Maternal Exposure to Ambient Air Pollution and Risk of Preeclampsia: A Population-Based Cohort Study in Scania, Sweden

 and
and 
Abstract
:1. Introduction
2. Materials and Methods
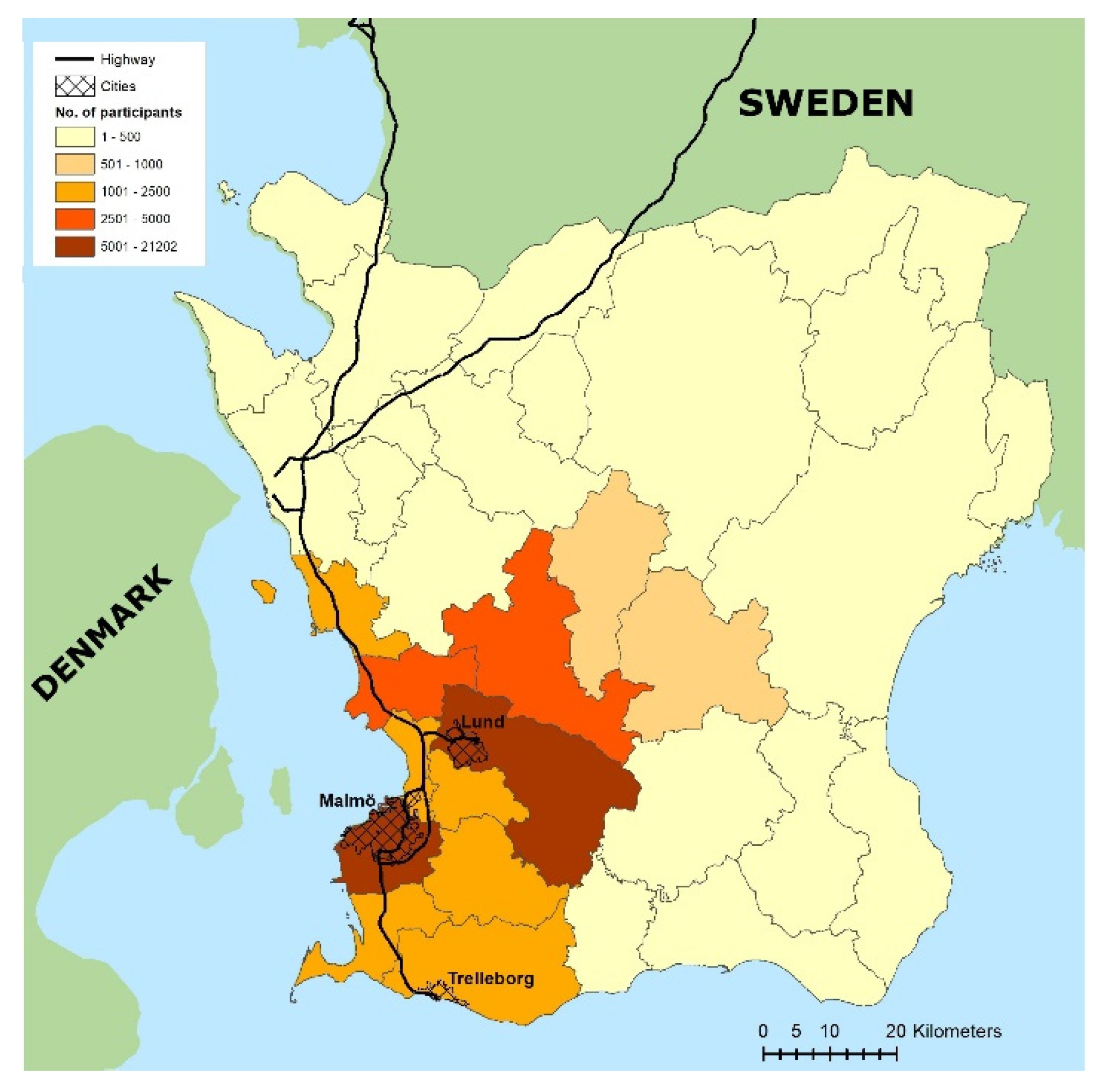
2.1. Study Design and Setting
2.2. Exposure Assessment
2.3. Variables
2.3.1. Outcome Variable
2.3.2. Exposure Variable
2.3.3. Predictors
2.4. Statistical Methods
2.5. Ethics Approval
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cohen, A.J.; Brauer, M.; Burnett, R.; Anderson, H.R.; Frostad, J.; Estep, K.; Balakrishnan, K.; Brunekreef, B.; Dandona, L.; Dandona, R.; et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the Global Burden of Diseases Study 2015. Lancet 2017, 389, 1907–1918. [Google Scholar] [CrossRef] [Green Version]
- WHO. Ambient Air Pollution: A Global Assessment of Exposure and Burden of Disease; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Koman, P.D.; Hogan, K.A.; Sampson, N.; Mandell, R.; Coombe, C.M.; Tetteh, M.M.; Hill-Ashford, Y.R.; Wilkins, D.; Zlatnik, M.G.; Loch-Caruso, R.; et al. Examining Joint Effects of Air Pollution Exposure and Social Determinants of Health in Defining “At-Risk” Populations Under the Clean Air Act: Susceptibility of Pregnant Women to Hypertensive Disorders of Pregnancy. World Med. Health Policy 2018, 10, 7–54. [Google Scholar] [CrossRef] [PubMed]
- Westergaard, N.; Gehring, U.; Slama, R.; Pedersen, M. Ambient air pollution and low birth weight - are some women more vulnerable than others? Env. Int 2017, 104, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Malley, C.S.; Kuylenstierna, J.C.I.; Vallack, H.W.; Henze, D.K.; Blencowe, H.; Ashmore, M.R. Preterm birth associated with maternal fine particulate matter exposure: A global, regional and national assessment. Environ. Int. 2017, 101, 173–182. [Google Scholar] [CrossRef]
- Pedersen, M.; Giorgis-Allemand, L.; Bernard, C.; Aguilera, I.; Andersen, A.M.; Ballester, F.; Beelen, R.M.; Chatzi, L.; Cirach, M.; Danileviciute, A.; et al. Ambient air pollution and low birthweight: A European cohort study (ESCAPE). Lancet. Respir. Med. 2013, 1, 695–704. [Google Scholar] [CrossRef]
- Pedersen, M.; Stayner, L.; Slama, R.; Sorensen, M.; Figueras, F.; Nieuwenhuijsen, M.J.; Raaschou-Nielsen, O.; Dadvand, P. Ambient air pollution and pregnancy-induced hypertensive disorders: A systematic review and meta-analysis. Hypertension 2014, 64, 494–500. [Google Scholar] [CrossRef] [Green Version]
- Brown, M.A.; Magee, L.A.; Kenny, L.C.; Karumanchi, S.A.; McCarthy, F.P.; Saito, S.; Hall, D.R.; Warren, C.E.; Adoyi, G.; Ishaku, S. The hypertensive disorders of pregnancy: ISSHP classification, diagnosis & management recommendations for international practice. Pregnancy Hypertens. 2018, 13, 291–310. [Google Scholar] [CrossRef]
- Maher, G.M.; O’Keeffe, G.W.; Kearney, P.M.; Kenny, L.C.; Dinan, T.G.; Mattsson, M.; Khashan, A.S. Association of Hypertensive Disorders of Pregnancy With Risk of Neurodevelopmental Disorders in Offspring: A Systematic Review and Meta-analysis. JAMA Psychiatry 2018, 75, 809–819. [Google Scholar] [CrossRef] [Green Version]
- Nomura, Y.; John, R.M.; Janssen, A.B.; Davey, C.; Finik, J.; Buthmann, J.; Glover, V.; Lambertini, L. Neurodevelopmental consequences in offspring of mothers with preeclampsia during pregnancy: Underlying biological mechanism via imprinting genes. Arch. Gynecol. Obstet. 2017, 295, 1319–1329. [Google Scholar] [CrossRef]
- Say, L.; Chou, D.; Gemmill, A.; Tuncalp, O.; Moller, A.B.; Daniels, J.; Gulmezoglu, A.M.; Temmerman, M.; Alkema, L. Global causes of maternal death: A WHO systematic analysis. Lancet. Glob. Health 2014, 2, e323–e333. [Google Scholar] [CrossRef] [Green Version]
- Walker, C.K.; Krakowiak, P.; Baker, A.; Hansen, R.L.; Ozonoff, S.; Hertz-Picciotto, I. Preeclampsia, Placental Insufficiency, and Autism Spectrum Disorder or Developmental Delay. JAMA Pediatrics 2015, 169, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Redman, C.W.; Sargent, I.L.; Staff, A.C. IFPA Senior Award Lecture: Making sense of pre-eclampsia – Two placental causes of preeclampsia? Placenta 2014, 35, S20–S25. [Google Scholar] [CrossRef] [PubMed]
- Redman, C.W. Current topic: Pre-eclampsia and the placenta. Placenta 1991, 12, 301–308. [Google Scholar] [CrossRef]
- Hansson, S.R.; Naav, A.; Erlandsson, L. Oxidative stress in preeclampsia and the role of free fetal hemoglobin. Front. Physiol. 2014, 5, 516. [Google Scholar] [CrossRef] [Green Version]
- Harmon, A.C.; Cornelius, D.C.; Amaral, L.M.; Faulkner, J.L.; Cunningham, M.W.; Wallace, K.; LaMarca, B. The role of inflammation in the pathology of preeclampsia. Clin. Sci. 2016, 130, 409–419. [Google Scholar] [CrossRef] [Green Version]
- Huppertz, B. The critical role of abnormal trophoblast development in the etiology of preeclampsia. Curr. Pharm. Biotechnol. 2018, 19, 771–780. [Google Scholar] [CrossRef]
- Hu, H.; Ha, S.; Roth, J.; Kearney, G.; Talbott, E.O.; Xu, X. Ambient Air Pollution and Hypertensive Disorders of Pregnancy: A Systematic Review and Meta-analysis. Atmos. Environ. 2014, 97, 336–345. [Google Scholar] [CrossRef] [Green Version]
- Lee, P.C.; Roberts, J.M.; Catov, J.M.; Talbott, E.O.; Ritz, B. First trimester exposure to ambient air pollution, pregnancy complications and adverse birth outcomes in Allegheny County, PA. Matern. Child. Health J. 2013, 17, 545–555. [Google Scholar] [CrossRef]
- Malmqvist, E.; Jakobsson, K.; Tinnerberg, H.; Rignell-Hydbom, A.; Rylander, L. Gestational diabetes and preeclampsia in association with air pollution at levels below current air quality guidelines. Environ. Health Perspect 2013, 121, 488–493. [Google Scholar] [CrossRef] [Green Version]
- Olsson, D.; Mogren, I.; Forsberg, B. Air pollution exposure in early pregnancy and adverse pregnancy outcomes: A register-based cohort study. BMJ Open 2013, 3. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, M.; Halldorsson, T.I.; Olsen, S.F.; Hjortebjerg, D.; Ketzel, M.; Grandstrom, C.; Raaschou-Nielsen, O.; Sorensen, M. Impact of Road Traffic Pollution on Pre-eclampsia and Pregnancy-induced Hypertensive Disorders. Epidemiology 2017, 28, 99–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pereira, G.; Haggar, F.; Shand, A.W.; Bower, C.; Cook, A.; Nassar, N. Association between pre-eclampsia and locally derived traffic-related air pollution: A retrospective cohort study. J. Epidemiol. Community Health 2013, 67, 147–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Q.; Zhang, H.; Liang, Q.; Knibbs, L.D.; Ren, M.; Li, C.; Bao, J.; Wang, S.; He, Y.; Zhu, L.; et al. Effects of prenatal exposure to air pollution on preeclampsia in Shenzhen, China. Environ. Pollut. 2018, 237, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Dadvand, P.; Figueras, F.; Basagaña, X.; Beelen, R.; Martinez, D.; Cirach, M.; Schembari, A.; Hoek, G.; Brunekreef, B.; Nieuwenhuijsen, M.J. Ambient air pollution and preeclampsia: A spatiotemporal analysis. Environ. Health Perspect. 2013, 121, 1365–1371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dadvand, P.; Ostro, B.; Amato, F.; Figueras, F.; Minguillón, M.C.; Martinez, D.; Basaganã, X.; Querol, X.; Nieuwenhuijsen, M. Particulate air pollution and preeclampsia: A source-based analysis. Occup. Environ. Med. 2014, 71, 570–577. [Google Scholar] [CrossRef] [PubMed]
- Madsen, C.; Haberg, S.E.; Aamodt, G.; Stigum, H.; Magnus, P.; London, S.J.; Nystad, W.; Nafstad, P. Preeclampsia and Hypertension During Pregnancy in Areas with Relatively Low Levels of Traffic Air Pollution. Matern. Child. Health J. 2018, 22, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Savitz, D.A.; Elston, B.; Bobb, J.F.; Clougherty, J.E.; Dominici, F.; Ito, K.; Johnson, S.; McAlexander, T.; Ross, Z.; Shmool, J.L.; et al. Ambient Fine Particulate Matter, Nitrogen Dioxide, and Hypertensive Disorders of Pregnancy in New York City. Epidemiology 2015, 26, 748–757. [Google Scholar] [CrossRef] [Green Version]
- Wesselink, A.K.; Carwile, J.L.; Fabian, M.P.; Winter, M.R.; Butler, L.J.; Mahalingaiah, S.; Aschengrau, A. Residential Proximity to Roadways and Ischemic Placental Disease in a Cape Cod Family Health Study. Int J. Environ. Res. Public Health 2017, 14, 682. [Google Scholar] [CrossRef]
- SCB. Population in the Country, Counties and Municipalities on 31/12/2017 and Population Change in 2017. Available online: http://www.scb.se/en/finding-statistics/statistics-by-subject-area/population/population-composition/population-statistics/pong/tables-and-graphs/yearly-statistics--municipalities-counties-and-the-whole-country/population-in-the-country-counties-and-municipalities-on-31122017-and-population-change-in-2017/ (accessed on 12 September 2018).
- Malmqvist, E.; Liew, Z.; Källén, K.; Rignell-Hydbom, A.; Rittner, R.; Rylander, L.; Ritz, B. Fetal growth and air pollution—A study on ultrasound and birth measures. Environ. Res. 2017, 152, 73–80. [Google Scholar] [CrossRef] [Green Version]
- Socialstyrelsen. The Swedish Medical Birth Register—A Summary of Content and Quality; Centre for Epidemiology, The National Board of Health and Welfare: Stockholm, Sweden, 2003; p. 33. [Google Scholar]
- Malmqvist, E.; Rittner, R.; Stroh, E.; Spanne, M.; Gustafsson, S. Dispersion Modelling for Particles in Scania; Arbets- och Miljömedicin Syd Miljöförvaltningen Malmö Stad: Malmö, Sweden, 2016. [Google Scholar]
- Gustafsson, S. Uppbyggnad och Validering av Emissionsdatabas Avseende Luftföroreningar för Skåne med Basår 2001; Lund University: Lund, Sweden, 2007. [Google Scholar]
- Windmark, F.; Jakobsson, M.; Segersson, D.; Andersson, C. Underlag till Uppskattning av Marginalkostnader för Svensk Sjöfart: Modellering av ozon, Sekundära Partiklar och Deposition av Svavel och Kväve; SMHI: Norrköping, Sweden, 2016. [Google Scholar]
- Socialstyrelsen. ICD-10-SE. Available online: http://www.socialstyrelsen.se/publikationer2018/2018-4-13 (accessed on 20 September 2018).
- Petzold, A.; Ogren, J.A.; Fiebig, M.; Laj, P.; Li, S.-M.; Baltensperger, U.; Holzer-Popp, T.; Kinne, S.; Pappalardo, G.; Sugimoto, N.; et al. Recommendations for reporting "black carbon" measurements. Atmos. Chem. Phys. 2013, 13, 8365–8379. [Google Scholar] [CrossRef] [Green Version]
- Spong, C.Y. Defining “term” pregnancy: Recommendations from the defining “term” pregnancy workgroup. JAMA 2013, 309, 2445–2446. [Google Scholar] [CrossRef] [PubMed]
- Khalil, A.; Syngelaki, A.; Maiz, N.; Zinevich, Y.; Nicolaides, K.H. Maternal age and adverse pregnancy outcome: A cohort study. Ultrasound Obstet. Gynecol. Off. J. Int. Soc. Ultrasound Obstet. Gynecol. 2013, 42, 634–643. [Google Scholar] [CrossRef]
- Magee, L.A.; Helewa, M.; Rey, E.; Cote, A.M.; Douglas, J.; Gibson, P. SOGC Clinical Practice Guideline: Diagnosis, evaluation, and management of the hypertensive disorders of pregnancy. J. Obstet. Gynaecol. Can. 2008, 30, S1–S48. [Google Scholar] [CrossRef]
- Neal, S.; Mahendra, S.; Bose, K.; Camacho, A.V.; Mathai, M.; Nove, A.; Santana, F.; Matthews, Z. The causes of maternal mortality in adolescents in low and middle income countries: A systematic review of the literature. BMC Pregnancy Childbirth 2016, 16, 352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valensise, H.; Vasapollo, B.; Gagliardi, G.; Novelli, G.P. Early and Late Preeclampsia. Two Differ. Matern. Hemodynamic States Latent Phase Dis. 2008, 52, 873–880. [Google Scholar] [CrossRef] [Green Version]
- Wright, D.; Syngelaki, A.; Akolekar, R.; Poon, L.C.; Nicolaides, K.H. Competing risks model in screening for preeclampsia by maternal characteristics and medical history. Am. J. Obstet. Gynecol. 2015, 213. [Google Scholar] [CrossRef]
- Greenland, S.; Pearl, J.; Robins, J.M. Causal diagrams for epidemiologic research. Epidemiology 1999, 10, 37–48. [Google Scholar] [CrossRef]
- EU. Directive 2008/50/EC of the European Parliament and of the council of 21 May 2008 on ambient air quality and cleaner air for Europe. Off. J. Eur. Union 2008, 152, 1–44. [Google Scholar]
- Burton, G.J.; Yung, H.W.; Cindrova-Davies, T.; Charnock-Jones, D.S. Placental endoplasmic reticulum stress and oxidative stress in the pathophysiology of unexplained intrauterine growth restriction and early onset preeclampsia. Placenta 2009, 30, S43–S48. [Google Scholar] [CrossRef] [Green Version]
- Redman, C.W.G.; Staff, A.C. Preeclampsia, biomarkers, syncytiotrophoblast stress, and placental capacity. Am. J. Obstet. Gynecol. 2015, 213, S9.e1–S9.e4. [Google Scholar] [CrossRef]
- Weldy, C.S.; Liu, Y.; Liggitt, H.D.; Chin, M.T. In Utero Exposure to Diesel Exhaust Air Pollution Promotes Adverse Intrauterine Conditions, Resulting in Weight Gain, Altered Blood Pressure, and Increased Susceptibility to Heart Failure in Adult Mice. PLoS ONE 2014, 9, e88582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nawrot, T.S.; Saenen, N.D.; Schenk, J.; Janssen, B.G.; Motta, V.; Tarantini, L.; Cox, B.; Lefebvre, W.; Vanpoucke, C.; Maggioni, C.; et al. Placental circadian pathway methylation and in utero exposure to fine particle air pollution. Environ. Int. 2018, 114, 231–241. [Google Scholar] [CrossRef] [PubMed]
- Abraham, E.; Rousseaux, S.; Agier, L.; Giorgis-Allemand, L.; Tost, J.; Galineau, J.; Hulin, A.; Siroux, V.; Vaiman, D.; Charles, M.A.; et al. Pregnancy exposure to atmospheric pollution and meteorological conditions and placental DNA methylation. Environ. Int. 2018, 118, 334–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.-L.; Yang, H.-L.; Shiao, S. Meta-Prediction of MTHFR Gene Polymorphisms and Air Pollution on the Risk of Hypertensive Disorders in Pregnancy Worldwide. Int. J. Environ. Res. Public Health 2018, 15, 326. [Google Scholar] [CrossRef] [Green Version]
- Correa, P.J.; Palmeiro, Y.; Soto, M.J.; Ugarte, C.; Illanes, S.E. Etiopathogenesis, prediction, and prevention of preeclampsia. Hypertens. Pregnancy 2016, 35, 280–294. [Google Scholar] [CrossRef]
- Labarrere, C.A.; DiCarlo, H.L.; Bammerlin, E.; Hardin, J.W.; Kim, Y.M.; Chaemsaithong, P.; Haas, D.M.; Kassab, G.S.; Romero, R. Failure of physiologic transformation of spiral arteries, endothelial and trophoblast cell activation, and acute atherosis in the basal plate of the placenta. Am. J. Obstet. Gynecol. 2017, 216, 287.e1–287.e16. [Google Scholar] [CrossRef] [Green Version]
- Redman, C.W.G.; Sargent, I.L. REVIEW ARTICLE: Immunology of Pre-Eclampsia. Am. J. Reprod. Immunol. 2010, 63, 534–543. [Google Scholar] [CrossRef]
- Zamudio, S. High-altitude hypoxia and preeclampsia. Front. Biosci. A J. Virtual Libr. 2007, 12, 2967–2977. [Google Scholar] [CrossRef]
- Mistry, H.D.; Kurlak, L.O.; Broughton Pipkin, F. The placental renin-angiotensin system and oxidative stress in pre-eclampsia. Placenta 2013, 34, 182–186. [Google Scholar] [CrossRef]
- Kurlak, L.O.; Mistry, H.D.; Cindrova-Davies, T.; Burton, G.J.; Broughton Pipkin, F. Human placental renin-angiotensin system in normotensive and pre-eclamptic pregnancies at high altitude and after acute hypoxia-reoxygenation insult. J. Physiol. 2016, 594, 1327–1340. [Google Scholar] [CrossRef]
- Janssen, N.A.; Gerlofs-Nijland, M.E.; Lanki, T.; Salonen, R.O.; Cassee, F.; Hoek, G.; Fischer, P.; Brunekreef, B.; Krzyzanowski, M. Health Effects of Black Carbon; WHO Regional Office for Europe: Copenhagen, Denmark, 2012. [Google Scholar]



{kind=link}
{kind=link}
| Characteristics | Non-PE, n (%) | PE, n (%) | Total, n (%) |
|---|---|---|---|
| Births | |||
| 34,536 (97.1) | 1034 (2.9) | 35,570 (100) | |
| Maternal age | |||
| ≤19 | 434 (1.3) | 17 (1.6) | 451 (1.3) |
| 20–34 | 27,508 (79.7) | 800 (77.4) | 28,308 (79.6) |
| ≥35 | 6594 (19.1) | 217 (21.0) | 6811 (19.1) |
| Parity | |||
| Nulliparous | 16,464 (47.7) | 719 (69.5) | 17,183 (48.3) |
| Parous | 18,072 (52.3) | 315 (30.5) | 18,387 (51.7) |
| Pre-pregnancy BMI | |||
| <18.5 | 899 (2.6) | 14 (1.4) | 913 (2.6) |
| 18.5–24.9 | 21,801 (63.1) | 479 (46.3) | 22,280 (62.6) |
| 25–29.9 | 8410 (24.4) | 308 (29.8) | 8718 (24.5) |
| ≥30 | 3426 (9.9) | 233 (22.5) | 3659 (10.3) |
| Smoking (cigarettes per day) | |||
| Non-smoker | 31,097 (90.0) | 964 (93.2) | 32,061 (90.1) |
| <10 | 2441 (7.1) | 48 (4.6) | 2489 (7.0) |
| ≥10 | 998 (2.9) | 22 (2.1) | 1020 (2.9) |
| Diabetes Mellitus | |||
| No | 34,317 (99.4) | 1016 (98.3) | 35,333 (99.3) |
| Yes | 219 (0.6) | 18 (1.7) | 237 (0.7) |
| Gestational Mellitus | |||
| No | 33,647 (97.4) | 975 (94.3) | 34,622 (97.3) |
| Yes | 889 (2.6) | 59 (5.7) | 948 (2.7) |
| Essential hypertension | |||
| No | 34,395 (99.6) | 1003 (97.0) | 35,398 (99.5) |
| Yes | 141 (0.4) | 31 (3.0) | 172 (0.5) |
| Gestational hypertension | |||
| No | 34,072 (98.7) | 903 (87.3) | 34,975 (98.3) |
| Yes | 464 (1.3) | 131 (12.7) | 595 (1.7) |
| Maternal education | |||
| Pre-secondary | 4500 (13.0) | 123 (11.9) | 4623 (13.0) |
| Secondary | 15,040 (43.5) | 476 (46.0) | 15,516 (43.6) |
| Post-secondary | 14,996 (43.4) | 435 (42.1) | 15,431 (43.4) |
| Household income (SEK/year) | |||
| <200,000 | 7598 (22.0) | 228 (22.1) | 7826 (22.0) |
| 200,000–300,000 | 8468 (24.5) | 277 (26.8) | 8745 (24.6) |
| 300,000–400,000 | 9712 (28.1) | 284 (27.5) | 9996 (28.1) |
| >400,000 | 8758 (25.4) | 245 (23.7) | 9003 (25.3) |
| Maternal country of birth | |||
| Nordic country | 25,433 (73.6) | 815 (78.8) | 26,248 (73.8) |
| Other country | 9103 (26.4) | 219 (21.2) | 9322 (26.2) |
| Fetal sex | |||
| Male | 17,667 (51.2) | 544 (52.6) | 18,211 (51.2) |
| Female | 16,869 (48.8) | 490 (47.4) | 17,359 (48.8) |
| Year of birth | |||
| 2000 | 2858 (8.3) | 67 (6.5) | 2925 (8.2) |
| 2001 | 3172 (9.2) | 93 (9.0) | 3265 (9.2) |
| 2002 | 3432 (9.9) | 101 (9.8) | 3533 (9.9) |
| 2003 | 3723 (10.8) | 76 (7.4) | 3799 (10.7) |
| 2004 | 3742 (10.8) | 100 (9.7) | 3842 (10.8) |
| 2005 | 3583 (10.4) | 117 (11.3) | 3700 (10.4) |
| 2006 | 3491 (10.1) | 144 (13.9) | 3635 (10.2) |
| 2007 | 3937 (11.4) | 120 (11.6) | 4057 (11.4) |
| 2008 | 3903 (11.3) | 123 (11.9) | 4026 (11.3) |
| 2009 | 2695 (7.8) | 93 (9.0) | 2788 (7.8) |
| Season of birth | |||
| Winter | 7921 (22.9) | 233 (22.5) | 8154 (22.9) |
| Spring | 9115 (26.4) | 319 (30.9) | 9434 (26.5) |
| Summer | 9082 (26.3) | 230 (22.2) | 9312 (26.2) |
| Autumn | 8418 (24.4) | 252 (24.4) | 8670 (24.4) |
| Pollutant | n | Mean (SD) | Range |
|---|---|---|---|
| Black carbon | 32,341 | 0.36 (0.17) | 0.03–1.93 |
| Local PM2.5 | 30,892 | 1.56 (0.73) | 0.13–7.52 |
| Local PM10 | 31,033 | 2.92 (1.55) | 0.20–9.97 |
| Total PM2.5 | 25,050 | 11.09 (1.16) | 6.85–17.30 |
| Total PM10 | 31,039 | 15.81 (2.35) | 10.25–25.62 |
| NOx | 33,074 | 14.82 (7.62) | 1.01–47.68 |
| Pollutant | Exposure Window | Quartile 2 AOR § (95% CI) | Quartile 3 AOR § (95% CI) | Quartile 4 AOR§ (95% CI) |
|---|---|---|---|---|
| Black carbon | ||||
| Entire pregnancy | 1.17 (0.96, 1.44) | 1.32 ** (1.08, 1.62) | 1.42 ** (1.16, 1.73) | |
| 1st trimester | 1.05 (0.86, 1.28) | 1.29 * (1.06, 1.57) | 1.33 ** (1.09, 1.63) | |
| 2nd trimester | 1.19 (0.98, 1.45) | 1.16 (0.95, 1.43) | 1.50 ** (1.23, 1.82) | |
| 3rd trimester | 1.08 (0.88, 1.31) | 1.20 (0.99, 1.46) | 1.35 ** (1.11, 1.63) | |
| Local PM2.5 | ||||
| Entire pregnancy | 1.14 (0.93, 1.41) | 1.25 * (1.01, 1.53) | 1.50 ** (1.22, 1.85) | |
| 1st trimester | 1.03 (0.85, 1.26) | 1.21 * (1.00, 1.47) | 1.34 ** (1.09, 1.64) | |
| 2nd trimester | 0.96 (0.79, 1.17) | 1.04 (0.85, 1.27) | 1.28 * (1.05, 1.57) | |
| 3rd trimester | 1.27 * (1.05, 1.55) | 1.32 ** (1.08, 1.61) | 1.36 ** (1.10, 1.67) | |
| Local PM10 | ||||
| Entire pregnancy | 1.11 (0.90, 1.36) | 1.21 (0.98, 1.48) | 1.39 ** (1.13, 1.71) | |
| 1st trimester | 1.02 (0.84, 1.24) | 1.19 (0.99, 1.45) | 1.32 ** (1.07, 1.62) | |
| 2nd trimester | 1.05 (0.86, 1.28) | 1.07 (0.87, 1.30) | 1.32 ** (1.07, 1.62) | |
| 3rd trimester | 1.22* (1.00, 1.48) | 1.24 * (1.01, 1.51) | 1.43 ** (1.16, 1.76) | |
| Total PM2.5 | ||||
| Entire pregnancy | 1.05 (0.83, 1.32) | 1.25 (0.99, 1.57) | 1.40 * (1.08, 1.81) | |
| 1st trimester | 1.23 * (1.01, 1.51) | 1.17 (0.95, 1.45) | 1.24 (0.99, 1.55) | |
| 2nd trimester | 1.07 (0.86, 1.34) | 1.11 (0.88, 1.41) | 1.14 (0.90, 1.45) | |
| 3rd trimester | 1.03 (0.83, 1.27) | 1.01 (0.81, 1.27) | 1.27 * (1.02, 1.59) | |
| Total PM10 | ||||
| Entire pregnancy | 1.02 (0.83, 1.25) | 1.15 (0.93, 1.43) | 1.43 ** (1.12, 1.82) | |
| 1st trimester | 1.20 (0.99, 1.47) | 1.33 ** (1.09, 1.63) | 1.24 * (1.00, 1.54) | |
| 2nd trimester | 1.11 (0.91, 1.35) | 1.15 (0.94, 1.40) | 1.27 * (1.02, 1.57) | |
| 3rd trimester | 1.02 (0.84, 1.24) | 1.07 (0.87, 1.31) | 1.19 (0.96, 1.48) | |
| NOx | ||||
| Entire pregnancy | 1.26 * (1.04, 1.53) | 1.36 ** (1.12, 1.66) | 1.61 ** (1.32, 1.97) | |
| 1st trimester | 1.11 (0.91, 1.34) | 1.27 * (1.05, 1.54) | 1.46 ** (1.20, 1.78) | |
| 2nd trimester | 1.15 (0.95, 1.39) | 1.31 ** (1.09, 1.59) | 1.47 ** (1.21, 1.80) | |
| 3rd trimester | 1.35 ** (1.12, 1.63) | 1.23 * (1.02, 1.50) | 1.51 ** (1.24, 1.84) |
| Pollutant | Exposure Window | Quartile 2 AOR § (95% CI) | Quartile 3 AOR § (95% CI) | Quartile 4 AOR § (95% CI) |
|---|---|---|---|---|
| Black carbon | ||||
| Entire pregnancy | 1.14 (0.94, 1.39) | 1.26 * (1.03, 1.54) | 1.37 ** (1.12, 1.67) | |
| 1st trimester | 1.03 (0.85, 1.25) | 1.27 * (1.05, 1.53) | 1.30 * (1.06, 1.58) | |
| 2nd trimester | 1.16 (0.96, 1.40) | 1.14 (0.93, 1.39) | 1.45 ** (1.20, 1.76) | |
| 3rd trimester | 1.05 (0.87, 1.28) | 1.15 (0.94, 1.39) | 1.32 ** (1.09, 1.60) | |
| Local PM2.5 | ||||
| Entire pregnancy | 1.12 (0.91, 1.38) | 1.23 * (1.00, 1.51) | 1.49 ** (1.22, 1.83) | |
| 1st trimester | 1.01 (0.84, 1.23) | 1.20 * (0.99, 1.46) | 1.32 ** (1.08, 1.62) | |
| 2nd trimester | 0.94 (0.77, 1.14) | 1.03 (0.85, 1.26) | 1.27 * (1.04, 1.55) | |
| 3rd trimester | 1.24 * (1.02, 1.50) | 1.29 ** (1.06, 1.57) | 1.32 ** (1.08, 1.62) | |
| Local PM10 | ||||
| Entire pregnancy | 1.08 (0.88, 1.31) | 1.18 (0.96, 1.44) | 1.36 ** (1.11, 1.67) | |
| 1st trimester | 1.02 (0.85, 1.24) | 1.20 (0.99, 1.45) | 1.31 ** (1.07, 1.61) | |
| 2nd trimester | 1.02 (0.84, 1.24) | 1.06 (0.87, 1.29) | 1.29 * (1.05, 1.58) | |
| 3rd trimester | 1.21 (1.00, 1.47) | 1.22 (1.00, 1.48) | 1.40 ** (1.14, 1.73) | |
| Total PM2.5 | ||||
| Entire pregnancy | 1.03 (0.82, 1.30) | 1.27 * (1.01, 1.59) | 1.43 ** (1.11, 1.83) | |
| 1st trimester | 1.22 (1.00, 1.48) | 1.17 (0.95, 1.44) | 1.23 (0.99, 1.53) | |
| 2nd trimester | 1.09 (0.88, 1.36) | 1.14 (0.91, 1.44) | 1.17 (0.92, 1.48) | |
| 3rd trimester | 1.01 (0.81, 1.25) | 1.02 (0.82, 1.27) | 1.26 * (1.01, 1.57) | |
| Total PM10 | ||||
| Entire pregnancy | 1.00 (0.81, 1.22) | 1.14 (0.92, 1.40) | 1.43 ** (1.12, 1.81) | |
| 1st trimester | 1.18 (0.97, 1.44) | 1.32 ** (1.08, 1.61) | 1.23 (0.99, 1.52) | |
| 2nd trimester | 1.09 (0.90, 1.33) | 1.15 (0.94, 1.40) | 1.28 * (1.04, 1.59) | |
| 3rd trimester | 1.00 (0.82, 1.21) | 1.06 (0.87, 1.30) | 1.19 (0.97, 1.47) | |
| NOx | ||||
| Entire pregnancy | 1.23 * (1.01, 1.49) | 1.31 ** (1.08, 1.59) | 1.58 ** (1.29, 1.92) | |
| 1st trimester | 1.09 (0.90, 1.32) | 1.26 * (1.05, 1.53) | 1.42 ** (1.17, 1.72) | |
| 2nd trimester | 1.12 (0.93, 1.35) | 1.28 ** (1.06, 1.55) | 1.45 ** (1.19, 1.76) | |
| 3rd trimester | 1.34 ** (1.12, 1.61) | 1.22 * (1.01, 1.48) | 1.48 ** (1.22, 1.79) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mandakh, Y.; Rittner, R.; Flanagan, E.; Oudin, A.; Isaxon, C.; Familari, M.; Hansson, S.R.; Malmqvist, E. Maternal Exposure to Ambient Air Pollution and Risk of Preeclampsia: A Population-Based Cohort Study in Scania, Sweden. Int. J. Environ. Res. Public Health 2020, 17, 1744. https://doi.org/10.3390/ijerph17051744
Mandakh Y, Rittner R, Flanagan E, Oudin A, Isaxon C, Familari M, Hansson SR, Malmqvist E. Maternal Exposure to Ambient Air Pollution and Risk of Preeclampsia: A Population-Based Cohort Study in Scania, Sweden. International Journal of Environmental Research and Public Health. 2020; 17(5):1744. https://doi.org/10.3390/ijerph17051744
Chicago/Turabian StyleMandakh, Yumjirmaa, Ralf Rittner, Erin Flanagan, Anna Oudin, Christina Isaxon, Mary Familari, Stefan Rocco Hansson, and Ebba Malmqvist. 2020. "Maternal Exposure to Ambient Air Pollution and Risk of Preeclampsia: A Population-Based Cohort Study in Scania, Sweden" International Journal of Environmental Research and Public Health 17, no. 5: 1744. https://doi.org/10.3390/ijerph17051744