The Impact of Policy Modifiable Factors on Inequalities in Rates of Child Dental Caries in Australia


 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
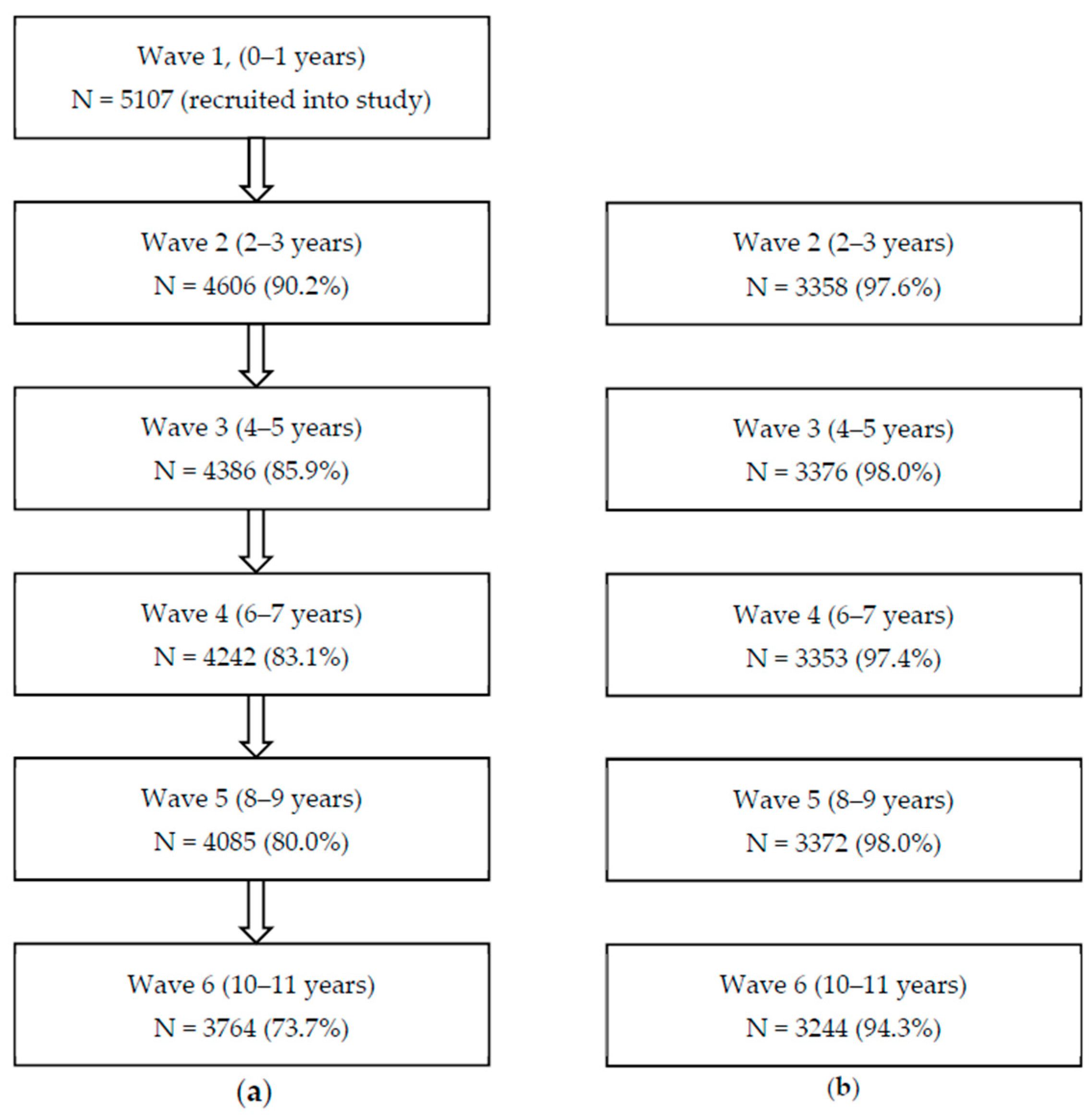
2.1. Data Source
2.2. Measures
2.2.1. Dental Caries Experience
2.2.2. Socioeconomic Position (SEP)
2.2.3. Policy Modifiable Oral Health Factors
2.2.4. Demographic Variables
2.3. Statistical Analysis
3. Results
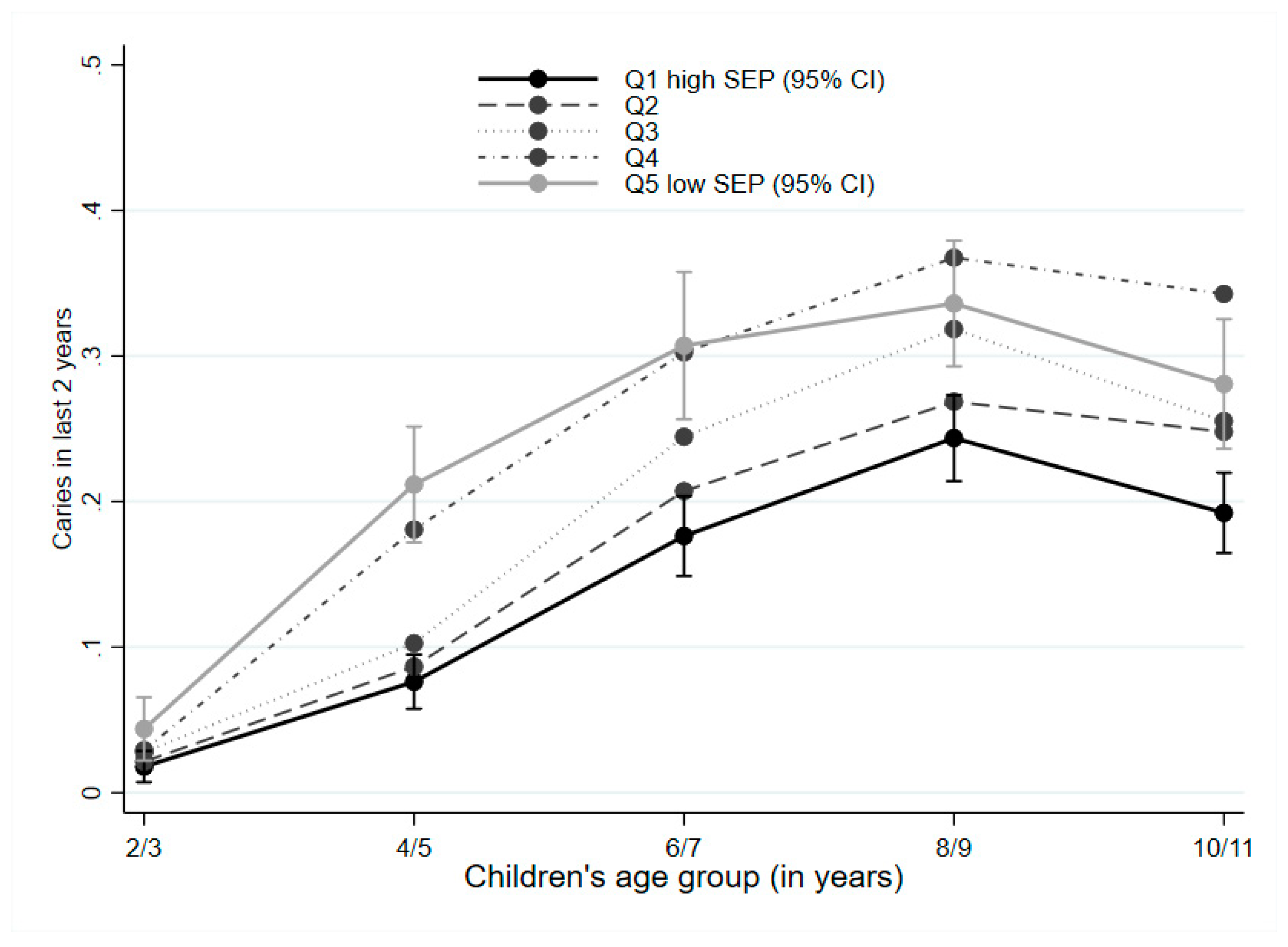
3.1. Dental Caries over Time
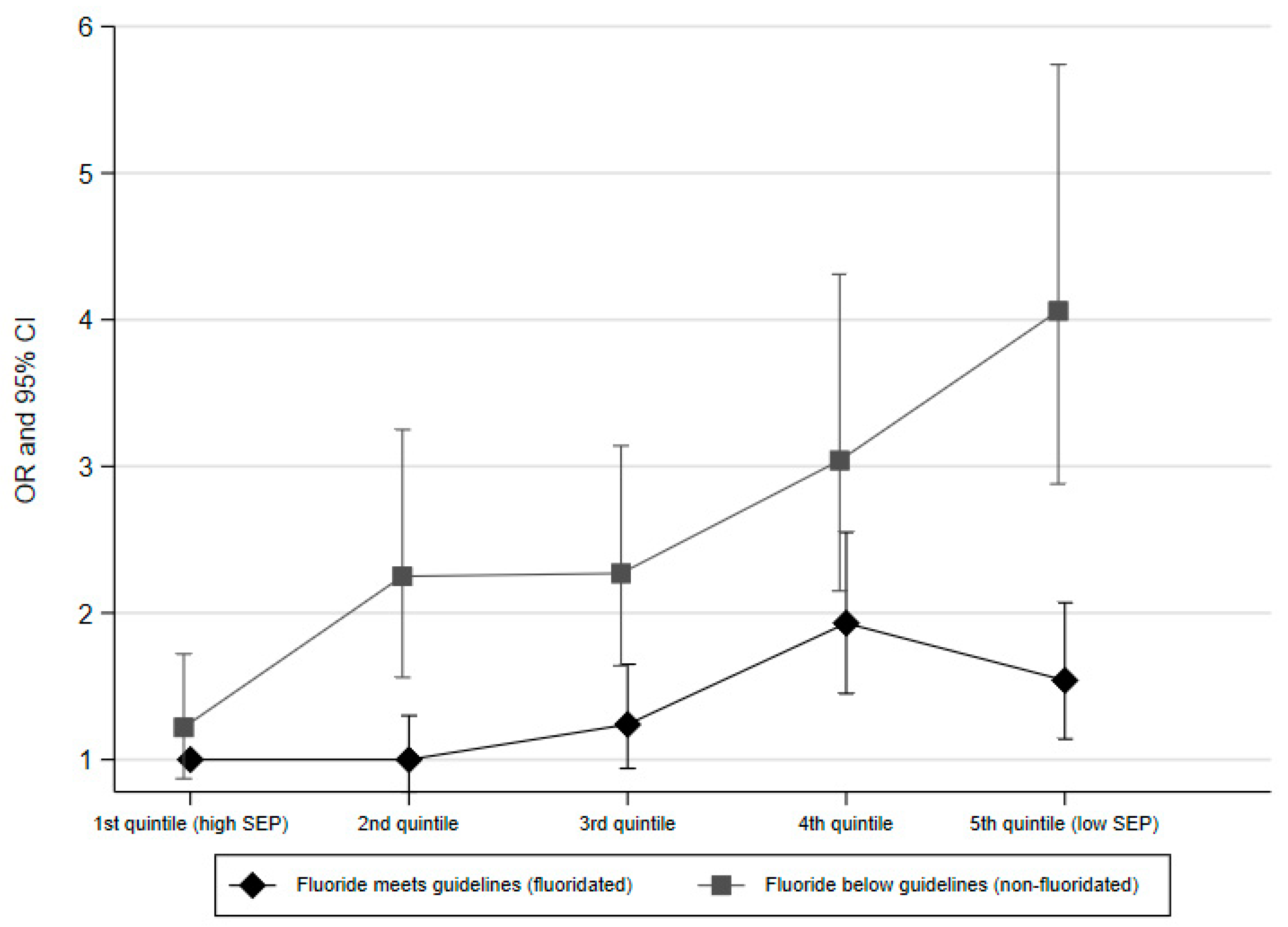
3.2. Factors Associated with Dental Caries Experience
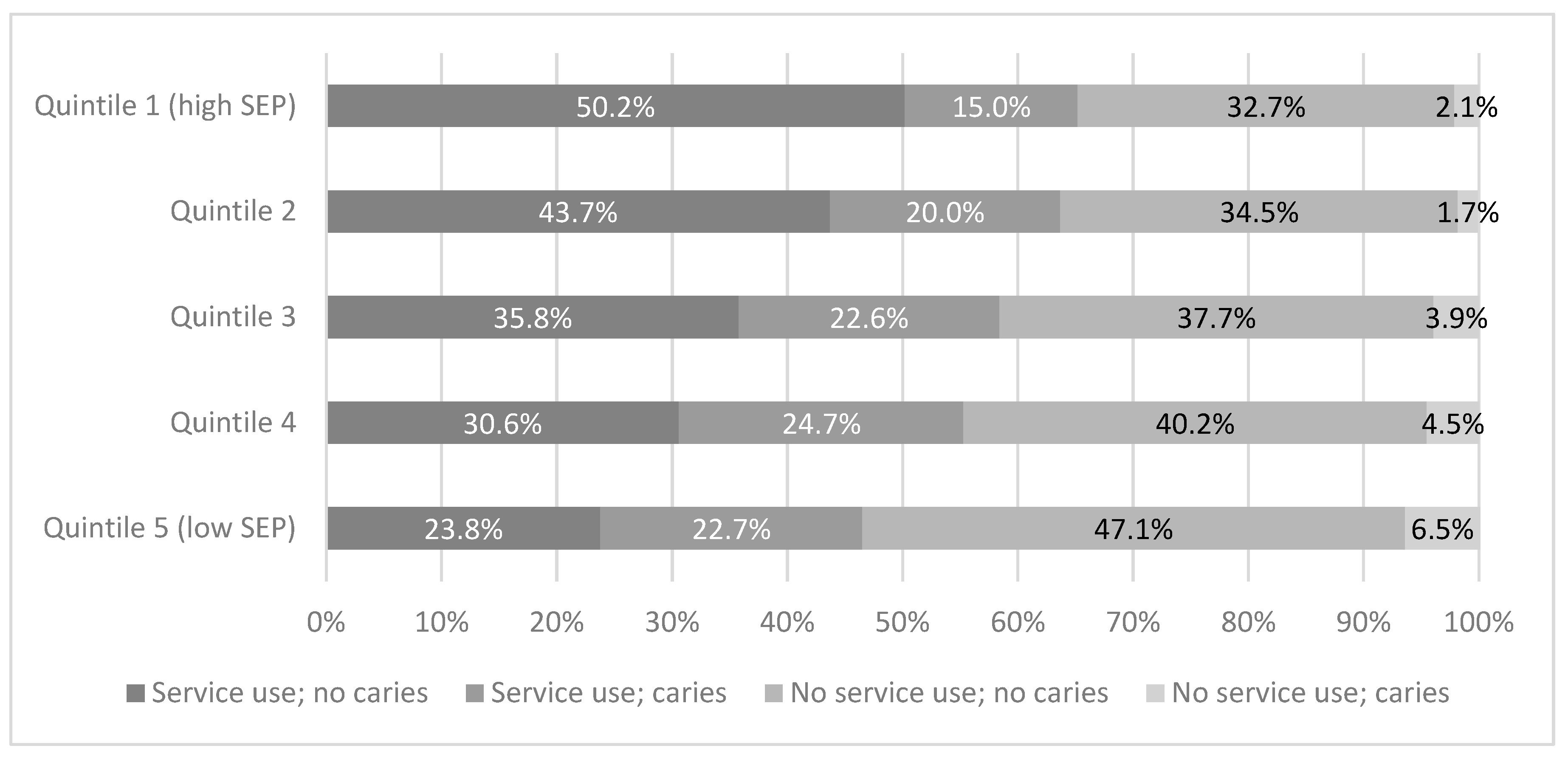
3.3. Service Use
4. Discussion
4.1. Fluoridation of the Water Supply
4.2. Oral Health Promotion Factors
4.3. Dental Services
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Petersen, P.; Bourgeois, D.; Ogawa, H.; Estupinan-Day, S.; Ndiaye, C. The Global Burden of Oral Diseases and Risks to Oral Health. Bull. World Health Organ. 2005, 83, 661–669. [Google Scholar] [PubMed]
- Bourgeois, D.M.; Llodra, J.C. Global Burden of Dental Condition Among Children in Nine Countries Participating in an International Oral Health Promotion Programme, 2012–2013. Int. Dent. J. 2014, 64, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Kassebaum, N.J.; Bernabe, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.; Marcenes, W. Global Burden of Untreated Caries: A Systematic Review and Metaregression. J. Dent. Res. 2015, 94, 650–658. [Google Scholar] [CrossRef]
- Kassebaum, N.J.; Smith, A.G.C.; Bernabe, E.; Fleming, T.D.; Reynolds, A.E.; Vos, T.; Murray, C.J.L.; Marcenes, W.; GBD 2015 Oral Health Collaborators. Global, Regional, and National Prevalence, Incidence, and Disability-Adjusted Life Years for Oral Conditions for 195 Countries, 1990–2015: A Systematic Analysis for the Global Burden of Diseases, Injuries, and Risk Factors. J. Dent. Res. 2017, 96, 380–387. [Google Scholar] [CrossRef]
- Harris, R.; Nicoll, A.; Adair, P.; Pine, C. Risk Factors for Dental Caries in Young Children: A Systematic Review of the Literature. Community Dent. Health 2004, 21, 71–85. [Google Scholar] [PubMed]
- Mount, G.; Hume, W. Preservation and Restoration of Tooth Structure, 2nd ed.; Knowledge Books and Software: Sandgate, Australia, 2005. [Google Scholar]
- Berkowitz, R. Causes, Treatment and Prevention of Early Childhood Caries: A Microbiologic Perspective. J. Can. Dent. Assoc. 2003, 69, 304–307. [Google Scholar]
- Qin, M.; Li, J.; Zhang, S.; Ma, W. Risk Factors for Severe Early Childhood Caries in Children Younger than 4 Years Old in Beijing, China. Pediatr. Dent. 2008, 30, 122–128. [Google Scholar]
- Leong, P. A Systematic Review of Risk Factors during First Year of Life for Early Childhood Caries. Int. J. Paediatr. Dent. 2013, 23, 235–250. [Google Scholar] [CrossRef]
- Goldfeld, S.; Cameron, A.; Doyle, K.; Drummond, B.; Kilpatrick, N.; Morris, P.; Phelan, C.; Thomas, E. The Royal Australasian College of Physicians Oral Health in Children and Young People Position Statement; Royal Australasian College of Physicians: Sydney, Australia, 2012. [Google Scholar]
- Casamassimo, P.S.; Thikkurissy, S.; Edelstein, B.L.; Maiorini, E. Beyond the Dmft: The Human and Economic Cost of Early Childhood Caries. J. Am. Dent. Assoc. 2009, 140, 650–657. [Google Scholar] [CrossRef]
- Ha, D.; Roberts-Thomson, K.; Arrow, P.; Peres, K.; Do, L.G.; Spencer, A.J. Children′s Oral Health Status in Australia, 2012-14. In Oral Health of Australian Children: The National Child Oral Health Study 2012-2014; Do, L., Spencer, A., Eds.; University of Adelaide Press: Adelaide, Australia, 2016. [Google Scholar]
- Chrisopoulos, S.; Harford, S.; Ellershaw, A. Oral Health and Dental Care in Australia: Key Facts and Figures 2015; Australian Institute of Health and Welfare: Canberra, Australia, 2016.
- Canadian Dental Association. The State of Oral Health in Canada; Canadian Dental Association: Ottawa, ON, Canada, 2017. [Google Scholar]
- World Dental Federation. FDI Data Hub for Global Oral Health. Available online: http://datahub.fdiworlddental.org/ (accessed on 30 April 2018).
- Mejia GC, A.N.; Ha, D.H.; Roberts-Thomson, K.F.; Ellershaw, A.C. Child Dental Health Survey Australia 2007: 30-Year Trends in Child Oral Health; AIHW: Canberra, Australia, 2012.
- Luzzi, L.; Ha, D.; Roberts-Thomson, K.; Chrisopoulos, S.; Armfield, J.; Do, L.G.; Spencer, A.J. Trends in Child Oral Health in Australia. In Oral Health of Australian Children: The National Child Oral Health Survey 2012–14; Do, L.G., Spencer, A.J., Eds.; University of Adelaide Press: Adelaide, Australia, 2016. [Google Scholar]
- Davies, G. Early Childhood Caries—A Synopsis. Community Dent. Oral Epidemiol. 1998, 26, 106–116. [Google Scholar] [CrossRef]
- Australian Health Ministers′ Conference; National Advisory Committee on Oral Health; South Australia Department of Health. Healthy Mouths, Healthy Lives: Australia’s National Oral Health Plan 2004–2013; South Australian Department of Health: Adelaide, Australia, 2004.
- Watt, R. Strategies and Approaches in Oral Disease Prevention and Health Promotion. Bull. World Health Organ. 2005, 83, 711–718. [Google Scholar]
- Kilpatrick, N.; Neumann, A.; Lucas, N.; Chapman, J.; Nicholson, J. Oral Health Inequalities in a National Sample of Australian Children Aged 2–3 and 6–7 Years. Aust. Dent. J. 2012, 57, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Psoter, W.; Pendrys, D.; Morse, D.; Zhang, H.; Mayne, S. Associations of Ethnicity/Race and Socioeconomic Status with Early Childhood Caries Patterns. J. Public Health Dent. 2006, 66, 23–29. [Google Scholar] [CrossRef]
- Reisine, S.; Psoter, W. Socioeconomic Status and Selected Behavioral Determinants as Risk Factors for Dental Caries. J. Dent. Educ. 2001, 65, 1009–1016. [Google Scholar] [PubMed]
- Mouradian, W.; Wehr, E.; Crall, J. Disparities in Children′s Oral Health and Access to Dental Care. JAMA 2000, 284, 2625–2631. [Google Scholar] [CrossRef]
- AIHW. Health Expenditure Australia 2016–17; Health and Welfare Expenditure Series No. 64. Cat. No. HWE 74; AIHW: Canberra, Australia, 2018.
- Department of Health. The Child Dental Benefits Schedule. Available online: http://www.health.gov.au/internet/main/publishing.nsf/content/childdental (accessed on 27 August 2018).
- Department of Health. Report on the Third Review of the Dental Benefits Act 2008; Department of Health: Canberra, Australia, 2016.
- Australian Institute of Health and Welfare. A Discussion of Public Dental Waiting Times Information in Australia: 2013–14 to 2016–17. Cat No. DEN 230; Australian Institute of Health and Welfare: Canberra, Australia, 2018.
- Calache, J.; Hopcraft, M.; Martin, J. Minimum Intervention Dentistry—A New Horizon in Public Oral Health Care. Aust. Dent. J. 2013, 58, 17–25. [Google Scholar] [CrossRef]
- Jones, C.; Worthington, H. The Relationship between Water Fluoridation and Socioeconomic Deprivation on Tooth Decay in 5-Year-Old Children. Br. Dent. J. 1999, 186, 397–400. [Google Scholar] [CrossRef]
- Armfield, J. Public Water Fluoridation and Dental Health in New South Wales. Aust. N. Z. J. Public Health 2005, 29, 477–483. [Google Scholar] [CrossRef] [PubMed]
- National Health and Medical Research Council. A Systematic Review of the Efficacy and Safety of Fluoridation: Part A: Review of Methodology and Results; Australian Government: Canberra, Australia, 2007.
- CDC. Ten Great Public Health Achievements—United States, 1900–1999. MMWR Morb. Mortal. Wkly. Rep. 1999, 48, 241–243. [Google Scholar]
- National Health and Medical Research Council (NHMRC). NHMRC Public Statement 2017: Water Fluoridation and Human Health in Australia; National Health and Medical Research Council (NHMRC): Canberra, Australia, 2017.
- Australian Institute for Health and Welfare. Oral Health and Access to Dental Care in Rural and Remote Areas of Australia; Australian Institute for Health and Welfare: Adelaide, Australia, 1999.
- Ha, D.; Amarasena, N.; Crocombe, L. The Dental Health of Australia’s Children by Remoteness: Child Dental Health Survey Australia 2009; Australian Institute of Health and Welfare: Canberra, Australia, 2009.
- Petersen, P. The World Oral Health Report 2003: Continuous Improvement of Oral Health in the 21st Century—The Approach of the WHO Global Oral Health Programme. Community Dent. Oral Epidemiol. 2003, 31, 3–24. [Google Scholar] [CrossRef]
- Northridge, M.E.; Schrimshaw, E.W.; Estrada, I.; Greenblatt, A.P.; Metcalf, S.S.; Kunzel, C. Intergenerational and Social Interventions to Improve Children′s Oral Health. Dent. Clin. N. Am. 2017, 61, 533–548. [Google Scholar] [CrossRef] [PubMed]
- Seow, W.K. Early Childhood Caries. Pediatr. Clin. North Am. 2018, 65, 941–954. [Google Scholar] [CrossRef] [PubMed]
- Marinho, V.C.C.; Chong, L.Y.; Worthington, H.V.; Walsh, T. Fluoride Mouthrinses for Preventing Dental Caries in Children and Adolescents. Cochrane Database Syst. Rev. 2016, 7, CD002284. [Google Scholar] [CrossRef]
- Soloff, C.; Lawrence, D.; Misson, S.; Johnstone, R. LSAC Technical Paper No. 3. Wave 1 Weighting and Non-Response; Australian Institute of Family Studies: Melbourne, Australia, 2006.
- Soloff, C.; Lawrence, D.; Johnstone, R. LSAC Technical Paper No. 1. Sample Design; Australian Institute of Family Studies: Melbourne, Australia, 2005.
- Gray, M.; Smart, D. Growing up in Australia: The Longitudinal Study of Australian Children is Now Walking and Talking. Fam. Matt. 2008, 79, 5–13. [Google Scholar]
- Talekar, B.; Rozier, R.; Slade, G.; Ennett, S. Parental Perceptions of Their Preschool-Aged Children′s Oral Health. J. Am. Dent. Assoc. 2005, 136, 364–372. [Google Scholar] [CrossRef]
- Locker, D. Validity of Single-Item Parental Ratings of Child Oral Health. Int. J. Paediatr. Dent. 2008, 18, 407–414. [Google Scholar] [CrossRef]
- Lim, M.; Crocombe, L.A.; Do, L.G. Perceptions of Dental Treatment Need in Australian-Born and Migrant Populations. Eur. J. Oral Sci. 2017, 125, 479–486. [Google Scholar] [CrossRef]
- Blakemore, T.; Strazdins, L.; Gibbings, J. Measuring Family Socioeconomic Position. Aust. Soc. Policy 2009, 8, 121–168. [Google Scholar]
- Department of Health and Aged Care. Measuring Remoteness: Accessibility/Remoteness Index of Australia (ARIA); Commonwealth of Australia: Canberra, Australia, 2001.
- Do, L.G.; Ha, D.H.; Roberts-Thomson, K.F.; Jamieson, L.; Peres, M.A.; Spencer, A.J. Race—And Income-Related Inequalities in Oral Health of Australian Children by Fluoridation Status. J. Dent. Res. Clin. Trans. Res. 2018, 3, 170–179. [Google Scholar] [CrossRef] [PubMed]
- Schluter, P.J.; Lee, M. Water Fluoridation and Ethnic Inequities in Dental Caries Profiles of New Zealand Children Aged 5 and 12–13 Years: Analysis of National Cross-Sectional Registry Databases for the Decade 2004–2013. BMC Oral Health 2016, 16, 21. [Google Scholar] [CrossRef]
- Dogar, F.; Kruger, E.; Dyson, K.; Tennant, M. Oral Health of Pre-School Children in Rural and Remote Western Australia. Rural Remote Health 2011, 11, 1869. [Google Scholar] [PubMed]
- John, J.R.; Mannan, H.; Nargundkar, S.; D′Souza, M.; Do, L.G.; Arora, A. Predictors of Dental Visits among Primary School Children in the Rural Australian Community of Lithgow. BMC Health Serv. Res. 2017, 17, 264. [Google Scholar] [CrossRef] [PubMed]
- Carlisle, K.; Larkins, S.; Croker, F. Disparities in Dental Health of Rural Australians: Hospitalisation Rates and Utilisation of Public Dental Services in Three Communities in North Queensland. Rural Remote Health 2017, 17, 3807. [Google Scholar] [CrossRef] [PubMed]
- Llena, C.; Calabuig, E. Risk Factors Associated with New Caries Lesions in Permanent First Molars in Children: A 5-Year Historical Cohort Follow-Up Study. Clin. Oral Investig. 2018, 22, 1579–1586. [Google Scholar] [CrossRef] [PubMed]
- Pita-Fernández, S.; Pombo-Sánchez, A.; Suárez-Quintanilla, J.; Novio-Mallón, S.; Rivas-Mundiña, B.; Pértega-Díaz, S. Clinical Relevance of Tooth Brushing in Relation to Dental Caries. Aten. Pr. 2010, 42, 372–379. [Google Scholar] [CrossRef]
- Wagner, Y.; Heinrich-Weltzien, R. Evaluation of a Regional German Interdisciplinary Oral Health Programme for Children from Birth to 5 Years of Age. Clin. Oral Investig. 2017, 21, 225–235. [Google Scholar] [CrossRef]
- Cakar, T.; Harrison-Barry, L.; Pukallus, M.L.; Kazoullis, S.; Seow, W.K. Caries Experience of Children in Primary Schools with Long-Term Tooth Brushing Programs: A Pilot Australian Study. Int. J. Dent. Hyg. 2018, 16, 233–240. [Google Scholar] [CrossRef]
- Dos Santos, A.P.P.; De Oliveira, B.H.; Nadanovsky, P. A Systematic Review of the Effects of Supervised Toothbrushing on Caries Incidence in Children and Adolescents. Int. J. Paediatr. Dent. 2018, 28, 3–11. [Google Scholar] [CrossRef]
- Bourdeaudhuij, I.D.; Oost, P.V. Personal and Family Determinants of Dietary Behaviour in Adolescents and Their Parents. Psychol. Health 2000, 15, 751–770. [Google Scholar] [CrossRef]
- Martins, C.C.; Oliveira, M.J.; Pordeus, I.A.; Paiva, S.M. Comparison between Observed Children′s Tooth Brushing Habits and Those Reported by Mothers. BMC Oral Health 2011, 11, 22. [Google Scholar] [CrossRef]
- Sanzone, L.A.; Lee, J.Y.; Divaris, K.; DeWalt, D.A.; Baker, A.D.; Vann, W.F., Jr. A Cross Sectional Study Examining Social Desirability Bias in Caregiver Reporting of Children′s Oral Health Behaviors. BMC Oral Health 2013, 13, 24. [Google Scholar] [CrossRef] [PubMed]
- Nambiar, D.; Mander, H. Inverse Care and the Role of the State: The Health of the Urban Poor. Bull. World Health Organ. 2017, 95, 152–153. [Google Scholar] [CrossRef] [PubMed]
- Hart, J.T. The Inverse Care Law. Lancet 1971, 1, 405–412. [Google Scholar] [CrossRef]
- Anikeeva, O.; Brennan, D.S.; Teusner, D.N. Household Income Modifies the Association of Insurance and Dental Visiting. BMC Health Serv. Res. 2013, 13, 432. [Google Scholar] [CrossRef]
- Shaban, R.; Kassim, S.; Sabbah, W. Socioeconomic Inequality in the Provision of Specific Preventive Dental Interventions among Children in the UK: Children′s Dental Health Survey 2003. Br. Dent. J. 2017, 222, 865–869. [Google Scholar] [CrossRef] [PubMed]
- National Health Service. Get Help with Dental Costs. Available online: https://www.nhs.uk/using-the-nhs/help-with-health-costs/get-help-with-dental-costs/ (accessed on 25 March 2019).
- Weyant, R.; Manz, M.; Corby, P.; Rustveld, L.; Close, J. Factors Associated with Parents′ and Adolescents′ Perceptions of Oral Health and Need for Dental Treatment. Community Dent. Oral Epidemiol. 2007, 35, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Family Studies. The Longitudinal Study of Australian Children Data User Guide—November 2015; Australian Institute of Family Studies: Melbourne, Australia, 2015.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Wave 2 | Wave 3 | Wave 4 | Wave 5 | Wave 6 | |
|---|---|---|---|---|---|
| Age in months (mean (SD)) | 33.8 (4.0) | 57.6 (3.3) | 81.9 (4.4) | 107.2 (4.5) | 131.1 (5.2) |
| Gender (female) (%) 1 | 48.4 | 48.4 | 48.4 | 48.4 | 48.4 |
| Caries experience | |||||
| No caries experience in last two years (%) | 97.2 | 86.8 | 75.3 | 69.3 | 73.5 |
| Had caries experience in last two years (%) | 2.8 | 13.2 | 24.7 | 30.7 | 26.5 |
| SEP 2 | |||||
| Quintile 1 (high SEP) to Quintile 5 (low SEP) (%) | Each 20.0 | 20.0 | 20.0 | 20.0 | 20.0 |
| Remoteness | |||||
| Major cities (%) | 68.5 | 68.0 | 66.8 | 66.1 | 65.7 |
| Inner regional (%) | 19.0 | 20.3 | 21.1 | 22.2 | 22.5 |
| Outer regional (%) | 11.2 | 10.6 | 10.9 | 10.5 | 10.6 |
| Remote (%) | 0.8 | 0.7 | 0.8 | 0.9 | 0.9 |
| Very remote (%) | 0.4 | 0.4 | 0.3 | 0.4 | 0.4 |
| Water fluoride level: Residential area in infancy 1 | |||||
| ≤ 0.6 mg/L (non-fluoridated) (%) | 28.1 | 28.1 | 28.1 | 28.1 | 28.1 |
| 0.6 mg/L to 1.1 mg/L (fluoridated) (%) | 71.9 | 71.9 | 71.9 | 71.9 | 71.9 |
| Sugary diet 3 (mean (SD)) | 2.2 (1.9) | 2.2 (1.7) | 2.1 (1.6) | 2.1 (1.5) | 2.2 (2.0) |
| Frequency of teeth brushing 4 | |||||
| Twice a day or more (%) | 42.8 | 63.7 5 | 63.7 | 64.5 | 62.7 |
| Less than twice a day (%) | 57.2 | 36.4 | 36.4 | 35.5 | 37.3 |
| Age started cleaning teeth 1 | |||||
| 0–<7 months (%) | 20.4 | 20.4 | 20.4 | 20.4 | 20.4 |
| 7–12 months (%) | 57.1 | 57.1 | 57.1 | 57.1 | 57.1 |
| 13–24 months (%) | 21.7 | 21.7 | 21.7 | 21.7 | 21.7 |
| 25–36 months (%) | 0.7 | 0.7 | 0.7 | 0.7 | 0.7 |
| Dental service use in previous 12 months (%) 6 | |||||
| Caries in last 2 years, no service use | 3.7 | 3.7 | 4.6 | ||
| Caries in last 2 years, service use | 9.4 | 21.0 | 26.1 | ||
| No caries in last 2 years, no service use | 60.5 | 38.6 | 32.3 | ||
| No caries in last 2 years, service use | 26.3 | 36.7 | 37.0 |
| Adj OR 1 | 95% CI | p | ||
|---|---|---|---|---|
| Lower | Upper | |||
| SEP | ||||
| Quintile 1 (high SEP) | 1.00 | - | - | - |
| Quintile 2 | 1.16 | 0.93 | 1.44 | 0.196 |
| Quintile 3 | 1.34 | 1.06 | 1.69 | 0.013 |
| Quintile 4 | 1.96 | 1.55 | 2.49 | <0.001 |
| Quintile 5 (low SEP) | 1.92 | 1.49 | 2.46 | <0.001 |
| Water fluoride level: Residential area in infancy | ||||
| ≤ 0.6 mg/L (non-fluoridated) | 1.0 | - | - | - |
| 0.6 mg/L to 1.1 mg/L (fluoridated) | 0.53 | 0.43 | 0.64 | <0.001 |
| Remoteness | ||||
| Major cities | 1.0 | - | - | - |
| Inner regional | 1.09 | 0.90 | 1.32 | 0.393 |
| Outer regional | 1.33 | 1.06 | 1.66 | 0.013 |
| Remote | 0.82 | 0.44 | 1.52 | 0.529 |
| Very remote | 2.41 | 1.02 | 5.78 | 0.047 |
| Frequency of teeth brushing | ||||
| Twice a day or more | 1.0 | |||
| Less than twice a day | 0.88 | 0.76 | 1.02 | 0.088 |
| Age started cleaning teeth | ||||
| 0–<7 months | 1.0 | - | - | - |
| 7–12 months | 0.94 | 0.77 | 1.17 | 0.595 |
| 13–24 months | 1.01 | 0.77 | 1.32 | 0.958 |
| 25–36 months | 1.21 | 0.38 | 3.89 | 0.749 |
| Sugary diet | 1.02 | 0.97 | 1.06 | 0.459 |
| Age in months | 1.02 | 1.02 | 1.03 | <0.001 |
| Adj OR 1 | 95% CI | p | ||||
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| SEP | + | Water fluoride level | ||||
| Quintile 1 (high SEP) | + | Fluoridated | 1.00 | - | - | - |
| Quintile 2 | + | Fluoridated | 1.00 | 0.78 | 1.30 | 0.975 |
| Quintile 3 | + | Fluoridated | 1.24 | 0.94 | 1.65 | 0.129 |
| Quintile 4 | + | Fluoridated | 1.93 | 1.45 | 2.55 | <0.001 |
| Quintile 5 (low SEP) | + | Fluoridated | 1.54 | 1.14 | 2.07 | 0.005 |
| Quintile 1 (high SEP) | + | Non-fluoridated | 1.22 | 0.87 | 1.72 | 0.251 |
| Quintile 2 | + | Non-fluoridated | 2.25 | 1.56 | 3.25 | <0.001 |
| Quintile 3 | + | Non-fluoridated | 2.27 | 1.64 | 3.14 | <0.001 |
| Quintile 4 | + | Non-fluoridated | 3.04 | 2.15 | 4.31 | <0.001 |
| Quintile 5 (low SEP) | + | Non-fluoridated | 4.06 | 2.88 | 5.74 | <0.001 |
| Remoteness | ||||||
| Major cities | 1.0 | - | - | - | ||
| Inner regional | 1.09 | 0.89 | 1.32 | 0.399 | ||
| Outer regional | 1.33 | 1.06 | 1.65 | 0.013 | ||
| Remote | 0.82 | 0.45 | 1.50 | 0.516 | ||
| Very remote | 2.33 | 1.00 | 5.42 | 0.049 | ||
| Frequency of teeth brushing | ||||||
| Twice a day or more | 1.0 | - | - | - | ||
| Less than twice a day | 0.88 | 0.76 | 1.02 | 0.085 | ||
| Age started cleaning teeth | ||||||
| 0–<7 months | 1.0 | - | - | - | ||
| 7–12 months | 0.94 | 0.76 | 1.16 | 0.580 | ||
| 13–24 months | 1.00 | 0.77 | 1.31 | 0.979 | ||
| 25–36 months | 1.19 | 0.37 | 3.79 | 0.765 | ||
| Sugary diet | 1.01 | 0.97 | 1.07 | 0.413 | ||
| Age in months | 1.02 | 1.02 | 1.03 | <0.001 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goldfeld, S.; Francis, K.L.; Hoq, M.; Do, L.; O’Connor, E.; Mensah, F. The Impact of Policy Modifiable Factors on Inequalities in Rates of Child Dental Caries in Australia. Int. J. Environ. Res. Public Health 2019, 16, 1970. https://doi.org/10.3390/ijerph16111970
Goldfeld S, Francis KL, Hoq M, Do L, O’Connor E, Mensah F. The Impact of Policy Modifiable Factors on Inequalities in Rates of Child Dental Caries in Australia. International Journal of Environmental Research and Public Health. 2019; 16(11):1970. https://doi.org/10.3390/ijerph16111970
Chicago/Turabian StyleGoldfeld, Sharon, Kate Louise Francis, Monsurul Hoq, Loc Do, Elodie O’Connor, and Fiona Mensah. 2019. "The Impact of Policy Modifiable Factors on Inequalities in Rates of Child Dental Caries in Australia" International Journal of Environmental Research and Public Health 16, no. 11: 1970. https://doi.org/10.3390/ijerph16111970