The Unholy Trinity: Childhood Trauma, Adulthood Anxiety, and Long-Term Pain

 , ,
, ,  and
and
Abstract
:1. Introduction
1.1. Epidemiology of Chronic Pain and Anxiety
1.2. Childhood Trauma in Chronic Pain and Anxiety
2. Methods
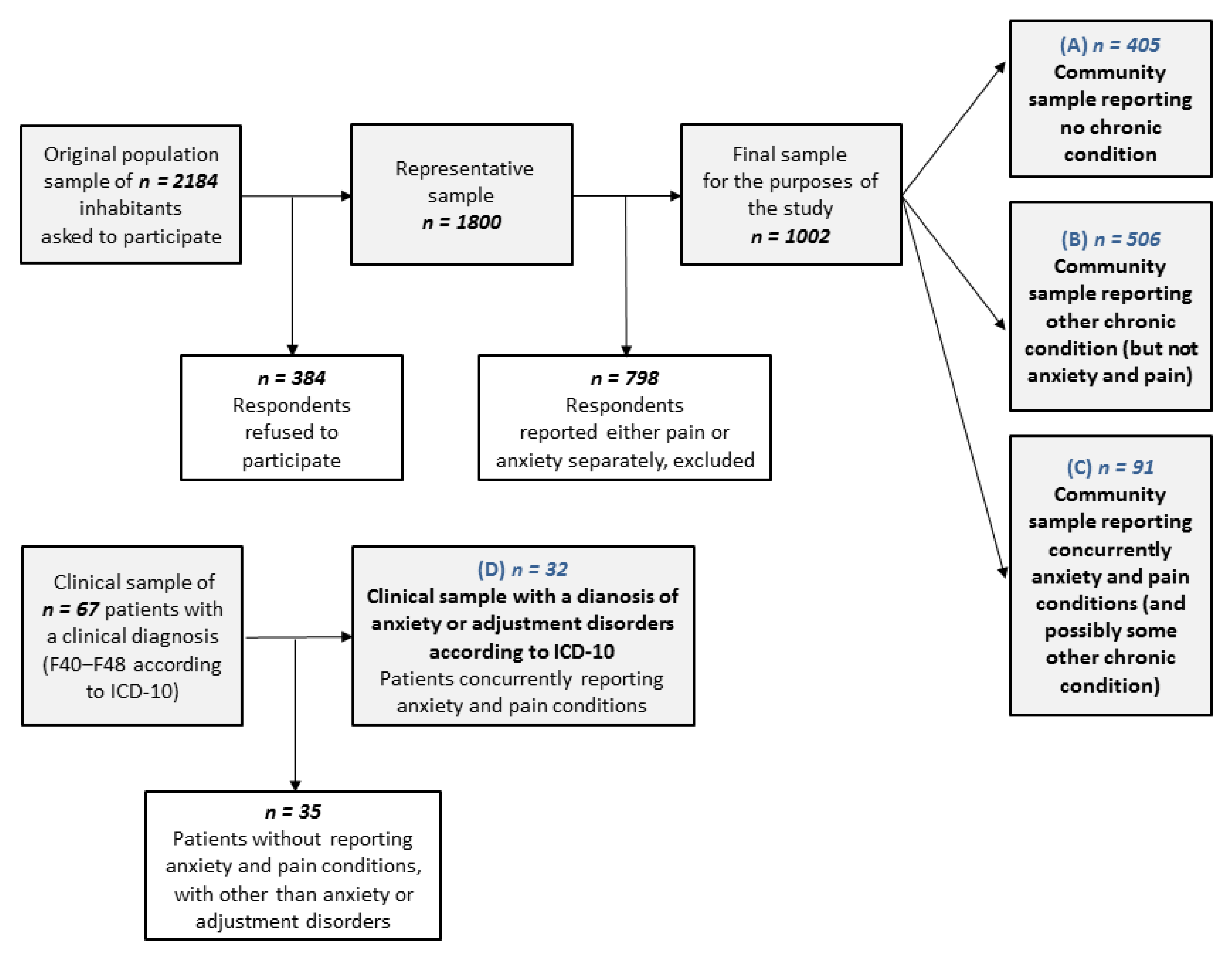
2.1. Sample
2.2. Measures
2.2.1. Sociodemographic Data
2.2.2. Long-Term Health Complaints
2.2.3. Childhood Trauma
2.3. Statistical Analyses
3. Results
3.1. Sociodemographic Characteristics
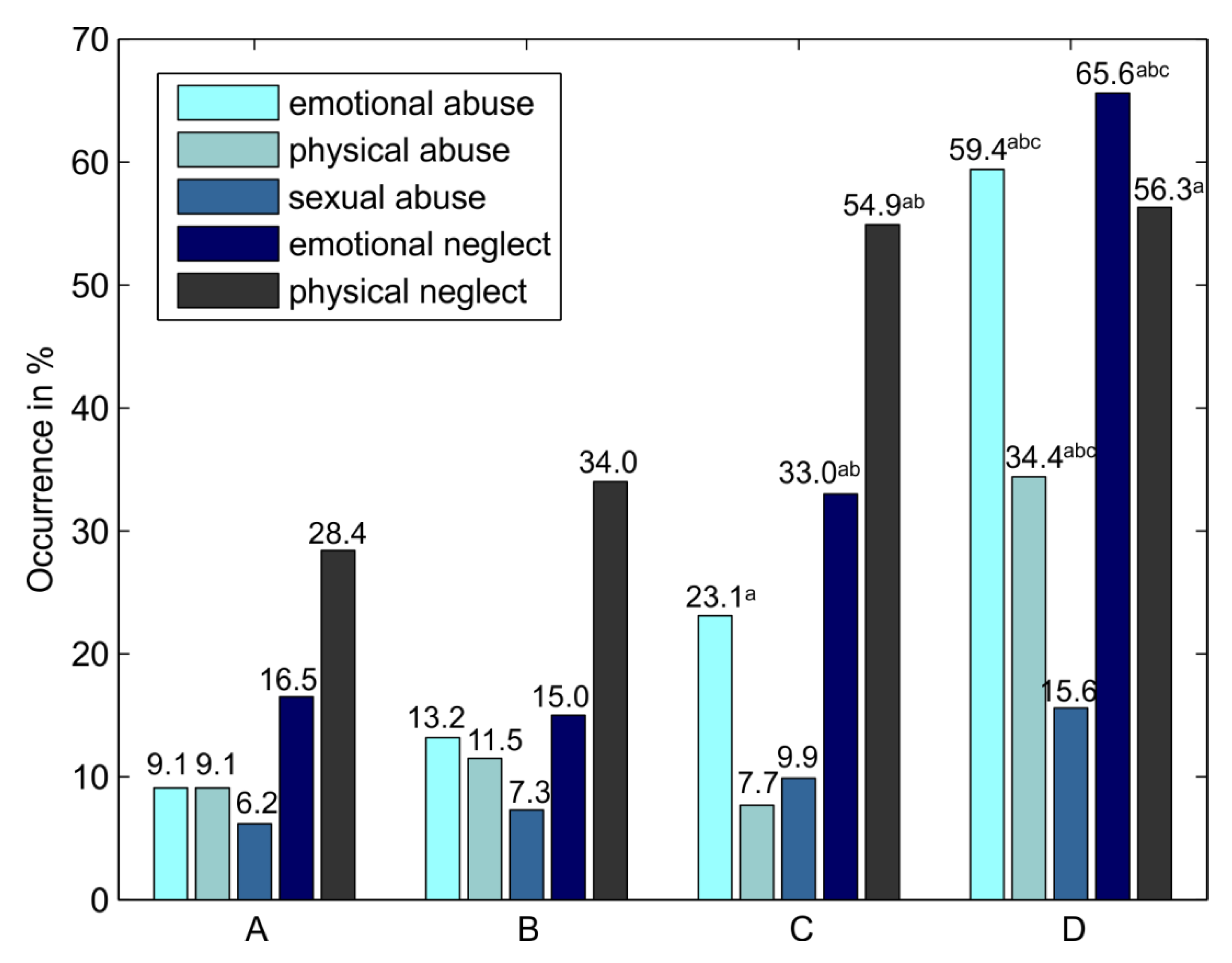
3.2. Prevalence of Various Childhood Trauma Experiences
3.3. Odds of Reporting Anxiety and Pain in the Community and Clinical Samples in Subjects Reporting Various Types of Childhood Trauma
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Davis, D.A.; Luecken, L.J.; Zautra, A.J. Are reports of childhood abuse related to the experience of chronic pain in adulthood?: A meta-analytic review of the literature. Clin. J. Pain 2005, 21, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.C. Associations of adverse childhood experiences and bullying on physical pain in the general population of Germany. J. Pain Res. 2018, 11, 3099–3108. [Google Scholar] [CrossRef] [Green Version]
- Afari, N. Psychological trauma and functional somatic syndromes: A systematic review and meta-analysis. Psychosom. Med. 2014, 76, 2–11. [Google Scholar] [CrossRef] [Green Version]
- Mikulincer, M.; Shaver, P.R. An attachment perspective on psychopathology. World Psychiatry 2012, 11, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Adshead, G. Security of mind: 20 years of attachment theory and its relevance to psychiatry. Br. J. Psychiatry 2018, 213, 511–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kisely, S. Child maltreatment and mental health problems in adulthood: Birth cohort study. Br. J. Psychiatry 2018, 213, 698–703. [Google Scholar] [CrossRef] [PubMed]
- Asmundson, G.J.; Katz, J. Understanding the co-occurrence of anxiety disorders and chronic pain: State-of-the-art. Depress. Anxiety 2009, 26, 888–901. [Google Scholar] [CrossRef]
- McWilliams, L.A.; Cox, B.J.; Enns, M.W. Mood and anxiety disorders associated with chronic pain: An examination in a nationally representative sample. Pain 2003, 106, 127–133. [Google Scholar] [CrossRef]
- Gureje, O. Comorbidity of pain and anxiety disorders. Curr. Psychiatry Rep. 2008, 10, 318–322. [Google Scholar] [CrossRef]
- Viana, M.C. Previous Mental Disorders and Subsequent Onset of Chronic Back or Neck Pain: Findings from 19 Countries. J. Pain 2018, 19, 99–110. [Google Scholar] [CrossRef] [Green Version]
- Pereira, F.G. Prevalence and clinical profile of chronic pain and its association with mental disorders. Rev. Saude Publica 2017, 51, 96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sachs-Ericsson, N.J. When emotional pain becomes physical: Adverse Childhood Experiences, pain, and the role of mood and anxiety disorders. J. Clin. Psychol. 2017, 73, 1403–1428. [Google Scholar] [CrossRef] [PubMed]
- Scott, K.M. Association of childhood adversities and early-onset mental disorders with adult-onset chronic physical conditions. Arch. Gen. Psychiatry 2011, 68, 838–844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raphael, K.G.; Widom, C.S. Post-traumatic stress disorder moderates the relation between documented childhood victimization and pain 30 years later. Pain 2011, 152, 163–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicol, A.L. The association between a history of lifetime traumatic events and pain severity, physical function, and affective distress in patients with chronic pain. J. Pain 2016, 17, 1334–1348. [Google Scholar] [CrossRef]
- Smith, D. Chronic pain and mortality: A systematic review. PLoS ONE 2014, 9, e99048. [Google Scholar] [CrossRef] [Green Version]
- Henschke, N.; Kamper, S.J.; Maher, C.G. The epidemiology and economic consequences of pain. Mayo Clin. Proc. 2015, 90, 139–147. [Google Scholar] [CrossRef] [Green Version]
- Breivik, H. Survey of chronic pain in Europe: Prevalence, impact on daily life, and treatment. Eur. J. Pain 2006, 10, 287–333. [Google Scholar] [CrossRef]
- WHO. ICD-10: International Statistical Classification of Diseases and Related Health Problems: Tenth Revision, 5th ed.; World Health Organization: Geneva, Switzerland, 2015; Available online: https://apps.who.int/iris/handle/10665/246208 (accessed on 15 October 2019).
- Alonso, J. Prevalence of mental disorders in Europe: Results from the European Study of the Epidemiology of Mental Disorders (ESEMeD) project. Acta Psychiatr. Scand. 2004, 109, 21–27. [Google Scholar] [CrossRef]
- Formánek, T. Prevalence of mental disorders and associated disability: Results from the cross-sectional CZEch mental health Study (CZEMS). Eur. Psychiatry 2019, 60, 1–6. [Google Scholar] [CrossRef]
- Evans, S.C. Psychologists’ perspectives on the diagnostic classification of mental disorders: Results from the WHO-IUPsyS Global Survey. Int. J. Psychol. 2013, 48, 177–193. [Google Scholar] [CrossRef] [PubMed]
- Reed, G.M. The WPA-WHO global survey of psychiatrists’ attitudes towards mental disorders classification. World Psychiatry 2011, 10, 118–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velly, A.M.; Mohit, S. Epidemiology of pain and relation to psychiatric disorders. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2018, 87, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Demyttenaere, K. Mental disorders among persons with chronic back or neck pain: Results from the World Mental Health Surveys. Pain 2007, 129, 332–342. [Google Scholar] [CrossRef] [PubMed]
- Knaster, P. Psychiatric disorders as assessed with SCID in chronic pain patients: The anxiety disorders precede the onset of pain. Gen. Hosp. Psychiatry 2012, 34, 46–52. [Google Scholar] [CrossRef]
- Tegethoff, M. Comorbidity of mental disorders and chronic pain: Chronology of onset in adolescents of a national representative cohort. J. Pain 2015, 16, 1054–1064. [Google Scholar] [CrossRef]
- Gureje, O.; Simon, G.E.; Von Korff, M. A cross-national study of the course of persistent pain in primary care. Pain 2001, 92, 195–200. [Google Scholar] [CrossRef]
- Carleton, R.N. Pain-related anxiety and anxiety sensitivity across anxiety and depressive disorders. J. Anxiety Disord. 2009, 23, 791–798. [Google Scholar] [CrossRef]
- Vlaeyen, J.W.; Linton, S.J. Fear-avoidance model of chronic musculoskeletal pain: 12 years on. Pain 2012, 153, 1144–1147. [Google Scholar] [CrossRef] [PubMed]
- Engel, G.L. “Psychogenic” pain and the pain-prone patient. Am. J. Med. 1959, 26, 899–918. [Google Scholar] [CrossRef]
- Green, J.G. Childhood adversities and adult psychopathology in the National Comorbidity Survey Replication (NCS-R) I: Associations with first onset of DSM-IV disorders. Arch. Gen. Psychiatry 2010, 67, 113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hovens, J.G. Childhood life events and childhood trauma in adult patients with depressive, anxiety and comorbid disorders vs. controls. Acta Psychiatr. Scand. 2010, 122, 66–74. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, V.; Osório, F.L. Are there associations between early emotional trauma and anxiety disorders? Evidence from a systematic literature review and meta-analysis. Eur. Psychiatry 2015, 30, 756–764. [Google Scholar] [CrossRef] [PubMed]
- Afifi, T.O. Child abuse and mental disorders in Canada. CMAJ 2014, 186, E324–E332. [Google Scholar] [CrossRef] [Green Version]
- Nemeroff, C.B. Paradise lost: The neurobiological and clinical consequences of child abuse and neglect. Neuron 2016, 89, 892–909. [Google Scholar] [CrossRef] [Green Version]
- McEwen, B.S. Mechanisms of stress in the brain. Nat. Neurosci. 2015, 18, 1353–1363. [Google Scholar] [CrossRef]
- Heim, C.; Nemeroff, C.B. The role of childhood trauma in the neurobiology of mood and anxiety disorders: Preclinical and clinical studies. Biol. Psychiatry 2001, 49, 1023–1039. [Google Scholar] [CrossRef] [Green Version]
- Heim, C. Neurobiological and psychiatric consequences of child abuse and neglect. Dev. Psychobiol. 2010, 52, 671–690. [Google Scholar] [CrossRef]
- Arnow, B.A. Severity of child maltreatment, pain complaints and medical utilization among women. J. Psychiatr. Res. 2000, 34, 413–421. [Google Scholar] [CrossRef]
- Lampe, A. Chronic pain syndromes and their relation to childhood abuse and stressful life events. J. Psychosom. Res. 2003, 54, 361–367. [Google Scholar] [CrossRef]
- Tietjen, G.E. Recalled maltreatment, migraine, and tension-type headache: Results of the AMPP study. Neurology 2015, 84, 132–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norman, R.E. The long-term health consequences of child physical abuse, emotional abuse, and neglect: A systematic review and meta-analysis. PLoS Med. 2012, 9, e1001349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sansone, R.A.; Watts, D.A.; Wiederman, M.W. Childhood trauma and pain and pain catastrophizing in adulthood: A cross-sectional survey study. Prim. Care Companion CNS Disord. 2013, 15, PCC.13m01506. [Google Scholar] [CrossRef] [Green Version]
- Spertus, I.L. Childhood emotional abuse and neglect as predictors of psychological and physical symptoms in women presenting to a primary care practice. Child Abuse Negl. 2003, 27, 1247–1258. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, D.P. Development and validation of a brief screening version of the Childhood Trauma Questionnaire. Child Abuse Negl. 2003, 27, 169–190. [Google Scholar] [CrossRef]
- Bernstein, D.P.; Fink, L. Childhood Trauma Questionnaire: A Retrospective Self-Report Manual; NCS Pearson: San Antonio, TX, USA, 1998. [Google Scholar]
- Walker, E.A. Adult health status of women with histories of childhood abuse and neglect. Am. J. Med. 1999, 107, 332–339. [Google Scholar] [CrossRef]
- Kascakova, N. Psychometric analysis of the Czech version of Childhood Trauma Questionnaire (CTQ) with the sociodemografic differences in traumatization of Czech adults. Ceskoslov. Psychol. 2018, 62, 212–230. [Google Scholar]
- Kopec, J.A.; Sayre, E.C. Stressful experiences in childhood and chronic back pain in the general population. Clin. J. Pain 2005, 21, 478–483. [Google Scholar] [CrossRef]
- Hovens, J.G.F.M. Emotional Scars: Impact of Childhood Trauma on Depressive and Anxiety Disorders; Department of Psychiatry, Faculty of Medicine, Leiden University Medical Center (LUMC), Leiden University: Leiden, The Netherlands, 2015. [Google Scholar]
- Teicher, M.H. Sticks, stones, and hurtful words: Relative effects of various forms of childhood maltreatment. Am. J. Psychiatry 2006, 163, 993–1000. [Google Scholar] [CrossRef]
- Strathearn, L. Maternal neglect: Oxytocin, dopamine and the neurobiology of attachment. J. Neuroendocrinol. 2011, 23, 1054–1065. [Google Scholar] [CrossRef]
- Walsh, C.A. Child abuse and chronic pain in a community survey of women. J. Interpers. Violence 2007, 22, 1536–1554. [Google Scholar] [CrossRef] [PubMed]
- Cougle, J.R. Examining the unique relationships between anxiety disorders and childhood physical and sexual abuse in the National Comorbidity Survey-Replication. Psychiatry Res. 2010, 177, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Beesdo, K. Pain associated with specific anxiety and depressive disorders in a nationally representative population sample. Soc. Psychiatry Psychiatr. Epidemiol. 2010, 45, 89–104. [Google Scholar] [CrossRef] [PubMed]
- Arnold, B. Multimodale Schmerztherapie für die Behandlung chronischer Schmerzsyndrome. Der Schmerz 2014, 28, 459–472. [Google Scholar] [CrossRef]
- Baumeister, H. High agreement of self-report and physician-diagnosed somatic conditions yields limited bias in examining mental–physical comorbidity. J. Clin. Epidemiol. 2010, 63, 558–565. [Google Scholar] [CrossRef]
- Raphael, K.G.; Widom, C.S.; Lange, G. Childhood victimization and pain in adulthood: A prospective investigation. Pain 2001, 92, 283–293. [Google Scholar] [CrossRef]
- Hardt, J.; Rutter, M. Validity of adult retrospective reports of adverse childhood experiences: Review of the evidence. J. Child Psychol. Psychiatry 2004, 45, 260–273. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Sociodemographic Groups | (A) Community Sample Reporting No Chronic Conditions | (B) Community Sample Reporting Other Chronic Conditions | (C) Community Sample Reporting Anxiety and Pain * | (D) Clinical Sample ** Reporting Anxiety and Pain |
|---|---|---|---|---|
| n = 405 | n = 506 | n = 91 | n = 32 | |
| Age: Mean (SD) | 36.4 (14.3) | 46.3 (17.6) | 51.6 (18.6) | 39.1 (12.6) |
| Gender: n (%) | ||||
| 1. Male | 235 (58.0) | 266 (52.6) | 27 (29.7) | 6 (18.8) |
| 2. Female | 170 (42.0) | 240 (47.4) | 64 (70.3) | 26 (81.3) |
| Living arrangement: n (%) | ||||
| 1. With a partner in marriage | 152 (37.5) | 266 (52.6) | 39 (42.9) | 11 (34.4) |
| 2. With a partner | 98 (24.2) | 98 (19.4) | 20 (22.0) | 1 (3.1) |
| 3. Alone | 94 (23.2) | 91 (18.0) | 25 (27.5) | 10 (31.3) |
| 4. With parents, siblings | 61 (15.1) | 51 (10.1) | 7 (7.7) | 10 (31.3) |
| Education level: n (%) | ||||
| 1. Primary | 18 (4.4) | 41 (8.1) | 10 (11.0) | 3 (9.4) |
| 2. Skilled operative | 81 (20.0) | 100 (19.8) | 33 (36.3) | 9 (28.1) |
| 3. High school, graduated | 212 (52.3) | 259 (51.2) | 32 (35.2) | 14 (43.8) |
| 4. College/University | 94 (23.2) | 106 (20.9) | 16 (17.6) | 6 (18.8) |
| Childhood Trauma Questionnaire (CTQ) | Group (C) vs. (A) | Group (D) vs. (A) | Group (C) vs. (B) | Group (D) vs. (B) | Group (D) vs. (C) |
|---|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Emotional abuse (cut-off score 10) | 3.79 (2.02‒7.12) *** | 14.71 (6.56–32.95) *** | 2.14 (1.21‒3.77) * | 8.28 (3.83‒17.90) *** | 3.88 (1.61‒9.31) ** |
| Physical abuse (cut-off score 8) | 0.82 (0.34‒1.95) | 5.23 (2.30‒11.89) *** | 0.63 (0.28‒1.45) | 4.04 (1.82‒8.96) *** | 6.39 (2.18‒18.74) *** |
| Sexual abuse (cut-off score 8) | 1.52 (0.69‒3.51) | 2.51 (0.88‒7.20) | 1.32 (0.61‒2.88) | 2.19 (0.78‒6.13) | 1.65 (0.50‒5.46) |
| Emotional neglect (cut-off score 15) | 2.42 (1.41‒4.14) *** | 9.56 (4.35‒21.00) *** | 2.78 (1.67‒4.63) *** | 10.99 (5.03‒24.03) *** | 3.95 (1.67‒9.36) ** |
| Physical neglect (cut-off score 8) | 2.55 (1.56‒4.15) *** | 3.30 (1.57‒6.95) ** | 2.24 (1.41‒3.55) *** | 2.90 (1.39‒6.06) ** | 1.30 (0.57‒2.96) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kascakova, N.; Furstova, J.; Hasto, J.; Madarasova Geckova, A.; Tavel, P. The Unholy Trinity: Childhood Trauma, Adulthood Anxiety, and Long-Term Pain. Int. J. Environ. Res. Public Health 2020, 17, 414. https://doi.org/10.3390/ijerph17020414
Kascakova N, Furstova J, Hasto J, Madarasova Geckova A, Tavel P. The Unholy Trinity: Childhood Trauma, Adulthood Anxiety, and Long-Term Pain. International Journal of Environmental Research and Public Health. 2020; 17(2):414. https://doi.org/10.3390/ijerph17020414
Chicago/Turabian StyleKascakova, Natalia, Jana Furstova, Jozef Hasto, Andrea Madarasova Geckova, and Peter Tavel. 2020. "The Unholy Trinity: Childhood Trauma, Adulthood Anxiety, and Long-Term Pain" International Journal of Environmental Research and Public Health 17, no. 2: 414. https://doi.org/10.3390/ijerph17020414