Effectiveness of a Combined Intervention on Psychological and Physical Capacities of Frail Older Adults: A Cluster Randomized Controlled Trial

 , , , ,
, , , ,  , ,
, ,
Abstract
:1. Introduction
Intervention Rational
2. Materials and Methods
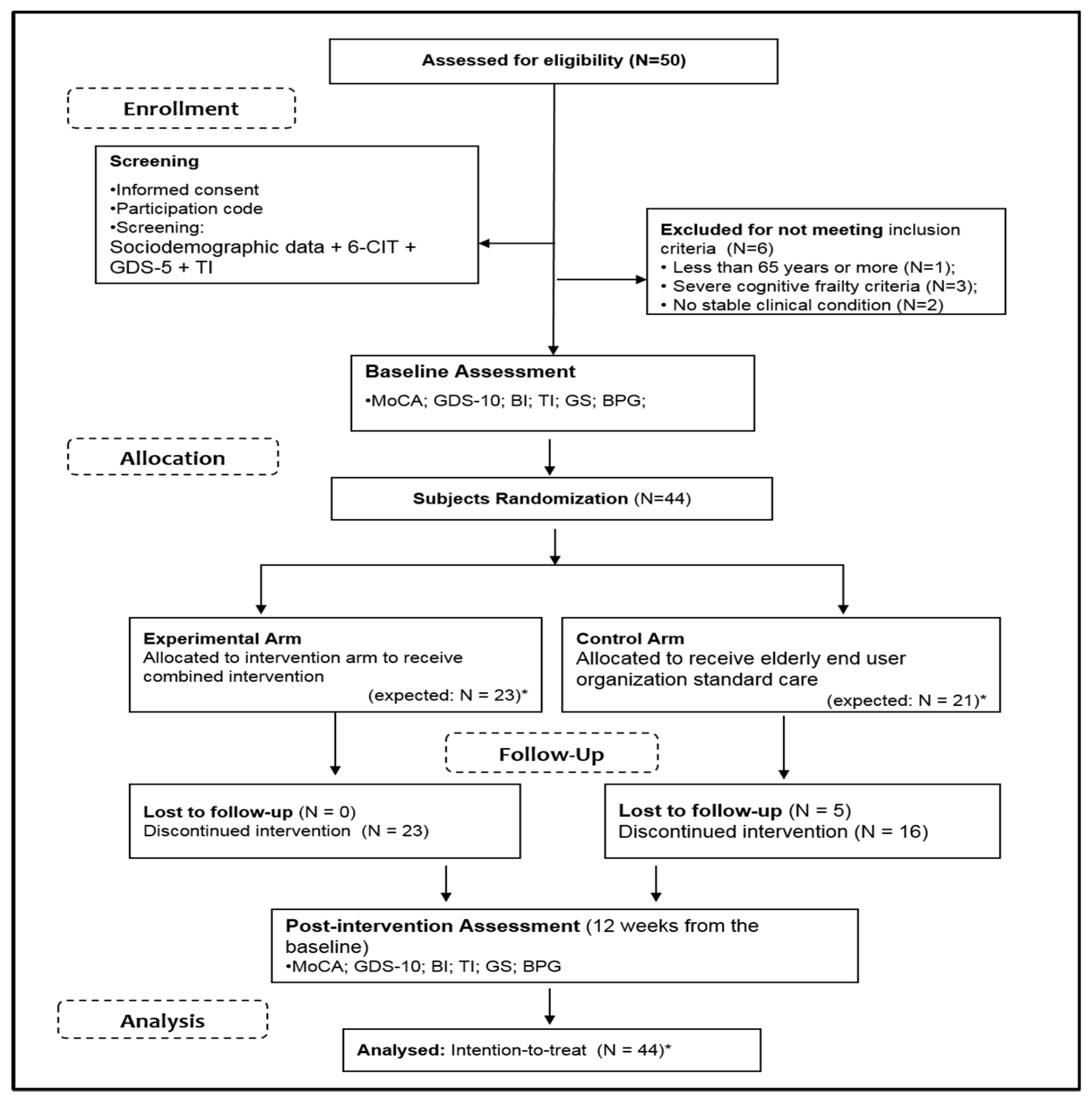
2.1. Aims, Design and Setting
2.2. Recruitment and Sampling
- (i)
- aged 65 years or above;
- (ii)
- the ability to consent their participation in the study in an informed manner;
- (iii)
- the presence of medical clinical conditions that allow them participation on CI;
- (iv)
- (v)
- (vi)
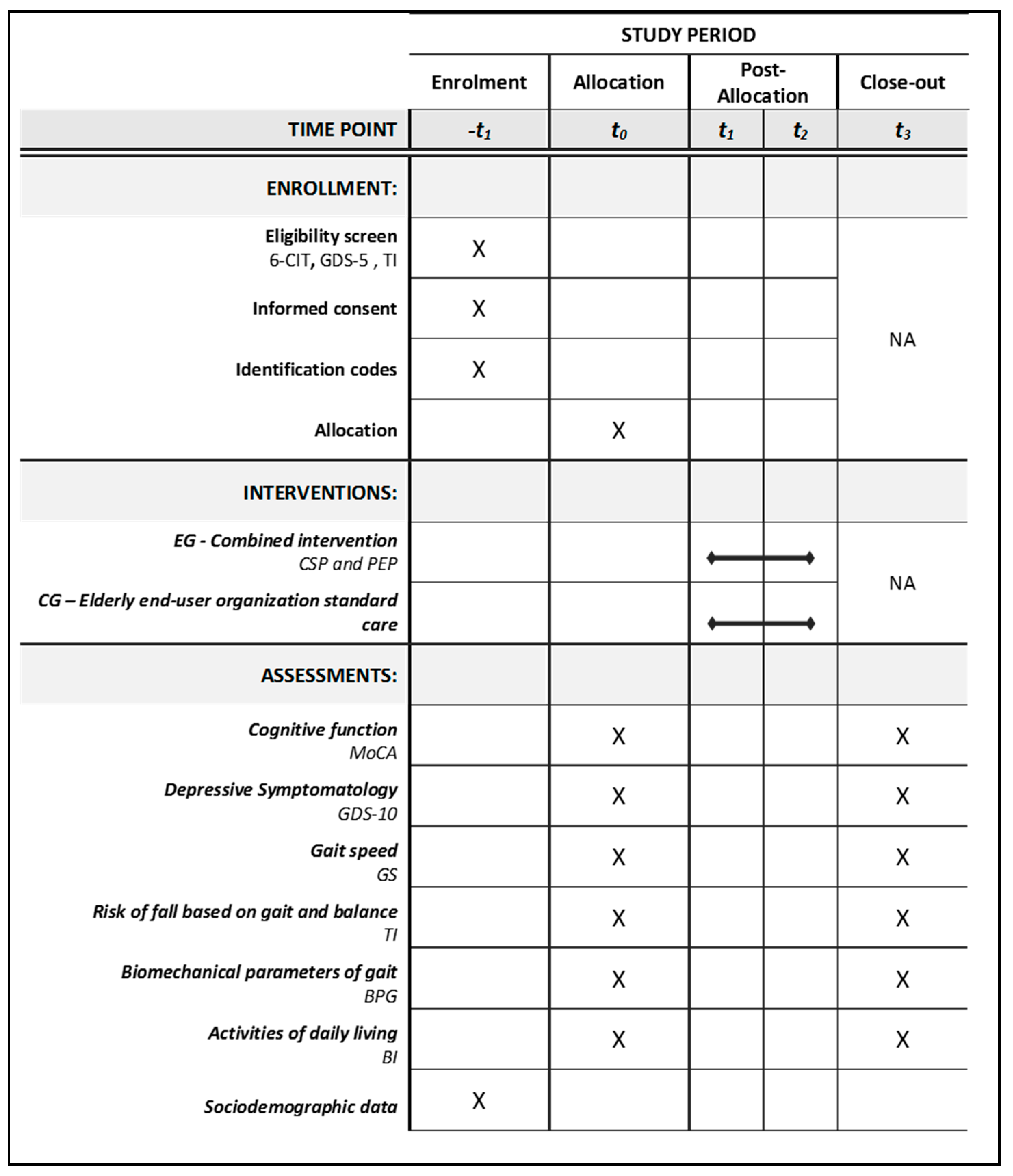
2.3. Randomization and Assessment
2.4. Intervention
2.4.1. Cognitive Stimulation Component
2.4.2. Physical Exercise Component
2.5. Instruments
2.5.1. Sociodemographic Data
2.5.2. Primary Outcomes
2.5.3. Secondary Outcome
2.6. Statistical Analysis
2.7. Ethical Considerations
3. Results
3.1. Baseline Assessment
3.2. Post-Intervention Assessment
3.2.1. Between-Group Analysis of Primary and Secondary Outcomes
3.2.2. Within-Group Analysis of Primary and Secondary Outcomes
4. Discussion
5. Forces and Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. World Report on Ageing and Health; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Panza, F.; Solfrizzi, V.; Barulli, M.R.; Santamato, A.; Seripa, D.; Pilotto, A.; Logroscino, G. Cognitive Frailty: A Systematic Review of Epidemiological and Neurobiological Evidence of an Age-Related Clinical Condition. Rejuvenation Res. 2015, 18, 389–412. [Google Scholar] [CrossRef] [PubMed]
- Chodzko-Zajko, W.J.; Proctor, D.N.; Fiatarone Singh, M.A.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. Exercise and Physical Activity for Older Adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef] [PubMed]
- Bauman, A.; Merom, D.; Bull, F.C.; Buchner, D.M.; Fiatarone Singh, M.A. Updating the Evidence for Physical Activity: Summative Reviews of the Epidemiological Evidence, Prevalence, and Interventions to Promote “Active Aging”. GERONT 2016, 56, S268–S280. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older Adults: Evidence for a Phenotype. J. Gerontol. Ser. A Biol. Sci. Med Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef] [PubMed]
- Gobbens, R.J.; van Assen, M.A.; Luijkx, K.G.; Schols, J.M. Testing an Integral Conceptual Model of Frailty: Testing an Integral Conceptual Model of Frailty. J. Adv. Nurs. 2012, 68, 2047–2060. [Google Scholar] [CrossRef] [PubMed]
- Langlois, F.; Vu, T.T.M.; Kergoat, M.J.; Chassé, K.; Dupuis, G.; Bherer, L. The Multiple Dimensions of Frailty: Physical Capacity, Cognition, and Quality of Life. Int. Psychogeriatr. 2012, 24, 1429–1436. [Google Scholar] [CrossRef] [PubMed]
- Gwyther, H.; Bobrowicz-Campos, E.; Luis Alves Apóstolo, J.; Marcucci, M.; Cano, A.; Holland, C.A. Realist Review to Understand the Efficacy and Outcomes of Interventions Designed to Minimise, Reverse or Prevent the Progression of Frailty. Health Psychol. Rev. 2018, 12, 382–404. [Google Scholar] [CrossRef] [PubMed]
- Levers, M.J.; Estabrooks, C.A.; Ross Kerr, J.C. Factors Contributing to Frailty: Literature Review. J. Adv. Nurs. 2006, 56, 282–291. [Google Scholar] [CrossRef]
- Apóstolo, J.; Cooke, R.; Bobrowicz-Campos, E.; Santana, S.; Marcucci, M.; Cano, A.; Vollenbroek-Hutten, M.; Germini, F.; Holland, C. Predicting Risk and Outcomes for Frail Older Adults: An Umbrella Review of Frailty Screening Tools. JBI Database Syst. Rev. Implement. Rep. 2017, 15, 1154–1208. [Google Scholar] [CrossRef]
- Theill, N.; Schumacher, V.; Adelsberger, R.; Martin, M.; Jäncke, L. Effects of Simultaneously Performed Cognitive and Physical Training in Older Adults. BMC Neurosci. 2013, 14, 103. [Google Scholar] [CrossRef]
- Apóstolo, J.; Cooke, R.; Bobrowicz-Campos, E.; Santana, S.; Marcucci, M.; Cano, A.; Vollenbroek-Hutten, M.; Germini, F.; D’Avanzo, B.; Gwyther, H.; et al. Effectiveness of Interventions to Prevent Pre-Frailty and Frailty Progression in Older Adults: A Systematic Review. JBI Database Syst. Rev. Implement. Rep. 2018, 16, 140–232. [Google Scholar] [CrossRef] [PubMed]
- Reeves, N.D.; Narici, M.V.; Maganaris, C.N. Musculoskeletal Adaptations to Resistance Training in Old Age. Man. Ther. 2006, 11, 192–196. [Google Scholar] [CrossRef] [PubMed]
- de Labra, C.; Guimaraes-Pinheiro, C.; Maseda, A.; Lorenzo, T.; Millán-Calenti, J.C. Effects of Physical Exercise Interventions in Frail Older Adults: A Systematic Review of Randomized Controlled Trials. BMC Geriatr. 2015, 15, 154. [Google Scholar] [CrossRef] [PubMed]
- Apostolo, J.; Holland, C.; O’Connell, M.D.L.; Feeney, J.; Tabares-Seisdedos, R.; Tadros, G.; Campos, E.; Santos, N.; Robertson, D.A.; Marcucci, M.; et al. Mild Cognitive Decline. A Position Statement of the Cognitive Decline Group of the European Innovation Partnership for Active and Healthy Ageing (EIPAHA). Maturitas 2016, 83, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Tardif, S.; Simard, M. Cognitive Stimulation Programs in Healthy Elderly: A Review. Int. J. Alzheimer’s Dis. 2011, 2011, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Moretti, F.; De Ronchi, D.; Bernabei, V.; Marchetti, L.; Ferrari, B.; Forlani, C.; Negretti, F.; Sacchetti, C.; Atti, A.R. Pet Therapy in Elderly Patients with Mental Illness: Data from an Italian Case-Control Study. Psychogeriatrics 2011, 11, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Olsen, C.; Pedersen, I.; Bergland, A.; Enders-Slegers, M.J.; Ihlebæk, C. Engagement in Elderly Persons with Dementia Attending Animal-Assisted Group Activity. Dementia 2019, 18, 245–261. [Google Scholar] [CrossRef]
- Dookie, A.L. Perspectives of Animal Assisted Activities on Empowerment, Self-Esteem and Communication with Caregivers on Elders in Retirement Homes. Act. Adapt. Aging 2013, 37, 189–212. [Google Scholar] [CrossRef]
- Pattison, V. Implementation of an Animal Assisted Activity Program into a Rural Long-Term Care Facility to Increase the Perceived Quality of Life of Residents. Ph.D. Thesis, Regis University, Denver, CO, USA, 2015. [Google Scholar]
- Melo, A. Influência Das Atividades Assistidas Com Animais Sobre o Comportamento de Idosos Institucionalizados. 2017. Available online: http://www.animasportugal.org/uploads/instituicao_uploads/%C3%82NIMAS%20Informa%20n%C2%BA%201.pdf (accessed on 11 December 2018).
- Kelaiditi, E.; Cesari, M.; Canevelli, M.; Abellan van Kan, G.; Ousset, P.-J.; Gillette-Guyonnet, S.; Ritz, P.; Duveau, F.; Soto, M.E.; Provencher, V.; et al. Cognitive Frailty: Rational and Definition from an (I.A.N.A./I.A.G.G.) International Consensus Group. J. Nutr. Health Aging 2013, 17, 726–734. [Google Scholar] [CrossRef]
- Mewborn, C.M.; Lindbergh, C.A.; Stephen Miller, L. Cognitive Interventions for Cognitively Healthy, Mildly Impaired, and Mixed Samples of Older Adults: A Systematic Review and Meta-Analysis of Randomized-Controlled Trials. Neuropsychol. Rev. 2017, 27, 403–439. [Google Scholar] [CrossRef]
- Brooke, P.; Bullock, R. Validation of a 6 Item Cognitive Impairment Test with a View to Primary Care Usage. Int. J. Geriatr. Psychiatry 1999, 14, 936–940. [Google Scholar] [CrossRef]
- Apóstolo, J.L.A.; Paiva, D.; Silva, R.C.G.; Santos, E.J.F.; Schultz, T.J. Adaptation and Validation into Portuguese Language of the Six-Item Cognitive Impairment Test (6CIT). Aging Ment. Health 2018, 22, 1190–1195. [Google Scholar] [CrossRef] [PubMed]
- Apóstolo, J.; Loureiro, L.; Reis, I.; Silva, I.; Cardoso, D.; Sfetcu, R. Contribution to the Adaptation of the Geriatric Depression Scale-15 into Portuguese. Rev. Enf. Ref. 2014, 65–73. [Google Scholar] [CrossRef]
- Apóstolo, J.; Bobrowicz-Campos, E.; Reis, I.; Henriques, S.; Correia, C. Screening Capacity of Geriatric Depression Scale with 10 and 5 Items. Rev. Enf. Ref. 2018, 29–40. [Google Scholar] [CrossRef]
- Yesavage, J.A.; Brink, T.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and Validation of a Geriatric Depression Screening Scale: A Preliminary Report. J. Psychiatr. Res. 1982, 17, 37–49. [Google Scholar] [CrossRef]
- Yesavage, J.A.; Sheikh, J.I. Geriatric Depression Scale (GDS): Recent Evidence and Development of a Shorter Version. Clin. Gerontol. 1986, 5, 165–173. [Google Scholar] [CrossRef]
- Tinetti, M.E. Performance-Oriented Assessment of Mobility Problems in Elderly Patients. J. Am. Geriatr. Soc. 1986, 34, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Petiz, E.M. A Actividade Física, Equilíbrio e Quedas. um Estudo em Idosos Institucionalizados. Unpublished Master’s Thesis, Faculdade de Ciências do Desporto e de Educação Física da Universidade do Porto, Porto, Portugal, 2002. [Google Scholar]
- Morrison, M.L. Health Benefits of Animal-Assisted Interventions. Complement. Health Pract. Rev. 2007, 12, 51–62. [Google Scholar] [CrossRef]
- Scheibeck, R.; Pallauf, M.; Stellwag, C.; Seeberger, B. Elderly People in Many Respects Benefit from Interaction with Dogs. Eur. J. Med. Res. 2011, 16, 557. [Google Scholar] [CrossRef]
- Wohlfarth, R.; Sandstedt, L.; Wyższa, S.; Pedagogiczna, I.; Janusza, K. Wydawnictwo Dom Wydawniczy i Handlowy Elipsa. In Animal Assisted Activities with Dogs: Guideline for Basic Requirements Knowledge; Publishing House of Janusz Korczak Pedagogical University Publishing House Elipsa: Warsaw, Polska, 2016. [Google Scholar]
- Spector, A.; Thorgrimsen, L.; Woods, R.; Orrell, M. Making a Difference: An Evidencebased Group Programme to Offer Cognitive Stimulation Therapy (CST) to People with Dementia; Hawker Publications: London, UK, 2006. [Google Scholar]
- Apóstolo, J.; Cardoso, D. Estimulação Cognitiva Em Idosos: Síntese Da Evidência e Intervenção. In Literacia em Saúde Mental: Capacitar as Pessoas e As Comunidades Para Agir; Loureiro, L., Ed.; Unidade de Investigação em Ciências da Saúde: Enfermagem, Escola Superior de Enfermagem de Coimbra (ESEnfC): Coimbra, Portugal, 2014; pp. 157–183. [Google Scholar]
- Santos-Rocha, R.; Freitas, J.; Ramalho, F.; Couto, F.; Apóstolo, J. Programa de Exercício Físico Para o Idoso Com Fragilidade–Manual de Apoio; Unidade de Investigação em Ciências da Saúde: Enfermagem-Escola Superior de Enfermagem de Coimbra: Coimbra, Portugal, 2019. [Google Scholar]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Freitas, S.; Simões, M.R.; Santana, I.; Martins, C.; Nasreddine, Z.S. Montreal Cognitive Assessment (MoCA): Versão 1; Faculdade de Psicologia e de Ciências da Educação da Universidade de Coimbra: Coimbra, Portugal, 2013. [Google Scholar]
- Peel, N.M.; Kuys, S.S.; Klein, K. Gait Speed as a Measure in Geriatric Assessment in Clinical Settings: A Systematic Review. J. Gerontol. Ser. A 2013, 68, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Van Kan, A.G.; Rolland, Y.; Andrieu, S.; Bauer, J.; Beauchet, O.; Bonnefoy, M.; Cesari, M.; Donini, L.M.; Gillette-Guyonnet, S.; Inzitari, M.; et al. Gait Speed at Usual Pace as a Predictor of Adverse Outcomes in Community-Dwelling Older People an International Academy on Nutrition and Aging (IANA) Task Force. J. Nutr. Health Aging 2009, 13, 881–889. [Google Scholar] [CrossRef]
- Orlin, M.N.; McPoil, T.G. Plantar Pressure Assessment. Phys. Ther. 2000, 80, 399–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramalho, F.; Santos-Rocha, R.; Branco, M.; Moniz-Pereira, V.; André, H.I.; Veloso, A.; Carnide, F. Effect of 6-Month Community-Based Exercise Interventions on Gait and Functional Fitness of an Older Population: A Quasi-Experimental Study. CIA 2018, 13, 595–606. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, F.I.; Barthel, D. Functional Evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 56–61, Used with permission. [Google Scholar]
- Jesus, L.; Marques, A.; Roberto, M.; Rosa, M.; Patrício, B. Barthel Index (BI)-Versão Portuguesa (BI-EP). Maryland State Medical Society, MAPI Institute and University of Aveiro. 2014. Available online: https://eprovide.mapi-trust.org/ (accessed on 1 March 2018).
- Apóstolo, J.; Cardoso, D.; Marta, L.; Amaral, T. Efeito Da Estimulação Cognitiva Em Idosos. Rev. Enf. Ref. 2011, 193–201. [Google Scholar] [CrossRef]
- Alves Apóstolo, J.L.; Batista Cardoso, D.F.; Paúl, C.; Alves Rodrigues, M.; Sofia Macedo, M. Efectos de la estimulación cognitiva sobre las personas mayores en el ámbito comunitario. Enfermería Clínica 2016, 26, 111–120. [Google Scholar] [CrossRef] [PubMed]
- Field, A.P. Discovering Statistics Using SPSS: And Sex, Drugs and Rock “n” Roll, 3rd ed.; SAGE Publications: Los Angeles, CA, USA, 2009. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; L. Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Ranganathan, P.; Pramesh, C.; Aggarwal, R. Common Pitfalls in Statistical Analysis: Absolute Risk Reduction, Relative Risk Reduction, and Number Needed to Treat. Perspect. Clin. Res. 2016, 7, 51. [Google Scholar] [CrossRef] [PubMed]
- Baraldi, A.; Enders, C. Missing Data Methods. In Oxford Library of Psychology. The Oxford Handbook of Quantitative Methods: Statistical Analysis; Little, T.D., Ed.; Oxford University Press: New York, NY, USA, 2013; pp. 635–664. [Google Scholar]
- Burgener, S.C.; Yang, Y.; Gilbert, R.; Marsh-Yant, S. The Effects of a Multimodal Intervention on Outcomes of Persons with Early-Stage Dementia. Am. J. Alzheimers Dis. Other Demen. 2008, 23, 382–394. [Google Scholar] [CrossRef] [PubMed]
- Kraft, E. Cognitive Function, Physical Activity, and Aging: Possible Biological Links and Implications for Multimodal Interventions. Aging Neuropsychol. Cognit. 2012, 19, 248–263. [Google Scholar] [CrossRef] [PubMed]
- Aguirre, E.; Hoare, Z.; Streater, A.; Spector, A.; Woods, B.; Hoe, J.; Orrell, M. Cognitive Stimulation Therapy (CST) for People with Dementia-Who Benefits Most? CST for People with Dementia-Who Benefits Most? Int. J. Geriatr. Psychiatry 2013, 28, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Woods, B.; Aguirre, E.; Spector, A.E.; Orrell, M. Cognitive Stimulation to Improve Cognitive Functioning in People with Dementia. Cochrane Database Syst. Rev. 2012. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Han, J.W.; So, Y.; Seo, J.; Kim, Y.J.; Park, J.H.; Lee, S.B.; Lee, J.J.; Jeong, H.G.; Kim, T.H.; et al. Cognitive Stimulation as a Therapeutic Modality for Dementia: A Meta-Analysis. Psychiatry Investig. 2017, 14, 626. [Google Scholar] [CrossRef] [PubMed]
- Solfrizzi, V.; Scafato, E.; Seripa, D.; Lozupone, M.; Imbimbo, B.P.; D’Amato, A.; Tortelli, R.; Schilardi, A.; Galluzzo, L.; Gandin, C.; et al. Reversible Cognitive Frailty, Dementia, and All-Cause Mortality. The Italian Longitudinal Study on Aging. J. Am. Med. Dir. Assoc. 2017, 18, 89.e1–89.e8. [Google Scholar] [CrossRef] [PubMed]
- Borges, M.K.; Canevelli, M.; Cesari, M.; Aprahamian, I. Frailty as a Predictor of Cognitive Disorders: A Systematic Review and Meta-Analysis. Front. Med. 2019, 6, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukushima, R.L.M.; Carmo, E.G.d.; Pedroso, R.d.V.; Micali, P.N.; Donadelli, P.S.; Fuzaro Junior, G.; Venancio, R.C.d.P.; Viola, J.; Costa, J.L.R. Effects of Cognitive Stimulation on Neuropsychiatric Symptoms in Elderly with Alzheimer’s Disease: A Systematic Review. Dement. Neuropsychol. 2016, 10, 178–184. [Google Scholar] [CrossRef]
- The DEP-EXERCISE Group; López-Torres Hidalgo, J. Effectiveness of Physical Exercise in the Treatment of Depression in Older Adults as an Alternative to Antidepressant Drugs in Primary Care. BMC Psychiatry 2019, 19, 21. [Google Scholar] [CrossRef]
- Amemiya, A.; Noguchi, H.; Oe, M.; Ohashi, Y.; Ueki, K.; Kadowaki, T.; Mori, T.; Sanada, H. Elevated Plantar Pressure in Diabetic Patients and Its Relationship with Their Gait Features. Gait Posture 2014, 40, 408–414. [Google Scholar] [CrossRef]
- Lee, M.Y.; Lin, C.F.; Soon, K.S. New Foot Pressure Activated Sensory Compensation System for Posture-Control Enhancement in Amputees. IEEE/ASME Trans. Mechatron. 2007, 12, 236–243. [Google Scholar] [CrossRef]
- Abdul Razak, A.H.; Zayegh, A.; Begg, R.K.; Wahab, Y. Foot Plantar Pressure Measurement System: A Review. Sensors 2012, 12, 9884–9912. [Google Scholar] [CrossRef] [Green Version]
- Robinson, C.C.; Balbinot, L.F.; Silva, M.F.; Achaval, M.; Zaro, M.A. Plantar Pressure Distribution Patterns of Individuals with Prediabetes in Comparison with Healthy Individuals and Individuals with Diabetes. J. Diabetes Sci. Technol. 2013, 7, 1113–1121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simmonds, M.J.; Lee, C.E.; Etnyre, B.R.; Morris, G.S. The Influence of Pain Distribution on Walking Velocity and Horizontal Ground Reaction Forces in Patients with Low Back Pain. Pain Res. Treat. 2012, 2012, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.S.; Lin, T.C.; Jiang, B.C. Aerobic and Resistance Exercise Training Program Intervention for Enhancing Gait Function in Elderly and Chronically Ill Taiwanese Patients. Public Health 2015, 129, 1114–1124. [Google Scholar] [CrossRef] [PubMed]
- Iunes, D.H.; Rocha, C.B.J.; Borges, N.C.S.; Marcon, C.O.; Pereira, V.M.; Carvalho, L.C. Self-Care Associated with Home Exercises in Patients with Type 2 Diabetes Mellitus. PLoS ONE 2014, 9, e114151. [Google Scholar] [CrossRef] [PubMed]
- Parkatti, T.; Perttunen, J.; Wacker, P. Improvements in Functional Capacity from Nordic Walking: A Randomized Controlled Trial Among Older Adults. J. Aging Phys. Act. 2012, 20, 93–105. [Google Scholar] [CrossRef] [PubMed]
- Fernando, M.E.; Crowther, R.G.; Lazzarini, P.A.; Sangla, K.S.; Wearing, S.; Buttner, P.; Golledge, J. Plantar Pressures Are Higher in Cases with Diabetic Foot Ulcers Compared to Controls despite a Longer Stance Phase Duration. BMC Endocr. Disord. 2016, 16, 51. [Google Scholar] [CrossRef] [PubMed]
- Schwenk, M.; Howe, C.; Saleh, A.; Mohler, J.; Grewal, G.; Armstrong, D.; Najafi, B. Frailty and Technology: A Systematic Review of Gait Analysis in Those with Frailty. Gerontology 2014, 60, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Ritt, M.; Schülein, S.; Lubrich, H.; Bollheimer, L.C.; Sieber, C.C.; Gassmann, K.-G. High-Technology Based Gait Assessment in Frail People: Associations between Spatio-Temporal and Three-Dimensional Gait Characteristics with Frailty Status across Four Different Frailty Measures. J. Nutr. Health Aging 2017, 21, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Clegg, A.; Rogers, L.; Young, J. Diagnostic Test Accuracy of Simple Instruments for Identifying Frailty in Community-Dwelling Older People: A Systematic Review. Age Ageing 2015, 44, 148–152. [Google Scholar] [CrossRef]
- Feng, Z.; Lugtenberg, M.; Franse, C.; Fang, X.; Hu, S.; Jin, C.; Raat, H. Risk Factors and Protective Factors Associated with Incident or Increase of Frailty among Community-Dwelling Older Adults: A Systematic Review of Longitudinal Studies. PLoS ONE 2017, 12, e0178383. [Google Scholar] [CrossRef]
- Apóstolo, J.; Couto, F.; Bobrowicz-Campos, E.; Dixe, M.A.; Ribeiro, J.; Braúna, M.; Camacho, T.; Santos-Rocha, R.; Parreira, P.; Cruz, A.; et al. An Interregional, Transdisciplinary and Good Practice-Based Approach for Frailty: The Mind Gait Project. Transl Med. Unisa 2019, 19, 11–16. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Total Sample (N = 44) | Control Group (n = 21) | Experimental Group (n = 23) | ||
|---|---|---|---|---|---|
| N(%) | n(%) | n(%) | X2 | p | |
| Sex | |||||
| Male | 15 (34,1) | 5 (23.8) | 10 (43.5) | 1.89 | 0.213 |
| Female | 29 (65.9) | 16 (76.2) | 13 (56.5) | - | |
| M±SD (Median) | M±SD (Median) | M±SD (Median) | U | p | |
| Age | 80.54 ± 8.47 (81) | 82.04 ± 9.29 (85) | 79.17 ± 7.59 (80) | 192.500 | 0.249 |
| Registration time in the elderly end-user organization (months) | 49.97 ± 41.86 (36) | 57.85 ± 46.66 (48) | 42.78 ± 36.51 (24) | 207.500 | 0.420 |
| Variables | Baseline | Post-Intervention | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| CG (N = 21) | EG (N = 23) | U (p) | CG (N = 21) | EG (N = 23) | U (p) | |||||
| M (SD) | MR | M (SD) | MR | M (SD) | MR | M (SD) | MR | |||
| Cognitive performance (MoCA) | 15.33 (4.83) | 22.33 | 15.87 (4.88) | 22.65 | 238.00 (0.934) | 16.42 (6.49) | 22.40 | 16.91 (4.98) | 22.59 | 239.50 (0.962) |
| Depressive Symptomatology (GDS-10) | 3.81 (2.84) | 25.19 | 2.74 (2.70) | 20.04 | 185.00 (0.180) | 3 (2.24) | 27.00 | 1.65 (2.06) | 18.39 | 147.00 (0.024) |
| Risk of fall based on gait and balance (TI) | 19.67 (6.38) | 21.33 | 20.39 (7.28) | 23.57 | 217.00 (0.564) | 20.62 (6.61) | 20.00 | 22.17 (6.69) | 24.78 | 189.00 (0.211) |
| Gait Speed | 0.59 (0.29) | 22.68 | 0.55 (0.31) | 21.41 | 216.50 (0.742) | 2.46 (7.48) | 22.23 | 0.64 (0.37) | 21.80 | 225.50 (0.913) |
| Activities of daily living (BI) | 0.82 (0.14) | 20.26 | 0.84 (0.18) | 24.54 | 194.50 (0.264) | 0.75 (0.19) | 18.83 | 0.82 (0.19) | 25.85 | 164.50 (0.069) |
| Maximum force all foot right * | 100.87 (7.16) | 20.95 | 104.02 (19.79) | 20.05 | 191.00 (0.808) | 101.69 (6.73) | 18.28 | 112.99 (44.15) | 21.48 | 158.00 (0.382) |
| Maximum force all foot left * | 90.52 (29.96) | 18.60 | 105.26 (20.87) | 22.40 | 162.00 0.304) | 102.65 (6.76) | 18.94 | 151.66 (217.56) | 20.90 | 170.00 (0.592) |
| Peak pressure all foot right * | 445.53 (169.04) | 21.05 | 481.66 (302.16) | 19.95 | 189.00 (0.766) | 452.32 (193.34) | 19.28 | 524.31 (303.94) | 29.62 | 176.00 (0.714) |
| Peak pressure all foot left * | 410.46 (175.93) | 19.08 | 520.51 (278.35) | 21.93 | 171.50 (0.441 *) | 477.40 (198.84) | 19.50 | 545.35 (290.31) | 20.43 | 180.00 (0.800) |
| Variables | CG (N = 21) | EG (N = 23) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Status ** | N | % | Mean Rank | Z | p | Status ** | N | % | Mean Rank | Z | p | |
| Cognitive Performance (MoCA) | a | 10 | 47.6 | 8.50 | −1.43 | 0.153 | a | 14 | 60.9 | 9.00 | −1.78 | 0.075 |
| b | 5 | 23.8 | 7.00 | b | 4 | 17.4 | 11.25 | |||||
| c | 6 | 28.6 | c | 5 | 21.7 | |||||||
| Depressive Symptomatology (GDS-10) | a | 10 | 47.7 | 7.65 | −1.52 | 0.130 | a | 11 | 47.8 | 9.05 | −2.27 | 0.023 |
| b | 4 | 19.0 | 7.13 | b | 4 | 17.4 | 5.13 | |||||
| c | 7 | 33.3 | c | 8 | 34.8 | |||||||
| Risk of Fall Based on Gait and Balance (Tinetti) | a | 11 | 52.4 | 8.50 | −1.33 | 0.184 | a | 18 | 78.26 | 10.56 | −2.61 | 0.009 |
| b | 5 | 23.8 | 8.50 | b | 3 | 13.04 | 13.67 | |||||
| c | 5 | 23.8 | c | 2 | 8.7 | |||||||
| Gait Speed | a | 6 | 30 | 11.00 | −0.50 | 0.618 | a | 15 | 65.2 | 11.70 | −2.09 | 0.037 |
| b | 11 | 55 | 7.91 | b | 6 | 26.1 | 9.25 | |||||
| c | 3 | 15 | c | 2 | 8.7 | |||||||
| Activities of Daily Living (Barthel Index) | a | 2 | 9.5 | 6.25 | −2.31 | 0.021 | a | 3 | 13.0 | 7.17 | −1.03 | 0.303 |
| b | 11 | 52.4 | 7.14 | b | 8 | 34.8 | 5.56 | |||||
| c | 8 | 38.1 | c | 12 | 52.2 | |||||||
| Maximum Force all Foot Left * | a | 12 | 66.7 | 9.58 | −2.43 | 0.015 | a | 14 | 70 | 10.79 | −2.254 | 0.024 |
| b | 4 | 22.2 | 5.25 | b | 5 | 25 | 7.80 | |||||
| c | 2 | 11.1 | c | 1 | 5 | |||||||
| Maximum Force all Foot Right * | a | 10 | 55.6 | 8.90 | −1.086 | 0.278 | a | 16 | 80 | 9.31 | −2.173 | 0.030 |
| b | 6 | 33.3 | 7.83 | b | 3 | 15 | 13.67 | |||||
| c | 2 | 11.1 | c | 1 | 5 | |||||||
| Peak Pressure All Foot Left * | a | 11 | 61.1 | 8.73 | −2.045 | 0.041 | a | 11 | 55 | 11.27 | −1.167 | 0.243 |
| b | 4 | 22,2 | 6.00 | b | 8 | 40 | 8.25 | |||||
| c | 3 | 16.7 | c | 1 | 5 | |||||||
| Peak Pressure All Foot Right * | a | 11 | 61.1 | 8.09 | −1.086 | 0.278 | a | 13 | 65 | 10.12 | −2.004 | 0.045 |
| b | 5 | 27.8 | 9.40 | b | 5 | 25 | 7.90 | |||||
| c | 2 | 11.1 | c | 2 | 10 | |||||||
| Varaibles | Control Group | Experimental Group | ||
|---|---|---|---|---|
| Z | Effect Size (r) | Z | Effect Size (r) | |
| Depressive Symptomatology (GDS-10) | −2.27 | 0.33469 | ||
| Risk of Fall Based on Gait and balance (Tinetti) | −2.61 | 0.38482 | ||
| Gait Speed | −2.09 | 0.30815 | ||
| Activities of Daily Living (Barthel Index) | −2.31 | 0.35644 | ||
| Maximum Force All Foot Left * | −2.43 | 0.40500 | −2.254 | 0.35639 |
| Maximum Force All Foot Right * | −2.173 | 0.34358 | ||
| Peak Pressure All Foot Left * | −2.045 | 0.33400 | ||
| Peak Pressure All Foot Right * | −2.004 | 0.31686 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Apóstolo, J.; Dixe, M.d.A.; Bobrowicz-Campos, E.; Areosa, T.; Santos-Rocha, R.; Braúna, M.; Ribeiro, J.; Marques, I.; Freitas, J.; Almeida, M.d.L.; et al. Effectiveness of a Combined Intervention on Psychological and Physical Capacities of Frail Older Adults: A Cluster Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2019, 16, 3125. https://doi.org/10.3390/ijerph16173125
Apóstolo J, Dixe MdA, Bobrowicz-Campos E, Areosa T, Santos-Rocha R, Braúna M, Ribeiro J, Marques I, Freitas J, Almeida MdL, et al. Effectiveness of a Combined Intervention on Psychological and Physical Capacities of Frail Older Adults: A Cluster Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2019; 16(17):3125. https://doi.org/10.3390/ijerph16173125
Chicago/Turabian StyleApóstolo, João, Maria dos Anjos Dixe, Elzbieta Bobrowicz-Campos, Timóteo Areosa, Rita Santos-Rocha, Mónica Braúna, Jaime Ribeiro, Isabel Marques, Joana Freitas, Maria de Lurdes Almeida, and et al. 2019. "Effectiveness of a Combined Intervention on Psychological and Physical Capacities of Frail Older Adults: A Cluster Randomized Controlled Trial" International Journal of Environmental Research and Public Health 16, no. 17: 3125. https://doi.org/10.3390/ijerph16173125