Greenspace and Atopic Sensitization in Children and Adolescents—A Systematic Review

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion Criteria and Definitions
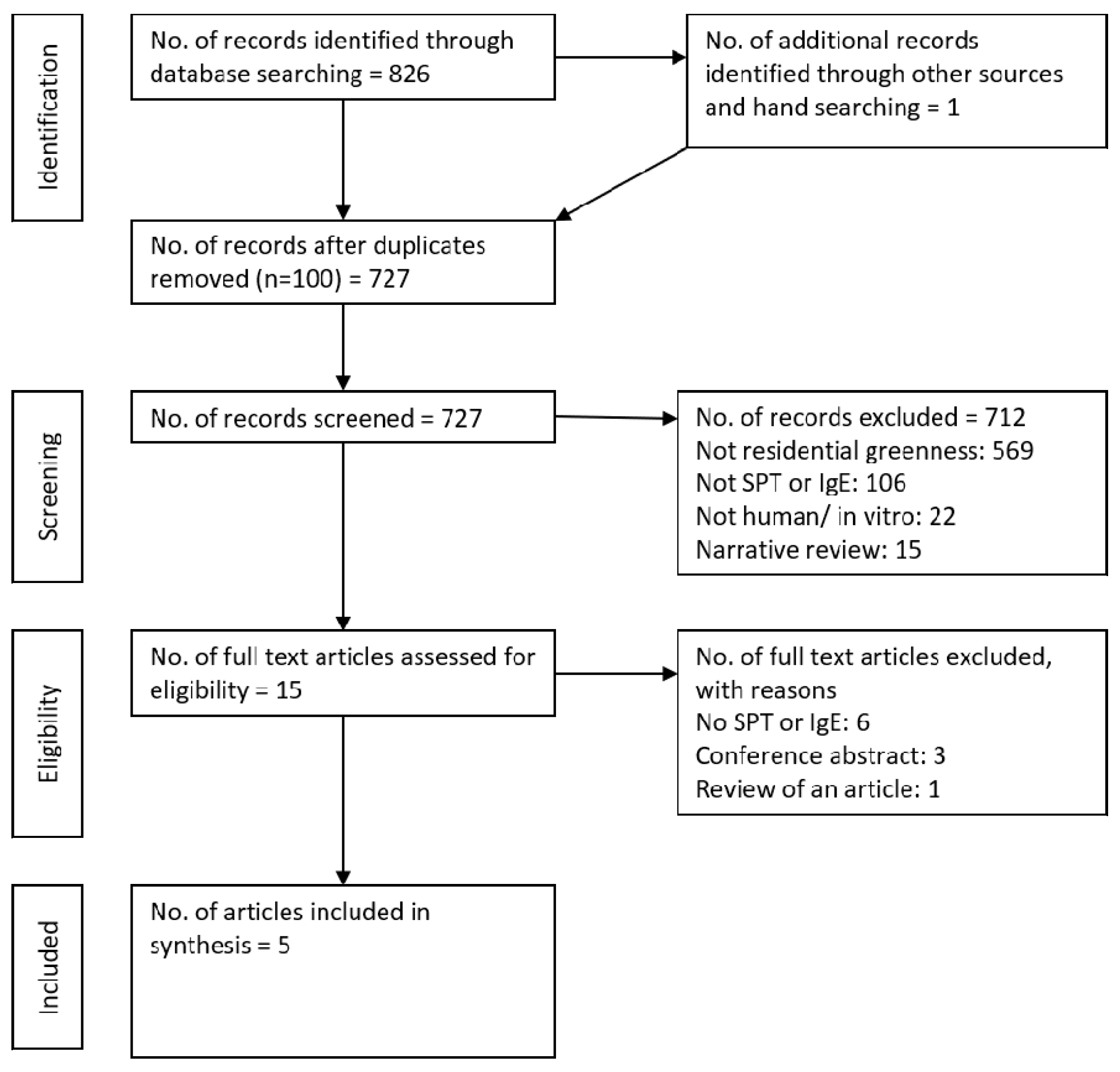
2.3. Selection of Included Articles
2.4. Data Extraction
2.5. Quality Assessment of the Included Studies
2.6. Assessment for Meta-Analysis
3. Results
3.1. Characteristics of Included Studies
3.2. Exposure Assessment
3.3. Outcome Assessment
3.4. Quality Assessment and Risk of Bias
3.5. Qualitative Synthesis of the Included Studies
3.6. Review by Exposure Methodology
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- United Nations. Department of Economic and Social Affairs, Population Division. World Urbanization Prospects: The 2014 Revision, Highlights (ST/ESA/SER.A/352). 2014. Available online: https://www.compassion.com/multimedia/world-urbanization-prospects.pdf (accessed on 10 May 2017).
- Dobbs, C.; Nitschke, C.; Kendal, D. Global drivers and tradeoffs of three urban vegetation ecosystem services. PLoS ONE 2014, 9, e113000. [Google Scholar] [CrossRef] [PubMed]
- Nieuwenhuijsen, M.J.; Khreis, H.; Triguero-Mas, M.; Gascon, M.; Dadvand, P. Fifty Shades of green: pathway to healthy urban living. Epidemiology 2017, 28, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Gascon, M.; Triguero-Mas, M.; Martínez, D.; Dadvand, P.; Forns, J.; Plasència, A.; Nieuwenhuijsen, M.J. Mental health benefits of long-term exposure to residential green and blue spaces: A systematic review. Int. J. Environ. Res. Public Health 2015, 12, 4354–4379. [Google Scholar] [CrossRef] [PubMed]
- Dzhambov, A.M.; Dimitrova, D.D.; Dimitrakova, E.D. Association between residential greenness and birth weight: Systematic review and meta-analysis. Urban For. Urban Green. 2014, 13, 621–629. [Google Scholar] [CrossRef]
- Gascon, M.; Triguero-Mas, M.; Martínez, D.; Dadvand, P.; Rojas-Rueda, D.; Plasència, A.; Nieuwenhuijsen, M.J. Residential green spaces and mortality: A systematic review. Environ. Int. 2016, 86, 60–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Markevych, I.; Schoierer, J.; Hartig, T.; Chudnovsky, A.; Hystad, P.; Dzhambov, A.M.; de Vries, S.; Triguero-Mas, M.; Brauer, M.; Nieuwenhuijsen, M.J.; et al. Exploring pathways linking greenspace to health: Theoretical and methodological guidance. Environ. Res. 2017, 158, 301–317. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Urban Green Spaces and Health. A Review of Evidence; WHO Regional Office for Europe: Copenhagen, Denmark, 2016. [Google Scholar]
- Lambert, K.A.; Bowatte, G.; Tham, R.; Lodge, C.; Prendergast, L.; Heinrich, J.; Abramson, M.J.; Dharmage, S.C.; Erbas, B. Residential greenness and allergic respiratory diseases in children and adolescents–A systematic review and meta-analysis. Environ. Res. 2017, 159, 221. [Google Scholar] [CrossRef] [PubMed]
- Pawankar, R. Allergic diseases and asthma: A global public health concern and a call to action. World Allergy Organ. J. 2014, 7, 12. [Google Scholar] [CrossRef] [PubMed]
- Soriano, J.B.; Abajobir, A.A.; Abate, K.H.; Abera, S.F.; Agrawal, A.; Ahmed, M.B.; Aichour, A.N.; Aichour, I.; Aichour, M.T.E.; Alam, K.; et al. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990-2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir. Med. 2017, 5, 691–706. [Google Scholar]
- Carlson, A.; Nesvold, J.H.; Liu, A. Population-based assessment of asthma symptom burden in children. J. Urban Health 2011, 88, 164–173. [Google Scholar] [CrossRef] [PubMed]
- Guilbert, T.W.; Garris, C.; Jhingran, P.; Bonafede, M.; Tomaszewski, K.J.; Bonus, T.; Hahn, R.M.; Schatz, M. Asthma that is not well-controlled is associated with increased healthcare utilization and decreased quality of life. J. Asthma 2011, 48, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.S.-S.; Sjakste, T.; Sakalauskas, R.; Sitkauskiene, B.; Paramonova, N.; Gasiuniene, E.; Jan, R.L.; Wang, J.Y. The burden of allergic asthma in children: a landscape comparison based on data from Lithuanian, Latvian, and Taiwanese populations. Pediatr. Neonatol. 2012, 53, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Thomsen, S.F. Epidemiology and natural history of atopic diseases. Eur. Respir. J. Suppl. 2015, 2. [Google Scholar] [CrossRef] [PubMed]
- Hanski, I.; Hertzen, L.V.; Fyhrquist, N.; Koskinen, K.; Torppa, K.; Laatikainen, T.; Karisola, P.; Auvinen, P.; Paulin, L.; Mäkelä, M.J.; et al. Environmental biodiversity, human microbiota, and allergy are interrelated. Proc. Natl. Acad. Sci. USA 2012, 109, 8334–8339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruokolainen, L.; Von Hertzen, L.; Fyhrquist, N.; Laatikainen, T.; Lehtomaki, J.; Auvinen, P.; Karvonen, A.M.; Hyvärinen, A.; Tillmann, V.; Niemelä, O.; et al. Green areas around homes reduce atopic sensitization in children. Allergy 2015, 70, 195–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuertes, E.; Markevych, I.; von Berg, A.; Bauer, C.P.; Berdel, D.; Koletzko, S.; Sugiri, D.; Heinrich, J. Greenness and allergies: Evidence of differential associations in two areas in Germany. J. Epidemiol. Comm. Health 2014, 68, 787–790. [Google Scholar] [CrossRef] [PubMed]
- Fuertes, E.; Markevych, I.; Bowatte, G.; Gruziev, O.; Gehring, U.; Becker, A.; Berdel, D.; von Berg, A.; Bergström, A.; Brauer, M.; et al. Residential greenness is differentially associated with childhood allergic rhinitis and aeroallergen sensitization in seven birth cohorts. Allergy 2016, 71, 1461–1471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lovasi, G.S.; O’Neil-Dunne, J.P.; Lu, J.W.; Sheehan, D.; Perzanowski, M.S.; Macfaden, S.W.; King, K.L.; Matte, T.; Miller, R.L.; Hoepner, L.A.; et al. Urban tree canopy and asthma, wheeze, rhinitis, and allergic sensitization to tree pollen in a New York City birth cohort. Environ. Health Persp. 2013, 121, 494–500. [Google Scholar] [CrossRef] [PubMed]
- Weier, J.; Herring, D. Measuring Vegetation (NDVI & EVI). NASA Earth Observatory 2000. Available online: http://earthobservatory.nasa.gov/Features/MeasuringVegetation/ (accessed on 31 May 2016).
- Rhew, I.C.; Vander, S.A.; Kearney, A.; Smith, N.L.; Dunbar, M.D. Validation of the normalized difference vegetation index as a measure of neighborhood greenness. Ann. Epidemiol. 2011, 21, 946–952. [Google Scholar] [CrossRef] [PubMed]
- Pekkarinen, P.T.; Von Hertzen, L.; Laatikainen, T.; Mäkelä, M.J.; Jousilahti, P.; Kosunen, T.U.; Pantelejev, V.; Vartiainen, E.; Haahtela, T. A disparity in the association of asthma, rhinitis, and eczema with allergen-specific IgE between Finnish and Russian Karelia. Allergy 2007, 62, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Naleway, A.L. Asthma and atopy in rural children: is farming protective? J. Clin. Med. Res. 2004, 2, 5–12. [Google Scholar] [CrossRef]
- Wickman, M.; Kull, I.; Pershagen, G.; Nordvall, S. The BAMSE Project: presentation of a prospective longitudinal birth cohort study. Pediatr. Allergy Immunol. 2002, 13, 11–13. [Google Scholar] [CrossRef] [PubMed]
- de Vos, G. Skin Testing versus serum-specific IgE testing: Which is better for diagnosing aeroallergen sensitization and predicting clinical allergy? Curr. Allergy Asthma Rep. 2014, 14, 430. [Google Scholar] [CrossRef] [PubMed]
- Lõhmus, M.; Balbus, J. Making green infrastructure healthier infrastructure. Infect. Ecol. Epidemiol. 2015, 5. [Google Scholar] [CrossRef] [PubMed]
- Haahtela, T.; Laatikainen, T.; Alenius, H.; Auvinen, P.; Fyhrquist, N.; Hanski, I.; von Hertzen, L.; Jousilahti, P.; Kosunen, T.U.; Markelova, O.; et al. Hunt for the origin of allergy–comparing the finnish and russian karelia. Clin. Exp. Allergy 2015, 45, 891–901. [Google Scholar] [CrossRef] [PubMed]
- Ober, C.; Yao, T.-C. The genetics of asthma and allergic disease: A 21(st) century perspective. Immunol. Rev. 2011, 242, 10–30. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author (Year) | Country (Cohort) | n | Study Design | Exposure Metric | Address at Age | Outcome (Cut-Off) | Age at Outcome | Risk of Bias |
|---|---|---|---|---|---|---|---|---|
| Hanski et al. (2012) | Finland (KARA) | 94 | Cross sectional sample with follow up | Land-cover database | 14 to 18 | IgE (≥2.5 kU/L) | 14 to 18 | Mod |
| Lovasi et al. (2013) | USA (CCCEH) | 549 | Population-based birth cohort | LiDAR imagery | Prenatal (sensitivity using address at age 7) | IgE (≥0.35 kU/L) | 7 | Low |
| Fuertes et al. (2014b) | Germany (GINIplus and LISAplus combined) | 5803 | Population-based birth cohorts | NDVI | Birth, 6- and 10-year addresses | IgE (≥0.35 kU/L) | 6 and 10 | Low |
| Ruokolainen et al. (2015) | Finland (KARA) | 94 | Cross sectional sample with follow up | Land-cover database | Not stated | IgE (multiple) | 6 to 20 | Mod |
| Finland (LUKAS) | 300 | Population-based birth cohorts | Birth | IgE (multiple) | 1 and 6 | |||
| Estonia and Finland (DIABIMMUNE) | 594 | High-Risk birth cohorts | Birth | IgE (multiple) | 0.5, 1.5 and 3 | |||
| Fuertes et al. (2016) | Sweden (BAMSE) | 13,016 | Population-based birth cohort | NDVI | 6 to 8 10 to 12 | IgE (≥0.35 kU/L) | 6 to 8 10 to 12 | Low |
| Canada (CAPPS) | Randomized controlled study with asthma intervention | SPT (≥3 mm) | ||||||
| Germany (GINIplus and LISAplus combined) | Population-based birth cohorts | IgE (≥0.35 kU/L) | ||||||
| Australia (MACS) | High-Risk birth cohort | SPT (≥3 mm) | ||||||
| Netherlands (PIAMA) | Population-based birth cohort | IgE (≥0.35 kU/L) | ||||||
| Canada (SAGE) | Population-based birth cohort | SPT (≥3 mm) |
| Author (Year) | Exposure Definition | Outcome Definition | Exposure Estimate (95% CI) |
|---|---|---|---|
| Hanski et al. (2012) | Vegetation cover of the yards and the major land-use types within 3 km of the homes of the study subjects. | Atopic individuals based on IgE antibody level with a cut-off value of 2.5 kUA/L | Increase in one unit of first principal component of land-use types OR: 0.594 (no 95%CI reported) Increase in the number of uncommon native flowering plant species in the yard OR: 0.905 (no 95%CI reported) |
| Lovasi et al. (2013) | Urban tree canopy coverage (combined high-resolution Light Detection and Ranging (LiDAR) data and color infrared aerial imagery) for address at time of birth (250 m). | Serum IgE antibody level with a cut-off value of 0.35 IU/mL | Relative risk (RR) increase per standard deviation of tree canopy coverage 1.20 (1.05, 1.37) |
| Fuertes et al. (2014b) | Residential greenness in a 500 m buffer around the 10-year home addresses (NDVI) | Aeroallergen sensitization (at 6 and 10 years)—IgE ≥ 0.35 kU/L | Aeroallergen sensitization (OR) per increase in mean NDVI: 0.96 (0.85, 1.07) |
| Ruokolainen et al. (2015) | The coverage of five land-use types (agricultural land, built area, forest, water bodies and wetland) around each home was calculated with the CORINE2006 land-cover data using a buffer with radius of 3 km. | Atopy (atopic sensitization) was defined based on the sum of IgE antibodies that are specific to inhalant allergens, such that an individual with log10(ΣIgEinhalant) > IgEth was classified as atopic, where IgEth is a cut-off level. | Significant (p-value < 0.05) associations were found for all log10 cut-off values (IgEth = −0.5 OR: 0.61 IgEth = 0 OR: 0.42, IgEth = 0.5 OR: 0.24, IgEth = 1 OR: 0.30). 95%CI were not reported. |
| Fuertes et al. (2016) | Mean NDVI at 500m and 1000m circular buffers around home address (age 6–8 and 10–12) taken during the spring and summer months of year of birth. | Sensitization was assessed by skin prick testing for CAPPS, MACS, and SAGE, with a positive reaction defined as having a wheal diameter of ≥3 mm. For all other cohorts, sensitization was assessed by measuring allergen-specific IgE levels, with a positive reaction defined as any value ≥0.35 kU/L | OR per 0.2 unit increase in mean NDVI Age 6–8: BAMSE: 1.41 (1.15, 1.73) CAPPS: 0.56 (0.29, 1.06) GINI/LISA North: 0.79 (0.56, 1.10) GINI/LISA South: 1.15 (0.90, 1.48) PIAMA: 0.81 (0.62, 1.05) SAGE: 0.93 (0.65, 1.32) Pooled Result: 0.96 (0.75, 1.22) Age 10–12: GINI/LISA North: 0.72 (0.51, 1.02) GINI/LISA South: 1.27 (1.00, 1.60) MACS: 0.57 (0.34, 0.96) PIAMA: 0.83 (0.63, 1.09) Pooled Result: 0.85 (0.61, 1.18) |
| Exposure Measure | Number of Cohorts | Distance | Age at Outcome | Name | Result | Note |
|---|---|---|---|---|---|---|
| Land-cover database | 3 | 3 km | 0.5–1 years old | DIABIMMUNE and LUKAS (pooled) | OR: 1.00 p = 0.997 | Atopy defined as >1 kU/L total IgE. No confidence intervals provided |
| 1.5–3 years old | DIABIMMUNE | OR: 0.83 p = 0.693 | ||||
| 6–12 years old | LUKAS and KARA (pooled) | OR: 0.33 p = 0.034 | ||||
| 13–20 years old | KARA | OR: 0.09 p = 0.003 | ||||
| LiDAR imagery | 1 | 250 m | 7 years old | CCCEH | RR: 1.20 (1.05, 1.37) | |
| NDVI | 7 | 500 m | 6–8 years old | BAMSE | OR: 1.41 (1.15, 1.73) | |
| CAPPS | OR: 0.56 (0.29, 1.06) | |||||
| GINI/LISA North | OR: 0.79 (0.56, 1.10) | |||||
| GINI/LISA South | OR: 1.15 (0.90, 1.48) | |||||
| PIAMA | OR: 0.81 (0.62, 1.05) | |||||
| SAGE | OR: 0.93 (0.65, 1.32) | |||||
| Pooled Result * | OR: 0.96 (0.75, 1.22) | Heterogeneity: I2 = 73.8% p = 0.0019 | ||||
| 10–12 years old | GINI/LISA North | OR: 0.72 (0.51, 1.02) | ||||
| GINI/LISA South | OR: 1.27 (1.00, 1.60) | |||||
| MACS | OR: 0.57 (0.34, 0.96) | |||||
| PIAMA | OR: 0.83 (0.63, 1.09) | |||||
| Pooled Results * | OR: 0.85 (0.61, 1.18) | Heterogeneity: I2 = 76.5% p = 0.0052 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lambert, K.A.; Bowatte, G.; Tham, R.; Lodge, C.J.; Prendergast, L.A.; Heinrich, J.; Abramson, M.J.; Dharmage, S.C.; Erbas, B. Greenspace and Atopic Sensitization in Children and Adolescents—A Systematic Review. Int. J. Environ. Res. Public Health 2018, 15, 2539. https://doi.org/10.3390/ijerph15112539
Lambert KA, Bowatte G, Tham R, Lodge CJ, Prendergast LA, Heinrich J, Abramson MJ, Dharmage SC, Erbas B. Greenspace and Atopic Sensitization in Children and Adolescents—A Systematic Review. International Journal of Environmental Research and Public Health. 2018; 15(11):2539. https://doi.org/10.3390/ijerph15112539
Chicago/Turabian StyleLambert, Katrina A., Gayan Bowatte, Rachel Tham, Caroline J. Lodge, Luke A. Prendergast, Joachim Heinrich, Michael J. Abramson, Shyamali C. Dharmage, and Bircan Erbas. 2018. "Greenspace and Atopic Sensitization in Children and Adolescents—A Systematic Review" International Journal of Environmental Research and Public Health 15, no. 11: 2539. https://doi.org/10.3390/ijerph15112539