Changes in Physical Activity Patterns from Childhood to Adolescence: Genobox Longitudinal Study

 , , , , , , ,
, , , , , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Cross-Sectional Study Design
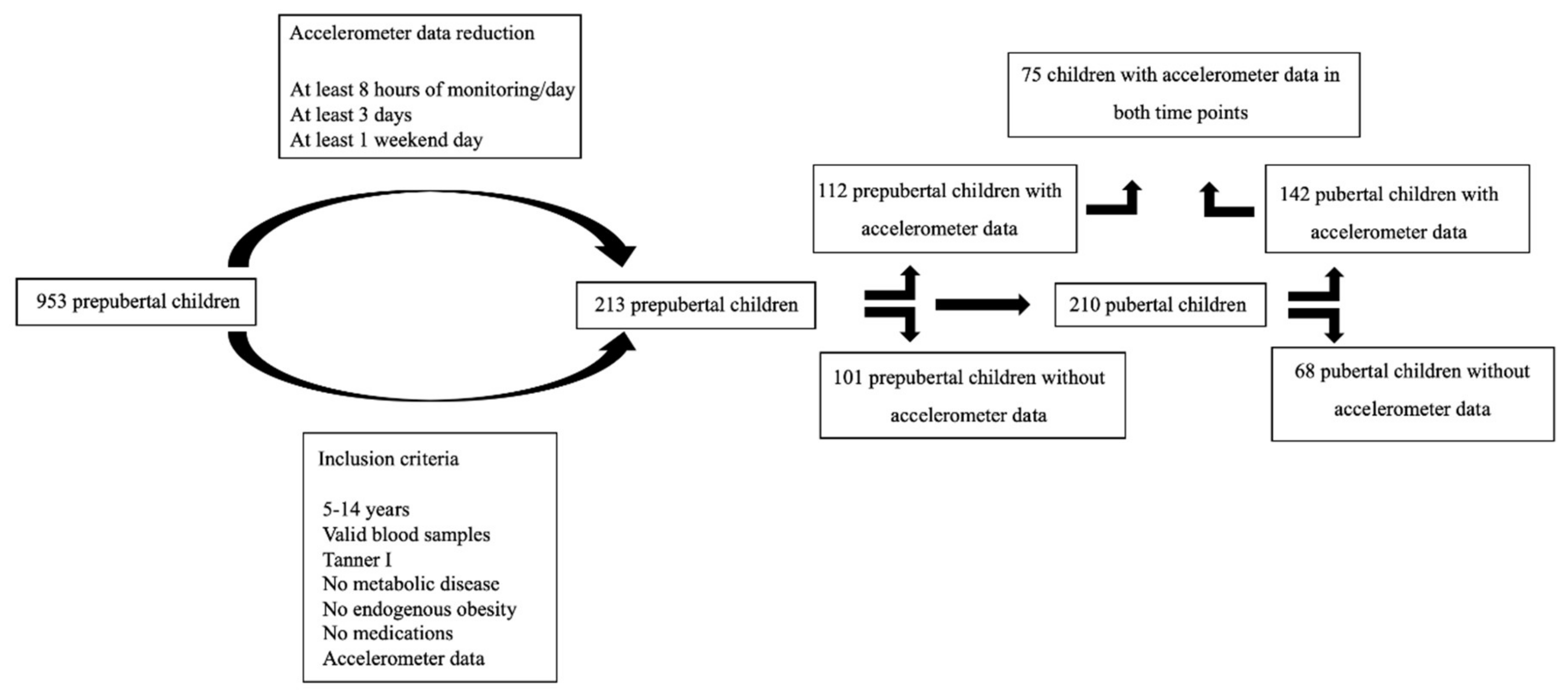
2.2. The Longitudinal Study Design
2.3. Anthropometric and Clinical Measurements
2.4. Biochemical Analysis
2.5. Accelerometry
2.6. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Janssen, I.; LeBlanc, A.G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2010, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Psaltopoulou, T.; Tzanninis, S.; Ntanasis-Stathopoulos, I.; Panotopoulos, G.; Kostopoulou, M.; Tzanninis, I.G.; Tsagianni, A.; Sergentanis, T.N. Prevention and Treatment of Childhood and Adolescent Obesity: A Systematic Review of Meta-Analyses; Springer: Singapore, 2019; Volume 15, ISBN 0123456789. [Google Scholar]
- Okely, T.D.; Salmon, J.; Vella, S.; Cliff, D.; Timperio, A.; Tremblay, M.; Trost, S.; Shilton, T.; Hinkley, T.; Ridgers, N.; et al. A Systematic Review to Update the Australian Physical Activity Guidelines for Children and Young People; Commonwealth of Australia: Canberra, Australia, 2012.
- Tremblay, M.S.; Carson, V.; Chaput, J.-P.; Connor Gorber, S.; Dinh, T.; Duggan, M.; Faulkner, G.; Gray, C.E.; Gruber, R.; Janson, K.; et al. Canadian 24-Hour Movement Guidelines for Children and Youth: An Integration of Physical Activity, Sedentary Behaviour, and Sleep. Appl. Physiol. Nutr. Metab. 2016, 41, S311–S327. [Google Scholar] [CrossRef] [PubMed]
- Weggemans, R.M.; Backx, F.J.G.; Borghouts, L.; Chinapaw, M.; Hopman, M.T.E.; Koster, A.; Kremers, S.; van Loon, L.J.C.; May, A.; Mosterd, A.; et al. The 2017 Dutch Physical Activity Guidelines. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A.; Fulton, J.E.; Galuska, D.A.; George, S.M.; Olson, R.D. The physical activity guidelines for Americans. JAMA J. Am. Med. Assoc. 2018, 320, 2020–2028. [Google Scholar] [CrossRef]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- McManus, A.M.; Mellecker, R.R. Physical activity and obese children. J. Sport Health Sci. 2012, 1, 141–148. [Google Scholar] [CrossRef] [Green Version]
- Poitras, V.J.; Gray, C.E.; Borghese, M.M.; Carson, V.; Chaput, J.P.; Janssen, I.; Katzmarzyk, P.T.; Pate, R.R.; Connor Gorber, S.; Kho, M.E.; et al. Systematic review of the relationships between objectively measured physical activity and health indicators in school-aged children and youth. Appl. Physiol. Nutr. Metab. 2016, 41, S197–S239. [Google Scholar] [CrossRef]
- Verloigne, M.; Loyen, A.; Van Hecke, L.; Lakerveld, J.; Hendriksen, I.; De Bourdheaudhuij, I.; Deforche, B.; Donnelly, A.; Ekelund, U.; Brug, J.; et al. Variation in population levels of sedentary time in European children and adolescents according to cross-European studies: A systematic literature review within DEDIPAC. Int. J. Behav. Nutr. Phys. Act. 2016, 13. [Google Scholar] [CrossRef] [Green Version]
- Biddle, S.J.H.; García Bengoechea, E.; Wiesner, G. Sedentary behaviour and adiposity in youth: A systematic review of reviews and analysis of causality. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 1–21. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M.; Aminian, S.; et al. Sedentary Behavior Research Network (SBRN)-Terminology Consensus Project process and outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Van Hecke, L.; Loyen, A.; Verloigne, M.; van der Ploeg, H.P.; Lakerveld, J.; Brug, J.; De Bourdeaudhuij, I.; Ekelund, U.; Donnelly, A.; Hendriksen, I.; et al. Variation in population levels of physical activity in European children and adolescents according to cross-European studies: A systematic literature review within DEDIPAC. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 1–22. [Google Scholar] [CrossRef] [Green Version]
- Keane, E.; Li, X.; Harrington, J.M.; Fitzgerald, A.P.; Perry, I.J.; Kearney, P.M. Physical activity, sedentary behavior and the risk of overweight and obesity in school-aged children. Pediatr. Exerc. Sci. 2017, 29, 408–418. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, J.A.; Pate, R.R.; Dowda, M.; Mattocks, C.; Riddoch, C.; Ness, A.R.; Blair, S.N. A prospective study of sedentary behavior in a large cohort of youth. Med. Sci. Sports Exerc. 2012, 44, 1081–1087. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craggs, C.; Corder, K.; Van Sluijs, E.M.F.; Griffin, S.J. Determinants of change in physical activity in children and adolescents: A systematic review. Am. J. Prev. Med. 2011, 40, 645–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dumith, S.C.; Gigante, D.P.; Domingues, M.R.; Kohl, H.W. Physical activity change during adolescence: A systematic review and a pooled analysis. Int. J. Epidemiol. 2011, 40, 685–698. [Google Scholar] [CrossRef] [Green Version]
- Gebremariam, M.K.; Bergh, I.H.; Andersen, L.F.; Ommundsen, Y.; Bjelland, M.; Lien, N. Stability and change in potential correlates of physical activity and association with pubertal status among Norwegian children in the transition between childhood and adolescence. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Lu, C.; Stolk, R.P.; Sauer, P.J.J.; Sijtsma, A.; Wiersma, R.; Huang, G.; Corpeleijn, E. Factors of physical activity among Chinese children and adolescents: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 36. [Google Scholar] [CrossRef] [Green Version]
- Nader, P.R.; Bradley, R.H.; Houts, R.M.; McRitchie, S.L.; O’Brien, M. Moderate-to-vigorous physical activity from ages 9 to 15 years. JAMA J. Am. Med. Assoc. 2008, 300, 295–305. [Google Scholar] [CrossRef]
- Sherar, L.B.; Cumming, S.P.; Eisenmann, J.C.; Baxter-Jones, A.D.G.; Malina, R.M. Adolescent biological maturity and physical activity: Biology meets behavior. Pediatr. Exerc. Sci. 2010, 22, 332–349. [Google Scholar] [CrossRef] [Green Version]
- Cumming, S.P.; Standage, M.; Gillison, F.; Malina, R.M. Sex Differences in Exercise Behavior During Adolescence: Is Biological Maturation a Confounding Factor? J. Adolesc. Health 2008, 42, 480–485. [Google Scholar] [CrossRef]
- Elmesmari, R.; Martin, A.; Reilly, J.J.; Paton, J.Y. Comparison of accelerometer measured levels of physical activity and sedentary time between obese and non-obese children and adolescents: A systematic review. BMC Pediatr. 2018, 18. [Google Scholar] [CrossRef]
- Anguita-Ruiz, A.; Mendez-Gutierrez, A.; Ruperez, A.I.; Leis, R.; Bueno, G.; Gil-Campos, M.; Tofe, I.; Gomez-Llorente, C.; Moreno, L.A.; Gil, Á. The protein S100A4 as a novel marker of insulin resistance in prepubertal and pubertal children with obesity. Metabolism 2020, 105. [Google Scholar] [CrossRef]
- Leis, R.; Jurado-Castro, J.M.; Llorente-Cantarero, F.J.; Anguita-Ruiz, A.; Iris-Rupérez, A.; Bedoya-Carpente, J.J.; Vázquez-Cobela, R.; Aguilera, C.M.; Bueno, G.; Gil-Campos, M. Cluster Analysis of Physical Activity Patterns, and Relationship with Sedentary Behavior and Healthy Lifestyles in Prepubertal Children: Genobox Cohort. Nutrients 2020, 12, 1288. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA J. Am. Med. Assoc. 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bornstein, M.H. Tanner Stages. In The SAGE Encyclopedia of Lifespan Human Development; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. Br. Med. J. 2000, 320, 1240–1243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCrindle, B.W. Assessment and management of hypertension in children and adolescents. Nat. Rev. Cardiol. 2010, 7, 155–163. [Google Scholar] [CrossRef]
- Migueles, J.H.; Cadenas-Sanchez, C.; Ekelund, U.; Delisle Nyström, C.; Mora-Gonzalez, J.; Löf, M.; Labayen, I.; Ruiz, J.R.; Ortega, F.B. Accelerometer Data Collection and Processing Criteria to Assess Physical Activity and Other Outcomes: A Systematic Review and Practical Considerations. Sport. Med. 2017, 47, 1821–1845. [Google Scholar] [CrossRef]
- Treuth, M.S.; Schmitz, K.; Catellier, D.J.; McMurray, R.G.; Murray, D.M.; Almeida, M.J.; Going, S.; Norman, J.E.; Pate, R. Defining accelerometer thresholds for activity intensities in adolescent girls. Med. Sci. Sports Exerc. 2004, 36, 1259–1266. [Google Scholar] [CrossRef]
- Evenson, K.R.; Catellier, D.J.; Gill, K.; Ondrak, K.S.; McMurray, R.G. Calibration of two objective measures of physical activity for children. J. Sports Sci. 2008, 26, 1557–1565. [Google Scholar] [CrossRef]
- Corder, K.; Sharp, S.J.; Atkin, A.J.; Griffin, S.J.; Jones, A.P.; Ekelund, U.; van Sluijs, E.M.F. Change in objectively measured physical activity during the transition to adolescence. Br. J. Sports Med. 2015, 49, 730–736. [Google Scholar] [CrossRef] [Green Version]
- Harding, S.K.; Page, A.S.; Falconer, C.; Cooper, A.R. Longitudinal changes in sedentary time and physical activity during adolescence. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 44. [Google Scholar] [CrossRef] [Green Version]
- Treuth, M.S.; Baggett, C.D.; Pratt, C.A.; Going, S.B.; Elder, J.P.; Charneco, E.Y.; Webber, L.S. A longitudinal study of sedentary behavior and overweight in adolescent girls. Obesity 2009, 17, 1003–1008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kandola, A.; Lewis, G.; Osborn, D.P.J.; Stubbs, B.; Hayes, J.F. Depressive symptoms and objectively measured physical activity and sedentary behaviour throughout adolescence: A prospective cohort study. Lancet Psychiatry 2020, 7, 262–271. [Google Scholar] [CrossRef] [Green Version]
- Ekelund, U.; Luan, J.; Sherar, L.B.; Esliger, D.W.; Griew, P.; Cooper, A. Moderate to vigorous physical activity and sedentary time and cardiometabolic risk factors in children and adolescents. JAMA J. Am. Med. Assoc. 2012, 307, 704–712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, A.R.; Goodman, A.; Page, A.S.; Sherar, L.B.; Esliger, D.W.; van Sluijs, E.M.F.; Andersen, L.B.; Anderssen, S.; Cardon, G.; Davey, R.; et al. Objectively measured physical activity and sedentary time in youth: The International children’s accelerometry database (ICAD). Int. J. Behav. Nutr. Phys. Act. 2015, 12, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Kwon, S.; Janz, K.F.; Letuchy, E.M.; Burns, T.L.; Levy, S.M. Developmental trajectories of physical activity, sports, and television viewing during childhood to young adulthood: Iowa bone development study. JAMA Pediatr. 2015, 169, 666–672. [Google Scholar] [CrossRef]
- Farooq, M.A.; Parkinson, K.N.; Adamson, A.J.; Pearce, M.S.; Reilly, J.K.; Hughes, A.R.; Janssen, X.; Basterfield, L.; Reilly, J.J. Timing of the decline in physical activity in childhood and adolescence: Gateshead Millennium Cohort Study. Br. J. Sports Med. 2018, 52, 1002–1006. [Google Scholar] [CrossRef] [Green Version]
- Collings, P.J.; Wijndaele, K.; Corder, K.; Westgate, K.; Ridgway, C.L.; Sharp, S.J.; Dunn, V.; Goodyer, I.; Ekelund, U.; Brage, S. Magnitude and determinants of change in objectively-measured physical activity, sedentary time and sleep duration from ages 15 to 17.5y in UK adolescents: The ROOTS study. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 61. [Google Scholar] [CrossRef] [Green Version]
- Corder, K.; Van Sluijs, E.M.F.; Ekelund, U.; Jones, A.P.; Griffin, S.J. Changes in children’s physical activity over 12 months: Longitudinal results from the SPEEDY study. Pediatrics 2010, 126, e926–e935. [Google Scholar] [CrossRef]


{kind=link}
| Prepubertal | Pubertal | p | |
|---|---|---|---|
| Days of Physical activity | 4.65 ± 0.70 | 6.52 ± 0.86 | <000.1 |
| Age (years) | 8.46 ± 1.37 | 13.84 ± 1.88 | <000.1 |
| Females (%) | 42 (56.0) | ||
| BMI (Kg/m2) | 21.92 ± 4.86 | 25.80 ± 6.78 | 0.001 |
| BMI Z-Score | 1.79 ± 1.95 | 1.63 ± 1.89 | 0.610 |
| Cole groups (%) | |||
| Normal-weight | 23 (30.6) | 29 (38.6) | |
| Overweight | 19 (25.3) | 18 (24.0) | |
| With Obesity | 33 (44.0) | 28 (37.3) | |
| Changes in BMI | |||
| No changes (%) | 55 (73.3) | ||
| Normal-weight | 21 | ||
| Overweight | 9 | ||
| Obesity | 25 | ||
| Improvement (%) | 15 (20) | ||
| Obesity to overweight | 7 | ||
| Overweight to normal-weight | 7 | ||
| Obesity to normal-weight | 1 | ||
| Worsening (%) | 5 (6.7) | ||
| Normal-weight to overweight | 2 | ||
| Overweight to obesity | 3 | ||
| Normal-weight to obesity | 0 | ||
| Mean Values (min ± SD) | Relative Values (% ± SD) | |||||||
|---|---|---|---|---|---|---|---|---|
| Prepubertal | Pubertal | Δ (%) | p | Prepubertal | Pubertal | Δ (%) | p | |
| Sedentary | ||||||||
| All | 443.3 ± 74.1 | 636.8 ± 164.2 | +43.6 | <0.001 | 56.0 ± 6.7 | 71.1 ± 8.2 | +15.1 | <0.001 |
| Boys | 445.2 ± 78.1 | 661.9 ± 146.4 | +48.6 | <0.001 | 56.1 ± 6.3 | 71.6 ± 7.0 | +15.5 | <0.001 |
| Girls | 441.8 ± 71.6 | 617.1 ± 176.1 | +39.6 | <0.001 | 55.9 ± 7.0 | 70.7 ± 9.1 | +14.8 | <0.001 |
| Light PA | ||||||||
| All | 286.8 ± 47.8 | 200.6 ± 50.1 | −32.0 | <0.001 | 36.7 ± 5.6 | 23.4 ± 6.9 | −13.3 | <0.001 |
| Boys | 281.5 ± 43.7 | 202.7 ± 60.1 | −27.9 | <0.001 | 35.9 ± 4.8 | 22.5 ± 5.6 | −13.4 | <0.001 |
| Girls | 291.0 ± 50.8 | 199.0 ± 51.5 | −31.6 | <0.001 | 37.3 ± 6.2 | 24.1 ± 7.8 | −13.2 | <0.001 |
| Moderate PA | ||||||||
| All | 40.9 ± 13.3 | 31.1 ± 12.3 | −23.9 | <0.001 | 5.2 ± 1.6 | 3.6 ± 1.5 | −1.6 | <0.001 |
| Boys | 43.7 ± 14.8 | 31.7 ± 13.3 | −27.4 | <0.001 | 5.7 ± 1.7 | 3.6 ± 1.5 | −2.1 | <0.001 |
| Girls | 38.6 ± 11.7 | 30.6 ± 11.6 | −20.7 | 0.003 | 4.9 ± 1.3 δ | 3.6 ± 1.5 | −1.3 δ | <0.001 |
| Vigorous PA | ||||||||
| All | 15.3 ± 9.2 | 15.2 ± 11.0 | −0.6 | 0.965 | 1.9 ± 1.1 | 1.7 ± 1.2 | −0.2 | 0.255 |
| Boys | 17.4 ± 10.5 | 19.0 ± 10.2 | +9.1 | 0.379 | 2.1 ± 1.2 | 2.1 ± 1.3 | 0 | 0.809 |
| Girls | 13.6 ± 7.8 | 12.2 ± 8.9 λ | −10.2 κ | 0.296 | 1.7 ± 0.9 | 1.4 ± 1.0 δ | −0.3 | 0.139 |
| MVPA | ||||||||
| All | 56.1 ± 20.4 | 45.5 ± 18.0 | −18.8 | <0.001 | 7.1 ± 2.5 | 5.3 ± 2.3 | −1.8 | <0.001 |
| Boys | 61.4 ± 22.4 | 49.3 ± 18.9 | −19.7 | 0.024 | 7.9 ± 2.8 | 5.6 ± 2.4 | −2.3 | 0.001 |
| Girls | 52.1 ± 18.1 δ | 42.6 ± 16.9 | −18.2 | 0.008 | 6.6 ± 2.1 δ | 5.1 ± 2.2 | −1.5 δ | 0.001 |
| Boys (%) | Girls (%) | |||
|---|---|---|---|---|
| MVPA (min) | Prepubertal | Pubertal | Prepubertal | Pubertal |
| <30 | 3 (9.0) | 7 (21.2) | 4 (9.5) | 12 (28.5) |
| 30–59.9 | 10 (30.3) | 17 (51.5) | 26 (61.9) | 20 (47.6) |
| 60–89.9 | 15 (45.4) | 9 (27.2) | 11 (26.1) | 10 (23.8) |
| >90 | 5 (15.1) | 0 | 1 (2.3) | 0 |
| Total Sample (n = 75) | Mean Values | Relative Values | ||||||
|---|---|---|---|---|---|---|---|---|
| Prepubertal | Pubertal | Δ (%) | p | Prepubertal | Pubertal | Δ (%) | p | |
| Sedentary | ||||||||
| NW | 429.3 ± 63.1 | 641.3 ± 174.5 δ | +49.3 | <0.001 | 55.5 ± 7.3 | 73.2 ± 8.1 | +17.7 | <0.001 |
| OW | 428.1 ± 68.1 | 695.5 ± 120.5 λ | +62.4 | <0.001 | 56.5 ± 8.1 | 72.9 ± 5.7 | +16.4 | <0.001 |
| OB | 444.9 ± 85.0 | 624.9 ± 152.6 | +40.4 κ | <0.001 | 55.9 ± 6.4 | 71.1 ± 8.0 | +15.2 | <0.001 |
| Light PA | ||||||||
| NW | 279.5 ± 46.6 | 186.2 ± 52.5 δ | −33.3 δ | <0.001 | 36.1 ± 5.3 | 21.7 ± 6.7 | −14.4 | <0.001 |
| OW | 279.1 ± 52.9 | 208.4 ± 58.2 | −25.3 | <0.001 | 36.8 ± 6.6 | 21.9 ± 5.1 | −14.9 | <0.001 |
| OB | 290.1 ± 54.7 | 204.1 ± 56.0 δ | −29.6 | <0.001 | 37.1 ± 5.8 | 23.7 ± 6.4 | −13.4 | <0.001 |
| Moderate PA | ||||||||
| NW | 45.4 ± 13.6 κ | 27.6 ± 12 δ | −39.2 κ | <0.001 | 5.8 ± 1.6 κ | 3.2 ± 1.5 | −2.6 | <0.001 |
| OW | 36.7 ± 15.4 | 31.7 ± 12.5 | −13.6 | 0.004 | 4.8 ± 1.9 | 3.3 ± 1.2 | −1.5 | <0.001 |
| OB | 39.7 ± 12.4 λ | 30.5 ± 14.0 | −23.1 δ | <0.001 | 5.1 ± 1.4 λ | 3.5 ± 1.5 | −1.6 | <0.001 |
| Vigorous PA | ||||||||
| NW | 18.8 ± 12.2 λ | 15.1 ± 10.2 | −19.6 δ | 0.009 | 2.4 ± 1.4 κ | 1.7 ± 1.2 | −0.7 | <0.001 |
| OW | 13.1 ± 9.7 | 16.6 ± 11.9 | +26.7 δ | 0.012 | 1.7 ± 1.1 | 1.7 ± 1.1 | 0 | 1.000 |
| OB | 14.2 ± 7.5 λ | 13.2 ± 10.8 | −7.0 | 0.405 | 1.7 ± 0.9 κ | 1.5 ± 1.2 | −0.2 | 0.143 |
| MVPA | ||||||||
| NW | 61.9 ± 21.2 λ | 42.0 ± 18.8 | −32.1 δ | <0.001 | 8.2 ± 2.9 κ | 4.9 ± 2.4 | −3.3 | <0.001 |
| OW | 49.8 ± 23.6 | 47.9 ± 19.9 | −3.8 | 0.482 | 6.5 ± 2.8 | 5.0 ± 1.9 | −1.5 | <0.001 |
| OB | 54.8 ± 17.6 δ | 42.3 ± 19.7 | −22.8 | <0.001 | 6.9 ± 2.1 λ | 5.0 ± 2.4 | −1.9 | <0.001 |
| Total Sample (n = 75) | Mean Values | Relative Values | ||||||
|---|---|---|---|---|---|---|---|---|
| Prepubertal | Pubertal | Δ (%) | p | Prepubertal (%) | Pubertal (%) | Δ (%) | p | |
| Normal-Weight No Changes (n = 21) | ||||||||
| Sedentary | 423.0 ± 60.6 | 595.0 ± 183.1 | +40.6 | 0.001 | 55.2 ± 6.3 | 69.9 ± 9.3 | +14.7 β | <0.001 |
| Light | 279.7 ± 42.0 | 196.2 ± 56.2 | −29.8 β | <0.001 | 3.6 ± 4.6 | 24.1 ± 7.7 | −12.4 | <0.001 |
| Moderate | 44.8 ± 10.5 | 30.5 ± 12.4 | −31.9 | 0.001 | 5.8 ± 1.3 | 3.8 ± 1.7 | −2.0 β | 0.001 |
| Vigorous | 17.9 ± 9.7 | 16.5 ± 10.0 | −7.8 | 0.523 | 2.3 ± 1.2 | 2.0 ± 1.2 | −0.2 | 0.384 |
| MVPA | 62.7 ± 19.2 | 47.0 ± 18.9 | −25.0 | 0.007 | 8.2 ± 2.4 | 5.8 ± 2.6 | −2.3 | 0.007 |
| Overweight/With Obesity No changes (n = 34) | ||||||||
| Sedentary | 445.8 ± 79.1 | 639.1 ± 162.1 | +43.3 | <0.001 | 55.4 ± 6.3 | 70.5 ± 7.4 | +15.1 β | <0.001 |
| Light | 300.7 ± 45.7 | 210.5 ± 51.8 | −29.9 β | <0.001 | 37.6 ± 6.2 | 24.0 ± 6.5 | −13.5 β | <0.001 |
| Moderate | 40.0 ± 12.4 | 32.2 ± 12.1 | −19.5 | 0.016 | 5.0 ± 1.2 | 3.7 ± 1.3 | −1.3 | 0.001 |
| Vigorous | 15.2 ± 9.6 | 14.9 ± 11.5 | −1.9 | 0.885 | 1.8 ± 1.0 | 1.6 ± 1.1 | −0.2 | 0.294 |
| MVPA | 56.3 ± 19.6 | 47.5 ± 18.8 | −15.6 | 0.066 | 6.9 ± 2.2 | 5.3 ± 1.9 | −1.6 | 0.005 |
| Improving (n = 15) | ||||||||
| Sedentary | 465.4 ± 70.4 | 728.6 ± 119.1 | +56.5 | <0.001 | 57.6 ± 5.4 | 76.5 ± 6.7 | +18.8 β | <0.001 |
| Light | 274.9 ± 44.2 | 178.1 ± 62.6 | −35.2 β | <0.001 | 35.8 ± 4.0 | 19.2 ± 6.2 | −16.5 β | <0.001 |
| Moderate | 37.5 ± 15.9 | 26.0 ± 10.0 | −30.6 | 0.020 | 4.8 ± 2.1 | 2.6 ± 0.7 | −2.1 β | 0.003 |
| Vigorous | 13.4 ± 7.8 | 13.9 ± 9.8 | +3.7 | 0.813 | 1.6 ± 1.0 | 1.5 ± 1.1 | −0.1 | 0.626 |
| MVPA | 50.6 ± 22.9 | 39.0 ± 15.9 | −22.9 | 0.045 | 6.4 ± 3.0 | 4.1 ± 1.6 | −2.2 | 0.010 |
| Worsening (n = 5) | ||||||||
| Sedentary | 444.6 ± 100.6 | 521.3 ± 85.3 | +17.2 | 0.285 | 58.5 ± 12.8 | 64.4 ± 5.6 | +5.8 δ,λ,κ | 0.329 |
| Light | 263.1 ± 78.7 | 226.1 ± 20.7 | −14.0 δ,λ,κ | 0.354 | 34.5 ± 9.6 | 28.1 ± 2.8 | −6.3 λ,κ | 0.252 |
| Moderate | 41.8 ± 20.8 | 43.1 ± 14.4 | +3.1 | 0.834 | 5.4 ± 2.5 | 5.3 ± 1.7 | −0.1 δ,κ | 0.932 |
| Vigorous | 10.4 ± 7.2 | 16.0 ± 16.8 | +53.8 | 0.306 | 1.3 ± 0.9 | 1.9 ± 2.0 | +0.5 | 0.383 |
| MVPA | 42.3 ± 16.3 | 46.5 ± 13.0 | +9.9 | 0.630 | 6.8 ± 3.2 | 7.3 ± 3.7 | +0.5 | 0.595 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Llorente-Cantarero, F.J.; Aguilar-Gómez, F.J.; Anguita-Ruiz, A.; Rupérez, A.I.; Vázquez-Cobela, R.; Flores-Rojas, K.; Aguilera, C.M.; Gonzalez-Gil, E.M.; Gil-Campos, M.; Bueno-Lozano, G.; et al. Changes in Physical Activity Patterns from Childhood to Adolescence: Genobox Longitudinal Study. Int. J. Environ. Res. Public Health 2020, 17, 7227. https://doi.org/10.3390/ijerph17197227
Llorente-Cantarero FJ, Aguilar-Gómez FJ, Anguita-Ruiz A, Rupérez AI, Vázquez-Cobela R, Flores-Rojas K, Aguilera CM, Gonzalez-Gil EM, Gil-Campos M, Bueno-Lozano G, et al. Changes in Physical Activity Patterns from Childhood to Adolescence: Genobox Longitudinal Study. International Journal of Environmental Research and Public Health. 2020; 17(19):7227. https://doi.org/10.3390/ijerph17197227
Chicago/Turabian StyleLlorente-Cantarero, Francisco Jesús, Francisco Javier Aguilar-Gómez, Augusto Anguita-Ruiz, Azahara Iris Rupérez, Rocío Vázquez-Cobela, Katherine Flores-Rojas, Concepción M. Aguilera, Esther M. Gonzalez-Gil, Mercedes Gil-Campos, Gloria Bueno-Lozano, and et al. 2020. "Changes in Physical Activity Patterns from Childhood to Adolescence: Genobox Longitudinal Study" International Journal of Environmental Research and Public Health 17, no. 19: 7227. https://doi.org/10.3390/ijerph17197227