Evidences from Clinical Trials in Down Syndrome: Diet, Exercise and Body Composition

 , and
, and
Abstract
:1. Introduction
- Consumption of less healthy foods, lower levels of physical activity and medication are factors that enhance weight gain in DS [8].
2. Methods
2.1. Search Strategy and Information Processing
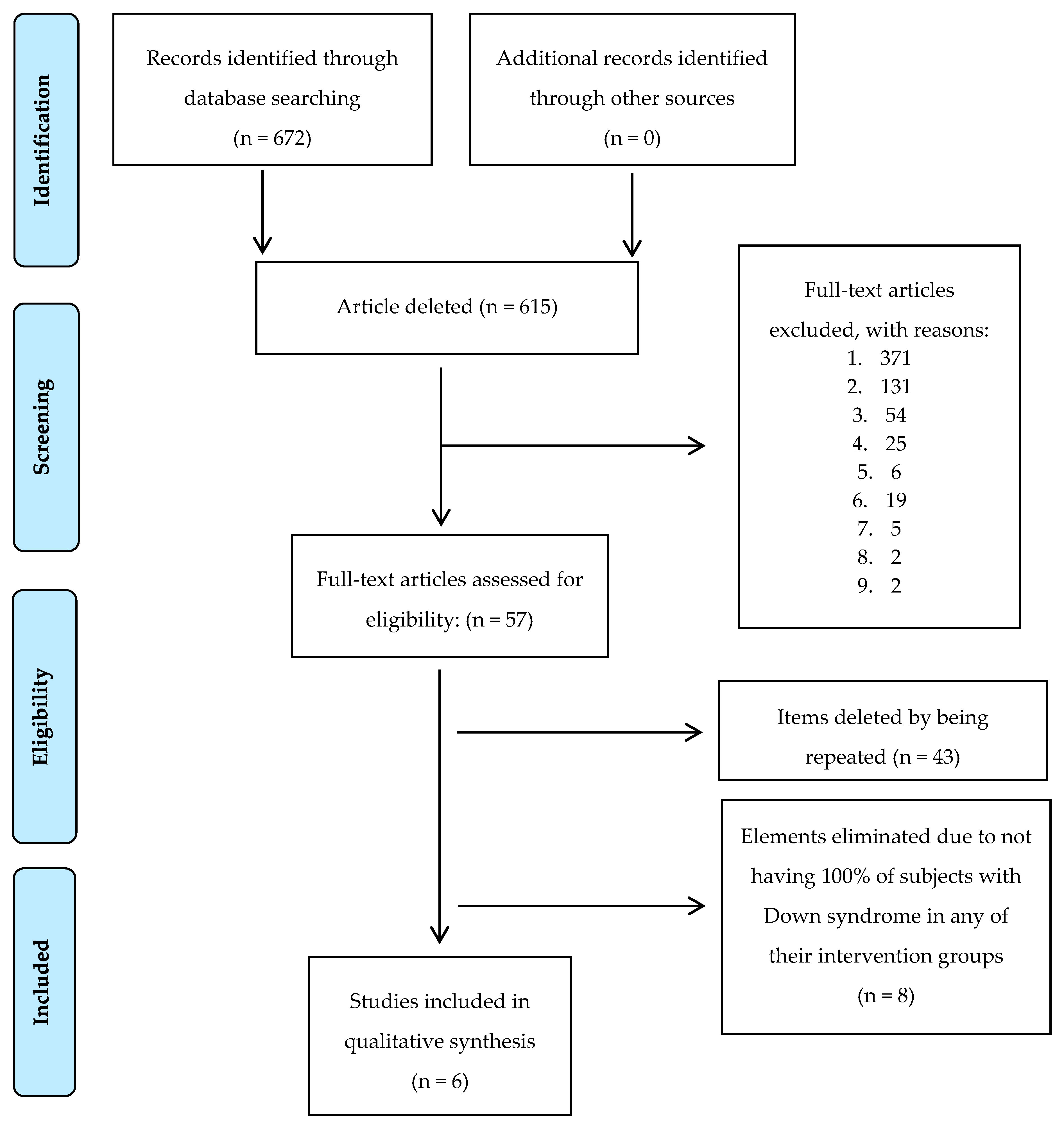
2.2. Selection of the Articles Previously Identify
- Population: characteristics of the population studied (country of origin, type of diagnostic criteria, number, age and gender), inclusion and exclusion criteria.
- Interventions: exclusive and multidisciplinary as therapeutic treatments.
- Comparators: inclusion of clinical trials, control and intervention groups are identified. In principle, only the intervention groups receive the therapeutic treatment that should cause changes in body composition.
- Results: they are identified as variation in body composition, presenting significant and not significant variations.
- Characteristics of clinical trials: authors, year of publication, type of clinical trial, duration of intervention, instrument of analysis of body composition, type of intervention used (exclusive or multidisciplinary) and body composition variation (measured with different anthropometric parameters and units of measurement).
2.3. Extraction of Data, Synthesis of Results and Risk of Loss of Information
2.4. Use of the CONSORT 2010 Methodology
2.5. Evaluation of Body Composition Measuring Instruments
3. Results
3.1. Search Features and Types of Interventions Identified
3.2. Instruments for Measuring Body Composition
3.3. Evaluation of the Design of Clinical Trials
3.4. Changes in Body Composition in Down Syndrome: Children and Adolescents
3.5. Changes in Body Composition in Down Syndrome: Adults
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Franceschi, C.; Garagnani, P.; Gensous, N.; Bacalini, M.G.; Conte, M.; Salvioli, S. Accelerated bio-cognitive aging in Down syndrome: State of the art and possible deceleration strategies. Aging Cell 2019, 18, e12903. [Google Scholar] [CrossRef] [PubMed]
- Whooten, R.; Schmitt, J.; Schwartz, A. Endocrine manifestations of Down syndrome. Curr. Opin. Endocrinol. Diabetes Obes. 2018, 25, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, B.K.; Berger, S.L.; Brunet, A.; Campisi, J.; Cuervo, A.M.; Epel, E.S.; Franceschi, C.; Lithgow, G.J.; Morimoto, R.I.; Pessin, J.E.; et al. Geroscience: Linking aging to chronic disease. Cell 2014, 159, 709–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tzanetakou, I.P.; Katsilambros, N.L.; Benetos, A.; Mikhailidis, D.P.; Perrea, D.N. Is obesity linked to aging? Ageing Res. Rev. 2012, 11, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, K.; Rimmer, J.H.; Heller, T. Obesity and associated factors in adults with intellectual disability. J. Intellect. Disabil. Res. 2013, 58, 851–863. [Google Scholar] [CrossRef]
- Bertapelli, F.; Pitetti, K.H.; Agiovlasitis, S.; Guerra-Junior, G. Overweight and obesity in children and adolescents with Down syndrome—Prevalence, determinants, consequences, and interventions: A literature review. Res. Dev. Disabil. 2016, 57, 181–192. [Google Scholar] [CrossRef]
- Brantmüller, É.; Gyuró, M.; Karácsony, I. Development of Walking and Self-sufficiency Ability Related to Nutrition among People with Down Syndrome. Pract. Theory Syst. Educ. 2015, 10, 165–176. [Google Scholar] [CrossRef] [Green Version]
- Cushing, P.; Spear, D.; Novak, P.; Rosenzweig, L.; Wallace, L.S.; Conway, C.; Wittenbrook, W.; Lemons, S.; Medlen, J.G. Academy of Nutrition and Dietetics: Standards of Practice and Standards of Professional Performance for Registered Dietitians (Competent, Proficient, and Expert) in Intellectual and Developmental Disabilities. J. Acad. Nutr. Diet. 2012, 112, 1454–1464.e35. [Google Scholar] [CrossRef]
- Frasca, D.; Blomberg, B.B. Adipose Tissue Inflammation Induces B Cell Inflammation and Decreases B Cell Function in Aging. Front. Immunol. 2017, 8, 1003. [Google Scholar] [CrossRef] [Green Version]
- Capone, G.; Chicoine, B.; Bulova, P.; Stephens, M.; Hart, S.J.; Crissman, B.; Videlefsky, A.; Myers, K.; Roizen, N.; Esbensen, A.; et al. Co-occurring medical conditions in adults with Down syndrome: A systematic review toward the development of health care guidelines. Am. J. Med. Genet. Part A 2017, 176, 116–133. [Google Scholar] [CrossRef]
- Harris, L.; Melville, C.; Murray, H.; Hankey, C. The effects of multi-component weight management interventions on weight loss in adults with intellectual disabilities and obesity: A systematic review and meta-analysis of randomised controlled trials. Res. Dev. Disabil. 2018, 72, 42–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ulijaszek, S.J.; A Kerr, D. Anthropometric measurement error and the assessment of nutritional status. Br. J. Nutr. 1999, 82, 165–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madden, A.M.; Smith, S. Body composition and morphological assessment of nutritional status in adults: A review of anthropometric variables. J. Hum. Nutr. Diet. 2014, 29, 7–25. [Google Scholar] [CrossRef] [PubMed]
- Hume, P.; Marfell-Jones, M. The importance of accurate site location for skinfold measurement. J. Sports Sci. 2008, 26, 1333–1340. [Google Scholar] [CrossRef] [PubMed]
- Nádas, J.; Putz, Z.; Kolev, G.; Nagy, S.; Jermendy, G. Intraobserver and interobserver variability of measuring waist circumference. Med. Sci. Monit. 2008, 14, 15–18. [Google Scholar]
- Gil, A.; Martínez de Victoria, E.; Maldonado, J. Tratado de Nutrición, 2nd ed.; Médica Panamericana: Madrid, Spain, 2010; Volume 3, pp. 100–131. [Google Scholar]
- Müller, M.; Braun, W.; Pourhassan, M.; Geisler, C.; Bosy-Westphal, A. Application of standards and models in body composition analysis. Proc. Nutr. Soc. 2015, 75, 181–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- The International Committee of Biomedical Journal Editors (ICMJE). Recommendations for the Preparation, Presentation, Editing and Publication of Academic Papers in Medical Journal. 2017. Available online: http://www.icmje.org/icmje-recommendations.pdf (accessed on 8 November 2019).
- Wiesman, F.; Hasman, A.; Herik, H.V.D. Information retrieval: An overview of system characteristics. Int. J. Med. Inform. 1997, 47, 5–26. [Google Scholar] [CrossRef]
- Ptomey, L.T.; Wittenbrook, W. Position of the Academy of Nutrition and Dietetics: Nutrition Services for Individuals with Intellectual and Developmental Disabilities and Special Health Care Needs. J. Acad. Nutr. Diet. 2015, 115, 593–608. [Google Scholar] [CrossRef] [PubMed]
- Rodd, C.J.; the Canadian Pediatric Endocrine Group (CPEG) Working Committee for National Growth Charts; Metzger, D.; Sharma, A.K. Extending World Health Organization weight-for-age reference curves to older children. BMC Pediatr. 2014, 14, 32. [Google Scholar] [CrossRef] [Green Version]
- The 10 Most Spoken Languages in the World. Descarga en. Available online: https://danivoiceovers.com/en/los-10-idiomas-mas-hablados-mundo/ (accessed on 16 May 2020).
- Los Idiomas, en Cifras: Cuántas Lenguas Hay en el Mundo? Europapress. Descarga en. Available online: https://www.europapress.es/sociedad/noticia-idiomas-cifras-cuantas-lenguas-hay-mundo-20190221115202.html (accessed on 16 May 2020).
- Seron, B.B.; Silva, R.A.; Greguol, M. Effects of two programs of exercise on body composition of adoles-cents with Down syndrome. Rev. Paul. Pediatr. 2014, 32, 92–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Constanza Mosso, C.; Patricia Santander, V.; Paulina Pettinelli, R.; Marcela Valdés, G.; Magdalena Celis, B.; Fabián Espejo, S. Evaluation of a physical activity intervention among children with down’s syndrome. Rev. Chil. Pediatr. 2011, 82, 311–318. [Google Scholar]
- Ordonez, F.J.; Rosety, M.; Rosety-Rodriguez, M. Influence of 12-week exercise training on fat mass per-centage in adolescents with Down syndrome. Med. Sci. Monit. 2006, 12, CR416–CR419. [Google Scholar] [PubMed]
- Boer, P.-H.; Moss, S.J. Effect of continuous aerobic vs. interval training on selected anthropometrical, physiological and functional parameters of adults with Down syndrome. J. Intellect. Disabil. Res. 2016, 60, 322–334. [Google Scholar] [CrossRef]
- Ordonez, F.J.; Fornieles, G.; Rosety, M.A.; Rosety, I.; Diaz, A.J.; Camacho, A. A Short Training Pro-gram Reduced Fat Mass and Abdominal Distribution in Obese Women with Intellectual Disability. Int. J. Morphol. 2013, 31, 570–574. Available online: https://scielo.conicyt.cl/scielo.php?script=sci_abstract&pid=S0717-95022013000200034&lng=es&nrm=iso&tlng=en (accessed on 8 November 2019). [CrossRef] [Green Version]
- Ordonez, F.J.; Fornieles-Gonzalez, G.; Camacho, A.; Rosety, M.A.; Rosety, I.; Diaz, A.J.; Rodríguez, J.R. Anti-inflammatory effect of exercise, via reduced leptin levels, in obese women with Down syndrome. Int. J. Sport Nutr. Exerc. Metab. 2012, 23, 239–244. [Google Scholar] [CrossRef]
- Ogg-Groenendaal, M.; Hermans, H.; Claessens, B. A systematic review on the effect of exercise interventions on challenging behavior for people with intellectual disabilities. Res. Dev. Disabil. 2014, 35, 1507–1517. [Google Scholar] [CrossRef]
- Shin, I.-S.; Park, E.-Y. Meta-analysis of the effect of exercise programs for individuals with intellectual disabilities. Res. Dev. Disabil. 2012, 33, 1937–1947. [Google Scholar] [CrossRef]
- Es, L.R.R.; Resende, E.S.; Diniz, A.L.D.; Penha-Silva, N.; O’Connell, J.L.; Gomes, P.F.S.; Zanetti, H.R.; Roerver-Borges, A.S.; Veloso, F.C.; De Souza, F.R.; et al. Epicardial adipose tissue and metabolic syndrome. Medicine 2018, 97, e0387. [Google Scholar] [CrossRef]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.M.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, U.G. CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. Int. J. Surg. 2012, 10, 28–55. [Google Scholar] [CrossRef] [Green Version]
- Fields, D.A.; Higgins, P.B.; Radley, D. Air-displacement plethysmography: Here to stay. Curr. Opin. Clin. Nutr. Metab. Care 2005, 8, 624–629. [Google Scholar] [CrossRef] [PubMed]
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gómez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.-C.; Pirlich, M.; et al. Bioelectrical impedance analysis-part II: Utilization in clinical practice. Clin. Nutr. 2004, 23, 1430–1453. [Google Scholar] [CrossRef] [PubMed]
- WHO. Human Genomics in Global Health. Available online: https://www.who.int/genomics/public/geneticdiseases/en/index1.html (accessed on 27 May 2020).
- Müller, M.; Bosy-Westphal, A. Effect of Over- and Underfeeding on Body Composition and Related Metabolic Functions in Humans. Curr. Diabetes Rep. 2019, 19, 108. [Google Scholar] [CrossRef] [PubMed]
- Bray, G.; E Heisel, W.; Afshin, A.; Jensen, M.D.; Dietz, W.H.; Long, M.W.; Kushner, R.F.; Daniels, S.R.; A Wadden, T.; Tsai, A.G.; et al. The Science of Obesity Management: An Endocrine Society Scientific Statement. Endocr. Rev. 2018, 39, 79–132. [Google Scholar] [CrossRef] [Green Version]
- Garvey, W.T.; Mechanick, J.I.; Brett, E.M.; Garber, A.J.; Hurley, D.L.; Jastreboff, A.M.; Nadolsky, K.; Pessah-Pollack, R.; Plodkowski, R. American Association of Clinical Endocrinologist and American College of Endocrinology Comprehensive Clinical Practice Guidelines for Medical Care of Patients with obesity. Endocr. Pract. 2016, 22, 1–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yumuk, V.; Tsigos, C.; Fried, M.; Schindler, K.; Busetto, L.; Micic, A.; Toplak, H.; Obesity Management Task Force of the European Association for the Study of Obesity. European Guidelines for Obesity Management in Adults. Obes. Facts 2015, 8, 402–424. [Google Scholar] [CrossRef] [PubMed]
- Fitch, A.; Fox, C.; Bauerly, K.; Gross, A.; Heim, C.; Judge-Dietz, J.; Kaufman, T.; Krych, E.; Kumar, S.; Landin, D.; et al. Prevention and Management of Obesity for Children and Adolescents. Institute for Clinical Systems Improvement. Available online: https://www.healthpartners.com/ucm/groups/public/@hp/@public/documents/documents/cntrb_037112.pdf (accessed on 11 November 2019).
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M. American Col-lege of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, J.E.; Blair, S.N.; Jakicic, J.M.; Manore, M.M.; Rankin, J.W.; Smith, B.K. Appropriate Physical Activity Intervention Strategies for Weight Loss and Prevention of Weight Regain for Adults. Med. Sci. Sports Exerc. 2009, 41, 459–471. [Google Scholar] [CrossRef]
- Grondhuis, S.N.; Aman, M.G. Overweight and obesity in youth with developmental disabilities: A call to action. J. Intellect. Disabil. Res. 2013, 58, 787–799. [Google Scholar] [CrossRef]
- Argimon, J.M.; Jimenéz, J. Métodos de Investigación Clínica y Epidemiológica, 4th ed.; Elsevier: Barcelona, Spain, 2013. [Google Scholar]
- Pitchford, E.A.; Adkins, C.; Hasson, R.E.; Hornyak, J.E.; Ulrich, D. Association between Physical Activity and Adiposity in Adolescents with Down Syndrome. Med. Sci. Sports Exerc. 2018, 50, 667–674. [Google Scholar] [CrossRef]
- Loyen, A.; Clarke-Cornwell, A.; Anderssen, S.A.; Hagströmer, M.; Sardinha, L.B.; Sundquist, K.; Ekelund, U.; Steene-Johannessen, J.; Baptista, F.; Hansen, B.H.; et al. Sedentary Time and Physical Activity Surveillance Through Accelerometer Pooling in Four European Countries. Sports Med. 2016, 47, 1421–1435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pastore, E.; Marino, B.; Calzolari, A.; Digilio, M.C.; Giannotti, A.; Turchetta, A. Clinical and cardiorespiratory assessment in children with Down syndrome without congenital heart disease. Arch. Pediatr. Adolesc. Med. 2000, 154, 408–410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carvalho, T.; Massetti, T.; Da Silva, T.D.; Crocetta, T.B.; Guarnieri, R.; De Abreu, L.C.; Monteiro, C.B.D.M.; Garner, D.M.; Ferreira, C. Heart rate variability in individuals with Down syndrome—A systematic review and meta-analysis. Auton. Neurosci. 2018, 213, 23–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oppewal, A.; Hilgenkamp, T.I.M.; Van Wijck, R.; Evenhuis, H.M. Cardiorespiratory fitness in individuals with intellectual disabilities—A review. Res. Dev. Disabil. 2013, 34, 3301–3316. [Google Scholar] [CrossRef] [PubMed]
- Nixon, D. Down Syndrome, Obesity, Alzheimer’s Disease, and Cancer: A Brief Review and Hypothesis. Brain Sci. 2018, 8, 53. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| PubMed Identified/Included | Scopus Identified/Included | Web of Science Identified/Included | Summation Identified/Included | |
|---|---|---|---|---|
| “Down’s syndrome” OR “Down syndrome” OR “cognitive disability” AND overweight OR obesity AND weight OR fat AND “physical activity” OR exercise OR weightlifting | 21/4 | 47/7 | 85/6 | 153/17 |
| “Down’s syndrome” OR “Down syndrome” OR “cognitive disability” AND overweight OR obesity AND weight OR fat AND feeding OR nutrition OR “nutritional counselling” or diet OR “dietary treatment” | 25/2 | 64/4 | 44/3 | 133/9 |
| “intellectual disability” or “Trisomy 21” AND overweight OR obesity AND weight OR fat AND “physical activity” OR exercise OR weightlifting | 45/4 | 94/8 | 72/7 | 211/19 |
| “intellectual disability” or “Trisomy 21” AND overweight OR obesity AND weight OR fat AND feeding OR nutrition OR “nutritional counselling” or diet OR “dietary treatment” | 33/2 | 86/4 | 56/6 | 175/12 |
| Summation Identified/Included | 124/12 | 291/23 | 257/22 | 615/57 |
| Reference [25,26,27] | Location | Study Design | Sample/Groups/Characteristics Studied | Intervention Method Characteristics Studied/Comparative Statistical Analysis of BC | Anthropometric Parameters (Statistical Results) | Variation in Body Composition Mean | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| BW (kg/%) | BF (kg/%) | FFM (kg/%) | BMI (kg/m2/%) | WC (cm/%) | ||||||
| [25] | South America (The Federative Republic of Brazil) | Clinical trial | YES (kg) | YES (%) | NO | YES (kg/m2) | YES (cm) | BW: | ||
| IG1: −0.7 kg | ||||||||||
| n = 41 (61% male) | IG2: −0.1 kg | |||||||||
| Comparative analysis: | CG: + 0.5 kg | |||||||||
| IG1, n = 16 | ||||||||||
| IG2, n = 15 | Within groups: | BF: | ||||||||
| CG, n = 10 | IG1 (group aerobic training) | NS | NS | p < 0.05 | p < 0.05 | IG1: −0.2% | ||||
| IG2 (training group resistance) | NS | NS | NS | NS | IG2: −0.5% | |||||
| Age: | CG (control group) | NS | p < 0.05 | NS | NS | CG: 2.7% | ||||
| IG1: 15.7 ± 2.7 years | ||||||||||
| IG2: 16 ± 2.8 years | Between groups | BMI: | ||||||||
| CG: 14.4 ± 2.5 years | IG1 vs. CG | NS | p < 0.05 | NS | NS | IG1: −0.5 kg/m2 | ||||
| IG2 vs. CG | NS | p < 0.05 | p < 0.05 | NS | IG2: −0.2 kg/m2 | |||||
| Duration: 3 months | IG1 vs. IG2 | NS | NS | p < 0.05 | NS | CG: 0 kg/m2 | ||||
| WC: | ||||||||||
| IG1: −1.1 cm | ||||||||||
| IG2: −0.1 cm | ||||||||||
| CG: 0.5 cm | ||||||||||
| [26] | South America (Chile) | Clinical trial | n = 18 (55.5% male) | Comparative analysis: | NO | YES (%) | NO | YES (kg/m2) | YES (cm) | BF: +0.18% |
| Age: 5–9 years | BMI: −0.16 kg/m2 | |||||||||
| NS | NS | p < 0.01 | ||||||||
| Duration: 3 months | WC: −3.07 cm | |||||||||
| [27] | Europe (Spain) | Clinical trial | YES (kg) | YES (kg/%) | YES (kg/%) | NO | NO | BW: −3.6 kg | ||
| n = 22 (100% male) | ||||||||||
| Comparative analysis: | p < 0.05 | p < 0.05 | NS | BF: −5.5 kg/−5.8% | ||||||
| Age: 16.2 ± 1.0 years | ||||||||||
| FFM: +1.8 kg/+5.8% | ||||||||||
| Duration: 3 months | ||||||||||
| Reference [28,29,30] | Location | Study Design | Sample/Groups/Characteristics Studied | Intervention Method Characteristics Studied/Comparative Statistical Analysis of BC | Anthropometric Parameters (Statistical Results) | Variation in Body Composition Mean | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| BW (kg/%) | BF (kg/%) | FFM (kg/%) | BMI (kg/m2/%) | WC (cm/%) | ||||||
| [28] | Africa (Republic of South Africa) | RCT | YES (kg) | YES (kg/%) | NO | YES (kg/m2) | YES (cm) | BW: | ||
| IG1: −2.3 kg | ||||||||||
| IG2: −1 kg | ||||||||||
| CG: +0.1 kg | ||||||||||
| Comparative analysis: | ||||||||||
| n = 42 (71.4% female) | BF: | |||||||||
| Within groups: | IG1: −1.4 kg/−1.3% | |||||||||
| IG1: 13 | IG1 (IT) | IG2: −1.2 kg/−0.8% | ||||||||
| IG2: 13 | IG2 (CAT) | NE | NE | NE | NE | CG: +2.3 kg/−0.7% | ||||
| CG: 16 | CG | NE | NE | NE | NE | |||||
| NE | NE | NE | NE | BMI: | ||||||
| Age: 33.8 ± 8.6 years | Between groups | IG1: −0.8 kg/m2 | ||||||||
| IG1 vs. CG | IG2: −0.4 kg/m2 | |||||||||
| Duration: 3 months | IG2 vs. CG | p < 0.05 | NS | p < 0.05 | NS | CG: −0.3 kg/m2 | ||||
| IG1 vs. IG2 | p < 0.05 | NS | NS | NS | ||||||
| p < 0.05 | NS | p < 0.05 | NS | WC: | ||||||
| IG1: −0.4 cm | ||||||||||
| IG2: −1.3 cm | ||||||||||
| CG: −1.4 cm | ||||||||||
| [29] | Europe (Spain) | RCT | NO | YES (%) | NO | YES (kg/m2) | YES (cm) | BF: −3.9% | ||
| n = 20 (100% female) | ||||||||||
| Comparative statistical: | BMI: −3.4 kg/m2 | |||||||||
| IG: 11 | ||||||||||
| CG: 9 | Within groups: | WC: −3.2 cm | ||||||||
| IG | p < 0.05 | p < 0.05 | p < 0.05 | |||||||
| Age: 18–30 years | CG | NS | NS | NS | ||||||
| BMI: >30 kg/m2 | Between groups | p < 0.05 | p < 0.05 | p < 0.05 | ||||||
| Duration: 2.5 months | ||||||||||
| [30] | Europe (Spain) | RCT | NO | YES (%) | NO | NO | YES (cm) | BF: | ||
| n = 20 (100% female) | IG: −3.9% | |||||||||
| Comparative analysis: | CG: NE | |||||||||
| IG: 11 | ||||||||||
| CG: 9 | Within groups: | |||||||||
| IG | p < 0.05 | p < 0.05 | WC: | |||||||
| Age: 18–30 years | CG | NS | NS | IG: −3.2 cm | ||||||
| BMI: >30 kg/m2 | Between groups | p < 0.05 | p < 0.05 | CG: NE | ||||||
| Duration: 2.5 months | ||||||||||
| Autor | BW | Height (BMI) | BF&FFM | WC | Individual Assessment (Mean) | General Evaluation (Mean) |
|---|---|---|---|---|---|---|
| Children and adolescents | ||||||
| [25] | Moderate | Moderate | High | Moderate | Moderate (2.3) | |
| [26] | Moderate | Moderate | Moderate | High | Moderate (2.3) | Moderate (2.4) |
| [27] | Moderate | High | High | APNM | Moderate–High (2.7) | |
| Adults | ||||||
| [28] | High | Moderate | High | High | Moderate–High (2.8) | |
| [29] | Moderate | Low | Moderate | Moderate | Low–Moderate (1.8) | Moderate (2.2) |
| [30] | APNM | Low | Moderate | High | Moderate (2) | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Espinosa, R.M.; Molina Vila, M.D.; Reig García-Galbis, M. Evidences from Clinical Trials in Down Syndrome: Diet, Exercise and Body Composition. Int. J. Environ. Res. Public Health 2020, 17, 4294. https://doi.org/10.3390/ijerph17124294
Martínez-Espinosa RM, Molina Vila MD, Reig García-Galbis M. Evidences from Clinical Trials in Down Syndrome: Diet, Exercise and Body Composition. International Journal of Environmental Research and Public Health. 2020; 17(12):4294. https://doi.org/10.3390/ijerph17124294
Chicago/Turabian StyleMartínez-Espinosa, Rosa María, Mariola D Molina Vila, and Manuel Reig García-Galbis. 2020. "Evidences from Clinical Trials in Down Syndrome: Diet, Exercise and Body Composition" International Journal of Environmental Research and Public Health 17, no. 12: 4294. https://doi.org/10.3390/ijerph17124294