The Mediation Effect of Self–Report Physical Activity Patterns in the Relationship between Educational Level and Cognitive Impairment in Elderly: A Cross-Sectional Analysis of Chilean Health National Survey 2016–2017

 ,
,  ,
,  ,
,  ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Survey and Sample
2.3. Educational Level
2.4. Physical Activity Patterns
2.4.1. Global Level of Physical Activity
2.4.2. Leisure-Time Physical Activity
2.4.3. Commute Mode
2.4.4. Sedentary Time
2.5. Cognitive Function
2.6. Covariates
2.7. Statistical Analysis
3. Results
3.1. Demographic Analysis of the Study Population
3.2. Association between Education Level and Cognitive Impairment
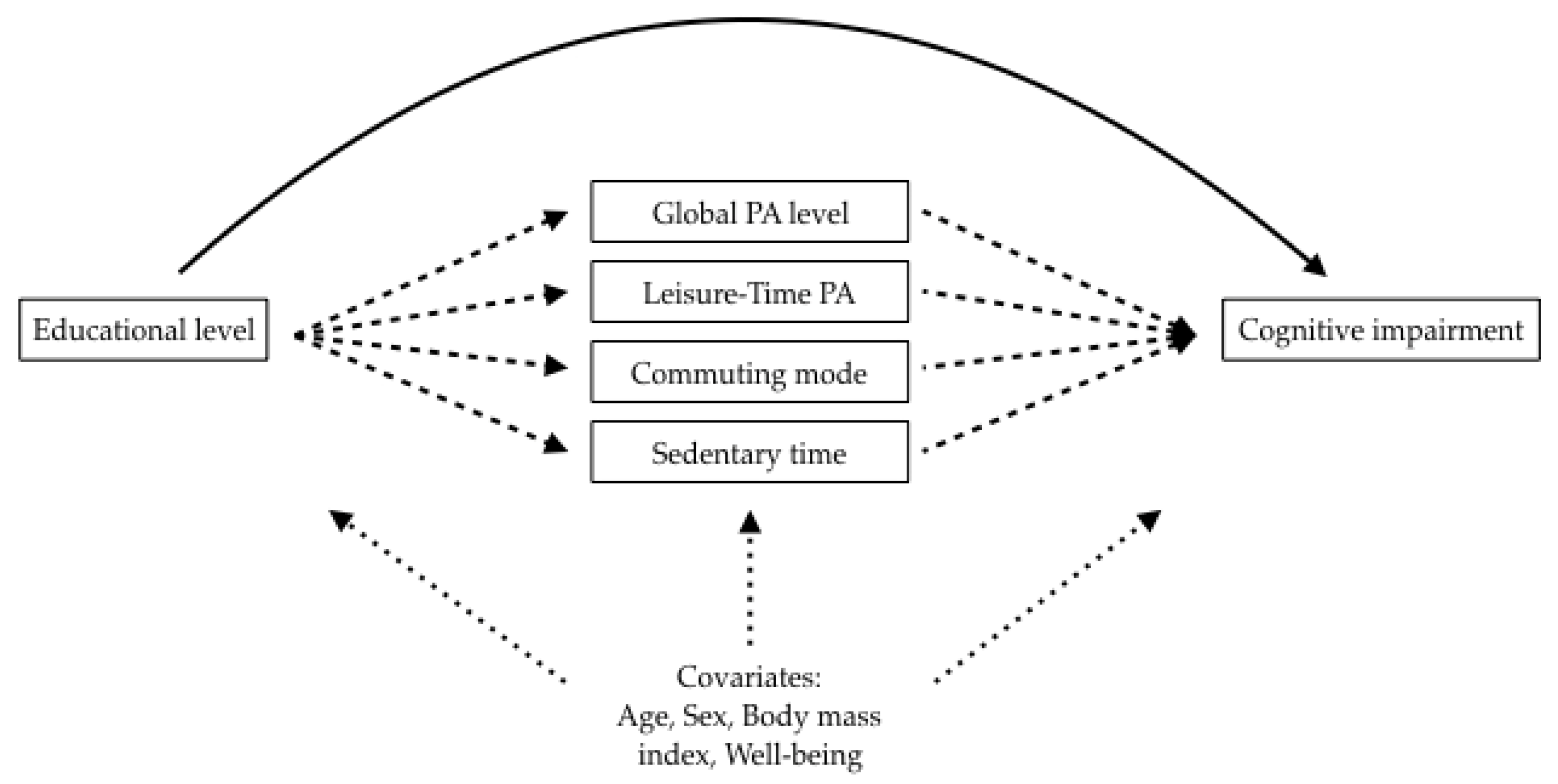
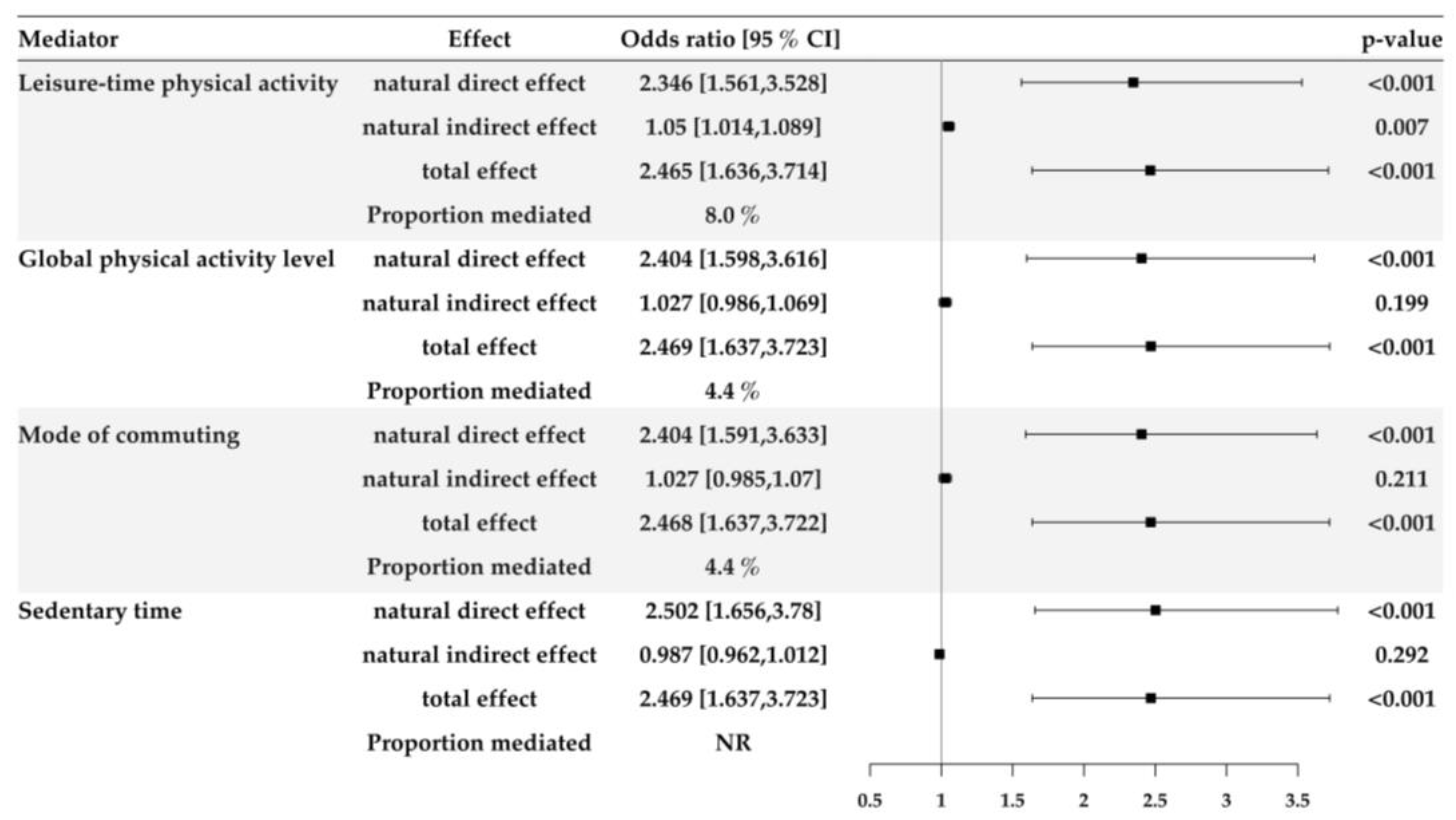
3.3. Mediation Analyses Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cahill, S. WHO’s global action plan on the public health response to dementia: Some challenges and opportunities. Aging Ment. Health 2020, 24, 197–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health, O. Global Action Plan on the Public Health Response to Dementia 2017–2025; World Health Organization: Geneva, Switzerland, 2017; ISBN 978-92-4-151348-7. [Google Scholar]
- Sherzai, D.; Sherzai, A. Preventing Alzheimer’s: Our Most Urgent Health Care Priority. Am. J. Lifestyle Med. 2019, 13, 451–461. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, A.; Ranis, G.; Stewart, F. Economic Growth and Human Development; Center Discussion Paper No. 787; Yale Economic Growth Center: New Haven, CT, USA, 1997. [Google Scholar]
- Matyas, N.; Keser Aschenberger, F.; Wagner, G.; Teufer, B.; Auer, S.; Gisinger, C.; Kil, M.; Klerings, I.; Gartlehner, G. Continuing education for the prevention of mild cognitive impairment and Alzheimer’s-type dementia: A systematic review and overview of systematic reviews. BMJ Open 2019, 9, e027719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reas, E.T.; Laughlin, G.A.; Bergstrom, J.; Kritz-Silverstein, D.; Barrett-Connor, E.; McEvoy, L.K. Effects of Sex and Education on Cognitive Change Over a 27-Year Period in Older Adults: The Rancho Bernardo Study. Am. J. Geriatr. Psychiatry 2017, 25, 889–899. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010; ISBN 978 92 4 159 997 9. [Google Scholar]
- McPhee, J.S.; French, D.P.; Jackson, D.; Nazroo, J.; Pendleton, N.; Degens, H. Physical activity in older age: Perspectives for healthy ageing and frailty. Biogerontology 2016, 17, 567–580. [Google Scholar] [CrossRef]
- Ohrnberger, J.; Fichera, E.; Sutton, M. The relationship between physical and mental health: A mediation analysis. Soc. Sci. Med. 2017, 195, 42–49. [Google Scholar] [CrossRef]
- Zhu, W.; Wadley, V.G.; Howard, V.J.; Hutto, B.; Blair, S.N.; Hooker, S.P. Objectively Measured Physical Activity and Cognitive Function in Older Adults. Med. Sci. Sports Exerc. 2017, 49, 47–53. [Google Scholar] [CrossRef] [Green Version]
- Hamer, M.; Chida, Y. Physical activity and risk of neurodegenerative disease: A systematic review of prospective evidence. Psychol. Med. 2009, 39, 3–11. [Google Scholar] [CrossRef]
- Willey, J.Z.; Gardener, H.; Caunca, M.R.; Moon, Y.P.; Dong, C.; Cheung, Y.K.; Sacco, R.L.; Elkind, M.S.; Wright, C.B. Leisure-time physical activity associates with cognitive decline: The Northern Manhattan Study. Neurology 2016, 86, 1897–1903. [Google Scholar] [CrossRef] [Green Version]
- Nazlieva, N.; Mavilidi, M.F.; Baars, M.; Paas, F. Establishing a scientific consensus on the cognitive benefits of physical activity. Int. J. Environ. Res. Public Health 2019, 17, 29. [Google Scholar] [CrossRef] [Green Version]
- Amarya, S.; Singh, K.; Sabharwal, M. Changes during aging and their association with malnutrition. J. Clin. Gerontol. Geriatr. 2015, 6, 78–84. [Google Scholar] [CrossRef] [Green Version]
- Chang, A.Y.; Skirbekk, V.F.; Tyrovolas, S.; Kassebaum, N.J.; Dieleman, J.L. Measuring population ageing: An analysis of the Global Burden of Disease Study 2017. Lancet Public Health 2019, 4, e159–e167. [Google Scholar] [CrossRef] [Green Version]
- Department of Economic and Social Affairs Population Division, U.N. World Population Ageing 2019; United Nations: New York, NY, USA, 2019; ISBN 978-92-1-148325-3. [Google Scholar]
- Rechel, B.; Grundy, E.; Robine, J.-M.; Cylus, J.; Mackenbach, J.P.; Knai, C.; McKee, M. Ageing in the European union. Lancet 2013, 381, 1312–1322. [Google Scholar] [CrossRef]
- Andersen, M.P.; Valeri, L.; Starkopf, L.; Mortensen, R.N.; Sessa, M.; Kragholm, K.H.; Vardinghus-Nielsen, H.; Boggild, H.; Lange, T.; Torp-Pedersen, C. The mediating effect of pupils’ physical fitness on the relationship between family socioeconomic status and academic achievement in a danish school cohort. Sports Med. 2019, 49, 1291–1301. [Google Scholar] [CrossRef]
- Abe, T.; Kitamura, A.; Taniguchi, Y.; Amano, H.; Seino, S.; Yokoyama, Y.; Nishi, M.; Narita, M.; Ikeuchi, T.; Fujiwara, Y.; et al. Pathway from gait speed to incidence of disability and mortality in older adults: A mediating role of physical activity. Maturitas 2019, 123, 32–36. [Google Scholar] [CrossRef]
- Van Dyck, D.; Teychenne, M.; McNaughton, S.A.; De Bourdeaudhuij, I.; Salmon, J. Relationship of the perceived social and physical environment with mental health-related quality of life in middle-aged and older adults: Mediating effects of physical activity. PLoS ONE 2015, 10, e0120475. [Google Scholar] [CrossRef]
- de Salud Pública, S. Encuesta Nacional de Salud 2016–2017 Primeros Resultados. Santiago. 2017. Available online: https://www.minsal.cl/wp-content/uploads/2017/11/ENS-2016-17_PRIMEROS-RESULTADOS.pdf (accessed on 17 March 2020).
- Armstrong, T.; Bull, F. Development of the world health organization global physical activity questionnaire (GPAQ). J. Public Health 2006, 14, 66–70. [Google Scholar] [CrossRef]
- Hallal, P.C.; Andersen, L.B.; Bull, F.C.; Guthold, R.; Haskell, W.; Ekelund, U.; Lancet Physical Activity Series Working Group. Global physical activity levels: Surveillance progress, pitfalls, and prospects. Lancet 2012, 380, 247–257. [Google Scholar] [CrossRef]
- Garcia-Hermoso, A.; Ramirez-Velez, R.; Celis-Morales, C.A.; Olloquequi, J.; Izquierdo, M. Can physical activity attenuate the negative association between sitting time and cognitive function among older adults? A mediation analysis. Exp. Gerontol. 2018, 106, 173–177. [Google Scholar] [CrossRef] [Green Version]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Quiroga, P.; Albala Brevis, C.; Klaasen, G. Validation of a Screening Test for Age Associated Cognitive Impairment, in Chile. Rev. Med. Chil. 2004, 132, 467–478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Icaza, M.G.; Albala, C. CA. Minimental State Examination: Análisis estadístico del estudio de demencia en Chile para validar una versión abreviada. In Investigaciones en Salud Publica: Documento Técnico; OPS: Washington, DC, USA, 1999. [Google Scholar]
- Moreno, X.; Lera, L.; Moreno, F.; Albala, C. Life expectancy with and without cognitive impairment among Chilean older adults: Results of the National Survey of Health (2003, 2009 and 2016). BMC Geriatr. 2019, 19, 374. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, H.M.; Tarraf, W.; Schneiderman, N.; Fornage, M.; Vasquez, P.M.; Zeng, D.; Youngblood, M.; Gallo, L.C.; Daviglus, M.L.; Lipton, R.B.; et al. Prevalence and correlates of mild cognitive impairment among diverse Hispanics/Latinos: Study of Latinos-Investigation of Neurocognitive Aging results. Alzheimers Dement. 2019, 15, 1507–1515. [Google Scholar] [CrossRef] [PubMed]
- Herkrath, F.J.; Vettore, M.V.; Werneck, G.L. Contextual and individual factors associated with dental services utilisation by Brazilian adults: A multilevel analysis. PLoS ONE 2018, 13, e0192771. [Google Scholar] [CrossRef]
- Lange, T.; Vansteelandt, S.; Bekaert, M. A simple unified approach for estimating natural direct and indirect effects. Am. J. Epidemiol. 2012, 176, 190–195. [Google Scholar] [CrossRef] [Green Version]
- Vansteelandt, S.; Bekaert, M.; Lange, T. Imputation strategies for the estimation of natural direct and indirect effects. Epidemiol. Methods 2012, 1, 131–158. [Google Scholar] [CrossRef]
- Vanderweele, T.J.; Vansteelandt, S. Odds ratios for mediation analysis for a dichotomous outcome. Am. J. Epidemiol. 2010, 172, 1339–1348. [Google Scholar] [CrossRef]
- Steen, J.; Loeys, T.; Moerkerke, B.; Vansteelandt, S. Medflex: An R package for flexible mediation analysis using natural effect models. J. Stat. Softw. 2017, 76. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Sanguinetti, M.A.; Leiva, A.M.; Petermann-Rocha, F.; Troncoso-Pantoja, C.; Villagran, M.; Lanuza-Rilling, F.; Nazar, G.; Poblete-Valderrama, F.; Diaz-Martinez, X.; Celis-Morales, C. Factors associated with cognitive impairment in older adults in Chile. Rev. Med. Chil. 2019, 147, 1013–1023. [Google Scholar] [CrossRef] [Green Version]
- Hugo, J.; Ganguli, M. Dementia and cognitive impairment: Epidemiology, diagnosis, and treatment. Clin. Geriatr. Med. 2014, 30, 421–442. [Google Scholar] [CrossRef] [Green Version]
- Kivimaki, M.; Singh-Manoux, A.; Pentti, J.; Sabia, S.; Nyberg, S.T.; Alfredsson, L.; Goldberg, M.; Knutsson, A.; Koskenvuo, M.; Koskinen, A.; et al. Physical inactivity, cardiometabolic disease, and risk of dementia: An individual-participant meta-analysis. BMJ 2019, 365, l1495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phansikar, M.; Mullen, S.P. Exploring Active Travel and Leisure-Time Physical Activity Relationships With Cognition Among Older Adults. J. Aging Phys. Act. 2019, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Rovio, S.; Kareholt, I.; Viitanen, M.; Winblad, B.; Tuomilehto, J.; Soininen, H.; Nissinen, A.; Kivipelto, M. Work-related physical activity and the risk of dementia and Alzheimer’s disease. Int. J. Geriatr. Psychiatry 2007, 22, 874–882. [Google Scholar] [CrossRef]
- Olanrewaju, O.; Stockwell, S.; Stubbs, B.; Smith, L. Sedentary behaviours, cognitive function, and possible mechanisms in older adults: A systematic review. Aging Clin. Exp. Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Maasakkers, C.M.; Claassen, J.; Gardiner, P.A.; Olde Rikkert, M.G.M.; Lipnicki, D.M.; Scarmeas, N.; Dardiotis, E.; Yannakoulia, M.; Anstey, K.J.; Cherbuin, N.; et al. The Association of Sedentary Behaviour and Cognitive Function in People Without Dementia: A Coordinated Analysis Across Five Cohort Studies from COSMIC. Sports Med. 2020, 50, 403–413. [Google Scholar] [CrossRef] [Green Version]
- Sabia, S.; Dugravot, A.; Dartigues, J.F.; Abell, J.; Elbaz, A.; Kivimaki, M.; Singh-Manoux, A. Physical activity, cognitive decline, and risk of dementia: 28 year follow-up of Whitehall II cohort study. BMJ 2017, 357, j2709. [Google Scholar] [CrossRef] [Green Version]
- Baumeister, S.-E.; Karch, A.; Bahls, M.; Teumer, A.; Leitzmann, M.; Baurecht, H. Physical activity and risk of Alzheimer’s disease: A two-sample Mendelian randomization study. bioRxiv 2019, 819821. [Google Scholar] [CrossRef]
- Winckers, A.N.; Mackenbach, J.D.; Compernolle, S.; Nicolaou, M.; van der Ploeg, H.P.; De Bourdeaudhuij, I.; Brug, J.; Lakerveld, J. Educational differences in the validity of self-reported physical activity. BMC Public Health 2015, 15, 1299. [Google Scholar] [CrossRef] [Green Version]
- Herbolsheimer, F.; Riepe, M.W.; Peter, R. Cognitive function and the agreement between self-reported and accelerometer-accessed physical activity. BMC Geriatr. 2018, 18, 56. [Google Scholar] [CrossRef]
- Folley, S.; Zhou, A.; Hypponen, E. Information bias in measures of self-reported physical activity. Int J. Obes. 2018, 42, 2062–2063. [Google Scholar] [CrossRef]
- Keating, X.D.; Zhou, K.; Liu, X.; Hodges, M.; Liu, J.; Guan, J.; Phelps, A.; Castro-Pinero, J. Reliability and Concurrent Validity of Global Physical Activity Questionnaire (GPAQ): A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 4128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stubbs, B.; Chen, L.J.; Chang, C.Y.; Sun, W.J.; Ku, P.W. Accelerometer-assessed light physical activity is protective of future cognitive ability: A longitudinal study among community dwelling older adults. Exp. Gerontol. 2017, 91, 104–109. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Cognitive Impairment (<13 mMMSE) n = 178 | Without Cognitive Impairment (≥13 mMMSE) n = 1492 | p-Value | |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| Age (years) | 75.3 ± 9.2 | 70.2 ± 7.4 | <0.001 |
| Body mass index (kg/m2) | 28 ± 4.9 | 29.3 ± 5.3 | <0.001 |
| Well-being | 2.8 ± 0.8 | 2.7 ± 0.7 | 0.02 |
| Healthy diet index | 1.8 ± 0.6 | 1.8 ± 0.6 | 0.84 |
| Sex | n (%) | n (%) | |
| Male | 73 (41) | 528 (35.4) | 0.163 |
| Female | 105 (59) | 964 (64.6) | |
| Depression treatment | |||
| Yes | 30 (16.9) | 305 (20.4) | 0.303 |
| No | 148 (83.1) | 1187 (79.6) | |
| Educational level | |||
| Primary | 129 (72.5) | 717 (48.1) | <0.001 |
| Beyond primary | 49 (27.5) | 775 (51.9) | |
| Global physical activity level * | |||
| Active | 49 (32.2) | 764 (53.8) | <0.001 |
| Inactive | 103 (67.8) | 655 (46.2) | |
| Leisure-Time physical activity * | |||
| Yes | 4 (2.6) | 162 (11.4) | 0.01 |
| No | 148 (97.4) | 1257 (88.6) | |
| Mode of commuting * | |||
| Active commuting | 46 (30.3) | 338 (23.8) | 0.09 |
| Passive commuting | 106 (69.7) | 1081 (76.2) | |
| Sedentary time * | |||
| Sedentary | 131 (86.2) | 1158 (81.6) | 0.198 |
| Non-sedentary | 21 (13.8) | 261 (28.4) |
| Explanatory Variable | Model 1 | Model 2 | Model 3 | Model 4 | ||||
|---|---|---|---|---|---|---|---|---|
| OR [95% CI] | p-Value | OR [95% CI] | p-Value | OR [95% CI] | p-Value | OR [95% CI] | p-Value | |
| Educational level | ||||||||
| Beyond primary (ref.) | 1 | 1 | 1 | 1 | ||||
| Primary | 2.846 [2.03,4.048] | <0.01 | 2.266 [1.593,3.265] | <0.01 | 2.305 [1.611,3.341] | <0.01 | 2.32 [1.62,3.366] | <0.01 |
| Age | 1.07 [1.049,1.091] | <0.01 | 1.064 [1.042,1.085] | <0.01 | 1.064 [1.042,1.086] | <0.01 | ||
| Sex (female) | 0.704 [0.507,0.981] | 0.037 | 0.737 [0.529,1.03] | 0.072 | 0.734 [0.523,1.034] | 0.075 | ||
| Well-being | 1.195 [0.966,1.476] | 0.1 | 1.199 [0.968,1.485] | 0.096 | ||||
| Body mass index | 0.96 [0.927,0.994] | 0.022 | 0.96 [0.927,0.993] | 0.021 | ||||
| Healthy diet index | 1.129 [0.853,1.494] | 0.394 | ||||||
| Depressive treatment (No) | 0.952 [0.605,1.458] | 0.826 | ||||||
| Goodness of fit | ||||||||
| AIC | 1.098.085 | 1.053.011 | 1.049.208 | 1.052.428 | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Solis-Urra, P.; Plaza-Diaz, J.; Álvarez-Mercado, A.I.; Rodríguez-Rodríguez, F.; Cristi-Montero, C.; Zavala-Crichton, J.P.; Olivares-Arancibia, J.; Sanchez-Martinez, J.; Abadía-Molina, F. The Mediation Effect of Self–Report Physical Activity Patterns in the Relationship between Educational Level and Cognitive Impairment in Elderly: A Cross-Sectional Analysis of Chilean Health National Survey 2016–2017. Int. J. Environ. Res. Public Health 2020, 17, 2619. https://doi.org/10.3390/ijerph17082619
Solis-Urra P, Plaza-Diaz J, Álvarez-Mercado AI, Rodríguez-Rodríguez F, Cristi-Montero C, Zavala-Crichton JP, Olivares-Arancibia J, Sanchez-Martinez J, Abadía-Molina F. The Mediation Effect of Self–Report Physical Activity Patterns in the Relationship between Educational Level and Cognitive Impairment in Elderly: A Cross-Sectional Analysis of Chilean Health National Survey 2016–2017. International Journal of Environmental Research and Public Health. 2020; 17(8):2619. https://doi.org/10.3390/ijerph17082619
Chicago/Turabian StyleSolis-Urra, Patricio, Julio Plaza-Diaz, Ana Isabel Álvarez-Mercado, Fernando Rodríguez-Rodríguez, Carlos Cristi-Montero, Juan Pablo Zavala-Crichton, Jorge Olivares-Arancibia, Javier Sanchez-Martinez, and Francisco Abadía-Molina. 2020. "The Mediation Effect of Self–Report Physical Activity Patterns in the Relationship between Educational Level and Cognitive Impairment in Elderly: A Cross-Sectional Analysis of Chilean Health National Survey 2016–2017" International Journal of Environmental Research and Public Health 17, no. 8: 2619. https://doi.org/10.3390/ijerph17082619