How Can the Lived Environment Support Healthy Ageing? A Spatial Indicators Framework for the Assessment of Age-Friendly Communities



Abstract
:1. Introduction
Age-Friendly Communities and the Lived Environment
2. Materials and Methods
| Measurable: Will variations in the indicator be observable over time due to specific actions? |
| Disaggregation possible: Can the indicator be disaggregated by gender, age group, or across neighbourhoods? There are also other strategies that could be important in the local context, including ethnicity, socioeconomic status, etc. |
| Aligns with local goals and targets: Does the indicator link to a broader local agenda? |
| Can be linked to action: Does the indicator provide an understanding of the various actions that might need to be undertaken? |
| Within local influence: Does the local government or community have the mandate or authority to act on this indicator? For example, a federal insurance scheme is mostly beyond the influence of the municipal government. |
| Easy to collect: Are the data required to produce the indicator easy to collect in a timely manner? |
| Socially acceptable: Is the collection of this information acceptable to the communities and individuals concerned? |
3. Results
Selection of Measures
4. Outdoor Spaces and Buildings
5. Transport
6. Housing
7. Social Participation
8. Respect and Social Inclusion
9. Civic Participation and Employment
10. Communications and Information
11. Community Support and Health Services
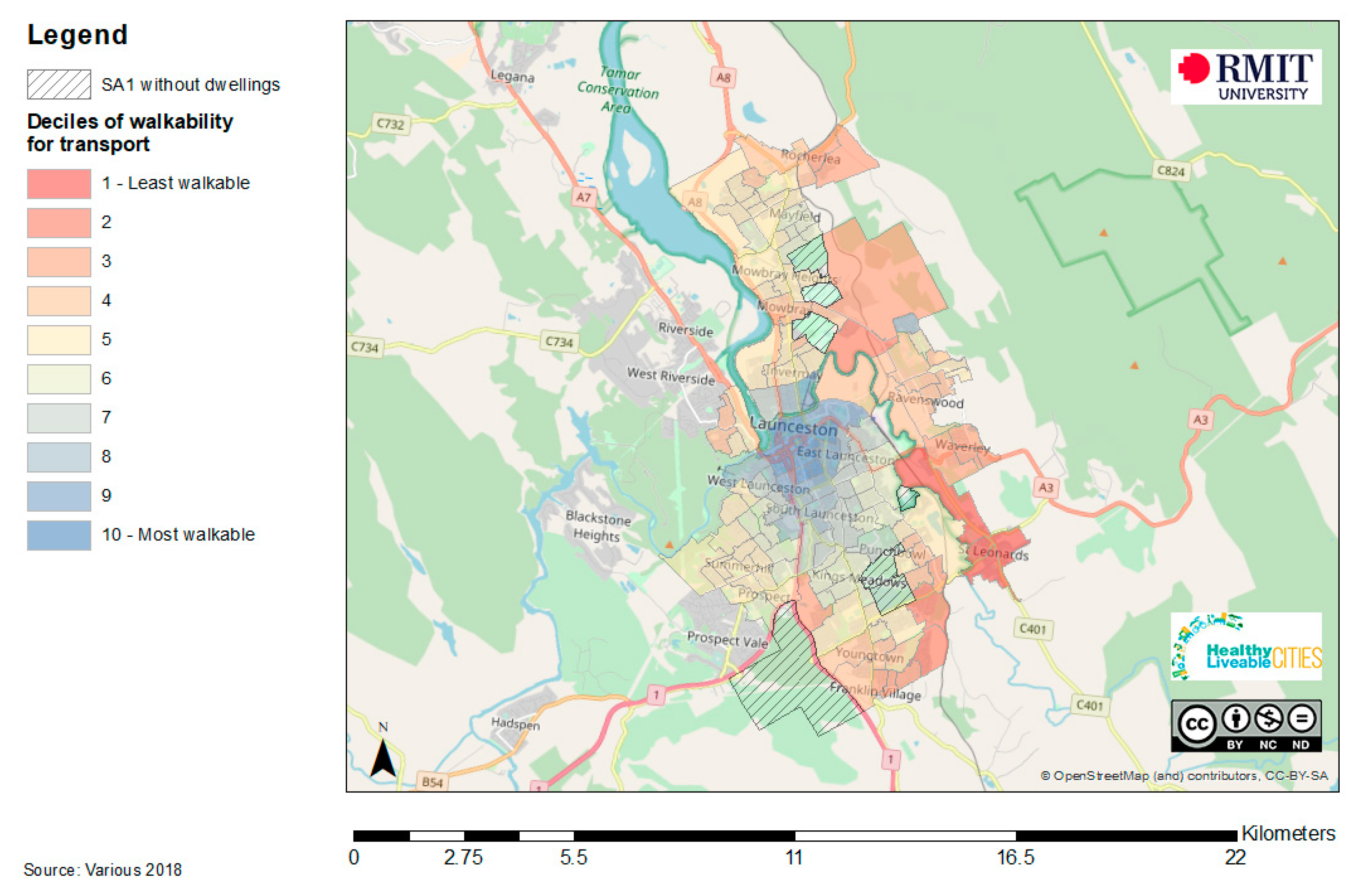
A Regional Case Study Example
12. Discussion
12.1. Linking Spatial AFC Indicators to Policy Contexts Outside of Ageing
12.2. Unique Contexts, Regional and Rural Localities
13. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Rowles, G.D.; Bernard, M.A. Environmental Gerontology: Making Meaningful Places in Old Age; Springer Publishing Company: Berlin/Heidelberg, Germany, 2013. [Google Scholar]
- Garon, S.; Paris, M. How Healthy Ageing Can Foster Age-Friendly Environment? In Prevention of Chronic Diseases and Age-Related Disability, Practical Issues in Geriatrics; Springer: Berlin/Heidelberg, Germany, 2019; pp. 161–167. [Google Scholar]
- World Health Organisation. Decade of Healthy Ageing 2020–2030; World Health Organisation: Geneva, Switzerland, 2020. [Google Scholar]
- Leeson, G.W. The growth, ageing and urbanisation of our world. J. Popul. Ageing 2018, 11, 107–115. [Google Scholar] [CrossRef] [Green Version]
- United Nations. World Population Prospects: The 2017 Revision, Key Findings and Advance Tables; United Nations, Department of Economics and Social Affairs: New York, NY, USA, 2017. [Google Scholar]
- World Health Organisation. World Report on Ageing and Health; World Health Organisation: Geneva, Switzerland, 2015. [Google Scholar]
- World Health Organisation. Global Age-Friendly Cities: A Guide; World Health Organisation: Geneva, Switzerland, 2007. [Google Scholar]
- World Health Organization. The Global Network for Age-Friendly Cities and Communities: Looking Back Over the Last Decade, Looking Forward to the Next; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Moulaert, T.; Garon, S. Age-Friendly Cities and Communities in International Comparison: Political Lessons, Scientific Avenues, and Democratic Issues; Springer: Berlin/Heidelberg, Germany, 2015. [Google Scholar]
- Lawler, K. Age-friendly communities: Go big or go home. Public Policy Aging Rep. 2015, 25, 30–33. [Google Scholar] [CrossRef]
- Park, S.; Lee, S. Age-friendly environments and life satisfaction among South Korean elders: Person-environment fit perspective. Aging Ment. Health 2017, 21, 693–702. [Google Scholar] [CrossRef]
- Dellamora, M.C.; Zecevic, A.A.; Baxter, D.; Cramp, A.; Fitzsimmons, D.; Kloseck, M. Review of assessment tools for baseline and follow-up measurement of age-friendliness. Ageing Int. 2015, 40, 149–164. [Google Scholar] [CrossRef]
- Zhang, X.; Warner, M.E.; Firestone, S. Overcoming Barriers to Livability for All Ages: Inclusivity Is the Key. Urban Plan. 2019, 4, 31–42. [Google Scholar] [CrossRef]
- Kano, M.; Rosenberg, P.E.; Dalton, S.D. A global pilot study of age-friendly city indicators. Soc. Indic. Res. 2018, 138, 1205–1227. [Google Scholar] [CrossRef] [Green Version]
- World Health Organisation. Measuring the Age-Friendliness of Cities: A Guide to Using Core Indicators; World Health Organisation: Geneva, Switzerland, 2015. [Google Scholar]
- Public Health Agency of Canada. Age-Friendly Communities Evaluation Guide: Using Indicators to Measure Progress; Public Health Agency of Canada Ottawa: Ottawa, ON, Canada, 2015.
- Orpana, H.; Chawla, M.; Gallagher, E.; Escaravage, E. Developing indicators for evaluation of age-friendly communities in Canada: Process and results. Health Promot. Chronic Dis. Prev. Can. Res. Policy Pract. 2016, 36, 214–223. [Google Scholar] [CrossRef] [Green Version]
- Scharlach, A.E. Age-Friendly Cities: For Whom? By Whom? For What Purpose? In Age-Friendly Cities and Communities in International Comparison; Moulaert, T., Garon, S., Eds.; Springer: Berlin/Heidelberg, Germany, 2016; pp. 305–329. [Google Scholar]
- Badland, H.; Whitzman, C.; Lowe, M.; Davern, M.; Aye, L.; Butterworth, I.; Hes, D.; Giles-Corti, B. Urban liveability: Emerging lessons from Australia for exploring the potential for indicators to measure the social determinants of health. Soc. Sci. Med. 2014, 111, 64–73. [Google Scholar] [CrossRef]
- Badland, H.; Mavoa, S.; Villanueva, K.; Roberts, R.; Davern, M.; Giles-Corti, B. The development of policy-relevant transport indicators to monitor health behaviours and outcomes. J. Transp. Health 2015, 2, 103–110. [Google Scholar] [CrossRef]
- Badland, H.M.; Rachele, J.N.; Roberts, R.; Giles-Corti, B. Creating and applying public transport indicators to test pathways of behaviours and health through an urban transport framework. J. Transp. Health 2017, 4, 208–215. [Google Scholar] [CrossRef]
- Villanueva, K.; Badland, H.; Hooper, P.; Koohsari, M.J.; Mavoa, S.; Davern, M.; Roberts, R.; Goldfeld, S.; Giles-Corti, B. Developing indicators of public open space to promote health and wellbeing in communities. Appl. Geogr. 2015, 57, 112–119. [Google Scholar] [CrossRef]
- Badland, H.; Foster, S.; Bentley, R.; Higgs, C.; Roberts, R.; Pettit, C.; Giles-Corti, B. Examining associations between area-level spatial measures of housing with selected health and wellbeing behaviours and outcomes in an urban context. Health Place 2017, 43, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Badland, H.; Davern, M.T.; Villanueva, K.; Mavoa, S.; Milner, A.; Roberts, R.; Giles-Corti, B. Conceptualising and measuring spatial indicators of employment through a liveability lens. Soc. Indic. Res. 2016, 127, 565–576. [Google Scholar] [CrossRef]
- Davern, M.; Gunn, L.; Whitzman, C.; Higgs, C.; Giles-Corti, B.; Simons, K.; Villanueva, K.; Mavoa, S.; Roberts, R.; Badland, H.M. Using spatial measures to test a conceptual model of social infrastructure that supports health and wellbeing. Cities Health 2017, 1, 194–209. [Google Scholar] [CrossRef] [Green Version]
- Murphy, M.; Badland, H.M.; Koohsari, M.J.; Astell-Burt, T.; Trapp, G.; Villanueva, K.; Mavoa, S.; Davern, M.T.; Giles-Corti, B. Indicators of a health-promoting local food environment: A conceptual framework to inform urban planning policy and practice. Health Promot. J. Aust. Off. J. Aust. Assoc. Health Promot. Prof. 2017, 28, 82. [Google Scholar] [CrossRef] [Green Version]
- Cunningham, G.O.; Michael, Y.L. Concepts guiding the study of the impact of the built environment on physical activity for older adults: A review of the literature. Am. J. Health Promot. 2004, 18, 435–443. [Google Scholar] [CrossRef] [PubMed]
- Frank, L.D.; Engelke, P.O. The built environment and human activity patterns: Exploring the impacts of urban form on public health. J. Plan. Lit. 2001, 16, 202–218. [Google Scholar] [CrossRef]
- Tietz, C. Is it Time to Move Beyond the Limits of ‘Built Environment’ Thinking? The Conversation. 15 October 2018. Available online: https://theconversation.com/is-it-time-to-move-beyond-the-limits-of-built-environment-thinking-102774 (accessed on 18 November 2019).
- Davern, M.; Both, A.; Higgs, C.; Gunn, L. The Average Regional City Resident Lacks Good Access to Two-Thirds of Community Services, and Liveability Suffers. The Conversation, 2020. Available online: https://theconversation.com/the-average-regional-city-resident-lacks-good-access-to-two-thirds-of-community-services-and-liveability-suffers-131910 (accessed on 18 November 2019).
- Beard, J.R.; Montawi, B. Age and the Environment: The Global Movement towards Age-Friendly Cities and Communities. J. Soc. Work Pract. 2015, 29, 5–11. [Google Scholar] [CrossRef]
- Steels, S. Key characteristics of age-friendly cities and communities: A review. Cities 2015, 47, 45–52. [Google Scholar] [CrossRef] [Green Version]
- Jackisch, J.; Zamaro, G.; Green, G.; Huber, M. Is a healthy city also an age-friendly city? Health Promot. Int. 2015, 30, 108–117. [Google Scholar] [CrossRef] [Green Version]
- United Nations. Transforming out World: The 2030 Agenda for Sustainable Development; United Nations: New York, NY, USA, 2015. [Google Scholar]
- World Health Organization. The WHO Age-Friendly Cities Framework. 2019. Available online: https://extranet.who.int/agefriendlyworld/age-friendly-cities-framework/ (accessed on 18 November 2019).
- Davern, M.T.; Gunn, L.; Giles-Corti, B.; David, S. Best practice principles for community indicator systems and a case study analysis: How community indicators Victoria is creating impact and bridging policy, practice and research. Soc. Indic. Res. 2017, 131, 567–586. [Google Scholar] [CrossRef]
- Lowen, T.; Davern, M.T.; Mavoa, S.; Brasher, K. Age-friendly cities and communities: Access to services for older people. Aust. Plan. 2015, 52, 255–265. [Google Scholar] [CrossRef]
- Giles-Corti, B.; Macaulay, G.; Middleton, N.; Boruff, B.J.; Bull, F.; Butterworth, I.; Badland, H.M.; Mavoa, S.; Roberts, R.; Christian, H. Developing a research and practice tool to measure walkability: A demonstration project. Health Promot. J. Aust. 2014, 25, 160–166. [Google Scholar] [CrossRef] [Green Version]
- Giles-Corti, B. Transport Walkability Index: Melbourne. McCaughey VicHealth Centre for Community Wellbeing; The University of Melbourne: Melbourne, Australia, 2014. [Google Scholar]
- Boulange, C.; Gunn, L.; Giles-Corti, B.; Mavoa, S.; Pettit, C.; Badland, H. Examining associations between urban design attributes and transport mode choice for walking, cycling, public transport and private motor vehicle trips. J. Transp. Health 2017, 6, 155–166. [Google Scholar] [CrossRef]
- Saelens, B.E.; Handy, S.L. Built environment correlates of walking: A review. Med. Sci. Sports Exerc. 2008, 40, S550. [Google Scholar] [CrossRef] [Green Version]
- Saelens, B.E.; Sallis, J.F.; Black, J.B.; Chen, D. Neighborhood-based differences in physical activity: An environment scale evaluation. Am. J. Public Health 2003, 93, 1552–1558. [Google Scholar] [CrossRef] [PubMed]
- Cerin, E.; Nathan, A.; van Cauwenberg, J.; Barnett, D.W.; Barnett, A.; on Behalf of the Council on Environment and Physical Activity (CEPA)—Older Adults Working Group. The neighbourhood physical environment and active travel in older adults: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 15. [Google Scholar] [CrossRef] [Green Version]
- Zapata-Diomedi, B.; Boulange, C.; Giles-Corti, B.; Phelan, K.; Washington, S.; Veerman, L.; Gunn, L. Physical activity-related health and economic benefits of building walkable neighbourhoods: A modelled comparison between brownfield and greenfield developments. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 11. [Google Scholar] [CrossRef]
- Davern, M.; Farrar, A.; Kendal, D.; Giles-Corti, B. Quality Green Space Supporting Health, Wellbeing and Biodiversity: A Literature Review; Heart Foundation of Australia: Adelaide, Australia, 2017. [Google Scholar]
- Winters, M.; Voss, C.; Ashe, M.C.; Gutteridge, K.; McKay, H.; Sims-Gould, J. Where do they go and how do they get there? Older adults’ travel behaviour in a highly walkable environment. Soc. Sci. Med. 2015, 133, 304–312. [Google Scholar] [CrossRef]
- Fielding, R.A.; Rejeski, W.J.; Blair, S.; Church, T.; Espeland, M.A.; Gill, T.M.; Guralnik, J.M.; Hsu, F.-C.; Katula, J.; King, A.C.; et al. The lifestyle interventions and independence for elders study: Design and methods. J. Gerontol. Ser. A Biomed. Sci. Med Sci. 2011, 66, 1226–1237. [Google Scholar] [CrossRef]
- Weuve, J.; Kang, J.; Malnson, J. Physical activity, including walking, and cognitive function in older women. JAMA 2004, 292, 1454–1461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aspinall, P.A.; Thompson, C.W.; Alves, S.; Sugiyama, T.; Brice, R.; Vickers, A. Preference and relative importance for environmental attributes of neighbourhood open space in older people. Environ. Plan. B Plan. Des. 2010, 37, 1022–1039. [Google Scholar] [CrossRef]
- Sugiyama, T.; Thompson, C.W.; Alves, S. Associations between neighborhood open space attributes and quality of life for older people in Britain. Environ. Behav. 2009, 41, 3–21. [Google Scholar] [CrossRef]
- Vine, D.; Buys, L.; Aird, R. Experiences of neighbourhood walkability among older Australians living in high density inner-city areas. Plan. Theory Pract. 2012, 13, 421–444. [Google Scholar] [CrossRef] [Green Version]
- Davern, M. Walkability Factsheet Summary: Assessing Walkability in Brighton, Clarence and Launceston for the Local Government Association of Tasmania; RMIT University: Melbourne, Australia, 2018. [Google Scholar]
- Grant, T.L.; Edwards, N.; Sveistrup, H.; Andrew, C.; Egan, M.Y. Inequitable walking conditions among older people: Examining the interrelationship of neighbourhood socio-economic status and urban form using a comparative case study. BMC Public Health 2010, 10, 677. [Google Scholar] [CrossRef] [Green Version]
- Newton, R.; Ormerod, M.; Burton, E.; Mitchell, L.; Thompson, C.W. Increasing independence for older people through good street design. J. Integr. Care 2010, 18, 24. [Google Scholar] [CrossRef]
- Meir, I.A.; Garb, Y.; Jiao, D.; Cicelsky, A. Post-occupancy evaluation: An inevitable step toward sustainability. Adv. Build. Energy Res. 2009, 3, 189–219. [Google Scholar] [CrossRef]
- White, M.P.; Elliott, L.R.; Gascon, M.; Roberts, B.; Fleming, L.E. Blue space, health and well-being: A narrative overview and synthesis of potential benefits. Environ. Res. 2020, 1, 110169. [Google Scholar] [CrossRef]
- Grellier, J.; White, M.P.; Albin, M.; Bell, S.; Elliott, L.R.; Gascón, M.; Gualdi, S.; Mancini, L.; Nieuwenhuijsen, M.J.; Sarigiannis, D.A.; et al. BlueHealth: A study programme protocol for mapping and quantifying the potential benefits to public health and well-being from Europe’s blue spaces. BMJ Open 2017, 7, e016188. [Google Scholar] [CrossRef] [Green Version]
- Andreucci, M.B.; Russo, A.; Olszewska-Guizzo, A. Designing Urban Green Blue Infrastructure for Mental Health and Elderly Wellbeing. Sustainability 2019, 11, 6425. [Google Scholar] [CrossRef] [Green Version]
- Garrett, J.K.; White, M.P.; Huang, J.; Ng, S.; Hui, Z.; Leung, C.; Tse, L.A.; Fung, F.; Elliott, L.R.; Depledge, M.H.; et al. Urban blue space and health and wellbeing in Hong Kong: Results from a survey of older adults. Health Place 2019, 55, 100–110. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, S.; Devine, M.T.; Gillespie, T.; Lyons, S.; Nolan, A. Coastal blue space and depression in older adults. Health Place 2018, 54, 110–117. [Google Scholar] [CrossRef] [Green Version]
- Raymond, C.M.; Breil, M.; Nita, M.R.; Kabisch, N.; de Bel, M. An Impact Evaluation Framework to Support Planning and Evaluation of Nature-Based Solutions Projects. Report Prepared by the EKLIPSE Expert Working Group on Nature-Based Solutions to Promote Climate Resilience in Urban Areas; Centre for Ecology and Hydrology: Wallingford, UK, 2017. [Google Scholar]
- Delbosc, A. The role of well-being in transport policy. Transp. Policy 2012, 23, 25–33. [Google Scholar] [CrossRef]
- Marmot, M.; Wilkinson, R. Social Determinants of Health; OUP Oxford: Oxford, UK, 2005. [Google Scholar]
- Klicnik, I.; Dogra, S. Perspectives on Active Transportation in a Mid-Sized Age-Friendly City: “You Stay Home”. Int. J. Environ. Res. Public Health 2019, 16, 4916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Currie, G. Quantifying spatial gaps in public transport supply based on social needs. J. Transp. Geogr. 2010, 18, 31–41. [Google Scholar] [CrossRef]
- Levasseur, M.; Généreux, M.; Bruneau, J.-F.; Vanasse, A.; Chabot, E.; Beaulac, C.; Bédard, M.-M. Importance of proximity to resources, social support, transportation and neighborhood security for mobility and social participation in older adults: Results from a scoping study. BMC Public Health 2015, 15, 503. [Google Scholar] [CrossRef] [Green Version]
- Truong, L.T.; Somenahalli, S.V. Exploring frequency of public transport use among older adults: A study in Adelaide, Australia. Travel Behav. Soc. 2015, 2, 148–155. [Google Scholar] [CrossRef]
- Wong, R.; Szeto, W.; Yang, L.; Li, Y.; Wong, S. Public transport policy measures for improving elderly mobility. Transp. Policy 2018, 63, 73–79. [Google Scholar] [CrossRef] [Green Version]
- Engels, B.; Liu, G.-J. Ageing in place: The out-of-home travel patterns of seniors in Victoria and its policy implications. Urban Policy Res. 2013, 31, 168–189. [Google Scholar] [CrossRef]
- McHugh, B. Pioneering open data standards: The GTFS Story. Beyond Transpar. Open Data Future Civ. Innov. 2013, 1, 125–135. [Google Scholar]
- Broome, K.; Worrall, L.; Fleming, J.; Boldy, D. Evaluation of age-friendly guidelines for public buses. Transp. Res. Part A Policy Pract. 2013, 53, 68–80. [Google Scholar] [CrossRef]
- Baker, E.; Lester, L.H.; Bentley, R.; Beer, A. Poor housing quality: Prevalence and health effects. J. Prev. Interv. Community 2016, 44, 219–232. [Google Scholar] [CrossRef] [PubMed]
- Bentley, R.; Baker, E.; Mason, M.K.; Subramanian, S.V.; Kavanagh, A.M. Association between Housing Affordability and Mental Health: A Longitudinal Analysis of a Nationally Representative Household Survey in Australia. Am. J. Epidemiol. 2011, 174, 753–760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pollack, C.E.; Griffin, B.A.; Lynch, J. Housing affordability and health among homeowners and renters. Am. J. Prev. Med. 2010, 39, 515–521. [Google Scholar] [CrossRef]
- Versey, H.S.; Murad, S.; Willems, P.; Sanni, M. Beyond Housing: Perceptions of Indirect Displacement, Displacement Risk, and Aging Precarity as Challenges to Aging in Place in Gentrifying Cities. Int. J. Environ. Res. Public Health 2019, 16, 4633. [Google Scholar] [CrossRef] [Green Version]
- Vanleerberghe, P.; De Witte, N.; Claes, C.; Schalock, R.L.; Verté, D. The quality of life of older people aging in place: A literature review. Qual. Life Res. 2017, 26, 2899–2907. [Google Scholar] [CrossRef]
- O’Neill, P. Housing affordability literature review and affordable housing program audit. In Urban Research Centre; University of Western Sydney: Sydney, Australia, 2008. [Google Scholar]
- Arnold, E.; Skaburskis, A. Measuring Ontario’s increasing housing affordability problem. Soc. Indic. Res. 1989, 21, 501–515. [Google Scholar] [CrossRef]
- Senate Select Committee on Housing Affordability in Australia. A Good Place is Hard to Find: Housing Affordability in Australia; Australia, C.O., Ed.; Parliament House: Canberra, Australia, 2008. [Google Scholar]
- Morris, A. Housing tenure and the health of older Australians dependent on the age pension for their income. Hous. Stud. 2018, 33, 77–95. [Google Scholar] [CrossRef]
- World Health Organisation. A Conceptual Framework for Action on the Social Determinants of Health: Social Determinants of Health Discussion Paper 2; World Health Organisation: Geneva, Switzerland, 2010. [Google Scholar]
- Kepper, M.M.; Myers, C.A.; Denstel, K.D.; Hunter, R.F.; Guan, W.; Broyles, S.T. The neighborhood social environment and physical activity: A systematic scoping review. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 14. [Google Scholar] [CrossRef]
- Kawachi, I.; Berkman, L.F. Social ties and mental health. J. Urban Health 2001, 78, 458–467. [Google Scholar] [CrossRef] [Green Version]
- Amagasa, S.; Fukushima, N.; Kikuchi, H.; Oka, K.; Takamiya, T.; Odagiri, Y.; Inoue, S. Types of social participation and psychological distress in Japanese older adults: A five-year cohort study. PLoS ONE 2017, 12, e0175392. [Google Scholar] [CrossRef]
- Rosengren, A.; Hawken, S.; Ôunpuu, S.; Sliwa, K.; Zubaid, M.; Almahmeed, W.; Blackett, K.N.; Sitthi-Amorn, C.; Sato, H.; Yusuf, S. Association of psychosocial risk factors with risk of acute myocardial infarction in 11 119 cases and 13 648 controls from 52 countries (the INTERHEART study): Case-control study. Lancet 2004, 364, 953–962. [Google Scholar] [CrossRef]
- Holt-Lunstad, J.; Smith, T.B.; Layton, J.B. Social relationships and mortality risk: A meta-analytic review. PLoS Med. 2010, 7, e1000316. [Google Scholar] [CrossRef]
- Au, A.; Lai, D.W.L.; Yip, H.-M.; Chan, S.; Lai, S.; Chaudhury, H.; Scharlach, A.; Leeson, G. Sense of Community Mediating Between Age-Friendly Characteristics and Life Satisfaction of Community-Dwelling Older Adults. Front. Psychol. 2020, 11, 86. [Google Scholar] [CrossRef] [Green Version]
- Zunzunegui, M.-V.; Alvarado, B.E.; Del Ser, T.; Otero, A. Social networks, social integration, and social engagement determine cognitive decline in community-dwelling Spanish older adults. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2003, 58, 93–100. [Google Scholar] [CrossRef] [Green Version]
- Roth, A.R. Social networks and health in later life: A state of the literature. Sociol. Health Illn. 2020, 42, 1642–1656. [Google Scholar] [CrossRef]
- Neville, S.; Adams, J.; Napier, S.; Shannon, K.; Jackson, D. “Engaging in my rural community”: Perceptions of people aged 85 years and over. Int. J. Qual. Stud. Health Well-Being 2018, 13, 1503908. [Google Scholar] [CrossRef]
- Jo Cox Loneliness Commission. Combatting Loneliness One Conversation at a Time: A Call to Action; Jo Cox Loneliness Commission: London, UK, 2017. [Google Scholar]
- Walker, R.B.; Hiller, J.E. Places and health: A qualitative study to explore how older women living alone perceive the social and physical dimensions of their neighbourhoods. Soc. Sci. Med. 2007, 65, 1154–1165. [Google Scholar] [CrossRef]
- Woolrych, R.; Sixsmith, J.; Fisher, J.; Makita, M.; Lawthom, R.; Murray, M. Constructing and negotiating social participation in old age: Experiences of older adults living in urban environments in the United Kingdom. Ageing Soc. 2019, 2019, 1–23. [Google Scholar] [CrossRef] [Green Version]
- Aabo, V. The role and value of public libraries in the age of digital technologies. J. Librariansh. Inf. Sci. 2005, 37, 205–211. [Google Scholar] [CrossRef]
- Barclay, D.A. Space and the Social Worth of Public Libraries. Public Libr. Q. 2017, 36, 267–273. [Google Scholar] [CrossRef] [Green Version]
- Swindell, R. U3A Online: Building a global learning community of older people. Australas. J. Ageing 2009, 28, A80. [Google Scholar]
- Swindell, R.; Thompson, J. An international perspective on the University-Of-The-3rd-Age. Educ. Gerontol. 1995, 21, 429–447. [Google Scholar] [CrossRef]
- Zajac-Gawlak, I.; Pośpiech, D.; Kroemeke, A.; Mossakowska, M.; Gába, A.; Pelclová, J.; Přidalová, M.; Kłapcińska, B. Physical activity, body composition and general health status of physically active students of the University of the Third Age (U3A). Arch. Gerontol. Geriatr. 2016, 64, 66–74. [Google Scholar] [CrossRef]
- Putnam, R.D. Bowling Alone: The Collapse and Revival of American Community; Simon and Schuster: New York, NY, USA, 2000. [Google Scholar]
- Chen, W.; Ling, L.; Renzaho, A.M.N. Building a new life in Australia: An analysis of the first wave of the longitudinal study of humanitarian migrants in Australia to assess the association between social integration and self-rated health. BMJ Open 2017, 7, 11. [Google Scholar] [CrossRef]
- Brown, R.K.; Taylor, R.J.; Chatters, L.M. Race/Ethnic and Social-Demographic Correlates of Religious Non-Involvement in America: Findings from Three National Surveys. J. Black Stud. 2015, 46, 335–362. [Google Scholar] [CrossRef]
- Maliepaard, M.; Phalet, K. Social Integration and Religious Identity Expression among Dutch Muslims: The Role of Minority and Majority Group Contact. Soc. Psychol. Q. 2012, 75, 131–148. [Google Scholar] [CrossRef]
- Coombs, T.; Nicholas, A.; Pirkis, J. A review of social inclusion measures. Aust. N. Z. J. Psychiatry 2013, 47, 906–919. [Google Scholar] [CrossRef]
- Morgan, C.; Burns, T.; Fitzpatrick, R.; Pinfold, V.; Priebe, S. Social exclusion and mental health: Conceptual and methodological review. Br. J. Psychiatry 2007, 191, 477–483. [Google Scholar] [CrossRef]
- Walsh, K.; Scharf, T.; Keating, N. Social exclusion of older persons: A scoping review and conceptual framework. Eur. J. Ageing 2017, 14, 81–98. [Google Scholar] [CrossRef] [Green Version]
- Whitehead, M.; Pennington, A.; Orton, L.; Nayak, S.; Petticrew, M.P.; Sowden, A.J.; White, M. How could differences in ‘control over destiny’ lead to socio-economic inequalities in health? A synthesis of theories and pathways in the living environment. Health Place 2016, 39, 51–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marmot, M.G.; Stansfeld, S.; Patel, C.; North, F.; Head, J.; White, I.; Brunner, E.; Feeney, A.; Smith, G. Health inequalities among British civil servants: The Whitehall II study. Lancet 1991, 337, 1387–1393. [Google Scholar] [CrossRef]
- Dahlgren, G.; Whitehead, M. European Strategies for Tackling Social Inequities in Health: Levelling up Part 2. Studies on Social and Economic Determinants of Population Health, No. 3; World Health Organization Regional Office for Europe Copenhagen: Copenhagen, Denmark, 2007; Volume 89384, Available online: http://www.euro.who.int/__data/assets/pdf_file/0018/103824E (accessed on 18 November 2019).
- Cahill, K.E.; Giandrea, M.D.; Quinn, J.F. Evolving Patterns of Work and Retirement. In Handbook of Aging and the Social Sciences, 8th ed.; George, L.K., Ferraro, K.F., Eds.; Academic Press: San Diego, CA, USA, 2016; pp. 271–291. [Google Scholar]
- Serrat, R.; Scharf, T.; Villar, F.; Gómez, C. Fifty-Five Years of Research Into Older People’s Civic Participation: Recent Trends, Future Directions. Gerontologist 2019, 60, e38–e51. [Google Scholar] [CrossRef] [Green Version]
- Burr, J.A.; Caro, F.G.; Moorhead, J. Productive aging and civic participation. J. Aging Stud. 2002, 16, 87–105. [Google Scholar] [CrossRef]
- Winterton, R.; Warburton, J. Healthy ageing in Australia’s rural places: The contribution of older volunteers. Volunt. Sect. Rev. 2014, 5, 181–201. [Google Scholar] [CrossRef] [Green Version]
- Winterton, R.; Warburton, J. Does place matter? Reviewing the experience of disadvantage for older people in rural Australia. Rural Soc. 2011, 20, 187–197. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. Household Use of Information Technology, Australia; 2016–2017 cat. no. 8146.0 2018; Australian Bureau of Statistics: Canberra, Australia, 2018.
- Everingham, J.-A.; Petriwskyj, A.; Warburton, J.; Cuthill, M.; Bartlett, H. Information provision for an age-friendly community. Ageing Int. 2009, 34, 79–98. [Google Scholar] [CrossRef]
- Sixsmith, A.; Sixsmith, J. Ageing in place in the United Kingdom. Ageing Int. 2008, 32, 219–235. [Google Scholar] [CrossRef]
- Hummert, M.L.; Wiemann, J.M.; Nussbaum, J.F. Interpersonal Communication in Older Adulthood; Sage: Thousand Oaks, CA, USA, 1994. [Google Scholar]
- Freeman, S.; Marston, H.R.; Olynick, J.; Musselwhite, C.; Kulczycki, C.; Genoe, M.R.; Xiong, B. Intergenerational Effects on the Impacts of Technology Use in Later Life: Insights from an International, Multi-Site Study. Int. J. Environ. Res. Public Health 2020, 17, 5711. [Google Scholar] [CrossRef]
- Liddle, J.; Pitcher, N.; Montague, K.; Hanratty, B.; Standing, H.; Scharf, T. Connecting at Local Level: Exploring Opportunities for Future Design of Technology to Support Social Connections in Age-Friendly Communities. Int. J. Environ. Res. Public Health 2020, 17, 5544. [Google Scholar] [CrossRef]
- Silvius, H.A.; Tak, E.C.P.M.; Mook-Kanamori, D.O.; Vos, H.M.; Numans, M.E.; Chavannes, N.H. Effects of Technology Use on Ageing in Place: The iZi Pilots. Int. J. Environ. Res. Public Health 2020, 17, 5052. [Google Scholar] [CrossRef] [PubMed]
- Marston, H.R.; van Hoof, J. “Who doesn’t think about technology when designing urban environments for older people?” A case study approach to a proposed extension of the WHO’s age-friendly cities model. Int. J. Environ. Res. Public Health 2019, 16, 3525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Browning, C.; Davis, J.; Thomas, S. Primary Health Care and Older People. In Ageing in Australia: Challenges and Opportunities; Oloughlin, K., Browning, C., Kendig, H., Eds.; WHO: Geneva, Switzerland, 2017; pp. 225–237. [Google Scholar]
- Van Dijk, H.M.; Cramm, J.M.; Van Exel, J.; Nieboer, A.P. The ideal neighbourhood for ageing in place as perceived by frail and non-frail community-dwelling older people. Ageing Soc. 2015, 35, 1771–1795. [Google Scholar] [CrossRef]
- Ratcliffe, S. Oxford Essential Quotations; Oxford University Press: Oxford, UK, 2016. [Google Scholar]
- Cobb, C.W.; Rixford, C. Lessons Learned from the History of Social Indicators; Redefining Progress: San Francisco, CA, USA, 1998; Volume 1. [Google Scholar]
- Innes, J.E. Disappointments and legacies of social indicators. J. Public Policy 1989, 9, 429–432. [Google Scholar] [CrossRef]
- Byrne, C.; Harris, C. Climate Change in an Ageing World. HelpAge International. 2015. Available online: https://reliefweb.int/sites/reliefweb.int/files/resources/COP21_HelpAge_PositionPaper_Final_0.pdf (accessed on 18 November 2019).
- Dicks, L.; Haddaway, N.; Hernández-Morcillo, M.; Mattsson, B.; Randall, N.; Failler, P.; Ferretti, J.; Livoreil, B.; Saarikoski, H.; Santamaria, L.; et al. Knowledge Synthesis for Environmental Decisions: An Evaluation of Existing Methods, and Guidance for their Selection, Use and Development: A Report from the EKLIPSE Project; European Union Funding for Research & Innovation: Brussels, Belgium, 2017. [Google Scholar]



{kind=link}
{kind=link}
| AFC Domains | Suggested Spatial Indicators for AFC Assessment and Monitoring |
|---|---|
| 1. Outdoor spaces and buildings |
|
| 2. Transport |
|
| 3. Housing |
|
| 4. Social Participation |
|
| 5. Respect and social inclusion |
|
| 6. Civic participation and employment |
|
| 7. Communications and information |
|
| 8. Community support and health services |
|
| Additional contextual factors for consideration include: the Estimated Resident Population; proportion of population aged more than 60 years; population age distribution including proportions of older and younger populations in area; ethnicity; education; homeownership; residential density; remoteness e.g., Accessibility/Remoteness Indices or the distance between towns in rural settings; the risk of natural disasters; climatic conditions; and the impact of climate change. | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Davern, M.; Winterton, R.; Brasher, K.; Woolcock, G. How Can the Lived Environment Support Healthy Ageing? A Spatial Indicators Framework for the Assessment of Age-Friendly Communities. Int. J. Environ. Res. Public Health 2020, 17, 7685. https://doi.org/10.3390/ijerph17207685
Davern M, Winterton R, Brasher K, Woolcock G. How Can the Lived Environment Support Healthy Ageing? A Spatial Indicators Framework for the Assessment of Age-Friendly Communities. International Journal of Environmental Research and Public Health. 2020; 17(20):7685. https://doi.org/10.3390/ijerph17207685
Chicago/Turabian StyleDavern, Melanie, Rachel Winterton, Kathleen Brasher, and Geoff Woolcock. 2020. "How Can the Lived Environment Support Healthy Ageing? A Spatial Indicators Framework for the Assessment of Age-Friendly Communities" International Journal of Environmental Research and Public Health 17, no. 20: 7685. https://doi.org/10.3390/ijerph17207685