Quality of Life in Cohabitants of Patients with Hidradenitis Suppurativa: A Cross-sectional Study



Abstract
:1. Introduction
2. Materials and Methods
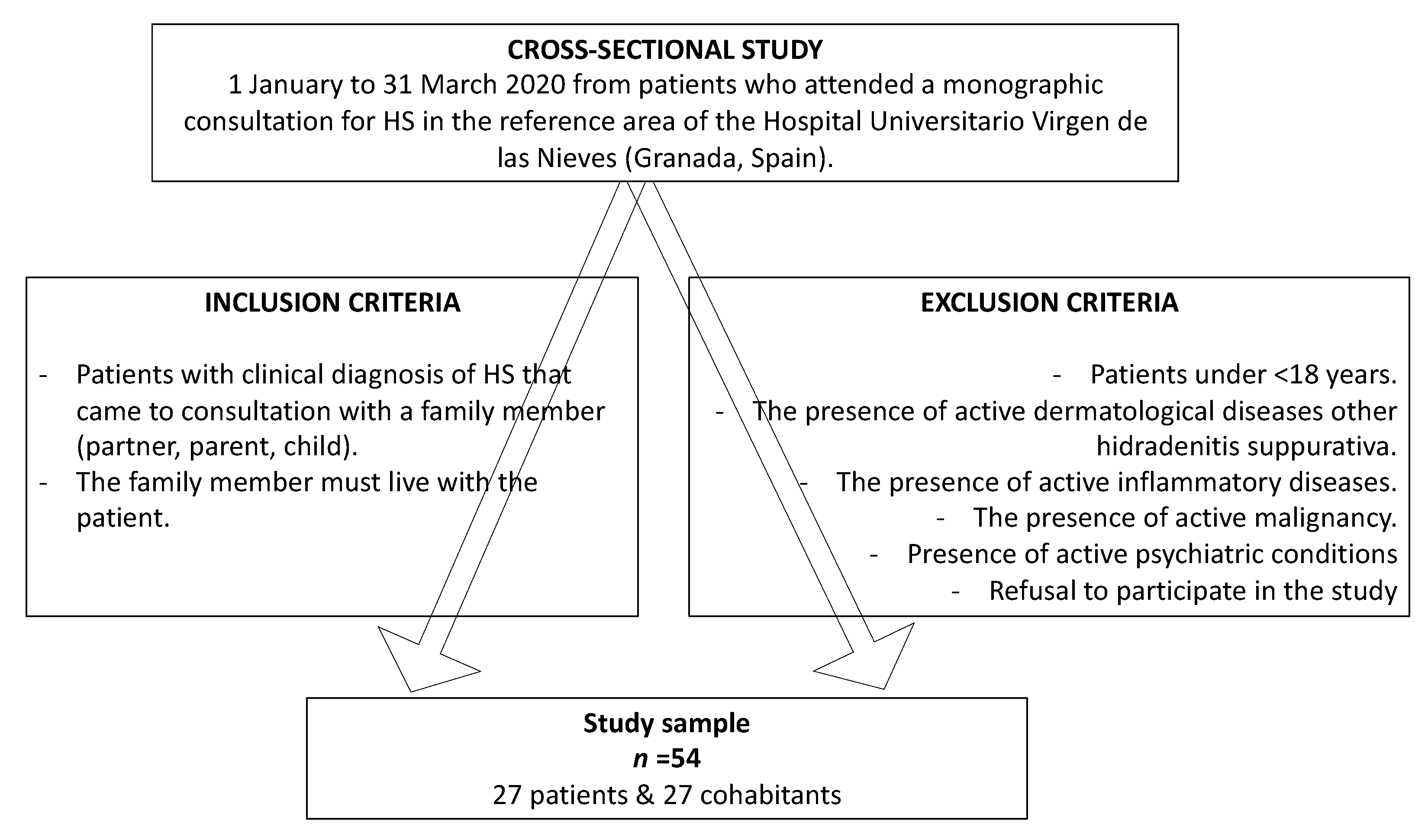
2.1. Design and Study Population
2.2. Study Variables
2.3. Data Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Duchatelet, S.; Miskinyte, S.; Delage, M.; Ungeheuer, M.N.; Lam, T.; Benhadou, F.; Vossen, A.R.; Prens, E.; Cogrel, O.; Beylot-Barry, M.; et al. Low Prevalence of GSC Gene Mutations in a Large Cohort of Predominantly Caucasian Patients with Hidradenitis suppurativa. J. Investig. Dermatol. 2020, S0022-202X, 30224-4. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.V.; Damiani, G.; Orenstein, L.A.V.; Hamzavi, I.; Jemec, G.B. Hidradenitis suppurativa: An update on epidemiology, phenotypes, diagnosis, pathogenesis, comorbidities and quality of life. J. Eur. Acad. Dermatol. Venereol. 2020. [Google Scholar] [CrossRef]
- Tzellos, T.; Zouboulis, C.C. Review of comorbidities of Hidradenitis Suppurativa: Implications for Daily Clinical Practice. Dermatol. Ther. 2020, 10, 63–71. [Google Scholar] [CrossRef] [Green Version]
- Matusiak, Ł. Profound consequences of Hidradenitis suppurativa: A review. Br. J. Dermatol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Marzano, A.V.; Damiani, G.; Ceccherini, I.; Berti, E.; Gattorno, M.; Cugno, M. Autoinflammation in Pyoderma gangrenosum and its syndromic form (pyoderma gangrenosum, acne and suppurative hidradenitis). Br. J. Dermatol. 2017, 176, 1588–1598. [Google Scholar] [CrossRef] [PubMed]
- Damiani, G.; Della Valle, V.; Iannone, M.; Dini, V.; Marzano, A.V. Autoinflammatory Disease Damage Index (ADDI): A possible newborn also in Hidradenitis suppurativa daily practice. Ann. Rheum. Dis. 2017, 76, e25. [Google Scholar] [CrossRef]
- Kridin, K.; Patel, P.M.; Jones, V.A.; Damiani, G.; Amber, K.T.; Cohen, A.D. Hidradenitis suppurativa is associated with acne keloidalis nuchae: A population-based study. Arch. Dermatol. Res. 2020. [Google Scholar] [CrossRef]
- Damiani, G.; Leone, S.; Fajgenbaum, K.; Bragazzi, N.L.; Pacifico, A.; Conic, R.R.; Pigatto, P.D.; Maiorana, C.; Poli, P.; Berti, E.; et al. Nonalcoholic fatty liver disease prevalence in an Italian cohort of patients with hidradenitis suppurativa: A multi-center retrospective analysis. World J. Hepatol. 2019, 11, 391–401. [Google Scholar] [CrossRef]
- Gooderham, M.; Papp, K. The psychosocial impact of hidradenitis suppurativa. J. Am. Acad. Dermatol. 2015, 73 (Suppl. 1), S19–S22. [Google Scholar] [CrossRef]
- Machado, M.O.; Stergiopoulos, V.; Maes, M.; Kurdyak, P.A.; Lin, P.Y.; Wang, L.J.; Shyu, Y.C.; Firth, J.; Koyanagi, A.; Solmi, M.; et al. Depression and anxiety in adults with hidradenitis suppurativa: A systematic review and meta-analysis. JAMA Dermatol. 2019, 155, 939–945. [Google Scholar] [CrossRef]
- Cuenca-Barrales, C.; Ruiz-Villaverde, R.; Molina-Leyva, A. Sexual distress in patients with hidradenitis suppurativa: A cross-sectional study. J. Clin. Med. 2019, 8, 532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finlay, A.Y.; Khan, G.K. Dermatology life quality index (DLQI)—A simple practical measure for routine clinical use. Clin. Exp. Dermatol. 1994, 19, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Basra, M.K.; Fenech, R.; Gatt, R.M.; Salek, M.S.; Finlay, A.Y. The Dermatology Life Quality Index 1994–2007: A comprehensive review of validation data and clinical results. Br. J. Dermatol. 2008, 159, 997–1035. [Google Scholar] [CrossRef] [PubMed]
- Basra, M.K.A.; Sue-Ho, R.; Finlay, A.Y. The Family Dermatology Life Quality Index: Measuring the secondary impact of skin disease. Br. J. Dermatol. 2007, 156, 528–538. [Google Scholar] [CrossRef]
- Family Dermatology Life Quality Index—School of Medicine—Cardiff University. Available online: https://www.cardiff.ac.uk/medicine/resources/quality-of-life-questionnaires/family-dermatology-life-quality-index (accessed on 12 November 2019).
- Zigmund, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatrica. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Alcaraz, S.; Hidalgo, M.D.; Godoy, C.; Fernández, E. Spanish validation of the type D personality scale (DS14). Behav. Psychol. 2018, 26, 195–209. [Google Scholar]
- Rosen, R.C.; Cappelleri, J.C.; Smith, M.D.; Lipsky, J.; Peña, B.M. Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction. Int. J. Impot. Res. 1999, 11, 319–326. [Google Scholar] [CrossRef] [Green Version]
- Isidori, A.M.; Pozza, C.; Esposito, K.; Giugliano, D.; Morano, S.; Vignozzi, L.; Corona, G.; Lenzi, A.; Jannini, E.A. Development and validation of a 6-item version of the female sexual function index (FSFI) as a diagnostic tool for female sexual dysfunction. J. Sex Med. 2010, 7, 1139–1146. [Google Scholar] [CrossRef]
- Zouboulis, C.C.; Desai, N.; Emtestam, L.; Hunger, R.E.; Ioannides, D.; Juhász, I.; Lapins, J.; Matusiak, L.; Prens, E.P.; Revuz, J.; et al. European S1 guideline for the treatment of Hidradenitis suppurativa/acne inversa. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 619–644. [Google Scholar] [CrossRef]
- Zouboulis, C.C.; Tzellos, T.; Kyrgidis, A.; Jemec, G.B.E.; Bechara, F.G.; Giamarellos-Bourboulis, E.J.; Ingram, J.R.; Kanni, T.; Karagiannidis, I.; Martorell, A.; et al. European Hidradenitis Suppurativa Foundation Investigator Group. Development and validation of the International Hidradenitis Suppurativa Severity Score System (IHS4), a novel dynamic scoring system to assess HS severity. Br. J. Dermatol. 2017, 177, 1401–1409. [Google Scholar] [CrossRef] [Green Version]
- Lindsø Andersen, P.; Nielsen, R.M.; Sigsgaard, V.; Jemec, G.B.; Riis, P.T. Body Image Quality of Life in Patients with Hidradenitis Suppurativa Compared with Other Dermatological Disorders. Acta Derm. Venereol. 2020, 100, adv00107. [Google Scholar] [CrossRef] [PubMed]
- Włodarek, K.; Głowaczewska, A.; Matusiak, Ł.; Szepietowski, J.C. Psychosocial burden of Hidradenitis Suppurativa patients’ partners. J. Eur. Acad. Dermatol. Venereol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Marasca, C.; Napolitano, M.; Monfrecola, G.; Masarà, A.; Annunziata, M.C.; Donnarumma, M.; Fabbrocini, G. Quality of life in people living with patients suffering from hidradenitis suppurativa. J. Eur. Acad. Dermatol. Venereol. 2020. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Patients (n = 27) | Cohabitants (n = 27) | p |
|---|---|---|---|
| DLQI | 13.88 (SD 9.53) | - | - |
| FDLQI | - | 10.48 (SD 7.76) | - |
| Type D Personality Negative Affectivity Score (NA) Social Inhibition Score (SI) NA + SI ≥ 10 | 15.22 (SD 6.68) 10.85 (SD 5.40) 51.85% (14/27) | 11.29 (SD 6.99) 10.11 (SD 7.21) 44.44% (12/27) | 0.03 0.67 0.58 |
| Anxiety HADS Score HADS-A ≥ 8 | 9.51 (SD 4.89) 62.96% (17/27) | 7.22 (SD 4.20) 37.03% (10/27) | 0.07 0.05 |
| Depression HADS Score HADS-D ≥ 8 | 7.70 (SD 5.11) 48.14% (13/27) | 5.14 (SD 4.52) 18.51% (5/27) | 0.05 0.02 |
| Sexual Dysfunction IIEF-5/FSFI-6 Score IIEF-5 ≤ 21/FSFI-6 ≤ 19 | 18.26 (SD 6.28) 50.00% (13/26) | 20.82 (SD 6.51) 35.29% (6/17) | 0.20 0.34 |
| Variables | DLQI | p |
|---|---|---|
| Age, Years | −0.02 (SD 0.13) | 0.85 |
| Sex Female Male | 15.40 (SD 2.46) 12.00 (SD 2.76) | 0.36 |
| Marital status Single Partner Married Divorced Widowed | 9.33 (SD 5.61) 13.00 (SD 3.43) 15.18 (SD 2.43) | 0.60 |
| Educational Level None Primary or Equivalent Secondary or Equivalent Vocational Training University or Higher | 6.00 (SD 9.34) 11.27 (SD 2.81) 13.25 (SD 4.67) 13.20 (SD 4.17) 21.00 (SD 3.81) | 0.30 |
| Occupation Employee Public Worker Freelancer Retiree Unemployed Student Other | 17.16 (SD 4.01) 8.00 (SD 4.91) 19.00 (SD 9.82) 9.25 (SD 4.91) 16.62 (SD 3.47) 19.00 (SD 9.82) 10.66 (SD 5.67) | 0.61 |
| Patients’ BMI | −0.09 (SD 0.23) | 0.67 |
| Hurley I II III | 11.50 (SD 3.31) 13.00 (SD 2.50) 20.20 (SD 4.19) | 0.25 |
| IHS4 | 0.56 (SD 0.20) | 0.01 * |
| Treatment Topical Systemic Drugs (+/- topical) Biological Drugs (+/- topical) Biological Drugs + Systemic (+/- topical) Surgery (+/- topical) Surgery + Systemic Drugs (+/- topical) | 2.00 (SD 9.63) 12.25 (SD 2.78) 17.33 (SD 5.56) 18.80 (DS 4.30) 16.00 (SD 4.81) 8.00 (SD 6.80) | 0.49 |
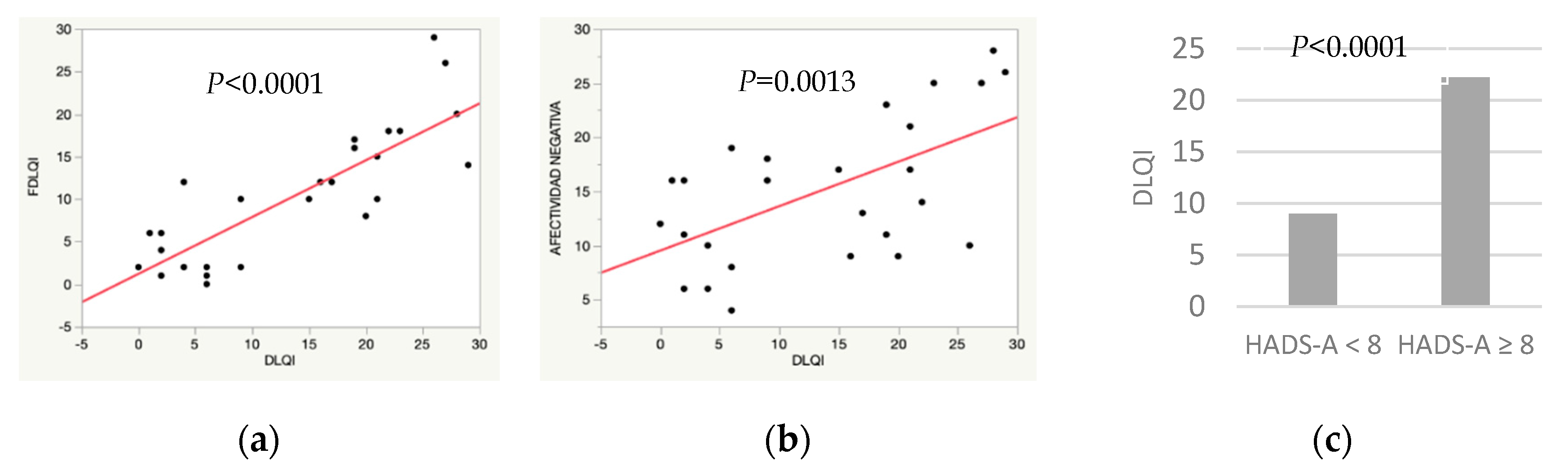
| Cohabitants’ FDLQI | 1.00 (SD 0.14) | <0.0001 |
| Negative Affectivity (NA) | 0.83 (SD 0.23) | 0.0013 |
| Social Inhibition (SI) | 0.38 (SD 0.34) | 0.27 |
| Type D personality NA + SI < 10 NA + SI ≥ 10 | 12.30 (SD 2.66) 15.35 (SD 2.56) | 0.41 |
| Cohabitants’ Negative Affectivity | 0.21 (SD 0.26) | 0.42 |
| Cohabitants’ Social Inhibition | 0.38 (SD 0.25) | 0.14 |
| Cohabitants’ Type D Personality | 3.20 (SD 3.71) | 0.39 |
| Anxiety HADS-A < 8 HADS-A ≥ 8 | 7.90 (SD 2.67) 17.41 (SD 2.05) | 0.0093 * |
| Cohabitants’ Anxiety HADS-A < 8 HADS-A ≥ 8 | 9.00 (SD 1.72) 22.20 (SD 2.25) | <0.0001 |
| Depression HADS-D < 8 HADS-D ≥ 8 | 8.78 (SD 2.14) 19.38 (SD 2.22) | 0.0021 * |
| Cohabitants’ Depression HADS-D < 8 HADS-D ≥ 8 | 12.63 (SD 1.99) 19.40 (SD 4.17) | 0.15 |
| Sexual Dysfunction IIEF-5 > 21/FSFI-6 > 19 IIEF-5 ≤ 21/FSFI-6 ≤ 19 | 12.00 (SD 2.57) 16.69 (SD 2.57) | 0.21 |
| Partners’ Sexual Dysfunction IIEF-5 > 21/FSFI-6 > 19 IIEF-5 ≤ 21/FSFI-6 ≤ 19 | 11.18 (SD 2.59) 18.33 (SD 3.51) | 0.12 |
| Relationship Patient - Cohabitant Partner Father/Mother–Son/Daughter Son/Daughter–Father/Mother | 15.30 (SD 2.64) 17.50 (SD 6.73) 9.25 (SD 4.76) | 0.48 |
| Years of Evolution | −0.13 (SD 0.29) | 0.66 |
| Variables | FDLQI | p |
|---|---|---|
| Age, Years | 0.08 (SD 0.10) | 0.44 |
| Sex Female Male | 9.29 (SD 1.87) 12.50 (SD 2.45) | 0.30 |
| Marital Status Single Partner Married Divorced Widowed | 8.00 (SD 4.57) 8.85 (SD 2.99) 10.64 (SD 2.11) 10.00 (SD 7.93) 19.00 (SD 5.60) | 0.58 |
| Educational Level None Primary or Equivalent Secondary or Equivalent Vocational Training University or Higher | 9.00 (SD 5.75) 13.00 (SD 2.87) 10.80 (DS 3.64) 7.71 (SD 3.07) 10.60 (SD 3.64) | 0.79 |
| Occupation Employee Public Worker Freelancer Retiree Unemployed Student Other | 18.25 (SD 3.51) 6.00 (SD 3.14) 15.00 (SD 4.97) 13.16 (SD 2.87) 7.16 (SD 2.87) 10.00 (SD 4.97) 4.00 (SD 4.97) | 0.12 |
| Patients’ BMI | −0.45 (SD 0.23) | 0.06 * |
| Hurley I II III | 8.87 (SD 2.65) 9.28 (SD 2.00) 16.40 (SD 3.35) | 0.16 |
| IHS4 | 0.34 (SD 0.18) | 0.06 * |
| Treatment Topical Systemic Drugs (+/− topical) Biological Drugs (+/− topical) biological Drugs + Systemic (+/− topical) Surgery (+/− topical) Surgery + Systemic Drugs (+/- topical) | 4.00 (SD 8.30) 10.91 (SD 2.39) 11.66 (SD 4.79) 13.00 (SD 3.71) 8.00 (SD 4.15) 8.00 (SD 5.87) | 0.88 |
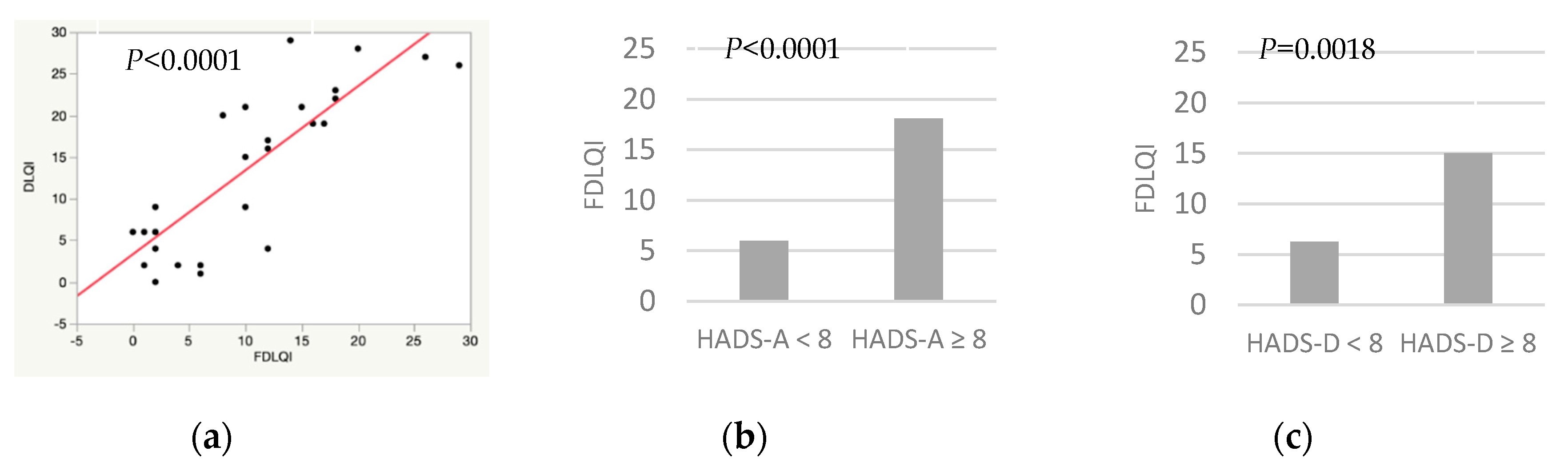
| Patients’ DLQI | 0.66 (SD 0.09) | <0.0001 |
| Negative Affectivity (NA) | 0.05 (SD 0.22) | 0.80 |
| Social Inhibition (SI) | 0.17 (SD 0.21) | 0.42 |
| Type D Personality NA + SI < 10 NA + SI ≥ 10 | 9.26 (SD 2.01) 12.00 (SD 2.24) | 0.37 |
| Patients’ Negative Affectivity | 0.50 (SD 0.21) | 0.02 * |
| Patients’ Social Inhibition | 0.18 (SD 0.28) | 0.53 |
| Patients’ Type D Personality | 0.78 (SD 3.04) | 0.79 |
| Anxiety HADS-A < 8 HADS-A ≥ 8 | 6.00 (SD 1.23) 18.10 (SD 1.60) | <0.0001 |
| Patients’ Anxiety HADS-A < 8 HADS-A ≥ 8 | 7.00 (SD 2.34) 12.52 (SD 1.79) | 0.07 * |
| Depression HADS-D < 8 HADS-D ≥ 8 | 9.72 (SD 1.65) 13.80 (SD 3.46) | 0.29 |
| Patients’ Depression HADS-D < 8 HADS-D ≥ 8 | 6.28 (SD 1.73) 15.00 (SD 1.80) | 0.0018 |
| Sexual Dysfunction IIEF-5 > 21/FSFI-6 > 19 IIEF-5 ≤ 21/FSFI-6 ≤ 19 | 8.81 (SD 2.26) 15.33 (SD 3.07) | 0.10 * |
| Partners’ Sexual Dysfunction IIEF-5 > 21/FSFI-6 > 19 IIEF-5 ≤ 21/FSFI-6 ≤ 19 | 8.4 (SD 2.35) 15.00 (SD 2.81) | 0.09 * |
| Relationship Patient - Cohabitant Partner Father/Mother–Son/Daughter Son/Daughter–Father/Mother | 10.55 (SD 1.88) 8.00 (SD 4.62) 11.50 (SD 3.27) | 0.82 |
| Years of Evolution | 0.05 (SD 0.08) | 0.48 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramos-Alejos-Pita, C.; Arias-Santiago, S.; Molina-Leyva, A. Quality of Life in Cohabitants of Patients with Hidradenitis Suppurativa: A Cross-sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 6000. https://doi.org/10.3390/ijerph17166000
Ramos-Alejos-Pita C, Arias-Santiago S, Molina-Leyva A. Quality of Life in Cohabitants of Patients with Hidradenitis Suppurativa: A Cross-sectional Study. International Journal of Environmental Research and Public Health. 2020; 17(16):6000. https://doi.org/10.3390/ijerph17166000
Chicago/Turabian StyleRamos-Alejos-Pita, Carmen, Salvador Arias-Santiago, and Alejandro Molina-Leyva. 2020. "Quality of Life in Cohabitants of Patients with Hidradenitis Suppurativa: A Cross-sectional Study" International Journal of Environmental Research and Public Health 17, no. 16: 6000. https://doi.org/10.3390/ijerph17166000