 534 (33.3) | 549 (34.9) | 500 (31.8) | 1337(92.65) | 106 (7.4) |
| Middle England and Wales | 49.1 (48.3–50.0) | 443 (33.4) | 423 (32) | 461 (34.7) | 1101 (91.9) | 97 (8.1) |
| Greater London | 47.2 (45.7–48.8) | 795 (35.0) | 702 (32.4) | 709 (32.7) | 353 (92.4) | 29 (7.6) |
| Southern England | 51.0 (50.3–51.7) | 125 (29.7) | 138 (32.8) | 158 (37.5) | 1858 (92.6) | 149 (7.4) |
| NA | - | |||||
| TV time (hours a day) | ||||||
| <1 | 51.1 (50.0–52.3) | 280 (34.4) | 289 (35.6) | 244 (30.0) | 698 (93.3) | 50 (6.7) |
| 1 to <3 | 50.0 (49.5–50.5) | 1335 (34.5) | 1251 (32.3) | 1282 (33.1) | 3290 (92.6) | 265 (7.5) |
| ≥3 | 46.7 (45.8–47.5) | 1251 (32.3) | 421 (32.3) | 463 (35.5) | 1082 (91.2) | 104 (8.8) |
| NA | 115 (2) | |||||
| Time Spent outdoors in summer (hours/day) | ||||||
| <1 | 43.9 (42.7–45.3) | 182 (37.9) | 147 (30.6) | 151 (31.5) | 404 (92.0) | 35 (8.0) |
| 1 to <3 | 48.2 (47.4–49.1) | 430 (32.6) | 434 (32.9) | 455 (34.5) | 1135 (92.5) | 92 (7.5) |
| ≥3 | 50.5 (50.0–51.1) | 1308 (34.0) | 1266 (32.9) | 1274 (33.1) | 3243 (92.5) | 264 (7.5) |
| NA | 453 (7) | |||||
| Vitamin D supplementation | ||||||
| No | 48.4 (48.0–48.9) | 1708 (34.1) | 1634 (32.7) | 1662 (33.2) | 4233 (92.4) | 346 (7.6) |
| Yes | 55.9 (54.6–57.2) | 223 (33.0) | 228 (33.8) | 224 (33.2) | 582 (92.5) | 47 (7.5) |
| NA | 421 (7) | |||||
| Oily fish consumption | ||||||
| Never | 45.9 (44.8–47.0) | 268 (35.6) | 253 (33.6) | 232 (30.8) | 620 (90.3) | 67 (9.8) |
| Less than weekly | 49.4 (48.8–49.9) | 1137 (33.6) | 1129 (33.3) | 1120 (33.1) | 2888 (93.0) | 219 (7.1) |
| Weekly | 51.1 (50.3–51.9) | 636 (34.4) | 585 (31.7) | 626 (33.4) | 1565 (92.4) | 129 (7.6) |
| NA | 114 (2) | |||||
| Occupational Dust Exposure | ||||||
| No, never | 49.6 (49.0–50.1) | 1382 (35.6) | 1264 (32.5) | 1242 (31.9) | 3347 (93.4) | 236 (6.6) |
| Yes, in the last two years | 49.6 (48.1–51.1) | 244 (32.6) | 255 (34.1) | 250 (33.4) | 634 (92.3) | 53 (7.7) |
| Yes, more than two years ago | 47.1 (46.0–48.3) | 329 (30.6) | 348 (32.4) | 397 (37.0) | 866 (89.8) | 98 (10.2) |
| NA | 389 (6) | |||||
| Obesity (BMI > 30) | ||||||
| No | 51.1 (50.6–51.5) | 1596 (34.9) | 1501 (32.8) | 1483 (32.4) | 3931 (92.9) | 299 (7.1) |
| Yes | 44.4 (43.7–45.1) | 475 (31.3) | 503 (33.1) | 542 (35.7) | 1231 (90.5) | 129 (9.5) |
| NA | - | |||||
| Atopy Category | Vitamin D Status | 25(OH)D Level | ||
|---|---|---|---|---|
| Insufficient (<50 nmol/L) | Sufficient (50–75 nmol/L) | Optimal (>75 nmol/L) | Per 10 nmol/L Increase | |
| All categories | ||||
| Model 1 ¶ | Ref. | 0.84 (0.67–1.05) | 0.69 (0.48–0.98) * | 0.91 (0.86–0.96) ** |
| Model 2 # | Ref. | 0.88 (0.70–1.10) | 0.71 (0.49–1.02) | 0.92 (0.86–0.97) ** |
| Model 3 ¥ | Ref. | 0.94 (0.74–1.19) | 0.77 (0.52–1.12) | 0.94 (0.88–1.00) * |
| Low atopic | ||||
| Model 1 ¶ | Ref. | 0.70 (0.43–1.13) | 0.43 (0.18–1.05) | 0.79 (0.69–0.92) ** |
| Model 2 # | Ref. | 0.73 (0.44–1.22) | 0.46 (0.18–1.12) | 0.80 (0.69–0.93) ** |
| Model 3 ¥ | Ref. | 0.89 (0.52–1.52) | 0.62 (0.25–1.58) | 0.87 (0.74–1.02) |
| Moderate atopic | ||||
| Model 1 ¶ | Ref. | 0.90 (0.61–1.32) | 0.50 (0.25–1.00) * | 0.89 (0.80–0.99) * |
| Model 2 # | Ref. | 0.98 (0.66–1.47) | 0.50 (0.24–1.05) | 0.91 (0.82–1.02) |
| Model 3 ¥ | Ref. | 1.08 (0.71–1.63) | 0.45 (0.20–1.04) | 0.92 (0.82–1.04) |
| High atopic | ||||
| Model 1 ¶ | Ref. | 0.87 (0.67–1.13) | 0.94 (0.63–1.39) | 0.96 (0.90–1.02) |
| Model 2 # | Ref. | 0.89 (0.68–1.17) | 0.96 (0.64–1.44) | 0.96 (0.90–1.03) |
| Model 3 ¥ | Ref. | 0.92 (0.69–1.21) | 1.02 (0.68–1.55) | 0.98 (0.91–1.05) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cherrie, M.P.C.; Sarran, C.; Osborne, N.J. Association between Serum 25-Hydroxy Vitamin D Levels and the Prevalence of Adult-Onset Asthma. Int. J. Environ. Res. Public Health 2018, 15, 1103. https://doi.org/10.3390/ijerph15061103
Cherrie MPC, Sarran C, Osborne NJ. Association between Serum 25-Hydroxy Vitamin D Levels and the Prevalence of Adult-Onset Asthma. International Journal of Environmental Research and Public Health. 2018; 15(6):1103. https://doi.org/10.3390/ijerph15061103
Chicago/Turabian StyleCherrie, Mark P. C., Christophe Sarran, and Nicholas J. Osborne. 2018. "Association between Serum 25-Hydroxy Vitamin D Levels and the Prevalence of Adult-Onset Asthma" International Journal of Environmental Research and Public Health 15, no. 6: 1103. https://doi.org/10.3390/ijerph15061103