Impact of Alcohol Policies on Suicidal Behavior: A Systematic Literature Review

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
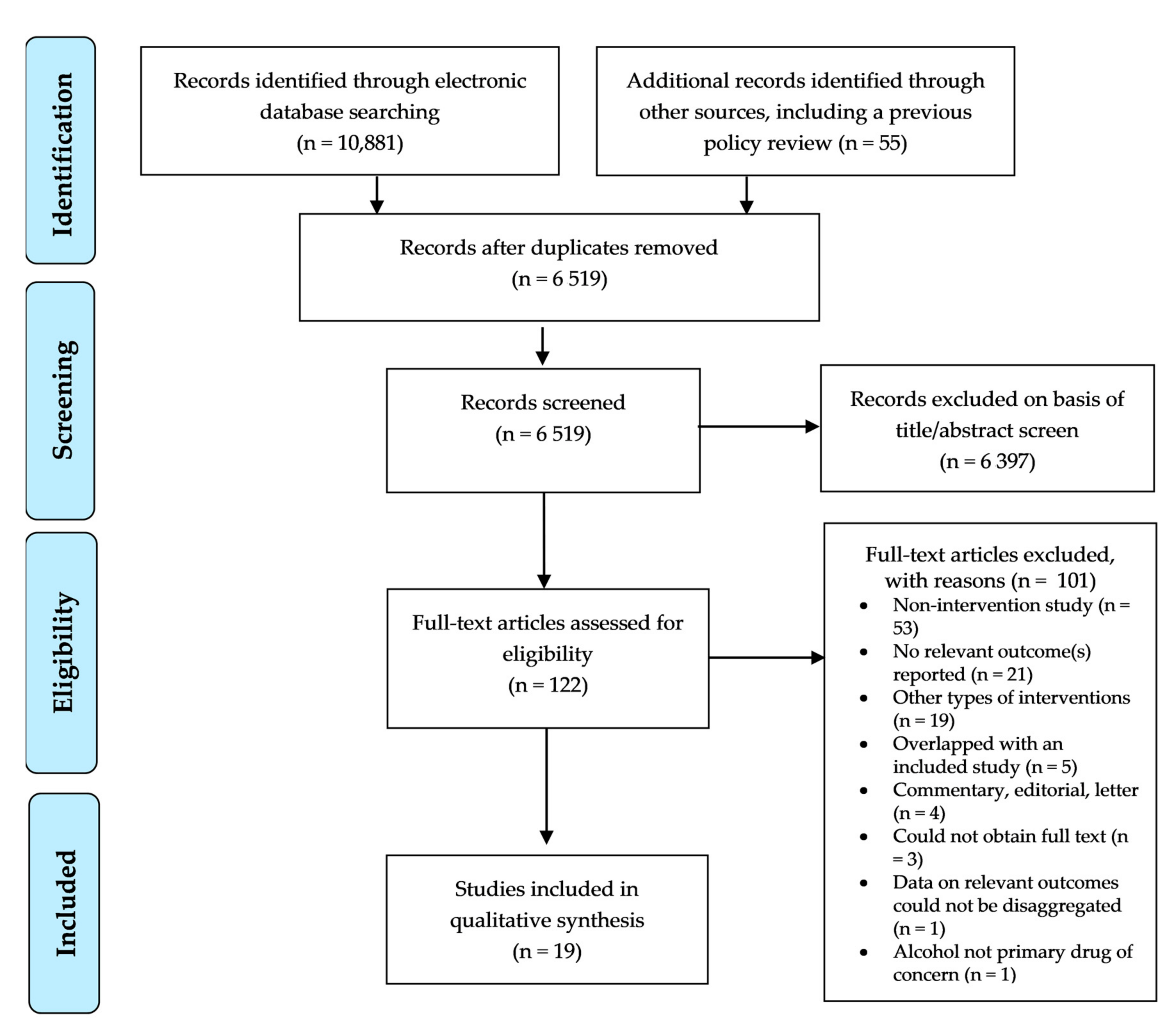
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Synthesis
2.4. Risk of Bias Assessment
3. Results
3.1. Alcohol Availability
3.2. Alcohol Pricing
3.3. Drink-Driving Countermeasures
3.4. Mixed Policies
3.5. Risk of Bias Assessment
4. Discussion
Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
| First Author | Confounding | Baseline Confounding | Selection Bias | Exposure Bias | Bias Due to Missing Data | Bias in the Measurement of Outcomes | Bias in the Selection of Reported Results | Other Bias |
|---|---|---|---|---|---|---|---|---|
| Andreasson [27] | Comment: No statistical adjustment made for any relevant confounders. High risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: Not reported; however, data ascertained from Swedish population registries. Low risk of bias. | Quote: “We use two alternative alcohol indicators: (i) alcohol sales and (ii) estimated total alcohol consumption (alcohol sales plus unregistered consumption as estimated from national surveys”. (p. 1097) Comment: Alcohol sales is from Systembolaget (a government-owned chain of liquor stores in Sweden) and unregistered consumption as estimated from national surveys (description of the methodology provided). Low risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: Outcomes ascertained from Swedish population registries. Low risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: N/A. |
| Berman [22] | Comment: No statistical adjustment made for any relevant confounders. High risk of bias. | Quote: “To analyze the potential effect of alcohol on Alaska Native injury deaths, we first divide the study population into two groups. The experimental group consists of Alaska Natives living in Alaska communities that used the state local option to restrict alcohol (went ‘dry’ of ‘damp’) at some point between 1980 and 1993. The control group consists of communities that did not exercise the local option (remained ‘wet’) throughout the period 1980-93”. (p. 313). Comment: Not reported; however, it is likely there are further differences between those communities that chose restrictive options versus those that remained ‘wet’. High risk of bias. | Quote: “To analyze the potential effect of alcohol on Alaska Native injury deaths, we first divide the study population into two groups. The experimental group consists of Alaska Natives living in Alaska communities that used the state local option to restrict alcohol (went ‘dry’ of ‘damp’) at some point between 1980 and 1993. The control group consists of communities that did not exercise the local option (remained ‘wet’) throughout the period 1980-93”. (p. 313). Comment: Not reported; however, it is likely there are further differences between those communities that chose restrictive options versus those that remained ‘wet’. High risk of bias. | Comment: Not reported. Unclear risk of bias. | Quote: “We exclude…2 of the 99 Alaska communities that passed one or more alcohol control measures because they had fewer than five Alaska Native residents in 1990”. (p. 313). Comment: Unclear risk of bias. | Comment: “The coroner’s legal determination was used to classify injury deaths as accidents, suicides, and homicides”. (p. 313). Comment: Whilst some variation in coroner’s deliberations may be expected at the individual-level, this is unlikely to have significantly biased estimates. Low risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: N/A. |
| Birckmayer [23] | Quote: “To control for factors that vary within the states across time or within years across states, we included in our model 3 independent variables what have been found to be associated with suicide: the percentage of a state population completing high school, the state divorce rate, and the state unemployment rate”. (p. 1366). Comment: In addition, border population, police per capita, beer tax and liquor law arrests were controlled for. Low risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: Not reported. Unclear risk of bias. | Quote: “We obtained state-by-state legal drinking ages by reviewing each state’s statutes for changes in the state’s MLDA”. (p. 1366). Comment: Unclear risk of bias. | Comment: Not reported. Unclear risk of bias. | Quote: “Data for the primary outcome of the study—the number of suicide victims classified by age and year…came from the Mortality Files of the National Center for Health Statistics. Although suicides are known to be under-reported in this data set [i.e., the Mortality Files of the National Center for Health Statistics], there is no reason to expect that the depress of underreporting of suicide is related to a state’s MLDA”. (p. 1366). Comment: Unclear risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: N/A. |
| Carpenter [36] | Comment: No statistical adjustment made for any relevant confounders. High risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: Not reported. Unclear risk of bias. | Quote: “The suicide data for this study come from the CDC’s National Center for Health Statistics Mortality Detail Files”. (p. 834). Comment: Low risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: N/A. |
| Joubert [24] | Comment: No statistical adjustment made for any relevant confounders. High risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: Compared ‘wet’ versus ‘dry’ counties. It is likely there are further differences between those communities that chose restrictive options versus those that remained ‘wet’. High risk of bias. | Quote: “The listings of the 67 Alabama counties that were “wet” or “dry” came from the Alabama County Data Book, 1986”. (p. 296). Comment: Unclear risk of bias. | Comment: Not reported. Unclear risk of bias. | Quote: “Alabama’s Vital Records (Alabama Department of Public Health, 1978 through 1988) served as the source of data for the annual suicide…rate”. (p. 296). Comment: Low risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: N/A. |
| Lester [31] | Comment: No statistical adjustment made for any relevant confounders. High risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: N/A. |
| Markowitz [28] | Quote: “Each model includes a number of other state-level factors which may influence the number of suicides over time. These variables include the female labor force participation rate, the unemployment rate, real income per capita, the percentage of the population living in rural areas, and the percentage of the population 25 years and older that has obtained a bachelor’s degree…All models include state and time dummies…The percentage of each state’s population identifying with certain religions…is also included” (p. 39). Comment: Low risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: Not reported. Unclear risk of bias. | Quote: “Beer taxes come from the Beer Institute’s Brewers Almanac… [for the] number of retail outlets…these data come from Jabson’s Liquor Handbook…” (p. 39). Comment: Unclear risk of bias. | Comment: Not reported. Unclear risk of bias. | Quote: “Data on completed suicides come from the National Center for Health Statistic’s Compressed Mortality File”. (p. 38). Comment: Low risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: N/A. |
| Northridge [25] | Comment: No statistical adjustment made for any relevant confounders. High risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: Not reported. Unclear risk of bias. | Quote: “All patients aged 12 and over with self poisoning are admitted to the acute medical unit”. (pp. 1466–1467). Comment: Most self-harm in the community involves self-injury, and few present to acute services following an episode. High risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: N/A. |
| Pridemore [37] | Comment: Whilst ARIMA modelling was used to adjust for time trends, no statistical adjustment made for any relevant confounders. High risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: Not reported. Unclear risk of bias. | Quote: “The dependent varies in this study were…suicide counts…cause of death is determined by the doctor who treated by decedent and is then confirmed by a coroner or pathologist. Deaths are classified according to the International Classification of Diseases, 10th Revision (ICD-10), with suicides coded as X60 to X84”. (p. 916). Comment: Whilst some variation in coroner’s deliberations may be expected at the individual-level, this is unlikely to have significantly biased estimates. Low risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: N/A. |
| Pridemore [32] | Comment: Whilst ARIMA modelling was used to adjust for time trends, and results were age and sex adjusted, no statistical adjustment made for other relevant confounders. High risk of bias. | Comment: Not reported. Unclear risk of bias | Comment: Not reported. Unclear risk of bias | Comment: Not reported. Unclear risk of bias | Comment: Not reported. Unclear risk of bias | Quote: “Deaths are classified according to the International Classification of Diseases, 10thRevision,22 with suicides coded X60-X84. Data for this study were obtained via a specialtabulation of anonymous death records collected by the Russian Federal State Statistics Service”. (p. 2022). Comment: Low risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: N/A. |
| Sauliene [38] | Comment: No statistical adjustment made for any relevant confounders. High risk of bias. | Comment: Not reported. Unclear risk of bias. | Quote: “The analyses for this study were based on data for the entire country”. (p. 459). However, “[o]nly individuals aged 15–64 years were included in this study…” (p. 459). Comment: High risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: Not reported. Unclear risk of bias. | Quote: “The 2006–2009 computerized database of the Lithuanian Department of Statistics provided information on deaths were injuries are recorded as the underlying cause of death”. (p. 459). Comment: Unclear risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: N/A. |
| Skog [33] | Comment: No statistical adjustment made for any relevant confounders. High risk of bias. | Comment: Not reported. Unclear risk of bias. | Quote: “Data…in Denmark during the period 1911–1924…” (p. 1190). Comment: Low risk of bias. | Quote: “…victims drinking status (abuse or not) was collected by a public commission…The drinking status was determined on the basis of coroner’s report”. (p. 1190). Comment: Unclear risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: N/A. |
| Sloan [29] | Comment: No statistical adjustment made for any relevant confounders. High risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: Not reported. Unclear risk of bias. | Quote: “The mortality data were based on…cause of death information abstracted from all death certificates filed with vital statistics offices in each state. Cause of death was classified according to the 9th Revision of the International Classification of Diseases (ICD-9-CM)”. (p. 456). Comment: Unclear risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: N/A. |
| Son [35] | Quote: “The state dummy variables deal with time-invariant differences among the states, and year dummies deal with the effects attributable to time-series differences”. (p. 110)Comment: Models were further adjusted for real and lagged per capita income, outlet density rates, unemployment rate, college rate, black rate and male rate, justifications for all adjustments were discussed. Low risk of bias. | Comment: Not reported. Unclear risk of bias. | Quote: “This study covers all but 18 controlled states in the United States for the years 1995 through 2004 (the lagged independent variables are included in 1994) and limits its analysis to death rates of persons between the ages of 25 and 64”. (p. 104). Comment: High risk of bias. | Quote: “State excise taxes for spirits, wines, and beer were obtained from the Tax Foundation web-site (http://www.taxfoundation.org/). The tax foundation publishes state excise taxes on alcoholic beverages annually”. (p. 105) Comment: Low risk of bias. | Comment: Not reported. Unclear risk of bias. | Quote:: “The causes of injury deaths were categorized according to the categorization of International Classification of Disease, revision 9 (ICD-9) for the years 1995–1999 and revision 10 (ICD- 10) for the years 2000–2004. The multiple Cause-of-Death data is published and released by the National Center for the Health Statistics (NCHS) and the Center for Disease Control and Prevention (CDC) [5]. The National Bureau of Economic Research (NBER) provides death data to the public” (p. 105). Comment: Low risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: N/A. |
| Wasserman [38] | Comment: No statistical adjustment made for any relevant confounders. High risk of bias. | Comment: Not reported. Unclear risk of bias. | Quote: “…we chose to analyze self-destructive behavior on the part of men…” (p. 306). Comment: Includes only data for males. High risk of bias. | Comment: Not reported; however, likely that data on alcohol consumption were obtained from the same data source as in Wasserman et al. 1998. Low risk of bias. | Comment: Not reported. Unclear risk of bias. | Quote: “…statistics on violent death were based on death certificates issued by forensicdoctors. In these certificates, the cause of death was described in words, without any code being used, but the doctor was obliged to specify whether it was an accident, suicide or murder. The diagnoses on death certificates were subsequently coded by…the statistical committees of the respective republic and formed the basis for the official statistics….All data were collected by the authors from primary documents kept by the All-Union State Statistical Committee of the USSR…” (p. 307). Comment: Low risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: N/A. |
| Wasserman [40] | Comment: No statistical adjustment made for any relevant confounders. High risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: Includes only data for females. High risk of bias. | Quote: “Figures for annual consumption of pure alcohol…were taken from official sources”. (p. 27). Comment: Low risk of bias. | Comment: Not reported. Unclear risk of bias. | Quote: “Data on causes of death were taken from official sources…from unpublished documents kept by the All-Union State Statistical Committee…” (p. 27). Comment: Low risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: N/A. |
| Wood [26] | Quote: “Given that the likelihood of serious injury occurring…is largely a function of the number of residents, it was necessary to standardize each model for the population at risk”. (p. 397). Comment: Authors also presented rates adjusted by age. However, other relevant confounders were not adjusted. High risk of bias. | Comment: Not reported. Unclear risk of bias. | Quote: “…all villages in what has been defined by the sampling framework of the Alaska Behavioral Risk Factor Surveillance System as the ‘Bush’ stratum…Excluded from this analysis were five communities with populations of greater than 1000 people, 11 villages that are connected to communities and to other villages by state maintained solid roads, and another 15 villages that had five or fewer residents…” (p. 395). Comment: High risk of bias. | Quote: “The present study also used Landenet al’s (1997) definitionsof ‘dry’ villages as those that prohibited the saleand importation and/or possession of alcohol and ‘wet’ villages as those that allowed for the importation and/orsale of alcohol”. Comment: Unclear risk of bias. | Comment: Not reported. Unclear risk of bias. | Quote: “[Data were obtained] from the Alaska Trauma Registry and from the Alaska Bureau of Vital Statistics death certificate records database…” (p. 395). Comment: Low risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: N/A. |
| Yamasaki [34] | Comment: Authors presented rates adjusted by age and sex. However, other relevant confounders were not adjusted. High risk of bias. | Comment: Not reported. Unclear risk of bias. | Quote: “This study was based on…time-series data in Switzerland…” (p. 214). Comment: Low risk of bias. | Quote: “From the OECD…[t]ax on alcohol…and alcohol consumption”. (p. 214). Comment: Low risk of bias. | Comment: Not reported. Unclear risk of bias. | Quote: “From OECD Health Data…the standardized suicide rate for men and women…” (p. 214). Comment: Low risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: N/A. |
| Zalcman [30] | Quote: “In addition to controlling for confounding effects by employing a multiple interventions design, we also used Ontario as a control area. We also used per capita consumption measures, unemployment rate and rate of AA membership per 100,000 population in Alberta as control variables to help strengthen the model design”. (p. 595–596). Comment: ARIMA modelling was further used to adjust for time trends. Low risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: Includes people aged 15 years and over in Alberta and Ontario as a control region. High risk of bias. | Quote: “Alberta data on per capita total alcohol consumption were obtained from Statistics Canada, (Statistics Canada 1976–1999) and were expressed as litres of absolute alcohol for the population aged 15 years and older”. (p. 592). Comment: Low risk of bias. | Quote: “…the data points missing between existing data points … were interpolated by cubic spline functions, a nonparametric method identified by Ferreiro (1987) for dealing with a time series that has many missing values”. (p. 594). Comment: Low risk of bias. | Quote: “Age-standardized male and female suicide mortality rates…were obtained from Statistics Canada…” (p. 592). Comment: Low risk of bias. | Comment: Not reported. Unclear risk of bias. | Comment: N/A. |
References
- Norström, T.; Rossow, I. Alcohol Consumption as a Risk Factor for Suicidal Behavior: A Systematic Review of Associations at the Individual and at the Population Level. Arch. Suicide Res. 2016, 20, 489–506. [Google Scholar] [CrossRef] [Green Version]
- Borges, G.; Bagge, C.L.; Cherpitel, C.J.; Conner, K.R.; Orozco, R.; Rossow, I. A meta-analysis of acute use of alcohol and the risk of suicide attempt. Psychol. Med. 2016, 47, 949–957. [Google Scholar] [CrossRef] [Green Version]
- Cherpitel, C.; Borges, G.; Wilcox, H.C. Acute alcohol use and suicidal behavior: A review of the literature. Alcohol. Clin. Exp. Res. 2004, 28, 18S–28S. [Google Scholar] [CrossRef] [PubMed]
- Turecki, G.; Brent, D.A. Suicide and suicidal behaviour. Lancet 2016, 2016. 387, 1227–1239. [Google Scholar] [CrossRef]
- Ramstedt, M. Alcohol and suicide in 14 European countries. Addiction 2001, 96, 59–75. [Google Scholar] [CrossRef]
- Norström, T.; Ramstedt, M. Mortality and population drinking: A review of the literature. Drug Alcohol Rev. 2005, 24, 537–547. [Google Scholar] [CrossRef] [PubMed]
- Norström, T.; Stickley, A.; Shibuya, K. The importance of alcoholic beverage type for suicide in Japan: A time-series analysis, 1963–2007. Drug Alcohol Rev. 2011, 31, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Conner, K.R.; Bagge, C.L. Suicidal Behavior: Links between Alcohol Use Disorder and Acute Use of Alcohol. Alcohol Res. Curr. Rev. 2019, 40. [Google Scholar] [CrossRef]
- Lubman, D.I.; Lubman, D.I. Effective suicide prevention: Where is the discussion on alcohol? Aust. N. Z. J. Psychiatry 2018, 52, 507–508. [Google Scholar] [CrossRef]
- Xuan, Z.; Naimi, T.S.; Kaplan, M.S.; Bagge, C.L.; Few, L.R.; Maisto, S.; Saitz, R.; Freeman, R. Alcohol Policies and Suicide: A Review of the Literature. Alcohol. Clin. Exp. Res. 2016, 40, 2043–2055. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e10000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berman, M. Suicide among young Alaska Native men: Community risk factors and alcohol control. Am. J. Public Heath 2014, 104, S329–S335. [Google Scholar] [CrossRef]
- Branas, C.C.; Richmond, T.S.; Have, T.R.T.; Wiebe, U.J. Acute alcohol consumption, alcohol outlets, and gun suicide. Subst. Use Misuse 2011, 46, 1592–1603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mann, R.E.; Zalcman, R.F.; Rush, B.R.; Smart, R.G.; Rhodes, A.E. Alcohol factors in suicide mortality rates in Manitoba. Can. J. Psychiatry 2008, 53, 243–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mann, R.E.; Zalcman, R.F.; Smart, R.G.; Rush, B.R.; Suurvali, H. Alcohol Consumption, Alcoholics Anonymous Membership, and Suicide Mortality Rates, Ontario, 1968–1991. J. Stud. Alcohol 2006, 67, 445–453. [Google Scholar] [CrossRef] [PubMed]
- Landen, M.; Beller, M.; Funk, E.; Propst, M.; Middaugh, J.; Moolenaar, R.L. Alcohol-related injury death and alcohol availability in remote Alaska. JAMA 1997, 278, 1755–1758. [Google Scholar] [CrossRef]
- Zupanc, T.; Agius, M.; Paska, A.V.; Pregelj, P. Reduced Blood Alcohol Concentration in Suicide Victims in Response to a New National Alcohol Policy in Slovenia. Eur. Addict. Res. 2013, 19, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Nemtsov, A. Suicides and alcohol consumption in Russia, 1965–1999. Drug Alcohol Depend. 2003, 71, 161–168. [Google Scholar] [CrossRef]
- Värnik, A.; Kõlves, K.; Väli, M.; Tooding, L.-M.; Wasserman, D. Do alcohol restrictions reduce suicide mortality? Addiction 2007, 102, 251–256. [Google Scholar] [CrossRef]
- World Health Organization. Global Status Report on Alcohol and Health, 2018; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- University of Bristol, Centre for Research Synthesis and Decision Analysis. Analysis, The ROBINS-E Tool (Risk of Bias in Non-Randomized Studies-of Exposures). 2018. Available online: https://www.bristol.ac.uk/population-health-sciences/centres/cresyda/barr/riskofbias/robins-e/ (accessed on 25 January 2019).
- Berman, M.; Hull, T.; May, P. Alcohol control and injury death in Alaska native communities: Wet, damp and dry under Alaska’s local option law. J. Stud. Alcohol 2000, 61, 311–319. [Google Scholar] [CrossRef]
- Birckmayer, J.; Hemenway, D. Minimum-age drinking laws and youth suicide, 1970–1990. Am. J. Public Health 1999, 89, 1365–1368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joubert, C. “Wet” or “dry” contry status and its correlates with suicide, homicide, and illegitimacy. Psychol. Rep. 1994, 74, 296. [Google Scholar] [PubMed]
- Northridge, D.; McMurray, J.; Lawson, A. Association between liberalisation of Scotland’s liquor licensing laws and admissions for self poisoning in West Fife. BMJ 1986, 293, 1466–1468. [Google Scholar] [PubMed] [Green Version]
- Wood, D.S.; Gruenewald, P.J. Local alcohol prohibition, police presence and serious injury in isolated Alaska Native villages. Addiction 2006, 101, 393–403. [Google Scholar] [CrossRef] [PubMed]
- Andréasson, S.; Holder, H.D.; Norström, T.; Österberg, E.; Rossow, I. Estimates of harm associated with changes in Swedish alcohol policy: Results from past and present estimates. Addiction 2006, 101, 1096–1105. [Google Scholar] [CrossRef] [PubMed]
- Markowitz, S.; Chatterji, P.; Kaestner, R. Estimating the impact of alcohol policies on youth suicides. J. Ment. Health Policy Econ. 2003, 6, 37–46. [Google Scholar]
- Sloan, F.A.; Reilly, B.A.; Schenzler, C. Effects of prices, civil and criminal sanctions, and law enforcement on alcohol-related mortality. J. Stud. Alcohol 1994, 55, 454–465. [Google Scholar] [CrossRef]
- Zalcman, R.F.; Mann, R.E. The Effects of Privatization of Alcohol Sales in Alberta on Suicide Mortality Rates. Contemp. Drug Probl. 2007, 34, 589–609. [Google Scholar] [CrossRef]
- Lester, D. Wine consumption and suicide rates. Psychol. Rep. 1999, 84, 1054. [Google Scholar]
- Pridemore, W.A.; Chamlin, M.B.; Andreev, E. Reduction in Male Suicide Mortality Following the 2006 Russian Alcohol Policy: An Interrupted Time Series Analysis. Am. J. Public Health 2013, 103, 2021–2026. [Google Scholar] [CrossRef]
- Skog, O.-J. Alcohol and suicide in Denmark 1911-24-experiences from a ‘natural experiment’. Addiction 1993, 88, 1189–1193. [Google Scholar] [CrossRef] [PubMed]
- Yamasaki, A.; Chinami, M.; Suzuki, M.; Kaneko, Y.; Fujita, D.; Shirakawa, T. Tobacco and alcohol tax relationships with suicide in Switzerland. Psychol. Rep. 2005, 2005. 97, 213–216. [Google Scholar] [CrossRef]
- Son, C.H.; Topyan, K. The effect of alcoholic beverage excise tax on alcohol-attributable injury mortalities. Eur. J. Health Econ. 2010, 12, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, C. Heavy alcohol use and youth suicide: Evidence from tougher drunk driving laws. J. Policy Anal. Manag. 2004, 23, 831–842. [Google Scholar] [CrossRef]
- Pridemore, W.A.; Snowden, A.J. Reduction in Suicide Mortality Following a New National Alcohol Policy in Slovenia: An Interrupted Time-Series Analysis. Am. J. Public Health 2009, 99, 915–920. [Google Scholar] [CrossRef]
- Sauliune, S.; Petrauskiene, J.; Kalediene, R. Alcohol-Related Injuries and Alcohol Control Policy in Lithuania: Effect of the Year of Sobriety. Alcohol Alcohol. 2012, 47, 458–463. [Google Scholar] [CrossRef] [Green Version]
- Wasserman, D.; Värnik, A.; Eklund, G. Male suicides and alcohol consumption in the former USSR. Acta Psychiatr. Scand. 1994, 89, 306–313. [Google Scholar] [CrossRef]
- Wasserman, D.; Värnik, A.; Eklund, G. Female suicides and alcohol consumption during perestroika in the former USSR. Acta Psychiatr. Scand. 1998, 98, 26–33. [Google Scholar] [CrossRef]
- Wagenaar, A.C.; Holder, H.D. Changes in alcohol consumption resulting from the elimination of retail wine monopolies: Results from five U.S. states. J. Stud. Alcohol 1995, 56, 566–572. [Google Scholar] [CrossRef]
- Woo, J.-M.; Okusaga, O.; Postolache, T.T. Seasonality of Suicidal Behavior. Int. J. Environ. Res. Public Health 2012, 9, 531–547. [Google Scholar] [CrossRef] [Green Version]
- Bero, L.; Chartres, N.; Diong, J.; Fabbri, A.; Ghersi, D.; Lam, J.; Lau, A.; McDonald, S.; Mintzes, B.; Sutton, P.M.; et al. The risk of bias in observational studies of exposures (ROBINS-E) tool: Concerns arising from application to observational studies of exposures. Syst. Rev. 2018, 7, 242. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.-S.; Stuckler, D.; Yip, P.; Gunnell, D. Impact of 2008 global economic crisis on suicide: Time trend study in 54 countries. BMJ 2013, 347, f5239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kõlves, K.; Koo, Y.W.; De Leo, D. A drink before suicide: Analysis of the Queensland Suicide Register in Australia. Epidemiol. Psychiatr. Sci. 2020, 29, 94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Callaghan, R.C.; Sanches, M.; Gatley, J.M. Impacts of the minimum legal drinking age legislation on in-patient morbidity in Canada, 1997-2007: A regression-discontinuity approach. Addiction 2013, 108, 1590–1600. [Google Scholar] [CrossRef] [PubMed]
- Callaghan, R.C.; Sanches, M.; Gatley, J.M.; Cunningham, J.K. Effects of the Minimum Legal Drinking Age on Alcohol-Related Health Service Use in Hospital Settings in Ontario: A Regression–Discontinuity Approach. Am. J. Public Health 2013, 103, 2284–2291. [Google Scholar] [CrossRef] [PubMed]
- Pollock, N.J.; Naicker, K.; Loro, A.; Mulay, S.; Colman, I. Global incidence of suicide among Indigenous peoples: A systematic review. BMC Med. 2018, 16, 145. [Google Scholar] [CrossRef] [PubMed]
- Snijder, M.; Stapinski, L.; Lees, B.; Ward, J.; Conrod, P.; Mushquash, C.; Belone, L.; Champion, K.; Chapman, C.; Teesson, M.; et al. Preventing Substance Use Among Indigenous Adolescents in the USA, Canada, Australia and New Zealand: A Systematic Review of the Literature. Prev. Sci. 2020, 21, 65–85. [Google Scholar] [CrossRef] [Green Version]
- Clifford, A.C.; Doran, C.M.; Tsey, K. A systematic review of suicide prevention interventions targeting indigenous peoples in Australia, United States, Canada and New Zealand. BMC Public Health 2013, 13, 1–463. [Google Scholar] [CrossRef] [Green Version]
- Studdert, D.M.; Walter, S.J.; Kemp, C.; Sutherland, G. Duration of death investigations that proceed to inquest in Australia. Inj. Prev. 2016, 22, 314–320. [Google Scholar] [CrossRef] [Green Version]
- Witt, K.; Robinson, J. Sentinel Surveillance for Self-Harm. Crisis 2019, 40, 1–6. [Google Scholar] [CrossRef]
- Kõlves, K.; Draper, B.; Snowdon, J.; De Leo, D. Alcohol-use disorders and suicide: Results from a psychological autopsy study in Australia. Alcohol 2017, 64, 29–35. [Google Scholar] [CrossRef] [PubMed]

| Terms | Cochrane CENTRAL (Ovid) | Cochrane DARE (Ovid) | EMBASE (Elsevier) | Medline (Ovid) | Pro Quest | Psyc INFO | Pub Med | SCOPUS | Web of Science |
|---|---|---|---|---|---|---|---|---|---|
| ((alcohol adj3 consum *) OR (alcohol adj3 intox *) OR (alcohol adj3 polic *) OR (alcohol adj3 intervention) OR (alcohol adj3 control) OR (alcohol adj3 restrict *) OR (alcohol adj3 prevent *) OR (alcohol adj3 law) OR (alcohol adj3 legislat *) OR (alcohol adj3 pricing) OR (alcohol adj3 price) OR (alcohol adj3 tax) OR (alcohol adj3 taxation) OR (alcohol adj3 excise) OR (alcohol adj3 h) OR perestroika):ab,kw,ti | 7036 | 47 | 75,494 | 49,014 | 247,782 | 26,608 | 897,037 | 139,770 | 114,016 |
| ((self adj2 harm *) OR (self adj2 injur *) OR (self adj2 inflict *) OR (intent * adj2 injur *) OR suicide *): ab,kw,ti | 3935 | 57 | 102,019 | 69,718 | 1,273,227 | 66,145 | 190,687 | 148,277 | 152,837 |
| 1 AND 2 | 99 | 1 | 1365 | 874 | 2626 | 749 | 2589 | 3668 | 2401 |
| Limit to humans | 91 | 1 | 1249 | 872 | 104 | 748 | 2587 | 3319 | 1910 |
| TOTAL | 10,881 |
| First Author | Country | Methods | Population | Intervention | Date of Implementation | Component(s) of Standard Alcohol Policy Targeted | Follow-up | Outcomes | Main Findings |
|---|---|---|---|---|---|---|---|---|---|
| Andreasson [27] | Sweden | Interrupted time series analysis (implementing auto regressive integrated moving average [ARIMA] modelling) of mortality data. | Swedish resident population, 1994 to 2002. | Abolition of monopolies on the wholesale, import, and export of alcohol, as well as lifting of limits on the private import of alcohol associated with Sweden’s entry into the European Union. | 1 January 1995 | Alcohol availability | 8 years | Suicide mortality: national mortality registers. | An increase in alcohol consumption was estimated. Predicted alcohol-related harm was compared with real alcohol-related harm. Suicides showed a decreasing trend. Males: 22.5 per 100,000 in 1995 to 19.8 per 100,000 in 2002; Females: 9.2 per 100,000 in 1995 to 6.7 per 100,000 in 2002; data estimated from graphics presented in Figures 6 and 7. |
| Berman [22] | US (Alaska) | Study comparing an intervention community with a control community. | Residents of Alaska Native descent in either the intervention or control communities, 1980 to 1993. | State law (Alaska local option law) which enabled communities to choose between three alcohol availability policies: (1) ‘dry law’: sale and import of alcohol prohibited within the community; (2) ‘damp law’: sale of alcohol prohibited but import for personal use permitted, or sale permitted only at one specific store; (3) ‘wet law’: no prohibition on the sale or import of alcohol within the community. | 1981 | Alcohol availability | 12 years | Suicide mortality: the Alaska Bureau of Vital Statistics. | The suicide decreased from 120.3 per 100,000 to 64.8 per 100,000 (−55.5) in communities selecting less restrictive measures—‘damp law’. There were no reductions in suicide rates in communities selecting more restrictive measures—‘dry law’. |
| Birckmayer [23] | US (48 states) | Time series analysis implementing Poisson maximum likelihood regression. | Resident population between 15 and 23 years of age in any one of 48 contiguous states, 1970 to 1990. | State laws raising the minimum legal drinking age (MLDA) following implementation of the 1986 National Highway Safety Act. | 1986 | Alcohol availability | Between 2 and 13 years | Suicide mortality: the mortality files of the National Centre for Health Statistics. | States with younger MLDAs had 8% higher suicide rates amongst 18–20 year old’s and 6% higher rates in 21–23 year olds, even following adjustment for a number of indicators of socioeconomic disparity. No significant effects were found for adolescents below the MLDA. |
| Carpenter [36] | US | Negative binomial regression, weighted by estimated resident population for each state. | Resident population between 15 and 29 years of age, 1981 to 1998. | State zero blood alcohol level (so-called ‘zero tolerance’ [ZT]) laws for drivers under the age of 21 years following implementation of the 1995 National Highway Systems Designation Act. | 1995 | Drink driving countermeasures | Up to 17 years | Suicide mortality: the Center for Disease Control Nation Center for Health Statistics. | Reductions in suicide were found for 18–20 year olds (6.3%), for males between 15 and 17 (10.3%) and for males between 18–20 years (7.7%). No meaningful effects were found for females, or for older age groups. |
| Joubert [24] | US (Alabama) | Descriptive statistics | Alabama resident population, 1978 to 1988. | Legal prohibition of the sale of alcohol from 1920s, which is still followed by some ‘dry counties’, not allowing similar sales as ‘wet counties’. | 1920 | Alcohol availability | 11 years | Suicide mortality: the Alabama’s Vital Records. | Comparison between 41 ‘wet’ and 26 ‘dry’ countries showed higher mean suicide rate in ‘dry’ counties as compared to ‘wet’ counties (t65 = −2.24, p < 0.05). |
| Lester [29] | US (Idaho, Iowa, Maine, Montana, New Hampshire, and West Virginia) | No specific information provided. | Resident population of Idaho, Iowa, Maine, Montana, New Hampshire, or West Virginia. | Removal of state retain monopolies on wine sales. | 1971 & 1973 * | Alcohol pricing (including taxation) | 10 years | Suicide mortality: no specific information provided. | Four states experienced an increase in suicide rates following the removal of monopolies (Idaho: average increase of 1.50 per 100,000 persons per year; Iowa: average increase of 1.24; Maine: average increase of 1.06; West Virginia: average increase of 0.52). Two experienced a decrease (Montana: average decrease of 0.44 per 100,000 persons per year; New Hampshire: average decrease of 1.56) |
| Markowitz [28] | US | Negative binomial regression. | Resident population of the US between 10 to 24 years of age, 1976 to 1999. | Different state-based laws
| At various time points throughout the observation period | Different laws analyzed separately:
| 23 years | Suicide mortality: National Center for Health Statistics’ Compressed Mortality File. | Increase in the excise tax on beer was associated with the reduction of suicide numbers in young males (10% increase in beer tax reduced suicides up to 5%), but not for females. Number of alcohol outlets increases the number of male suicides. Higher proportion of dry counties is associated with the lower level of suicides in males aged 20–24. Drunk driving laws had some impact on teenage female suicides (negative association). |
| Northridge [25] | UK (Scotland) | Time series | Resident population of Scotland, aged 12+, admitted to Milesmark Hospital following an episode of self-poisoning, 1971 to 1982. | Relaxation of liquor licensing laws enabling bars to remain open for longer hours, and for pubs to remain open on Sundays. A limited number of premises were also permitted ‘all day licenses’. | 1 December 1976 | Alcohol availability | 6 years | Self-harm: admissions to a general hospital following an episode of self-poisoning. | Significant increase in hospital admissions of patients co-consuming alcohol for self-poisoning during the two years of liberalization of liquor licensing laws. |
| Pridemore [37] | Slovenia | Interrupted time series analysis (implementing auto regressive integrated moving average [ARIMA] modelling) of mortality data. | Resident population of Slovenia, 1997 to 2005. | Introduction of a law establishing a MLDA of 18 years for the purchase and consumption of alcohol, and tightening of liquor licensing laws governing what type of outlets could sell alcohol, the introduction of time limits on sales, and the prohibition of alcohol distribution from vending machines. | 2003 | Mixed
| 8 years | Suicide mortality: the Statistical Unit of the Institute of Public Health of the Republic of Slovenia. | The analyses of the effect of this new alcohol policy showed an immediate reduction in male suicide mortality in Slovenia (period of 1997–2006 was analyzed). There was a significant drop of 3.6 male suicides per month (approximately a 10% reduction). There was no effect on female suicides. |
| Pridemore [32] | Russia | Interrupted time series analysis (implementing auto regressive integrated moving average [ARIMA] modelling) of mortality data. | Resident population of Russia aged 15 years and older, 2000 to 2010. | Introduction of a law regulating the production and sale of ethyl alcohol and alcohol-containing products to control the availability of alcohol, and to require registration of alcohol production and distribution facilities. | 1 January 2006 | Alcohol pricing (including taxation) | 4 years | Suicide mortality: Russian Federal State Statistics Service. | There was a drop of 9.2% in monthly male suicide numbers after the introduction of the new policy in Russia (period of 2000–2010 was analyzed), the impact was not significant for females. |
| Sauliene [38] | Lithuania | Time series | Resident population of Lithuania, between 15 to 64 years of age, 2006 to 2009. | Introductions of regulations on alcohol advertising, including the introduction of laws against drink driving the illegal import of alcohol, as well as time limits on sales. Excise taxes were increased by 20% for spirits and 10% for beer/wine. | 1 January 2008 | Mixed
| 3 years | Suicide mortality: Lithuanian Department of Statistics. | There was an increase in suicide rates from 64.2 per 100,000 in 2006 to 73.4 in 2009 for males aged 15–64 years, there was no change for females. Similarly the years of potential life lost (YPLL) due to alcohol related suicides increased for males. |
| Skog [33] | Denmark | Time series | Resident population of Denmark, 1911 to 1924. | Introduction of taxation on alcohol due to shortages caused by the blockade of Denmark during World War I. | WW I (Not further specified) | Alcohol pricing (including taxation) | 13 years | Suicide mortality: Danish mortality register. | With reduction in alcohol consumption suicide numbers dropped by 19% in 1916–1920 compared to 1911–1915. Decrease was particularly pronounced (over 50%) in alcohol abusers (as defined by the coroner). |
| Sloan [29] | US (48 states) | Time series | Resident population of the US, aged 25 to 64 years, 1982 to 1988. | Different state-based laws
| Different between states | Different laws analyzed separately:
| 6 years | Suicide mortality: the National Center for Health Statistics. | Increase in alcohol price had a significant negative effect on suicide.Dram shop laws and mandatory jail terms for DUI did not have impact on suicide. |
| Son [35] | US | Time series - state level panel data | Resident population of the US, aged 25 to 64 years, 1995 to 2004. | Excise tax on spirits, wine, beer on state level | Different between states | Alcohol pricing (including taxation) | 9 years | Suicide mortality: the National Center for Health Statistics and the Center for Disease Control and Prevention. | There was significant negative association between wine tax and suicide rate, but no association with beer or spirits tax. |
| Wasserman [39] | States of the former Union of Soviet Socialist Republics (USSR) | Time series | Resident population of males, 1984, 1986, 1988, and 1990. | Introduction of a very restrictive alcohol policy, Perestroika, encompassing: anti-alcohol advertising, a decrease in alcohol production, a decrease in the number of retail outlets for the sale of alcohol, time limits on sales, and laws enabling persons to be arrested for public drunkenness. Taxation also increased alcohol prices by around 80% (53% per litre for vodka). Producing home-distilled alcohol was criminalized. | 1 June 1985 | Mixed
| 6 years | Suicide mortality: the All-Union State Statistical Committee of the USSR. | Aggregate level alcohol consumption was strongly correlated with a decline in male suicide rates in the former USSR from 1984 to 1990. A decline of suicide rates by 31.8% for males. The attributable fraction of alcohol for male suicides in the whole USSR was 50% of male suicides (calculated for the year prior to the campaign—1984). |
| Wasserman [40] | States of the former USSR | Time series | Resident population of females, 1984, 1986, 1988, and 1990. | Introduction of a very restrictive alcohol policy, Perestroika, encompassing: anti-alcohol advertising, a decrease in alcohol production, a decrease in the number of retail outlets for the sale of alcohol, time limits on sales, and laws enabling persons to be arrested for public drunkenness. Taxation also increased alcohol prices by around 80% (53% per litre for vodka). Producing home-distilled alcohol was criminalized. | 1 June 1985 | Mixed
| 6 years | Suicide mortality: the All-Union State Statistical Committee of the USSR. | Aggregate level alcohol consumption was strongly correlated with a decline in female suicide rates in the former USSR from 1984 to 1990. A decline of 19.3% in suicide rates of females was observed. The attributable fraction of alcohol for female suicides in the whole USSR was 27%, (calculated for the year prior to the campaign—1984). |
| Wood [26] | US (Alaska) | Negative binomial regression | Resident population of 132 predominately Alaska Native villages, 1991 to 2000. | State law which enabled communities to choose between three alcohol availability policies: (1) ‘dry law’: sale and import of alcohol prohibited within the community; (2) ‘damp law’: sale of alcohol prohibited but import for personal use permitted, or sale permitted only at one specific store; (3) ‘wet law’: no prohibition on the sale or import of alcohol within the community. | 1981 | Alcohol availability | 10 years | Suicide mortality: the Alaska Trauma Registry, supplemented by the Alaska Bureau of Vital Statistics. | Average annual age-adjusted rates per 100,000 population aged 15 and over for total self-harm injuries was 223 in ‘wet’ isolated Alaska Native villages and 245 in ‘dry’ isolated Alaska native villages (rate ratio of 0.91, 95% CI = 0.76–1.08). Self-harm fatality rates were 77 (‘wet’ isolated villages) and 76 (‘dry’ isolated villages). |
| Yamasaki [34] | Switzerland | Time series, accounting for autocorrelation using multiple regression based on an auto-regressive model. | Resident population of Switzerland, 1965 to 1994. | Changes in taxation on different alcohol products over time. | Changes in tax over time | Alcohol pricing (including taxation) | 19 years | Suicide mortality: the OECD Health Data. | Alcohol tax had a significant positive correlation to male age-standardized suicide rates (coef = 0.042, p < 0.001), but there was no association for females. |
| Zalcman [30] | Canada (Alberta) | Interrupted time series analysis (implementing auto regressive integrated moving average [ARIMA] modelling) of mortality data. | Resident population of Alberta (Canada), aged 15+, 1976 to 1999. | Three stage privatization of alcohol retail: (1) the opening of privately owned wine stores; (2) the opening of privately owned cold beer stores and sale of spirits and wine in hotels in rural areas; and (3) privatization of all liquor stores. | Stage 1: 1985, Stage 2: 1989, Stage 3: 1994 | Alcohol availability | 5–14 years | Suicide mortality: the Statistics Canada. | Stages 1 & 2 in 1985 and 1989 were both followed by a n increase in suicide rates for both males and females, the stage 3 in 1994 was followed by an increase in suicide rates for males only. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kõlves, K.; Chitty, K.M.; Wardhani, R.; Värnik, A.; de Leo, D.; Witt, K. Impact of Alcohol Policies on Suicidal Behavior: A Systematic Literature Review. Int. J. Environ. Res. Public Health 2020, 17, 7030. https://doi.org/10.3390/ijerph17197030
Kõlves K, Chitty KM, Wardhani R, Värnik A, de Leo D, Witt K. Impact of Alcohol Policies on Suicidal Behavior: A Systematic Literature Review. International Journal of Environmental Research and Public Health. 2020; 17(19):7030. https://doi.org/10.3390/ijerph17197030
Chicago/Turabian StyleKõlves, Kairi, Kate M. Chitty, Rachmania Wardhani, Airi Värnik, Diego de Leo, and Katrina Witt. 2020. "Impact of Alcohol Policies on Suicidal Behavior: A Systematic Literature Review" International Journal of Environmental Research and Public Health 17, no. 19: 7030. https://doi.org/10.3390/ijerph17197030