Framework for Participatory Quantitative Health Impact Assessment in Low- and Middle-Income Countries

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Methods
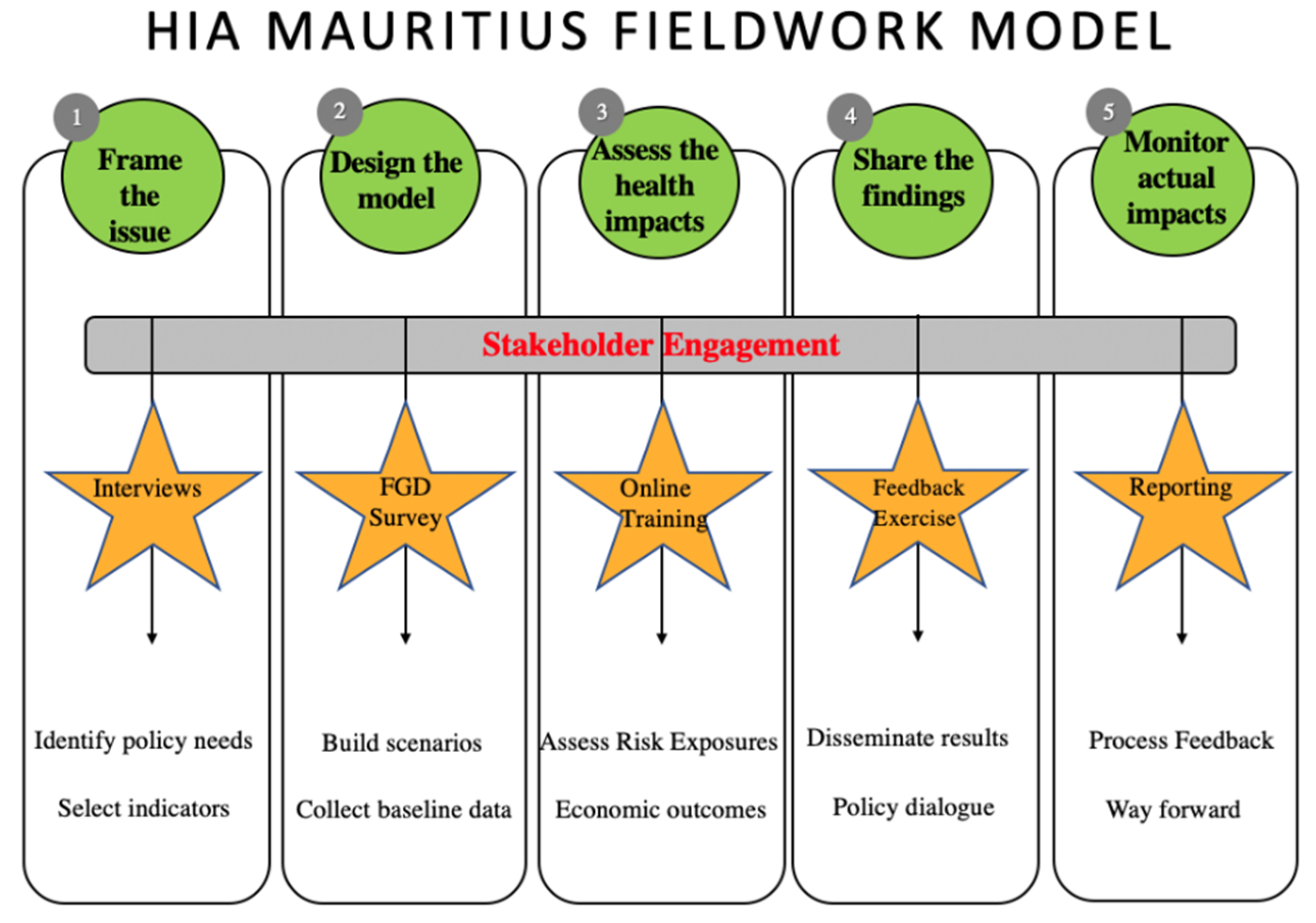
2.1. Case Study
2.1.1. Sampling and Participant Profiles
2.1.2. Individual Interviews
- Urban transport planning (UTP) measures that stakeholders are most familiar with;
- Different factors stakeholders consider to lie in the interface between urban transport planning and health;
- Factors missing in the current situation and challenges face by the UTP sector; and
- Idea of a healthy, feasible and sustainable UTP system and what is needed to achieve this.
2.1.3. Focus Group Discussions
- Their individual experiences as citizens, their needs and their priorities;
- Their opinions on the 3 proposed scenarios;
- How their visions differ and clash with the 3 scenarios; and
- Whether they can reach similar endpoints.
2.1.4. Feedback Exercise
- Reporting of baseline exposure data and final HIA results;
- Relevance of HIA outcomes to stakeholders’ positions and fields;
- Re-integration of HIA results in the society;
- Feedback on participatory HIA process; and
- Review and in some cases co-drafting, of the policy brief delivered to the authorities (see Supplementary Materials annex).
2.1.5. Fieldnotes
2.2. Quality Criteria Assessment
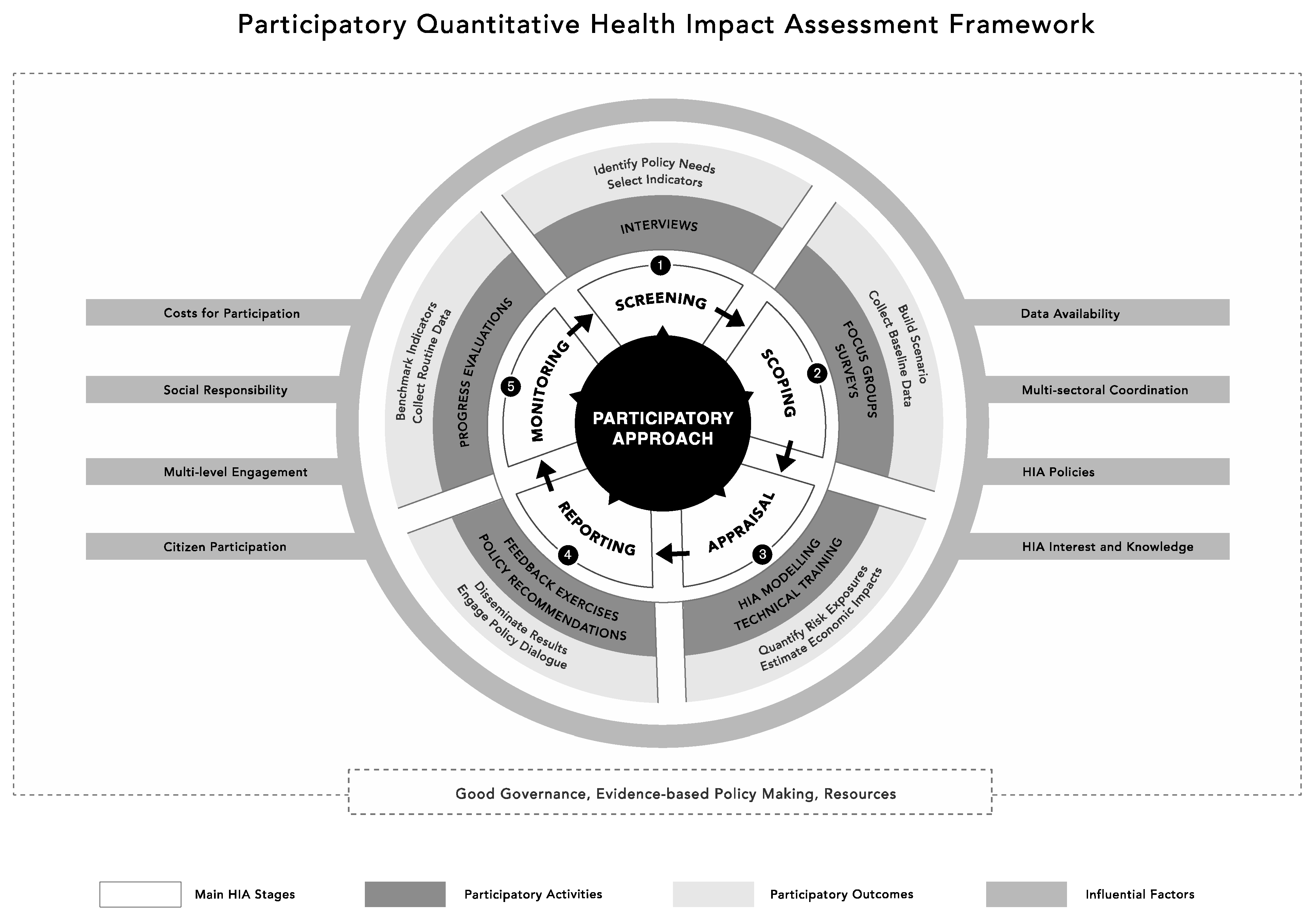
3. Results
- (1)
- A three-layered circular figure depicting the five main HIA stages. For each stage, a summary of participatory activities (intermediate circle) and outcomes (outer circle) is proposed.
- (2)
- A set of eight factors that can influence the process of PQHIA are presented as grey background rectangles.
- (3)
- A dotted rectangle presents three areas of opportunities for proper integration of PQHIA process in the outside environment.
3.1. Component 1
3.2. Component 2
3.2.1. Cost for Participation
3.2.2. Stakeholder Knowledge and Interest in HIA
‘In Mauritius, as soon as you come with monetary values, people take you seriously (…) We carry much attention to this issue [road accidents], yet, it all comes down to money if this is to be taken seriously’(ID07)
3.2.3. Social Responsibility
‘lately, they [policy makers] organised big consultation meetings and declared they would improve green spaces, increase pedestrianizations, plants trees on the Citadelle. All the newspapers reported this…But I see nothing, nothing, nothing...’(ID13)
3.2.4. HIA Policies
‘The underlying issue lies in the lack of regulatory policy frameworks: a legal administrative protocol to use tools such as HIA and a framework that goes beyond government or private mandates’(R, FGD2)
‘If we have policies, we need to apply them sustainably’ (R, FGD2). Finally, ‘having law is not enough, we need to enforce them’ (IDI4). Finally, a participant stresses that there should be continuity between policy-making and policy integration in order to translate HIA outcomes into actions. ‘It should be the same policymakers who formulate [policies] and integrate [policy-driven actions and interventions] too’(ID07)
3.2.5. Data Availability
‘I think they do not use what they have intelligently, they do not know what they have) […] there is a lot of data management equipment that is being under-utilized’ (ID 10). Such data (e.g., that there is better air quality on Sunday because people do not travel as much) should be directly used to encourage and increase awareness of the public(ID12)
‘People are concerned about their security on bicycle, but this is a lie that protects the car […] of course the road is dangerous, especially for the two-wheelers, but this should not be encouraging the restriction of cycling modes and favour the use of cars’(G, FGD1)
3.2.6. Multi-Sectoral Coordination
3.2.7. Multi-Level Stakeholder Engagement
‘Half of the doctors are very interested [in impacts of environment on health], but there are no avenues for them to actually get data […] All the policies or everything that they produce make sense but the human reality is different...it would be better if they were aware of the meaning of their work’(IDI 10)
3.2.8. Citizen Participation
3.3. Component 3
3.3.1. Good Governance
3.3.2. Evidence-Based Policymaking
3.3.3. Resources
‘In Mauritius, the best urban and transport planning achievements, including those that benefit health, have been completed without specific strategy and clear planning. There is local pride in this approach to development, leaving very little space for critique’(IDI08)
4. Conclusions
- Methods for participation (e.g., activities, sample size and study period) should be carefully planned, in advance, based on budget and time available.
- The flexibility afforded by choosing the type, form, and duration of HIA alongside local communities is crucial for stakeholders to use and most benefit from PQHIA.
- Focusing on the areas of opportunities highlighted in the framework can have wider benefits on governance systems, policy-making practices, and access to resources in LMICs.
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- European Centre for Health Policy. Gothenburg Consensus Paper; WHO Regional Office for Europe: Copenhagen, Denmark, 1999. [Google Scholar]
- Spickett, J.; Katscherian, D.; Brown, H.; Rumchev, K. Health impact assessment: Improving its effectiveness in the enhancement of health and well-being. Int. J. Environ. Res. Public Health 2015, 12, 3847–3852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knoblauch, A.M.; Divall, M.J.; Owuor, M.; Archer, C.; Nduna, K.; Ng’uni, H.; Musunka, G.; Pascall, A.; Utzinger, J.; Winkler, M.S. Monitoring of Selected Health Indicators in Children Living in a Copper Mine Development Area in Northwestern Zambia. Int. J. Environ. Res. Public Health 2017, 14, 315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knoblauch, A.M.; Hodges, M.H.; Bah, M.S.; Kamara, H.I.; Kargbo, A.; Paye, J.; Turay, H.; Nyorkor, E.D.; Divall, M.J.; Zhang, Y.; et al. Changing patterns of health in communities impacted by a bioenergy project in northern Sierra Leone. Int. J. Environ. Res. Public Health 2014, 11, 12997–13016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, H.; Spickett, J. Health consequence scales for use in health impact assessments of climate change. Int. J. Environ. Res. Public Health 2014, 11, 9607–9620. [Google Scholar] [CrossRef] [PubMed]
- Ata, A. Declaration of Alma-ata. In Proceedings of the International Conference on Primary Health Care, Almaty, Kazakhstan, 6–12 September 1978; p. 12. [Google Scholar]
- Iroz-Elardo, N.; McSharry McGrath, M. Social Learning through Stakeholder Engagement: New Pathways from Parcipitation to Health Equity in US West Coast HIA. Chron. Health Impact Assess. 2016, 1, 9–21. [Google Scholar] [CrossRef] [Green Version]
- Haigh, F.; Harris, E.; Chok, H.N.G.; Baum, F.; Harris-Roxas, B.; Kemp, L.; Spickett, J.; Keleher, H.; Morgan, R.K.; Harris, M.; et al. Characteristics of health impact assessments reported in Australia and New Zealand 2005–2009. Aust. N. Z. J. Public Health 2013, 37, 534–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamburrini, A.-L.; Gilhuly, K.; Harris-Roxas, B. Enhancing benefits in health impact assessment through stakeholder consultation. Impact Assess. Proj. Apprais. 2011, 29, 195–204. [Google Scholar] [CrossRef]
- Linzalone, N.; Bianchi, F.; Curzio, O.; Serasini, L.; Natali, M.; T4HIA Project Working Group. Theory and practice to integrating health in environmental assessment: Synthesis of an experience with stakeholders to deliver a national HIA guideline. Environ. Impact Assess. Rev. 2019, 77, 49–59. [Google Scholar] [CrossRef]
- Den Broeder, L.; Chung, K.Y.; Geelen, L.; Scholtes, M.; Schuit, A.J.; Wagemakers, A. We are all experts! Does stakeholder engagement in health impact scoping lead to consensus? A Dutch case study. Impact Assess. Proj. Apprais. 2016, 34, 294–305. [Google Scholar] [CrossRef] [Green Version]
- Jones, J.; Nix, N.A.; Snyder, E.H. Local perspectives of the ability of HIA stakeholder engagement to capture and reflect factors that impact Alaska Native health. Int. J. Circumpolar Health 2014, 73, 24411. [Google Scholar] [CrossRef]
- Kearney, M. Walking the walk? Community participation in HIA: A qualitative interview study. Environ. Impact Assess. Rev. 2004, 24, 217–229. [Google Scholar] [CrossRef]
- Greig, S.; Parry, N.; Rimmington, B. Promoting sustainable regeneration: Learning from a case study in participatory HIA. Environ. Impact Assess. Rev. 2004, 24, 255–267. [Google Scholar] [CrossRef]
- Den Broeder, L.; Uiters, E.; ten Have, W.; Wagemakers, A.; Schuit, A.J. Community participation in Health Impact Assessment. A scoping review of the literature. Environ. Impact Assess. Rev. 2017, 66, 33–42. [Google Scholar] [CrossRef]
- Negev, M.; Levine, H.; Davidovitch, N.; Bhatia, R.; Mindell, J. Integration of health and environment through health impact assessment: Cases from three continents. Environ. Res. 2012, 114, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Negev, M. Knowledge, data and interests: Challenges in participation of diverse stakeholders in HIA. Environ. Impact Assess. Rev. 2012, 33, 48–54. [Google Scholar] [CrossRef]
- Hurlbert, M.; Gupta, J. The split ladder of participation: A diagnostic, strategic, and evaluation tool to assess when participation is necessary. Environ. Sci. Policy 2015, 50, 100–113. [Google Scholar] [CrossRef]
- Thondoo, M.; Rojas-Rueda, D.; Gupta, J.; de Vries, D.H.; Nieuwenhuijsen, M.J. Systematic Literature Review of Health Impact Assessments in Low and Middle-Income Countries. Int. J. Environ. Res. Public Health 2019, 16, 2018. [Google Scholar] [CrossRef] [Green Version]
- Nieuwenhuijsen, M.J.; Khreis, H.; Verlinghieri, E.; Mueller, N.; Rojas-Rueda, D. Participatory quantitative health impact assessment of urban and transport planning in cities: A review and research needs. Environ. Int. 2017, 103, 61–72. [Google Scholar] [CrossRef] [Green Version]
- Mueller, N.; Rojas-Rueda, D.; Basagaña, X.; Cirach, M.; Cole-Hunter, T.; Dadvand, P.; Donaire-Gonzalez, D.; Foraster, M.; Gascon, M.; Martinez, D.; et al. Urban and transport planning related exposures and mortality: A health impact assessment for cities. Environ. Health Perspect. 2017, 125, 89–96. [Google Scholar] [CrossRef]
- Veerman, J.L. Quantitative Health Impact Assessment: An Exploration of Methods and Validity; Erasmus, M.C., Ed.; University Medical Center Rotterdam: Rotterdam, The Netherlands, 2007. [Google Scholar]
- Anggraeni, M.; Gupta, J.; Verrest, H.J.L.M. Cost and value of stakeholders participation: A systematic literature review. Environ. Sci. Policy 2019, 101, 364–373. [Google Scholar] [CrossRef]
- Thondoo, M.; Mueller, N.; Rojas-Rueda, D.; de Vries, D.; Gupta, J.; Nieuwenhuijsen, M.J. Participatory quantitative health impact assessment of urban transport planning: A case study from Eastern Africa. Environ. Int. 2020, 144, 106027. [Google Scholar] [CrossRef] [PubMed]
- Thondoo, M. Small Cities, Big Needs: Citizen Participation in Urban and Transport Planning. Environ. Epidemiol. 2019, 3, 394. [Google Scholar]
- Ramirez-Rubio, O.; Daher, C.; Fanjul, G.; Gascon, M.; Mueller, N.; Pajín, L.; Plasencia, A.; Rojas-Rueda, D.; Thondoo, M.; Nieuwenhuijsen, M.J. Urban health: An example of a “health in all policies” approach in the context of SDGs implementation. Glob. Health 2019, 15, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Arnstein, S.R. A ladder of citizen participation. J. Am. Inst. Plan. 1969, 35, 216–224. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Using Health Impact Assessment (HIA); WHO: Geneva, Switzerland, 2012. [Google Scholar]
- Green, J.; Thorogood, N. Qualitative Methods for Health Research; SAGE: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- World Bank. Countries by Population Density 2015 [Internet]. 2013. Available online: http://statisticstimes.com/population/countries-by-population-density.php (accessed on 1 October 2017).
- Dreaves, H.; Pennington, A.; Scott-Samuel, A. Urban Health Impact Assessment Methodology (UrHIA); University of Liverpool: Liverpool, UK, 2015. [Google Scholar]
- Domínguez-Ares, E.; Martín-Olmedo, P.; Iglesias-Merchan, C. Perception survey on the relevance of main categories of health determinants for conducting health impact assessment. Environ. Impact Assess. Rev. 2020, 85, 106445. [Google Scholar] [CrossRef]
- Lincoln, Y.S.; Lynham, S.A.; Guba, E.G. Paradigmatic controversies, contradictions, and emerging confluences, revisited. SAGE Handb. Qual. Res. 2011, 4, 97–128. [Google Scholar]
- Signal, L.; Langford, B.; Quigley, R.; Ward, M. Strengthening health, wellbeing and equity: Embedding policy-level HIA in New Zealand. Soc. Policy J. N. Z. 2006, 29, 17. [Google Scholar]
- Jones, B.A. What are the health costs of uranium mining? A case study of miners in Grants, New Mexico. Int. J. Occup. Environ. Health 2014, 20, 289–300. [Google Scholar] [CrossRef] [Green Version]
- Rojas-Rueda, D.; Gascon, M.; Torrico, S.; Torrico, F.; Manaca, M.N.; Plasència, A.; Nieuwenhuijsen, M.J. Urban Policies and Health in Developing Countries: The Case of Maputo (Mozambique) and Cochabamba (Bolivia). Public Health Open J. 2016, 1, 24–31. [Google Scholar]
- Harris, P.; Viliani, F.; Spickett, J. Assessing health impacts within environmental impact assessments: An opportunity for public health globally which must not remain missed. Int. J. Environ. Res. Public Health 2015, 12, 1044–1049. [Google Scholar] [CrossRef]
- De Blasio, A.; Giran, J.; Nagy, Z. Potentials of health impact assessment as a local health policy supporting tool. Perspect. Public Health 2012, 132, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Lazenbatt, A.; Lynch, U.; O’Neill, E. Revealing the hidden ‘troubles’ in Northern Ireland: The role of participatory rapid appraisal. Health Educ. Res. 2001, 16, 567–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mittelmark, M.B. Promoting social responsibility for health: Health impact assessment and healthy public policy at the community level. Promot. Health Int. 2001, 16, 269–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.H.; Robbel, N.; Dora, C. Cross-Country Analysis of the Institutionalization of Health Impact Assessment; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- Thondoo, M.; Gupta, J. Health impact assessment legislation in developing countries: A path to sustainable development? Rev. Eur. Comp. Int. Environ. Law 2020. [Google Scholar] [CrossRef]
- Hebert, K.A.; Wendel, A.M.; Kennedy, S.K.; Dannenberg, A.L. Health impact assessment: A comparison of 45 local, national, and international guidelines. Environ. Impact Assess. Rev. 2012, 34, 74–82. [Google Scholar] [CrossRef]
- International Institute for Sustainable Development. Health and Environment in Africa Bulletin; IISD: Winnipeg, MB, Canada, 2008; pp. 1–17. [Google Scholar]
- Chilaka, M.A.; Ndioho, I. Strategies and incentives for enhancing the application of health impact assessment (HIA) in Nigeria: A view from those who should know. Int. J. Health Promot. Educ. 2015, 53, 172–179. [Google Scholar] [CrossRef]
- Arts, J.; Runhaar, H.A.C.; Fischer, T.B.; Jha-Thakur, U.; Van Laerhoven, F.; Driessen, P.P.J.; Onyango, V. The effectiveness of EIA as an instrument for environmental governance: Reflecting on 25 years of EIA practice in the Netherlands and the UK. In Progress in Environmental Assessment Policy, and Management Theory and Practice; World Scientific: Singapore, 2016; pp. 171–210. [Google Scholar]
- Chanchitpricha, C.; Bond, A. Investigating the effectiveness of mandatory integration of health impact assessment within environmental impact assessment (EIA): A case study of Thailand. Impact Assess. Proj. Apprais. 2018, 36, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Gaber, J.; Overacker, T. Identifying community engagement research techniques and sampling strategies via Health Impact Assessments (HIAs): Applied planning lessons on generating emic and etic community observations. In Place-Based Evaluation for Integrated Land-Use Management; Routledge: London, UK, 2015; p. 113. [Google Scholar]
- Kaufmann, D. Governance Indicators: Where Are We, Where Should We Be Going? World Bank Tech Pap [Internet]. 2007. Available online: http://info.worldbank.org/governance/wgi/pdf/wps4370.pdf (accessed on 21 October 2020).
- Ståhl, T.; Wismar, M.; Ollila, E.; Lahtinen, E.; Leppo, K. Health in All Policies: Prospects and Potentials; Ministry of Social Affairs and Health Helsinki: Helsinki, Finland, 2006.
- Verlinghieri, E. Learning from the grassroots: A resourcefulness-based worldview for transport planning. Transp. Res. Part A Policy Pract. 2020, 133, 364–377. [Google Scholar] [CrossRef]
- Dinda, S. Environmental Kuznets curve hypothesis: A survey. Ecol. Econ. 2004, 49, 431–455. [Google Scholar] [CrossRef] [Green Version]
- Molnar, A.; Adam, B.; Antova, T.; Bosak, L.; Dimitrov, P.; Mileva, H.; Pekarcikova, J.; Zurlyte, I.; Gulis, G.; Ádány, R.; et al. Health impact assessment of Roma housing policies in Central and Eastern Europe: A comparative analysis. Environ. Impact Assess. Rev. 2012, 33, 7–14. [Google Scholar] [CrossRef] [Green Version]
- Mochungong, P.I.K.; Gulis, G.; Sodemann, M. Clinical waste incinerators in Cameroon—A case study. Int. J. Health Care Qual. Assur. 2012, 25, 6–18. [Google Scholar] [CrossRef]
- Winkler, M.S.; Divall, M.J.; Krieger, G.R.; Balge, M.Z.; Singer, B.H.; Utzinger, J. Assessing health impacts in complex eco-epidemiological settings in the humid tropics: The centrality of scoping. Environ. Impact Assess. Rev. 2011, 31, 310–319. [Google Scholar] [CrossRef]
- Briggs, D.J. A framework for integrated environmental health impact assessment of systemic risks. Environ. Health 2008, 7, 61. [Google Scholar] [CrossRef] [Green Version]
- Joffe, M.; Mindell, J. A framework for the evidence base to support Health Impact Assessment. J. Epidemiol. Community Health 2002, 56, 132–138. [Google Scholar] [CrossRef] [Green Version]
- Winkler, M.; Krieger, G.R.; Divall, M.J.; Cissé, G.; Wielga, M.; Singer, B.H.; Tanner, M.; Utzinger, J. Untapped potential of health impact assessment. Bull. World Health Organ. 2013, 91, 298–305. [Google Scholar] [CrossRef]
- Ross, C.L.; Orenstein, M.; Botchwey, N. Engaging Stakeholders and Vulnerable Populations in HIA. In Health Impact Assessment in the United States; Springer: Berlin/Heidelberg, Germany, 2014; pp. 157–166. [Google Scholar]
- Haigh, F.; Baum, F.; Dannenberg, A.L.; Harris, M.F.; Harris-Roxas, B.; Keleher, H.; Kemp, L.; Morgan, R.; Chok, H.N.G.; Spickett, J.; et al. The effectiveness of health impact assessment in influencing decision-making in Australia and New Zealand 2005–2009. BMC Public Health 2013, 13, 1188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wismar, M.; Blau, J.; Ernst, K.; Figueras, J. The Effectiveness of Health Impact Assessment: Scope and Limitations of Supporting Decision-Making in Europe; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Soria-Lara, J.A.; Banister, D. Participatory visioning in transport backcasting studies: Methodological lessons from Andalusia (Spain). J. Transp. Geogr. 2017, 58, 113–126. [Google Scholar] [CrossRef] [Green Version]
- Davenport, C.; Mathers, J.; Parry, J. Use of health impact assessment in incorporating health considerations in decision making. J. Epidemiol. Community Health 2006, 60, 196–201. [Google Scholar] [CrossRef] [Green Version]
- O’Mullane, M. Implementing the legal provisions for HIA in Slovakia: An exploration of practitioner perspectives. Health Policy 2014, 117, 112–119. [Google Scholar] [CrossRef]
- Gauld, R.; Bloomfield, A.; Kiro, C.; Lavis, J.; Ross, S. Conceptions and uses of public health ideas by New Zealand government policymakers: Report on a five-agency survey. Public Health 2006, 120, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Chilaka, M.A. Vital statistics relating to the practice of Health Impact Assessment (HIA) in the United Kingdom. Environ. Impact Assess. Rev. 2010, 30, 116–119. [Google Scholar] [CrossRef]
- Lavis, J.N.; Ross, S.E.; Stoddart, G.L.; Hohenadel, J.M.; McLeod, C.B.; Evans, R.G. Do Canadian civil servants care about the health of populations? Am. J. Public Health 2003, 93, 658–663. [Google Scholar] [CrossRef] [PubMed]
- Diallo, T.A. L’évaluation D’impact sur la Santé, L’outil le plus Efficace Pour Évaluer L’impact sur la Santé des Politiques Urbaines de Réduction des gaz à Effet de Serre; University of Geneva: Geneva, Switzerland, 2015. [Google Scholar]
- Linzalone, N.; Assennato, G.; Ballarini, A.; Cadum, E.; Cirillo, M.; Cori, L.; de Maio, F.; Musmeci, L.; Natali, M.; Rieti, S.; et al. Health Impact Assessment practice and potential for integration within environmental impact and strategic environmental assessments in Italy. Int. J. Environ. Res. Public Health 2014, 11, 12683–12699. [Google Scholar] [CrossRef] [Green Version]
- Inmuong, U.; Rithmak, P.; Srisookwatana, S.; Traithin, N.; Maisuporn, P. Participatory health impact assessment for the development of local government regulation on hazard control. Environ. Impact Assess. Rev. 2011, 31, 412–414. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Communities of Interest | Expertise (Information Held) | Reason to for Inclusion |
|---|---|---|
| Community-based organization | Expert (Ecosystems) | Active role in liaising between communities and developers of private urban project |
| Service provider/industry | Consultant (Sustainable development) | Consults for public and multilateral organizations on the environmental impacts of land and sea infrastructure projects |
| Elected official | Adviser (Land Transport) | Provides expert advice and strategies to the high-level politicians on transport related policies |
| Elected official | Permanent secretary (Medicine and health) | Reviews environmental impact assessment reports on national projects in order to identify health risks |
| Industry | Planner (Urban planning) | Leads on private and public transport urban planning projects such as main bus terminal |
| Public agency | Statistician (Land transport) | Updates and monitors data on land transport such as traffic incidents and deaths |
| International multilateral organization | Head of department (Sustainable development) | Reports on the advancement of sustainable development targets on the island including SDG 11 |
| Public agency | Head of department (Traffic Planning) | In charge of deploying public transport strategies and involved in the new light-rail public transit system |
| Public agency at parastatal level | Technician (Sustainable economic development) | Works on establishing urban standard guidelines for economic development focusing on investments in transport, social housing and real estate projects |
| Public Agency at municipal level | Municipal agent (Town planning and services) | Works at municipal level on housing and transport initiatives and municipal policies |
| Industry | Executive and board director (Economic investments, Food services and Sustainable development) | Directs decisions for different companies focused on services and investments in the city of Port Louis |
| Resident | Journalist (Urban development) | Critically analyses and reports on urban development projects across the island |
| Resident | Politician (Social and economic development) | Leads a stand-alone political party with expertise in sustainable economies |
| Resident | Social worker (Health and social justice) | Provides support and leads initiatives supporting the urban poor in the capital |
| Meeting with | Data Needed | Category | Institutional Affiliation |
|---|---|---|---|
| Health statistician | Population Census by gender and age | Demographic | National Institute of Statistics |
| Land transport agent | Mode and time of travel by gender and age | Transport | National Transport Agency Ministry of public infrastructure and land transport Private transport provider |
| Environmental expert | Air pollution emissions inventory and database | Air pollution | National Environmental Laboratory Ministry of Environment |
| Public Health statistician NCD expert Permanent secretary | Health and Physical activity survey data by gender and age | Physical activity | Ministry of Health |
| Police officers Hospital staff Transport expert | Records of traffic collisions Vital registration statistics Hospital records | Road deaths | Police headquarters and traffic offices Transport agency National institute of statistics Hospitals |
| Health researcher Health statistician | Vital registration statistics Burden of disease data | Burden of disease | National institute of statistics Health agency University of Mauritius |
| Climatologist Weather expert | Daily mean temperature | Heat | Mauritius Meteorological station |
| Urban planner GIS expert Permanent secretary Architect | Map of land use Topography layers Public transport route maps | Land use | Ministry of Housing and Lands Economic Development Board Ministry of Local Government and disaster risk management |
| Criteria | Description of Criteria | Proxy |
|---|---|---|
| Credibility | Internal validity of participation: Do participants feel that the findings represent their experience? | Was there a prolonged engagement with participants? Was there a debriefing session with the participants? |
| Transferability | External validity of participation: are the findings applicable to other contexts? | Are participants’ responses in harmony with researcher’s experience? Is there scope to provide a detailed description from both sending and receiving ends? |
| Dependability | Reliability in participation: are the findings consistent? | Can the researcher use documents and methods to check if research strategies have effect? |
| Confirmability | Can we confirm the findings using data analysis? | Can the findings be confirmed if data are recollected and analyzed? |
| Authenticity | Integrity of participation: are all the different views fairly represented? Did the process stimulate action from participants? | Were viewpoints from different participants considered? Did the participatory process lead to participants acting on HIA outcomes? |
| Activity | Item | Number of Items | Price Per Item | Total MUR | Total EUR | Working Days |
|---|---|---|---|---|---|---|
| Survey Data Collection | Fieldworker (FW) salary | 8 | 12,000 rps/FW | 96,000 | 2412 | 20 |
| Bus trips for FW | 320 | 25 rps/trip | 8000 | 201 | ||
| Weekend bonus | 8 | 1000 rps/wkend | 8000 | 201 | 4 | |
| Software and hosting | One-off fee | 24,000 rps | 24,000 | 603 | ||
| Intern Support | Intern support (1) | 20 hrs | 20 hrs | 1875 | 47 * | 4 |
| Intern support (2) | 20 hrs | 20 hrs | 1500 | 38 * | 4 | |
| FGD | Room location | 2hrs | 750 | 1500 | 38 * | 1 |
| Facilitation strategy | 3 hrs | 1000 | 3000 | 75 * | 1 | |
| Secondary data | Heat data | 5 | 200 rps | 1000 | 25 | 10 |
| Cartography Layers | 4 | 4000 | 16,000 | 402 | ||
| Transport | 40 hrs | 100 rps/hr | 4000 | 101 * | ||
| Outline Planning Scheme | 1 | 5000 | 126 | |||
| Total | 4268 EUR | 44 days |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thondoo, M.; De Vries, D.H.; Rojas-Rueda, D.; Ramkalam, Y.D.; Verlinghieri, E.; Gupta, J.; Nieuwenhuijsen, M.J. Framework for Participatory Quantitative Health Impact Assessment in Low- and Middle-Income Countries. Int. J. Environ. Res. Public Health 2020, 17, 7688. https://doi.org/10.3390/ijerph17207688
Thondoo M, De Vries DH, Rojas-Rueda D, Ramkalam YD, Verlinghieri E, Gupta J, Nieuwenhuijsen MJ. Framework for Participatory Quantitative Health Impact Assessment in Low- and Middle-Income Countries. International Journal of Environmental Research and Public Health. 2020; 17(20):7688. https://doi.org/10.3390/ijerph17207688
Chicago/Turabian StyleThondoo, Meelan, Daniel H. De Vries, David Rojas-Rueda, Yashila D. Ramkalam, Ersilia Verlinghieri, Joyeeta Gupta, and Mark J. Nieuwenhuijsen. 2020. "Framework for Participatory Quantitative Health Impact Assessment in Low- and Middle-Income Countries" International Journal of Environmental Research and Public Health 17, no. 20: 7688. https://doi.org/10.3390/ijerph17207688