4.1. Theoretical Contributions
The aim of the current study was to investigate if social resources can promote SE over time. Based on the definition of SE from van der Klink et al. [
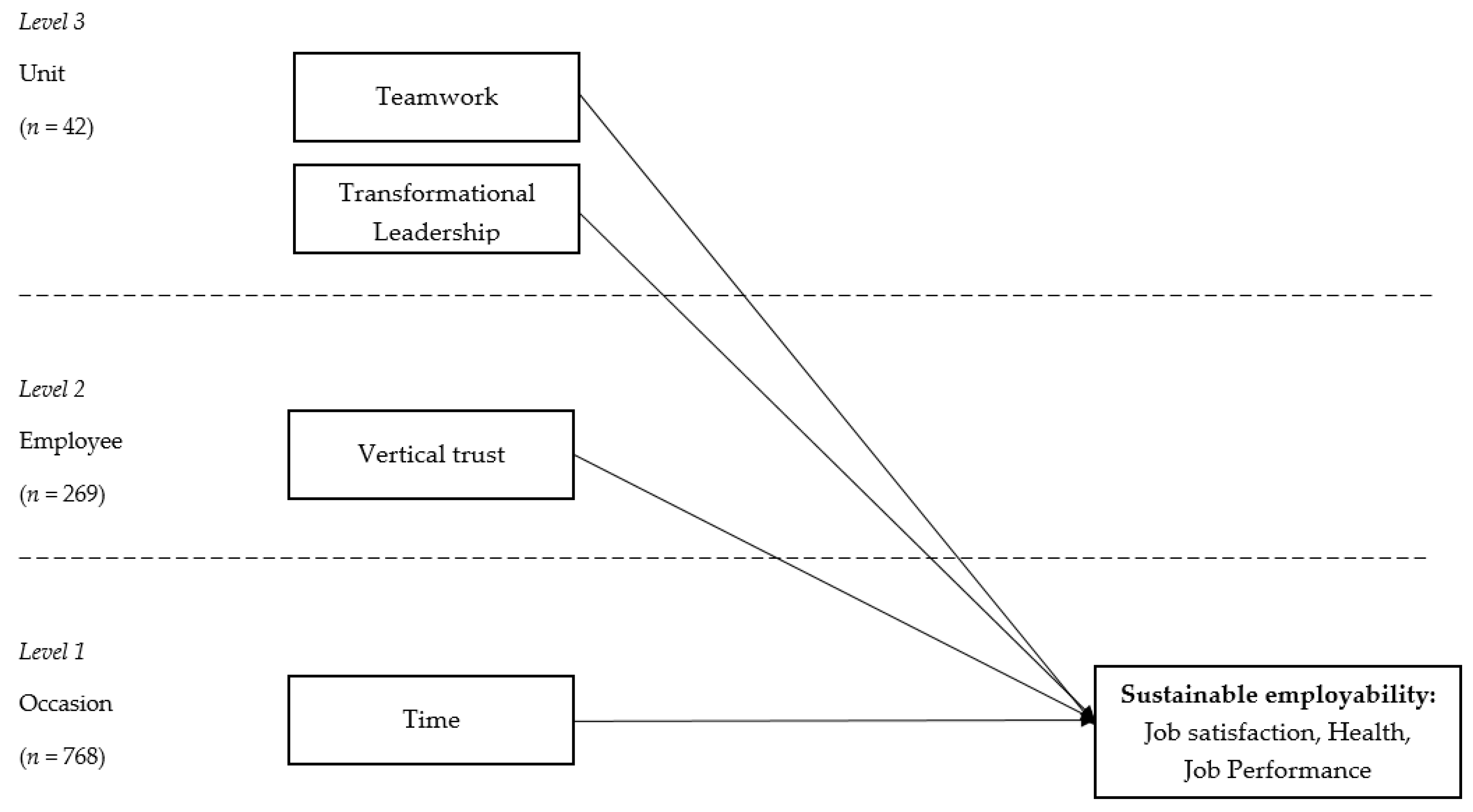
3], we operationalized SE as productivity, health, and job satisfaction, to capture employees’ ability to work productively while retaining health and well-being. Furthermore, in this study, vertical trust, team work, and transformation leadership were chosen as social resources, operating on different levels and different planes, furthering the JD-R theory [
16]. Overall, the findings demonstrated that social job resources have a role in shaping employee job satisfaction, health, and performance, partially supporting all three hypotheses. More specifically, distinct resources played different roles for these three facets of SE, with vertical trust having a positive impact on all three facets, teamwork on two, and transformational leadership lacking a positive impact.
Our results showed that vertical trust, measured at the individual level, was important for all three facets of sustainable employment in healthcare. It had a positive effect on employee job satisfaction, health, and job performance over time. Vertical trust represents how trustful an employee is with regard to the information that comes from management as well as employees’ perceptions of organizational justice. Hence, vertical trust is based on fair treatment (top–down) from the company, which generates employee trust towards the organization (bottom–up). Thus, this resource follows a vertical axis. According to the JD-R theory, vertical trust as a social job resource may trigger the motivational process and facilitate the achievement of goals at work. Our results corroborate other findings that link social capital with job well-being at work [
29], trust with job performance [
30], and justice with health [
44].
Another social job resource we investigated in this study was teamwork, i.e., the extent of the collaborative effort of the group members to achieve a common goal. The similarity of individual perceptions of group processes within units allowed us to analyze this resource at the group level. This aggregation made it possible to compare healthcare units with each other and investigate how the levels of teamwork in different units affect individual employees in these units. The results showed that, in units high in teamwork, individual employees reported better productivity and health, though there was no statistically significant impact on job satisfaction. First, this result might imply that good collaboration and communication among team members facilitate task execution. Medical care is a team effort [
32]; therefore, efficient cooperation translates into higher performance. Our research demonstrated that the influence of teamwork on productivity extends beyond individual perceptions. We showed a cross-level relationship in which unit-level teamwork affected individual performance; thus, we demonstrated that a work environment rich in good teamwork is beneficial for individual job performance. Next, the results also demonstrated that units with better teamwork have more healthy members than other units. Good teamwork signifies collaboration and support that can work as buffer in times of stress [
45], helping employees lower the psychological cost of their job demands. Indeed, in his meta-analysis, Halbesleben [
46] demonstrated that, after seeking social support at work, employees are less exhausted, which suggests that social resources are functional in dealing with stress. Given the link between stress and health (e.g., frequency of infections; [
47]), our result shows that teamwork may shield against the negative consequences of stressors on health in the workplace. Moreover, positive team collaboration may lead to the development of strong social bonds among team members. Multiple studies to date have linked the quality of social relationships with people’s health and life expectancy [
47,
48]. Thus, our research shows that units with a good teamwork climate benefit individual employees: in such workplaces, employee health is better.
Finally, we also examined how the leader-team dyad affects SE. Because each unit had its own leader and the leaders’ ratings within the group showed similarities, we treated transformational leadership as a group-level vertical social job resource. The results demonstrated that transformational leadership did not allow us to predict individual job satisfaction or health; thus, the third hypothesis was not supported. One possible explanation for this result may be the relative importance of this construct compared to teamwork and vertical trust: by controlling for the resources that are provided by other team members and individual trust towards the organization, leadership may be less central to individual satisfaction and health. In fact, while both leader–member exchange (LMX) and team–member exchange (TMX) are associated with workplace outcomes, such as job performance or job satisfaction, a recent meta-analysis [
49] demonstrated that TMX shows incremental validity above and beyond that of LMX for some outcomes (including job satisfaction). This result shows the distinctiveness of these variables but may also imply that they have separate roles for distinct employee outcomes, as we have observed here. Another possibility relates to the power that our study had to detect this potential relationship: with only 42 healthcare units, it is probable that a low-strength relationship was less likely to be detected.
Contrary to our hypothesis, transformational leadership was linked with lower productivity. Units in which managers displayed higher levels of transformational leadership than the managers of other units displayed lower individual job performance among followers than other units. This result largely contradicts previous studies, where transformational leadership in general is positively related to individual-level follower performance (for a meta-analysis see: [
50]). We reanalyzed our data to examine the sole influence of transformational leadership on job performance (with vertical trust and teamwork excluded from the model), and we found that, on its own, transformational leadership is indeed a significant and positive predictor of job performance. The change in the influence of transformational leadership on job performance upon the inclusion of the other variables in the model may represent a case of a ‘suppression effect’, where a variable becomes a more efficient predictor of the criterion when another variable is included [
51,
52]. Transformational leadership, vertical trust, and teamwork may all have reciprocal relationships. In this case, when other influences are controlled by adding vertical trust and teamwork to the equation, then the direct effect of transformational leadership is seen to increase to a more genuine level. However, because we did not hypothesize such a link, the mechanism explaining the possible negative link between transformational leadership and job performance should be investigated in future research.
To sum up, this paper makes three contributions to the existing literature. First, we investigate the role of distinct levels of social job resources for SE in healthcare. Although scholars recognize the complexity of organizational life, i.e., the fact that companies comprise different structural or hierarchical levels, job resources (as well as demands) have mostly been investigated at the individual level [
53]. While models that focus on the individual level have been valuable, it is still necessary to understand and model group (i.e., contextual) factors that affect an individual’s functioning in the workplace [
54]. By acknowledging the common psychosocial work environment that employees share in their units, we can more accurately capture the complexity of organizational phenomena and develop more sophisticated theoretical models. SE itself is a multilevel phenomenon that may have predictors located at many levels of the workplace. Thus, we extend the previous literature by exploring social job resources located at both the individual and group levels. Second, we examine how social job resources operate in distinct planes of organizational life, i.e., how they are exchanged in both vertical and horizontal axes. Including these different directions is important because it allows us to capture the meaning of organizational, managerial, and peer influences in the workplace. Finally, while the meaning of social support for employee well-being and organizational behaviors has received wide attention from scholars [
55], and in the healthcare setting [
56], here, we further the theory on other social job resources, i.e., vertical trust, teamwork, and transformational leadership, and their link with distinct facets of SE. While many studies addressed the importance of the factors that we chose here [
29,
30,
31,
32,
33,
34], to the best of our knowledge, no previous attempt was made to understand their joint effects as ‘social job resources’ and thus their relative importance in determining SE. Understanding which factors are more important to create SE is important from a practical view as it may indicate which goals interventions should target.
4.2. Practical Implications
The implementation of policies and practices aiming at developing staff’s employability is a valuable strategy to ensure employees’ commitment and productivity over time. Productivity, health, and well-being have been found to be related reciprocally [
7,
57]; thus, finding factors such as social resources that improve the quality of work and working conditions for employees’ health and well-being can ultimately equate to finding ways to achieve the high job performance that healthcare organizations strive for. Combined with other research [
15], our study points to the importance of building a pool of social job resources in the healthcare setting as a means of increasing SE. Thus, we propose that facilitating the creation of a resourceful work environment through top–down redesign strategies, leadership processes or human resource management and human resource development practices should be an important organizational aim.
More specifically, our results point to the importance of vertical trust in shaping all facets of employability, and thus, underline the role of integrity and fairness in the organizational conduct. The quantity as well as quality of organizational communication may be one mean to increase vertical trust [
58]. The information that is conveyed should provide not only clarity but also reinforce predictability of the work situation [
59]. When employees observe coherence between organizational communication and actual practice, employees tend to trust information from the management. Trust is especially important in healthcare, where changes aimed at optimizing patient care are introduced frequently. The uncertainty related to the change process may make employees especially attuned to the matters of fairness [
60,
61]. Managers should ensure accountability with clear performance standards that apply equally to everyone. Thus, our results call for following procedural, informational, and interpersonal justice rules [
62] as means of increasing SE. Moreover, alignment of the information given with organizational actions might be an important strategy to maintain or increase vertical trust in the long run [
63].
Next, our research demonstrates the relevance of promoting good teamwork to enhance individual health and performance at work. Teamwork is particularly relevant in healthcare given that patient care is a group effort [
32]. Coordination can be facilitated by providing appropriate channels of communication and ensuring the existence of project management supportive tools among the team members with clear divisions of tasks and deadlines. Teams could also learn about constructive feedback, problem-solving strategies, and ways of overcoming interpersonal conflicts. To provide an adequate context for teamwork, an organizational incentive system and a leadership that requires and rewards teamwork should be in place to facilitate teamwork in the long run.
Interestingly, transformational leadership demonstrated having a less profound role for employee job satisfaction and health than teamwork. This pattern of results suggests the need to ensure that social job resources can be exchanged in a horizontal direction, i.e., between teammates, because these resources may be more readily available and accessible, and thus exert a stronger impact on employee health and well-being. Therefore, programs that allow employees to develop their social skills are warranted. Another practical implication may involve individuals being proactive in reaching for social job resources, e.g., developing high quality social connections [
64].
Finally, the present study demonstrates that it is vital to acknowledge the level at which social resources function to understand and, in the long run, modify employee outcomes through designing and implementing interventions in the workplace that target the level in which these resources operate: at the individual, group or organizational level. [
65]. In a recent review on interventions to promote sustainable employability, seven different studies were identified [
66]. However, the majority of interventions were delivered at the individual level, e.g., where employees participated in individual training sessions with a physical therapist [
67]. Based on our finding that vertical trust and teamwork affect SE over time, interventions on the group or even organizational level might be more fruitful to increase SE. In addition to targeting the source on the appropriate level, interventions at the group or organizational level also have the benefit of reaching larger groups of employees in a structured and uniform way by targeting the organization, management, and design of work [
68]. Examples of these kinds of organizational interventions are training that target team-based burnout, teamwork, or implementation leadership [
26,
69,
70].
4.3. Limitations
Despite the contribution this paper makes to research on social job resources and employment sustainability, we must note several limitations of this study. First, our study measures were based on self-reports. These declarative and one-source data may be subject to bias due to common method variance (CMV) [
71]. To reduce this possibility, predictors have been aggregated over measurement occasions, and teamwork and transformational leadership have also been aggregated across the units to eliminate individual variance in group-level measures while maintaining the variability of the outcome variables. These precautions decrease but do not preclude the possibility that CMV affected the pattern of results in this study. Therefore, future research might include distinct measurement methods (e.g., objective performance reports) or sources of information (e.g., colleagues).
Next, the fact that the measurements were made during an active intervention may raise concern about the influence that the intervention itself had on the relationships we observed. One may argue, for instance, that social job resources might become especially relevant in times of stress [
55]. If this is the case, then the time of organizational change may have elevated the importance of social job resources as predictors in our study. However, it is important to note that it is hardly ever the case that nothing truly happens in the organization for a year. In fact, healthcare in Sweden is a workplace in which organizational changes and interventions occur on a regular basis: continuous changes to employees’ work practices are introduced so that patients are able to receive updated and high quality care [
72]. Therefore, the measurements we made happened in healthcare’s natural environment, and we believe that the shape of the results was not affected by the ongoing intervention. Moreover, the managers were trained in implementation-specific skills, and this was not directly the focus of our study variables.
In the current study, we solely focused on the motivational process as described by the JD-R model and a subset of job resources (i.e., social job resources) to predict SE. While this choice was justified given the previously discovered role of social job resources for staff retention among healthcare workers [
15], future research should develop our findings using other types of resources such as organizational (e.g., learning opportunities) or psychological resources (e.g., self-efficacy) to predict SE. In addition, the JD-R model [
16] proposes that apart from the motivational process, there is a simultaneous impairment process, wherein taxing job demands lead to employee exhaustion. While our research focused on factors promoting excellent work ability, for a fuller picture future studies should integrate both processes when investigating predictors of SE in healthcare.
Finally, this study focuses on a healthcare sample, which is a female-dominated sector in all Organisation for Economic Co-operation and Development (OECD) countries [
73]. Future studies should replicate our results in other countries as well as test if the relations of social resources and SE are similar in other female-dominated sectors, such as education.
4.4. Future Directions
SE occurs when employees are able to continue working productively and making valuable contributions throughout their lives while retaining their health and well-being [
3]. This conceptualization led us to differentiate three components of SE: productivity, health, and well-being. Researchers also argue that—apart from positive attitudes, job motivation, and psychological well-being—SE requires having the right competences for one’s work [
3,
66,
74]. Thus, given the long-term perspective of SE, employees should also possess the capability to continuously learn and develop their competences [
74,
75]. Future research may, therefore, investigate to what extent social resources may be beneficial to learning at the workplace that leads to sustainable employability. For one thing, knowledge sharing is a behavior in a team that may inspire such development [
76], and research demonstrates that trust is critical for knowledge sharing in teams [
77]. Similarly, team climate and empowering leadership are linked with individuals’ knowledge-sharing behaviors [
78]. Research should also examine other types of social job resources that may be specifically focused on learning and investigate their role for SE. For instance, mentoring may be viewed as a vertical top–down social job resource aimed at developing capabilities for future roles. It would be worth exploring to what extent mentoring opportunities allow the long-term goal of SE to be achieved.
In future research in this area, attention should be given to identifying what kind of organizational culture and leadership styles promote the presence and exchange of social job resources in the workplace. For example, a manager’s emotional intelligence may play a role in incorporating the focus on relations (and not just tasks) in the workplace [
79], and thus may promote the development of social job resources in that unit. Another important avenue would be to identify which social job resources are actually malleable and to what extent. This will enable HR practitioners and managers in the healthcare sector to apply evidence-based initiatives.
Organizational decision-makers may face a dilemma between stimulating workers’ employability and retaining them [
80]. Indeed, employees who are highly skilled may be motivated to find a new employment outside the organization if they are dissatisfied. It is possible, however, that the social job resources we investigated may act as “pull” factors affecting employees’ intentions to stay, because they satisfy the need for affiliation and relatedness. Social factors are among the most common influencers of staff retention [
15]. Future research could, thus, inspect the joint effects of organizational climate that emphasizes development for employability along with building social ties to examine whether the presence of social job resources can protect against actual turnover for highly employable workers.
Further, the focus of SE is a long-term perspective, i.e., future employability of employees regardless of how close they are to retirement. Future research should focus on investigating how social job resources are related to the length of working careers and, for example, if they can prevent early retirement. As loneliness often occurs among the elderly [
81], an opportunity to cultivate social bonds may be an important motivator to keep working.
SE is a mutual responsibility of both organizations and individuals. While organizational-level interventions have been acknowledged as optimal to tackle the problem of stress in the workplace [
82], it has simultaneously been recognized that employees themselves can also actively shape the demands and resources of their jobs to better adjust them to their preferences [
83]. This employee-driven solution to job redesign has been named job crafting. Through job crafting, employees can alter the characteristics of their jobs to answer their need for optimal levels of job demands and job resources. In fact, one type of job-crafting behavior is ‘increasing one’s social job resources’ [
84]. This goal can be achieved by, e.g., asking colleagues for help with task execution or seeking manager feedback about one’s competencies. Therefore, employees can proactively introduce the proper amount of social job resources to their environment as a bottom–up form of intervention in the workplace. Similarly, research points to the possibility of team crafting [
85,
86] by which employees collaboratively shape their demands and resources to achieve their group goals. Given these multiple potential ways to introduce optimal amounts of social job resources in the workplace, future research should investigate how top–down and bottom–up interventions that target social job resources can jointly affect the work environment in healthcare.
Social job resources should be introduced in a way that makes them functional to both employee well-being and organizational aims. If, at some point, interpersonal relations become more important than, e.g., the quality of work or productivity, the organizational goals may suffer. For instance, a psychological phenomenon called ‘groupthink’ [
87] describes a dysfunctional situation that occurs within a group in which the desire for group harmony and a tendency to avoid conflict result in irrational decision-making outcomes [
88]. It is therefore important to introduce productive forms of teamwork, where team members are open to discussing opposite points of view and deal with conflicts in an effective way. Furthermore, some individuals may not be motivated to seek more social job resources (e.g., supervisory feedback) to balance job demands and perform better but to satisfy their egos. In fact, Roczniewska and Bakker [
89] showed that employees who score high in narcissism tend to seek social job resources as a way to boost their self-esteem; because they strive for admiration, narcissists want this self-love to be reinforced by others [
90]. Therefore, when these individuals ask for feedback and guidance, they may actually unnecessarily consume a leader’s time, which is counterproductive. Are there any other downsides to an abundance of social job resources in the workplace? This topic seems understudied, and thus, we encourage future researchers to explore this phenomenon.
Achieving SE is a timely challenge for the healthcare sector in many countries. In this paper, we demonstrated that social job resources that operate at distinct levels and in different planes of organizational structure can substantially affect how satisfied, healthy, and productive employees are in these settings. By acknowledging the multiple levels and directions at which social job resources operate, we build a better understanding of the complexities of organizational life, and we can introduce occupational health interventions that address problems at the right level.




{kind=link}