Reducing Inequities in Early Childhood Mental Health: How Might the Neighborhood Built Environment Help Close the Gap? A Systematic Search and Critical Review

 , ,
, , 
Abstract
:1. Introduction
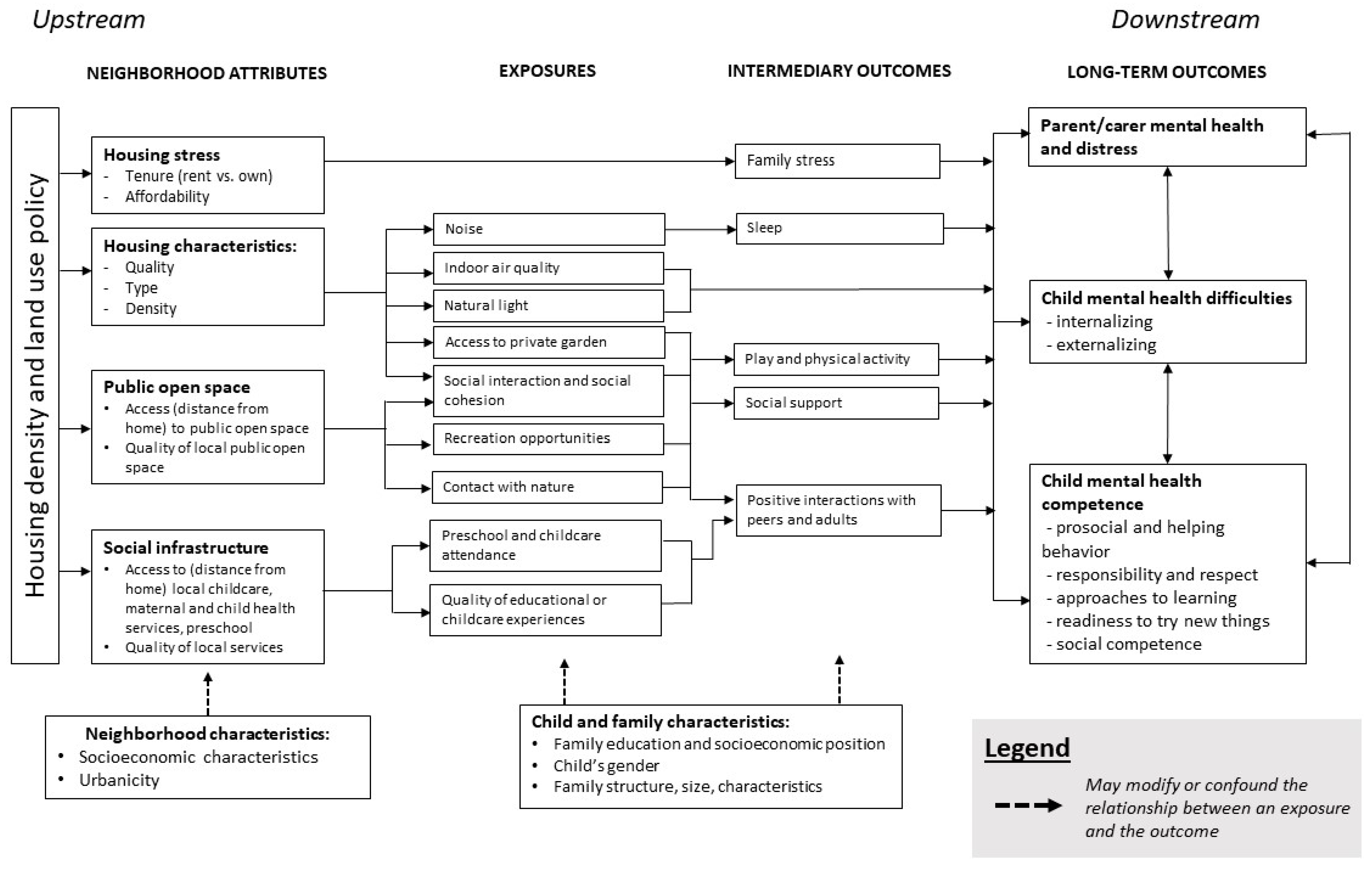
1.1. Conceptual Framework
1.2. Nature and Public Open Space
1.3. Local Service Access, Quality, and Social Infrastructure
1.4. Housing
1.5. Research Gaps
1.6. Project Aim
2. Materials and Methods
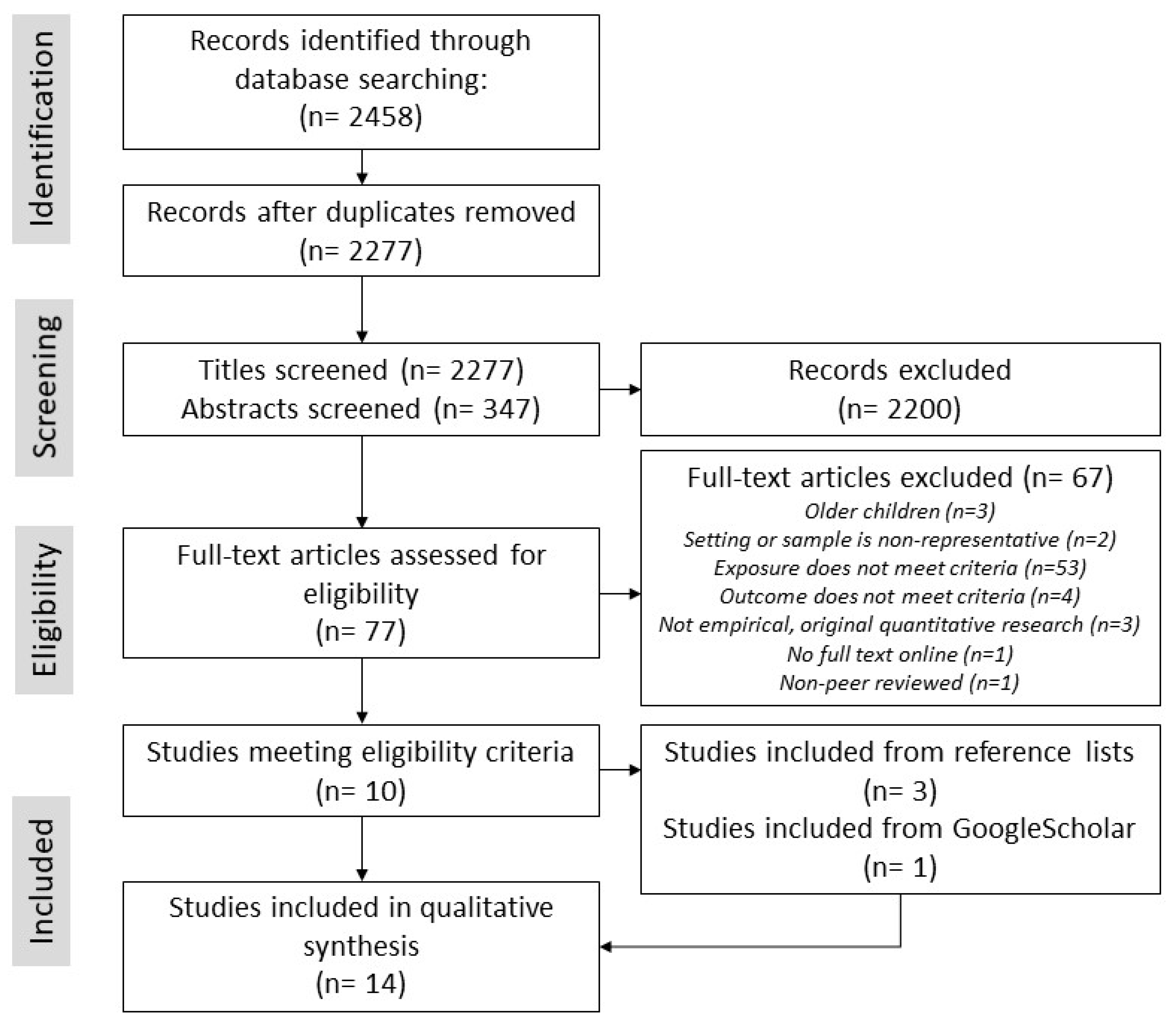
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Quality Assessment and Synthesis
3. Results
3.1. Description of Included Studies
3.2. Nature and Public Open Space in the Neighborhood
3.3. Social Infrastructure and Service Quality in the Neighborhood
3.4. Neighborhood Housing
4. Discussion
Future Research Agenda
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
Pub Med (including MEDLINE) Search Strategy
ProQuest Central Search Strategy
References
- Kieling, C.; Baker-Henningham, H.; Belfer, M.; Conti, G.; Ertem, I.; Omigbodun, O.; Rohde, L.A.; Srinath, S.; Ulkuer, N.; Rahman, A. Child and adolescent mental health worldwide: Evidence for action. Lancet 2011, 378, 1515–1525. [Google Scholar] [CrossRef]
- WHO Fact File: 10 Facts on Mental Health. Available online: https://www.who.int/features/factfiles/mental_health/mental_health_facts/en/ (accessed on 28 April 2019).
- Nagin, D.S.; Tremblay, R.E. Parental and early childhood predictors of persistent physical aggression in boys from kindergarten to high school. Arch. Gen. Psychiatry 2001, 58, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Bosquet, M.; Egeland, B. The development and maintenance of anxiety symptoms from infancy through adolescence in a longitudinal sample. Dev. Psychopathol. 2006, 18, 517–550. [Google Scholar] [CrossRef] [PubMed]
- Social Determinants of Health (CSDH). Closing the Gap in a Generation; World Health Organization (WHO): Geneva, Switzerland, 2008. [Google Scholar]
- Irwin, L.G.; Siddiqi, A.; Hertzman, C. Early Childhood Development: A Powerful Equalizer. Final Report for the World Health Organization’s Commission on the Social Determinants of Health. Available online: https://www.who.int/social_determinants/resources/ecd_kn_report_07_2007.pdf (accessed on 28 April 2019).
- World Health Organization. Promoting Mental Health: Concepts, Emerging Evidence, Practice. A Report of the World Health Organization. Available online: https://www.who.int/mental_health/evidence/en/promoting_mhh.pdf (accessed on 28 April 2019).
- Kvalsvig, A.; O’Connor, M.; Redmond, G.; Goldfeld, S. The unknown citizen: Epidemiological challenges in child mental health. J. Epidemiol. Community Health 2014, 68, 1004–1008. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, E.; O’Connor, M.; Gray, S.; Goldfeld, S. Profiles of mental health competence and difficulties as predictors of children’s early learning. Sch. Ment. Health 2018, 10, 402–416. [Google Scholar] [CrossRef]
- Friedli, L. Mental Health, Resilience and Inequalities. Available online: https://apps.who.int/iris/bitstream/handle/10665/107925/E92227.pdf (accessed on 28 April 2019).
- Moore, T.G.; Arefadib, N.; Deery, A.; West, S. The First Thousand Days. Available online: https://www.rch.org.au/uploadedFiles/Main/Content/ccchdev/CCCH-The-First-Thousand-Days-An-Evidence-Paper-September-2017.pdf (accessed on 28 April 2019).
- Bulotsky-Shearer, R.J.; Bell, E.R.; Domínguez, X. Latent profiles of problem behavior within learning, peer, and teacher contexts: Identifying subgroups of children at academic risk across the preschool year. J. Sch. Psychol. 2012, 50, 775–798. [Google Scholar] [CrossRef] [PubMed]
- Hertzman, C.; Siddiqi, A.; Hertzman, E.; Irwin, L.G.; Vaghri, Z.; Houweling, T.A.J.; Marmot, M. Bucking the inequality gradient through early child development. BMJ 2010, 340, C468. [Google Scholar] [CrossRef]
- Social Determinants of Health (CSDH). Closing the Gap in a Generation: Health Equity Through Action on the Social Determinants of Health. Final Report of the Commission on Social Determinants of Health; World Health Organization (WHO): Geneva, Switzerland, 2008. [Google Scholar]
- Indies, W.; Kingston, J.; Baker-Henningham, H.; Chang, S.M.; Powell, C.A.; Meeks, J.M.; Phd, G.; Walker, S.P.; Wachs, T.D.; Grantham-Mcgregor, S.; et al. Child development 1 inequality in early childhood: Risk and protective factors for early child development. Lancet 2011, 378, 1325–1338. [Google Scholar]
- Centre for Community Child Health. Policy Brief: Translating Early Childhood Research Evidence to Inform Policy and Practice; The Royal Children’s Hospital: Melbourne, Australia, 2012. [Google Scholar]
- Marmot, M.; Bell, R. Health equity and development: The commission on social determinants of health. Eur. Rev. 2010, 18, 1–7. [Google Scholar] [CrossRef]
- Bayer, J.K.; Ukoumunne, O.C.; Lucas, N.; Wake, M.; Scalzo, K.; Nicholson, J.M. Risk factors for childhood mental health symptoms: National longitudinal study of Australian children. Pediatrics 2011, 128, e865–e879. [Google Scholar] [CrossRef]
- Pillas, D.; Marmot, M.; Naicker, K.; Goldblatt, P.; Morrison, J.; Pikhart, H. Social inequalities in early childhood health and development: A European-wide systematic review. Pediatr. Res. 2014, 76, 418–424. [Google Scholar] [CrossRef] [PubMed]
- Goldfeld, S.; Kvalsvig, A.; Incledon, E.; O’Connor, M.; Mensah, F. Predictors of mental health competence in a population cohort of Australian children. J. Epidemiol. Community Health 2014, 68. [Google Scholar] [CrossRef] [PubMed]
- Evans, G.W. The environment of childhood poverty. Luthar 1997, 59, 77–92. [Google Scholar] [CrossRef] [PubMed]
- Bronfenbrenner, U. The Ecology of Human Development: Experiments by Nature and Design; Harvard University Press: Cambridge, MA, USA, 1979. [Google Scholar]
- Barry, M.M. Addressing the determinants of positive mental health: Concepts, evidence and practice. Int. J. Ment. Health Promot. 2009, 11, 4–17. [Google Scholar] [CrossRef]
- Brooks-Gunn, J.; Duncan, G.J. The effects of poverty on children. Futur. Child. 1997, 7, 55–71. [Google Scholar] [CrossRef]
- Leventhal, T.; Brooks-Gunn, J. The neighborhoods they live in: The effects of neighborhood residence on child and adolescent outcomes. Psychol. Bull. 2000, 126, 309–337. [Google Scholar] [CrossRef] [PubMed]
- Edwards, B. Does it takes a village? An investigation of neighbourhood effects on Australian children’s development. Fam. Matters 2005, 72, 36–43. [Google Scholar]
- Koohsari, M.J.; Badland, H.; Giles-Corti, B. (Re)Designing the built environment to support physical activity: Bringing public health back into urban design and planning. Cities 2013, 35, 294–298. [Google Scholar] [CrossRef]
- Astell-Burt, T.; Feng, X.; Mavoa, S.; Badland, H.M.; Giles-Corti, B. Do low-income neighbourhoods have the least green space? A cross-sectional study of Australia’s most populous cities. BMC Public Health 2014, 14, 292. [Google Scholar] [CrossRef] [PubMed]
- Goldfeld, S.; Villanueva, K.; Lee, J.L.; Robinson, R.; Moriarty, A.; Peel, D.; Tanton, R.; Giles-Corti, B.; Woolcock, G.; Brinkman, S.; et al. Foundational Community Factors (Fcfs) for Early Childhood Development: A Report on the Kids in Communities Study (Kics Report). Available online: https://www.rch.org.au/uploadedFiles/Main/Content/ccch/CCCH-KICS-Final-Report-April-2018.pdf (accessed on 28 April 2019).
- Villanueva, K.; Badland, H.; Kvalsvig, A.; O’Connor, M.; Christian, H.; Woolcock, G.; Giles-Corti, B.; Goldfeld, S. Can the neighborhood built environment make a difference in children’s development? Building the research agenda to create evidence for place-based children’s policy. Acad. Pediatr. 2016, 16, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Markevych, I.; Schoierer, J.; Hartig, T.; Chudnovsky, A.; Hystad, P.; Dzhambov, A.M.; De Vries, S.; Triguero-Mas, M.; Brauer, M.; Nieuwenhuijsen, M.J.; et al. Exploring pathways linking greenspace to health: Theoretical and methodological guidance. Environ. Res. 2017, 158, 301–317. [Google Scholar] [CrossRef] [PubMed]
- Markevych, I.; Tiesler, C.M.T.; Fuertes, E.; Romanos, M.; Dadvand, P.; Nieuwenhuijsen, M.J.; Berdel, D.; Koletzko, S.; Heinrich, J. Access to urban green spaces and behavioural problems in children: Results from the GINIplus and LISAplus studies. Environ. Int. 2014, 71, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Amoly, E.; Dadvand, P.; Forns, J.; Lopez-Vicente, M.; Basagana, X.; Julvez, J.; Alvarez-Pedrerol, M.; Nieuwenhuijsen, M.J.; Sunyer, J. Green and blue spaces and behavioral development in Barcelona schoolchildren: The BREATHE project. Environ. Health Perspect. 2014, 122, 1351–1358. [Google Scholar] [CrossRef] [PubMed]
- Gascon, M.; Triguero-Mas, M.; Martínez, D.; Dadvand, P.; Forns, J.; Plasència, A.; Nieuwenhuijsen, M.J. Mental health benefits of long-term exposure to residential green and blue spaces: A systematic review. Int. J. Environ. Res. Public Health 2015, 12, 4354–4379. [Google Scholar] [CrossRef] [PubMed]
- Giles-Corti, B.; Broomhall, M.H.; Knuiman, M.; Collins, C.; Douglas, K.; Ng, K.; Lange, A.; Donovan, R.J. Increasing walking how important is distance to, attractiveness, and size of public open space? Am. J. Prev. Med. 2005, 28, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, T.; Leslie, E.; Giles-Corti, B.; Owen, N. Associations of neighbourhood greenness with physical and mental health: Do walking, social coherence and local social interaction explain the relationships? BMJ 2008, 62. [Google Scholar] [CrossRef]
- Dadvand, P.; Bartoll, X.; Basagaña, X.; Dalmau-Bueno, A.; Martinez, D.; Ambros, A.; Cirach, M.; Triguero-Mas, M.; Gascon, M.; Borrell, C.; et al. Green spaces and general health: Roles of mental health status, social support, and physical activity. Environ. Int. 2016, 91, 161–167. [Google Scholar] [CrossRef]
- Fattore, T.; Mason, J.; Watson, E.; Mason, J.; Watson, E. When Children are asked about their well-being: Towards a framework for guiding policy. Child Indic. Res. 2009, 2, 57–77. [Google Scholar] [CrossRef]
- Hughey, S.M.; Walsemann, K.M.; Child, S.; Powers, A.; Reed, J.A.; Kaczynski, A.T. Using an environmental justice approach to examine the relationships between park availability and quality indicators, neighborhood disadvantage, and racial/ethnic composition. Landsc. Urban Plan. 2016, 148, 159–169. [Google Scholar] [CrossRef]
- Crawford, D.; Timperio, A.; Giles-Corti, B.; Ball, K.; Hume, C.; Roberts, R.; Andrianopoulos, N.; Salmon, J. Do features of public open spaces vary according to neighbourhood socio-economic status? Health Place 2008, 14, 889–893. [Google Scholar] [CrossRef]
- Davern, M.; Gunn, L.; Whitzman, C.; Higgs, C.; Giles-Corti, B.; Simons, K.; Villanueva, K.; Mavoa, S.; Roberts, R.; Badland, H. Using spatial measures to test a conceptual model of social infrastructure that supports health and wellbeing. Cities Health 2018, 1, 194–209. [Google Scholar] [CrossRef]
- Cloney, D.; Cleveland, G.; Hattie, J.; Tayler, C. Variations in the availability and quality of early childhood education and care by socioeconomic status of neighborhoods. Early Educ. Dev. 2015, 27, 384–401. [Google Scholar] [CrossRef]
- Leventhal, T.; Newman, S. Housing and child development. Child. Youth Serv. Rev. 2010, 32, 1165–1174. [Google Scholar] [CrossRef]
- Howden-Chapman, P.; Baker, M.G.; Bierre, S. The houses children live in: Policies to improve housing quality. Policy Q. 2013, 9, 35–39. [Google Scholar] [CrossRef]
- Kamp Dush, C.M.; Schmeer, K.K.; Taylor, M. Chaos as a social determinant of child health: Reciprocal associations? Soc. Sci. Med. 2013, 95, 69–76. [Google Scholar] [CrossRef]
- Evans, G.W.; Lercher, P.; Kofler, W.W. Crowding and children’s mental health: The role of house type. J. Environ. Psychol. 2002, 22, 221–231. [Google Scholar] [CrossRef]
- Evans, G.W. The built environment and mental health. J. Urban Heath. 2003, 80, 536–555. [Google Scholar] [CrossRef]
- Coulton, C.J.; Richter, F.; Kim, S.-J.; Fischer, R.; Cho, Y. Temporal effects of distressed housing on early childhood risk factors and kindergarten readiness. Child Youth Serv. Rev. 2016, 68, 59–72. [Google Scholar] [CrossRef]
- Evans, G.W.; Wells, N.M.; Moch, A. Housing and mental health: A review of the evidence and a methodological and conceptual critique. J. Soc. Issues 2003, 59, 475–500. [Google Scholar] [CrossRef]
- Lilius, J. Is there room for families in the inner city? Life-stage blenders challenging planning. Hous. Stud. 2014, 29, 843–861. [Google Scholar] [CrossRef]
- UNICEF. Children in an increasingly urban world. In The State of the World’s Children 2012; United Nations Children’s Fund (UNICEF): New York, NY, USA, 2012; pp. 1–11. [Google Scholar]
- Grant, M.J.; Booth, A. A typology of reviews: An analysis of 14 review types and associated methodologies. Health Inf. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D. The PRISMA group preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Richardson, E.A.; Pearce, J.; Shortt, N.K.; Mitchell, R. The role of public and private natural space in children’s social, emotional and behavioural development in Scotland: A longitudinal study. Environ. Res. 2017, 158, 729–736. [Google Scholar] [CrossRef] [PubMed]
- Feng, X.; Astell-Burt, T. Residential green space quantity and quality and child well-being: A longitudinal study. Am. J. Prev. Med. 2017, 53, 616–624. [Google Scholar] [CrossRef] [PubMed]
- Scott, J.T.; Kilmer, R.P.; Wang, C.; Cook, J.R.; Haber, M.G. Natural environments near schools: Potential benefits for socio-emotional and behavioral development in early childhood. Am. J. Community Psychol. 2018, 62, 419–432. [Google Scholar] [CrossRef] [PubMed]
- Balseviciene, B.; Sinkariova, L.; Grazuleviciene, R.; Andrusaityte, S.; Uzdanaviciute, I.; Dedele, A.; Nieuwenhuijsen, M.J. Impact of residential greenness on preschool children’s emotional and behavioral problems. Int. J. Environ. Res. Public Health 2014, 11, 6757–6770. [Google Scholar] [CrossRef] [PubMed]
- Zach, A.; Meyer, N.; Hendrowarsito, L.; Kolb, S.; Bolte, G.; Nennstiel-Ratzel, U.; Stilianakis, N.I.; Herr, C. Association of sociodemographic and environmental factors with the mental health status among preschool children—Results from a cross-sectional study in Bavaria, Germany. Int. J. Hyg. Environ. Health 2016, 219, 458–467. [Google Scholar] [CrossRef]
- Baumgardner, D.J.; Schreiber, A.L.; Havlena, J.A.; Bridgewater, F.D.; Steber, D.L.; Lemke, M.A. Geographic analysis of diagnosis of attention-deficit/hyperactivity disorder in children: Eastern wisconsin, USA. Int. J. Psychiatry Med. 2010, 40, 363–382. [Google Scholar] [CrossRef] [PubMed]
- Christian, H.; Ball, S.J.; Zubrick, S.R.; Brinkman, S.; Turrell, G.; Boruff, B.; Foster, S. Relationship between the neighbourhood built environment and early child development. Health Place 2017, 48, 90–101. [Google Scholar] [CrossRef]
- Flouri, E.; Midouhas, E.; Joshi, H. The role of urban neighbourhood green space in children’s emotional and behavioural resilience. J. Environ. Psychol. 2014, 40, 179–186. [Google Scholar] [CrossRef]
- Casas, L.; Torrent, M.; Zock, J.P.; Doekes, G.; Forns, J.; Guxens, M.; Täubel, M.; Heinrich, J.; Sunyer, J. Early life exposures to home dampness, pet ownership and farm animal contact and neuropsychological development in 4 year old children: A prospective birth cohort study. Int. J. Hyg. Environ. Health 2013, 216, 690–697. [Google Scholar] [CrossRef] [PubMed]
- Morales, E.; Julvez, J.; Torrent, M.; De Cid, R.; Guxens, M.; Bustamante, M.; Künzli, N.; Sunyer, J. Association of early-life exposure to household gas appliances and indoor nitrogen dioxide with cognition and attention behavior in preschoolers. Am. J. Epidemiol. 2009, 169, 1327–1336. [Google Scholar] [CrossRef]
- Richman, N. The effects of housing on pre-school children and their mothers. Dev. Med. Child Neurol. 1974, 16, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Richman, N. Behaviour problems in pre-school children: Family and social factors. Br. J. Psychiatry 1977, 131, 523–527. [Google Scholar] [CrossRef]
- Rijlaarsdam, J.; Tiemeier, H.; Hofman, A.; Jaddoe, V.W.V.; Mackenbach, J.P.; Verhulst, F.C.; Stevens, G.W.J.M. Home environments of infants: Relations with child development through age 3. J. Epidemiol. Community Health 2013, 67, 14–20. [Google Scholar] [CrossRef]
- Sonuga-Barke, E.; Stevenson, J.; Thompson, M.J.J. Mental health of preschool children and their mothers in a mixed urban/rural population. Br. J. Psychiatry 1996, 168, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Minh, A.; Muhajarine, N.; Janus, M.; Brownell, M.; Guhn, M. A review of neighborhood effects and early child development: How, where, and for whom, do neighborhoods matter? Health Place 2017, 46, 155–174. [Google Scholar] [CrossRef] [PubMed]
- Sharkey, P.; Faber, J.W. Where, when, why, and for whom do residential contexts matter? Moving away from the dichotomous understanding of neighborhood effects. Annu. Rev. Sociol. 2014, 40, 559–579. [Google Scholar] [CrossRef]
- Whitehead, M.; Dahlgren, G. Levelling up (Part 1): A Discussion Paper on Concepts and Principles for Tackling Social Inequities in Health. Available online: https://apps.who.int/iris/bitstream/handle/10665/107790/E89383.pdf (accessed on 28 April 2019).
- Wolch, J.R.; Byrne, J.; Newell, J.P. Urban green space, public health, and environmental justice: The challenge of making cities ‘just green enough’. Landsc. Urban Plan. 2014, 125, 234–244. [Google Scholar] [CrossRef] [Green Version]
- Abramson, M.; Lodge, C.; Heinrich, J.; Dharmage, S.; Tham, R.; Prendergast, L.; Erbas, B.; Bowatte, G.; Lambert, K. Greenspace and atopic sensitization in children and adolescents—A systematic review. Int. J. Environ. Res. Public Health 2018, 15, 2539. [Google Scholar]
- Lamb, K.E.; Mavoa, S.; Coffee, N.T.; Parker, K.; Richardson, E.A.; Thornton, L.E. Public open space exposure measures in Australian health research: A critical review of the literature. Geogr. Res. 2019, 57, 67–83. [Google Scholar] [CrossRef]
- Vich, G.; Marquet, O.; Miralles-Guasch, C. The scales of the metropolis: Exploring cognitive maps using a qualitative approach based on SoftGIS software. Geoforum 2018, 88, 49–56. [Google Scholar] [CrossRef]
- Kyttä, A.M.; Broberg, A.K.; Kahila, M.H. Urban environment and children’s active lifestyle: SoftGIS revealing children’s behavioral patterns and meaningful places. Am. J. Health Promot. 2012, 26, e137–e149. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author (Year) | Country | n | Design | Exposure | Outcome | Age at Outcome | Adjustments | Results |
|---|---|---|---|---|---|---|---|---|
| More than one built environment domain (n = 3 studies; N/POS: n = 3, HOUS: n = 3, SERV: n = 1) | ||||||||
| Baumgardner et al. (2010) [59] | USA | 50,463 | Case-control | N/POS-1: Distance from child’s home address to closest park N/POS-2: Distance from child’s home to nearest waterway HOUS: Suburban home address (compared with central-city address) | MHD: ADHD diagnosis (cases) versus no diagnosis (controls) | 5–17 years | Child’s age, child’s sex, child’s race, Eastern Wisconsin vs. Milwaukee County (stratified), population density, median household income (area-level) | N/POS-1 MHD: In Eastern Wisconsin, larger distance associated with higher odds of ADHD diagnosis (OR: 1.04, 95% CI 1.03–1.04). N/POS-2 MHD: In Eastern Wisconsin, NS. MHD: In Milwaukee County, larger distance to nearest waterway associated with lower odds of ADHD diagnosis (OR: 0.92, 95% CI 0.88–0.97). HOUS MHD: In Milwaukee County, suburban address associated with higher odds of ADHD (OR: 1.40, 95% CI 1.20–1.63). |
| Christian et al. (2017) [60] | Australia | 149 NHs (23,395 children) | Partial ecological | N/POS-1: Population-based median distance to nearest park N/POS-2: Population-based median distance to nearest attractive park N/POS-3: Population-based median distance to nearest pocket park N/POS-4: Population-based median distance to nearest nature/conservation area SERV-1: Population-based median distance to nearest Kindergarten SERV-2: Population-based median distance to nearest child-center-based care SERV-3: Population-based median distance to nearest family support service SERV-4: Population-based median distance to nearest child health clinic SERV-5: Population-based median distance to nearest playgroup HOUS-1: % residential land not part of building footprint (home yard space in NH) HOUS-2: Residential density | MHC: Social competence (TR): Odds of poor social competence. MHC: Emotional maturity (TR): Odds of poor emotional maturity. | 5 years | NH SES, % households in NH with 4 year old that were: female, Aboriginal or Torres Strait Islander origin, had one or more siblings, at least one parent > 24 years, single parent families, at least one parent educated beyond secondary school, family income < $3000/fortnight, moved in last 12 months | N/POS-1 MHC: Larger distance to nearest park associated with better social competence (OR: 0.996, 95% CI 0.993 to 0.999) and better emotional maturity (OR: 0.989, 95% CI 0.977 to 0.998). N/POS-2 MHC: Larger distance to nearest attractive park associated with better social competence (OR: 0.990, 95% CI 0.978 to 0.999). Emotional maturity: NS. N/POS-3 & N/POS-4 MHC: NS. SERV-2 MHC: Larger distance to child-center-based-care associated with better social competence and better emotional maturity. SERV-1, 3, 4, & 5 MHC: NS. HOUS-1 MHC: Higher % home yard space in NH associated with better emotional maturity (5th quintile OR: 0.745, 95% CI 0.567 to 0.969). HOUS-2 MHC: NS. |
| Richardson et al. (2017) [54] | Scotland | 2909 | Cross-sectional (by age 4 years); Prospective cohort (by age 6 years) | N/POS-1: % land area that is public parks around 500m (Euclidean) of child’s home postcode N/POS-2: % land area that is natural space around 500m (Euclidean) of child’s home postcode HOUS: Access to sole or shared private garden (yes/no) (PR) | MHD: Total difficulties (PR) MHC: Prosocial behavior Outcome at 6 years: change in MHD or MHC over time. | 4 years, 6 years | Child’s sex, maternal education (stratified) | N/POS-1 MHD: Overall and in both maternal education groups: NS at 4 years, 6 years. MHC: Overall and in both education groups: NS at 4 years, 6 years. N/POS-2 MHD: Overall NS at 4 years, 6 years. MHD: In lower education group, higher % area natural space associated with fewer peer problems (−0.08 per IQR increase) at 4 years, NS at 6 years. MHC: Higher % natural space associated with more prosocial behavior at 4 years (+0.08 per IQR increase), NS at 6 years. MHC: In higher education group, % area natural space associated with more prosocial behavior (+0.12 per IQR increase). HOUS MHD: Overall no garden access associated with higher: total difficulties (+1.15), peer problems (+0.23), hyperactivity (+0.52), conduct problems (+0.27) at 4 years. MHD: Overall, change in difficulties over time (at 6 years): NS. In high education group, no garden access associated with worsening emotional problems and total difficulties over time (at 6 years), but NS for low education group. MHC: Overall: NS. |
| Nature and public open space domain (n = 6) | ||||||||
| Balseviciene et al. (2014) [57] | Lithuania | 1,468 | Cross-sectional | N/POS-1: Distance (straight line) from child’s home address to closest park N/POS-2: Residential greenness (average NDVI in 300m buffer around child’s home) | MHD: Total difficulties (PR) MHC: Prosocial behavior (PR) | 4–6 years | Child’s sex, child’s age, maternal education (stratified), parenting stress | N/POS-1 MHD: In lower education group, larger distance associated with more total difficulties (β: 0.069, p < 0.05) and more peer problems, conditional problems, and hyperactivity. In higher education group, NS except for larger distance nearly associated with fewer emotional problems (β: −0.008, p < 0.1). MHC: In lower education group, larger distance associated with less prosocial behavior (β: −0.029, p < 0.05). Higher education group: NS. N/POS-2 MHD: In higher education group, higher NDVI associated with more total difficulties (β: 2.286, p < 0.1), and more conditional problems and hyperactivity. MHC: NS in low education group. In high education group, higher NDVI associated with less prosocial behavior (β: −1.104, p < 0.05). |
| Feng & Astell-Burt (2017) [55] | Australia | 4968 | Prospective Cohort | N/POS-1: % land area classified as parkland within child’s area of residence (SA-2). N/POS-2: Perception (PR) of good parks, playgrounds, play spaces in neighborhood (low quality vs high quality). | MHD: total difficulties, internalizing, externalizing (PR) | 6–7 years (ages 4–5 years at baseline) | Child’s sex, child’s Indigenous status, child’s age group, NH SES, NH urbanicity | N/POS-1 MHD: Higher % parkland associated with lower difficulties (21 to 40% bracket: −0.29 (95% CI −0.47 to −0.10), and both lower internalizing and externalizing difficulties. N/POS-2 MHD: Poor quality parks associated with higher difficulties (disagree vs. agree: 0.53, 95% CI 0.34 to 0.72) and both higher internalizing and externalizing difficulties. |
| Flouri et al. (2014) [61] | England | 6384 | Prospective Cohort | N/POS: % land area that is green space | MHD: Emotional and behavioral problems (PR) | 5 years, 7 years | Family SES (PR) (stratified), NH SES | MHD: Overall sample: NS. MHD: In low SES group, higher % green space associated with fewer emotional difficulties at 5 years. |
| Scott et al. (2018) [56] | USA | 1551 | Prospective Cohort | N/POS-1: % houses within 0.5 miles of public park (public, outdoor recreation area) around child’s home. N/POS-2: % impervious surface around child’s home. N/POS-3: % tree canopy around child’s home. | MHD: behavioral concerns (TR) MHC: Socio-emotional functioning (TR): Initiative, self-regulation, attachment | 4–5 years | Child’s age, child’s race (Hispanic ethnic status), area-level median income, violent crime rate, population density, multilevel techniques (accounted for nested data). | N/POS-1 MHD: NS. MHC: NS. N/POS-2 MHD: NS. MHC: NS. N/POS-3 MHD: Higher % tree canopy associated with improved (less) behavior concerns (γ = −0.19, p < 0.01). MHC: Higher % tree canopy associated with improved self-regulation (γ = 0.175, p < 0.01). |
| Zach et al. (2016) [58] | Germany | 5117 | Cross-sectional | N/POS: Availability (PR) of public parks or green space in neighborhood (yes vs. no). | MHD: total difficulties and hyperactivity. Binary—classified as ‘normal’ vs. ‘borderline or abnormal.’ (PR) | Preschool, age not specified | Child’s sex, family SES, NH traffic load, crowding | MHD: In sample (unweighted) no access to green space was associated with higher odds of difficulties (OR: 1.92, 95% CI 1.72–2.96) and higher odds of hyperactivity-inattention (OR: 1.53, 95% CI 0.99–2.35). MHD: In weighted data (representative of Bavaria), no access to green space associated with higher odds of difficulties (OR: 3.17, 95% CI 1.76–5.70) and higher odds of hyperactivity-inattention (OR: 3.03, 95% CI 1.64–5.58) |
| Housing domain (n = 6) | ||||||||
| Casas et al. (2013) [62] | Spain | 381 | Prospective cohort | HOUS: Dampness in child’s bedroom, parent’s bedroom, living room, any other room in first 2 years of life (PR). Categorized as ‘never’, ‘ever (<2 years)’, ‘persistent (2 years)’. | MHC: Social competence (TR) | 4 years | Child’s age, child’s sex, maternal education, maternal smoking during pregnancy, weeks of breastfeeding, folic acid intake during pregnancy, number of people living in the house, housing location (urban area, housing estate, country house) | MHC: Persistent dampness in child’s room associated with worse social competence scores (compared with non-persistent) (β: −6.54, 95%CI −12.19 to −0.89). MHC: Ever damp in child’s room (compared with never): NS. Dampness at home, in parent’s room, in living room: NS (irrespective of ever/never, persistent/non-persistent). |
| Morales et al. (2009) [63] | Spain | 398 | Prospective cohort | HOUS: Number (1 or 2) of household gas appliances (cooking, heating and cooling systems) compared with no gas appliances (HV) | MHD: ADHD (PR and TR). MHD: Inattention subset (PR and TR) MHD: Hyperactivity subset (PR and TR) | 4 years | Child’s sex, maternal SES, maternal education, school trimester at testing, outcome evaluator (neuropsychologist), maternal smoking during pregnancy, number of smokers at home, maternal alcohol consumption during pregnancy, home location. | MHD: Two gas appliances associated with higher odds of inattention (OR: 3.59, 95% CI 1.14–11.33) and nearly associated with higher odds of ADHD (OR: 2.72, 95% CI 1.01–7.28) compared with no gas appliances. MHD: One gas appliance: NS. |
| Richman (1974) [64] | England | 75 | Cross-sectional | HOUS: Living in high-rise flats (higher than four floors), low-rise flats (not higher than four floors), houses (HV). | MHD: proportion in each group with behavior problems (PR and HV). | 3 years | No statistical adjustments. Comparable SES between the three groups. | MHD: No significant differences between the three groups in proportion of behavior problems (high-rise flats: 16.0%, low-rise flats: 28.0%, houses: 20.0%). |
| Richman (1977) [65] | England | 196 | Case-control | HOUS-1: Living in high-rise flats. HOUS-2: Housing in poor condition (dampness, no electricity, no hot water) (HV). | MHD: behavior problems (PR and HV) | 3 years | No statistical adjustments. Comparable SES between cases and controls. | HOUS-1 MHD: Children living in high-rise housing had significantly higher behavior problems (30% scored 10+, compared with 14% in overall sample, p < 0.01). HOUS-2 MHD: Of the children with a behavior problem and maternal depression, 27% (12/44) had severe housing problems, compared with 7% (5/75) with no behavior problem or maternal depression (p < 0.01). |
| Rijlaarsdam et al. (2013) [66] | Netherlands | 2164 | Prospective Cohort | HOUS: Physical home environment: 10-items including cleanliness, central heating system present, cluttered, dark, building is safe, play area outside is safe, neighborhood is pleasant. | MHD: internalizing and externalizing (PR). | 3 years | Child’s sex, child’s age, child’s national origin (non-Western), family low income, maternal education, socio-emotional involvement with parent, maternal depressive symptoms at 20 weeks gestation. | MHD: NS. |
| Thompson et al. (1996) [67] | England | 1047 | Cross-sectional | HOUS: % households with ‘amenities’ (e.g., toilets, hot water) in the child’s ward of residence | MHD: behavior problem (yes/no), difficult temperament (yes/no), overactivity (yes/no) (PR) | 3 years | No statistical adjustments. | MHD: NS. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alderton, A.; Villanueva, K.; O’Connor, M.; Boulangé, C.; Badland, H. Reducing Inequities in Early Childhood Mental Health: How Might the Neighborhood Built Environment Help Close the Gap? A Systematic Search and Critical Review. Int. J. Environ. Res. Public Health 2019, 16, 1516. https://doi.org/10.3390/ijerph16091516
Alderton A, Villanueva K, O’Connor M, Boulangé C, Badland H. Reducing Inequities in Early Childhood Mental Health: How Might the Neighborhood Built Environment Help Close the Gap? A Systematic Search and Critical Review. International Journal of Environmental Research and Public Health. 2019; 16(9):1516. https://doi.org/10.3390/ijerph16091516
Chicago/Turabian StyleAlderton, Amanda, Karen Villanueva, Meredith O’Connor, Claire Boulangé, and Hannah Badland. 2019. "Reducing Inequities in Early Childhood Mental Health: How Might the Neighborhood Built Environment Help Close the Gap? A Systematic Search and Critical Review" International Journal of Environmental Research and Public Health 16, no. 9: 1516. https://doi.org/10.3390/ijerph16091516