Maternal Dietary Patterns during Pregnancy and Their Association with Gestational Weight Gain and Nutrient Adequacy

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Methods
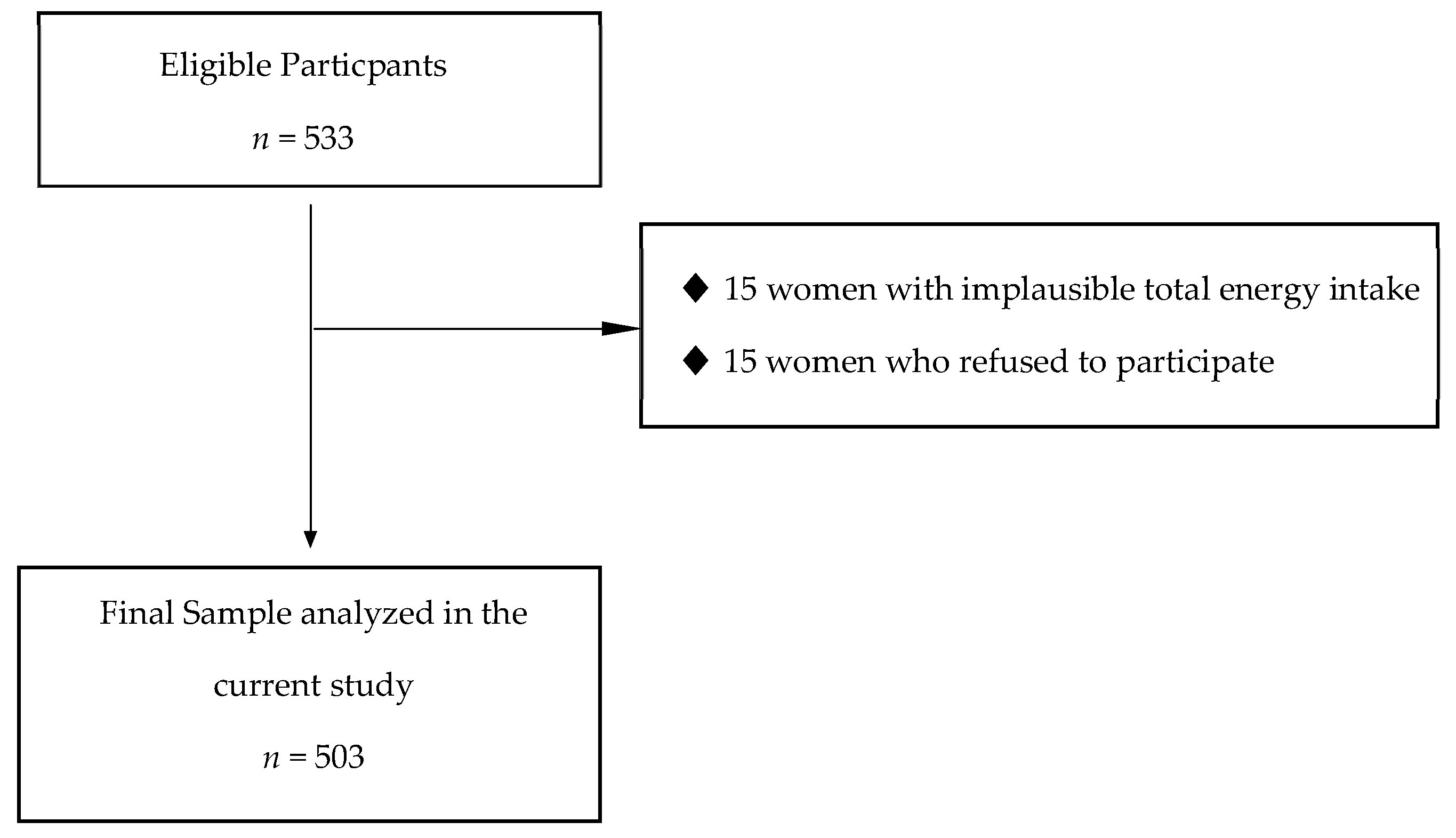
2.1. Study Design, Settings, and Participants
2.2. Data Collection and Outcomes
2.2.1. Dietary Assessment
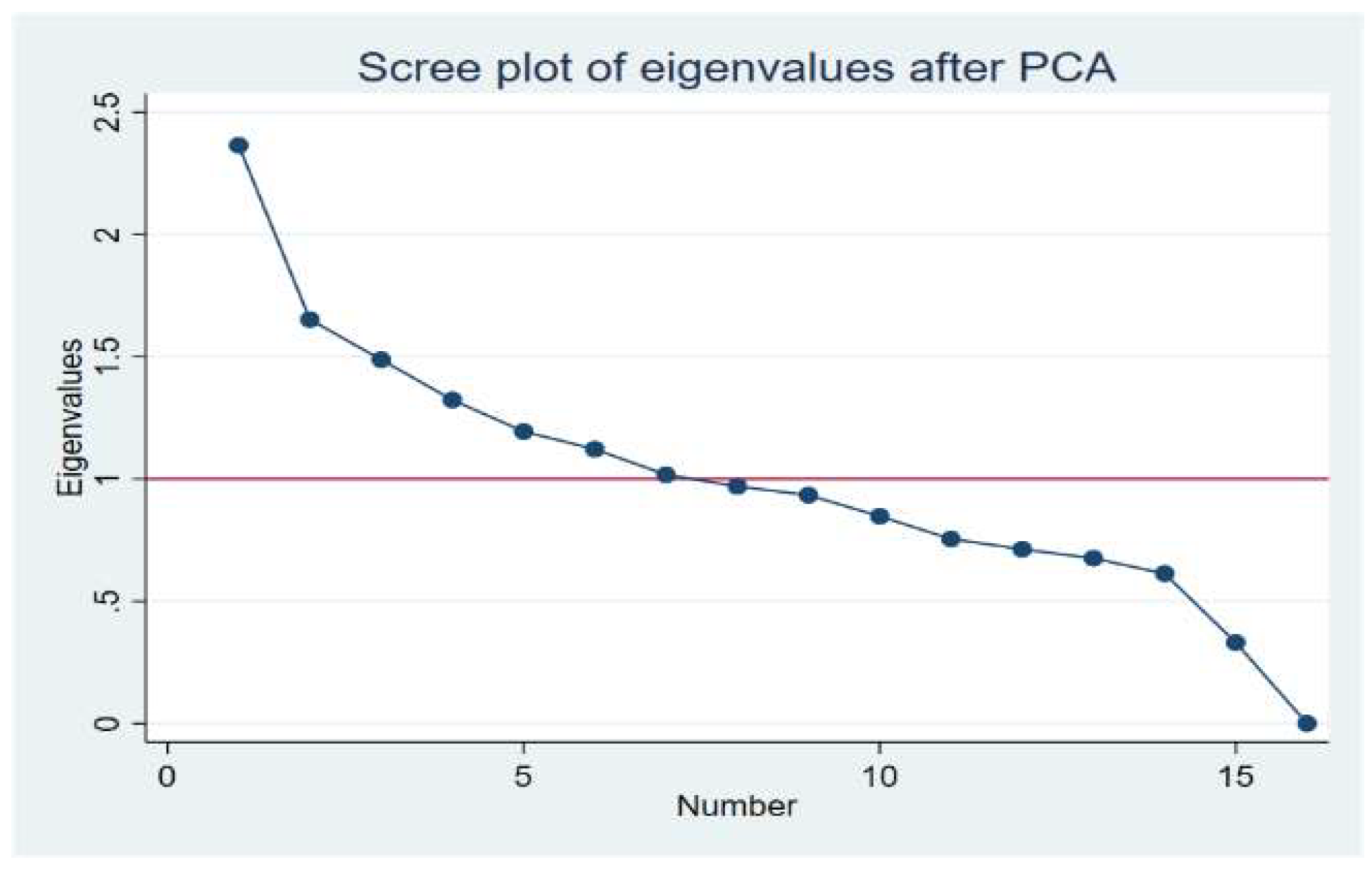
2.2.2. Dietary Pattern Construction
2.2.3. Anthropometry
2.2.4. Diet Quality: Nutrient Adequate Intake
2.2.5. Other Maternal Variables Related to Patient Characteristics
2.3. Statistical Analysis
3. Results
3.1. Characteristic of the Study Population
3.2. Dietary Patterns and GWG
3.3. Prevalence of Participants with Adequate, Deficient, or Excessive Nutrient Intake According to GWG
3.4. Association between Maternal Dietary Patterns and Nutrient Adequate Intake According to GWG
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Guelinckx, I.; Devlieger, R.; Beckers, K.; Vansant, G. Maternal obesity: Pregnancy complications, gestational weight gain and nutrition. Obes. Rev. 2008, 9, 140–150. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine and National Research Council Committee to Reexamine IOMPWG. The National Academies Collection: Reports funded by National Institutes of Health. In Weight Gain During Pregnancy: Reexamining the Guidelines; Rasmussen, K.M., Yaktine, A.L., Eds.; National Academies Press (US) National Academy of Sciences: Washington, DC, USA, 2009. [Google Scholar]
- Goldstein, R.F.; Abell, S.K.; Ranasinha, S.; Misso, M.; Boyle, J.A.; Black, M.H.; Li, N.; Hu, G.; Corrado, F.; Rode, L.; et al. Association of gestational weight gain with maternal and infant outcomes: A systematic review and meta-analysis. JAMA 2017, 317, 2207–2225. [Google Scholar] [CrossRef] [PubMed]
- Herring, S.J.; Rose, M.Z.; Skouteris, H.; Oken, E. Optimizing weight gain in pregnancy to prevent obesity in women and children. Diabetes Obes. Metab. 2012, 14, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Su, W.J.; Chen, Y.L.; Huang, P.Y.; Shi, X.L.; Yan, F.F.; Chen, Z.; Yan, B.; Song, H.-Q.; Lin, M.-Z.; Li, X.-J. Effects of Prepregnancy Body Mass Index, Weight Gain, and Gestational Diabetes Mellitus on Pregnancy Outcomes: A Population-Based Study in Xiamen, China, 2011–2018. Ann. Nutr. Metab. 2019, 75, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Gilmore, L.A.; Klempel-Donchenko, M.; Redman, L.M. Pregnancy as a window to future health: Excessive gestational weight gain and obesity. Semin. Perinatol. 2015, 39, 296–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guan, P.; Tang, F.; Sun, G.; Ren, W. Effect of maternal weight gain according to the Institute of Medicine recommendations on pregnancy outcomes in a Chinese population. J. Int. Med Res. 2019, 47, 4397–4412. [Google Scholar] [CrossRef] [PubMed]
- Tovar, A.; Kaar, J.L.; McCurdy, K.; Field, A.E.; Dabelea, D.; Vadiveloo, M. Maternal vegetable intake during and after pregnancy. BMC Pregnancy Childbirth 2019, 19, 267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, J.S.; Soh, S.E.; Loy, S.L.; Colega, M.; Kramer, M.S.; Chan, J.K.Y.; Tan, T.C.; Shek, L.P.C.; Yap, F.K.P.; Tan, K.H. Macronutrient composition and food groups associated with gestational weight gain: The GUSTO study. Eur. J. Nutr. 2019, 58, 1081–1094. [Google Scholar] [CrossRef] [PubMed]
- Tebbani, F.; Oulamara, H.; Agli, A. Factors associated with low maternal weight gain during pregnancy. Revue d’Epidemiologie et de Sante Publique 2019, 67, 253–260. [Google Scholar] [CrossRef]
- Campos, C.A.S.; Malta, M.B.; Neves, P.A.R.; Lourenço, B.H.; Castro, M.C.; Cardoso, M.A. Gestational weight gain, nutritional status and blood pressure in pregnant women. Revista de Saude Publica 2019, 53, 57. [Google Scholar] [CrossRef]
- Gernand, A.D.; Schulze, K.J.; Stewart, C.P.; West, K.P.; Christian, P. Micronutrient deficiencies in pregnancy worldwide: Health effects and prevention. Nat. Rev. Endocrinol. 2016, 12, 274–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Black, R.E. Micronutrients in pregnancy. Br. J. Nutr. 2001, 85 (Suppl. S2), S193–S197. [Google Scholar] [CrossRef] [Green Version]
- Cano-Ibáñez, N.; Martínez-Galiano, J.M.; Amezcua-Prieto, C.; Olmedo-Requena, R.; Bueno-Cavanillas, A.; Delgado-Rodríguez, M. Maternal dietary diversity and risk of small for gestational age newborn: Findings from a case–control study. Clin. Nutr. 2019, 39, 1943–1950. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; Martín-Calvo, N. The major European dietary patterns and metabolic syndrome. Rev. Endocr. Metab. Disord. 2013, 14, 265–271. [Google Scholar] [CrossRef]
- Plante, A.S.; Lemieux, S.; Labrecque, M.; Morisset, A.S. Relationship Between Psychosocial Factors, Dietary Intake and Gestational Weight Gain: A Narrative Review. J. Obstet. Gynaecol. Can. 2019, 41, 495–504. [Google Scholar] [CrossRef] [PubMed]
- Willet, W. Nutritional Epidemiology, 3rd ed.; Oxford University Press: New York, NY, USA, 2013. [Google Scholar]
- Martin-Moreno, J.M.; Boyle, P.; Gorgojo, L.; Maisonneuve, P.; Fernandez-Rodriguez, J.C.; Salvini, S.; Willett, W.C. Development and validation of a food frequency questionnaire in Spain. Int. J. Epidemiol. 1993, 22, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Ballarth, J.; Pinol, J.; Zazpe, I.; Corella, D.; Carrasco, P.; Toledo, E.; Perez-Bauer, M.; Martinez-Gonzalez, M.; Salas-Salvado, J.; Martin-Moreno, J. Relative validity of a semi-quantitative food-frequency questionnaire in an elderly Mediterranean population of Spain. Br. J. Nutr. 2010, 103, 1808–1816. [Google Scholar] [CrossRef] [Green Version]
- Moreiras, O.C.A.; Cabrera, L.; Cuadrado, C. Tablas de Composición de Alimentos. (Spanish Food Composition Tables); Pirámide: Madrid, Spain, 2003. [Google Scholar]
- Mataix, J.; Manas, M.; Llopis, J.; Martínez de Victoria, E.; Juan, J.; Borregón, A. Tabla de Composición de Alimentos Españoles. (Spanish Food Composition Tables); Universidad de Granada: Granada, Spain, 2003. [Google Scholar]
- Willett, W.; Stampfer, M. Implications of Total Energy Intake for Epidemiologic Analyses. In Nutritional Epidemiology; Oxford University Press: New York, NY, USA, 2009. [Google Scholar]
- Hu, F.B.; Rimm, E.; A Smith-Warner, S.; Feskanich, D.; Stampfer, M.J.; Ascherio, A.; Sampson, L.; Willett, W.C. Reproducibility and validity of dietary patterns assessed with a food- frequency questionnaire. Am. J. Clin. Nutr. 1999, 69, 243–249. [Google Scholar] [CrossRef] [Green Version]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef]
- Wei, X.; He, J.-R.; Lin, Y.; Lu, M.; Zhou, Q.; Li, S.; Lu, J.; Yuan, M.; Chen, N.; Zhang, L.; et al. The influence of maternal dietary patterns on gestational weight gain: A large prospective cohort study in China. Nutrition 2019, 59, 90–95. [Google Scholar] [CrossRef]
- EFSA. Dietary Reference Values and Dietary Guidelines. 2018. Available online: https://www.efsa.europa.eu/en/topics/topic/dietary-reference-values (accessed on 10 June 2019).
- Aranceta-Bartrina, J.; Serra-Majem, L.; Pérez-Rodrigo, C.; Llopis, J.; Mataix, J.; Ribas, L.; Tojo, R.; Tur, J.A. Vitamins in Spanish food patterns: The eVe study. Public Health Nutr. 2001, 4, 1317–1323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Álvarez-Dardet, C.A.J.; Domingo, A.; Regidor, E. La Medicina de la Clase Social en Ciencias de la Salud, Informe de un Grupo de Trabajo de la Sociedad Española de Epidemiología; SG Editores: Barcelona, Spain, 1995. [Google Scholar]
- Black, D.T.P. Inequalities in Health; Penguin: Harmondsworth, UK, 1983. [Google Scholar]
- Kessner, D.M.S.J.; Kalk, C.E.; Schlesinger, E.R. Infant Death: An Analysis by Maternal Risk and Health Care, Contrasts in Health Status; Institute of Medicine and National Academy of Sciences: Washington, DC, USA, 1973. [Google Scholar]
- Tielemans, M.J.; Garcia, A.H.; Santos, A.P.; Bramer, W.M.; Luksa, N.; Luvizotto, M.J.; Moreira, E.; Topi, G.; Jonge, E.A.L.D.; Visser, T.L.; et al. Macronutrient composition and gestational weight gain: A systematic review. Am. J. Clin. Nutr. 2016, 103, 83–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaiser, L.; Allen, L.H. Position of the American Dietetic Association: Nutrition and lifestyle for a healthy pregnancy outcome. J. Am. Diet. Assoc. 2008, 108, 553–561. [Google Scholar]
- Al Wattar, B.H.; Dodds, J.; Placzek, A.; Beresford, L.; Spyreli, E.; Moore, A.; Carreras, F.J.G.; Austin, F.; Murugesu, N.; Roseboom, T.J.; et al. Mediterranean-style diet in pregnant women with metabolic risk factors (ESTEEM): A pragmatic multicentre randomised trial. PLoS Med. 2019, 16, e1002857. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Hao, T.; Rimm, E.B.; Willett, W.C.; Hu, F.B. Changes in diet and lifestyle and long-term weight gain in women and men. New Engl. J. Med. 2011, 364, 2392–2404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wrottesley, S.V.; Pisa, P.T.; Norris, S.A. The influence of maternal dietary patterns on body mass index and gestational weight gain in urban black South African women. Nutrients 2017, 9, 732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maugeri, A.; Barchitta, M.; Favara, G.; La Rosa, M.C.; La Mastra, C.; Lio, R.M.S.; Agodi, A. Maternal dietary patterns are associated with pre-pregnancy body mass index and gestational weight gain: Results from the “mamma & bambino” cohort. Nutrients 2019, 11, 1308. [Google Scholar]
- Yang, J.; Cheng, Y.; Pei, L.; Jiang, Y.; Lei, F.; Zeng, L.; Wang, Q.; Li, Q.; Kang, Y.; Shen, Y.; et al. Maternal iron intake during pregnancy and birth outcomes: A cross-sectional study in Northwest China. Br. J. Nutr. 2017, 117, 862–871. [Google Scholar] [CrossRef] [Green Version]
- Simpson, J.L.; Bailey, L.B.; Pietrzik, K.; Shane, B.; Holzgreve, W. Micronutrients and women of reproductive potential: Required dietary intake and consequences of dietary deficiency or excess. Part i Folate, Vitamin B12, Vitamin B6. J. Matern. Fetal Neonatal Med. 2010, 23, 1323–1343. [Google Scholar] [CrossRef]
- Haider, B.A.; Yakoob, M.Y.; Bhutta, Z.A. Effect of multiple micronutrient supplementation during pregnancy on maternal and birth outcomes. BMC Public Health 2011, 11 (Suppl. S3), S19. [Google Scholar] [CrossRef] [Green Version]
- Cano-Ibáñez, N.; Gea, A.; Martínez-González, M.A.; Salas-Salvadó, J.; Corella, D.; Zomeño, M.D.; Romaguera, D.; Vioque, J.; Aros, F.; Wärnberg, J.; et al. Dietary diversity and nutritional adequacy among an older Spanish population with metabolic syndrome in the PREDIMED-plus study: A cross-sectional analysis. Nutrients 2019, 11, 958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trichopoulou, A.; Martínez-González, M.A.; Tong, T.Y.; Forouhi, N.G.; Khandelwal, S.; Prabhakaran, D.; Mozaffarian, D.; De Lorgeril, M. Definitions and potential health benefits of the Mediterranean diet: Views from experts around the world. BMC Med. 2014, 12, 112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fung, T.T.; Willett, W.C.; Stampfer, M.J.; Manson, J.E.; Hu, F.B. Dietary patterns and the risk of coronary heart disease in women. Arch. Intern. Med. 2001, 161, 1857–1862. [Google Scholar] [CrossRef] [Green Version]
- Serra-Majem, L.; Bes-Rastrollo, M.; Román-Viñas, B.; Pfrimer, K.; Sánchez-Villegas, A.; Martínez-González, M.A. Dietary patterns and nutritional adequacy in a Mediterranean country. Br. J. Nutr. 2009, 101, S21–S28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phillips, S.M.; Fulgoni, V.L.; Heaney, R.P.; Nicklas, T.A.; Slavin, J.L.; Weaver, C.M. Commonly consumed protein foods contribute to nutrient intake, diet quality, and nutrient adequacy. Am. J. Clin. Nutr. 2015, 101, 1346S–1352S. [Google Scholar] [CrossRef] [Green Version]
- Cano-Ibáñez, N.; Bueno-Cavanillas, A.; Martínez-González, M.Á.; Salas-Salvadó, J.; Corella, D.; Freixer, G.-L.; Romaguera, D.; Vioque, J.; Alonso-Gómez, Á.M.; Wärnberg, J.; et al. Effect of changes in adherence to Mediterranean diet on nutrient density after 1-year of follow-up: Results from the PREDIMED-Plus Study. Eur. J. Nutr. 2019, 59, 2395–2409. [Google Scholar]
- Crozier, S.R.; Robinson, S.M.; Godfrey, K.M.; Cooper, C.; Inskip, H.M. Women’s dietary patterns change little from before to during pregnancy. J. Nutr. 2009, 139, 1956–1963. [Google Scholar] [CrossRef]
- Martínez-Galiano, J.M.; Amezcua-Prieto, C.; Salcedo-Bellido, I.; Olmedo-Requena, R.; Bueno-Cavanillas, A.; Delgado-Rodriguez, M. Alcohol consumption during pregnancy and risk of small-for-gestational-age newborn. Women Birth 2019, 32, 284–288. [Google Scholar] [CrossRef]
- Rifas-Shiman, S.L.; Rich-Edwards, J.W.; Kleinman, K.P.; Oken, E.; Gillman, M.W. Dietary Quality during Pregnancy Varies by Maternal Characteristics in Project Viva: A US Cohort. J. Am. Diet. Assoc. 2009, 109, 1004–1011. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Food Groups | Food Subgroups |
|---|---|
| Vegetables | (1) Green leafy vegetables: spinach, cruciferous, lettuce, green beans, eggplant, peppers, and asparagus; (2) Orange and yellow vegetables: tomatoes, carrots, and pumpkin; (3) Mushrooms. |
| Fruits | Dried fruit, canned fruit, and fresh fruit |
| Dairy Products | (1) Milk: low fat and high fat; (2) Yogurt: low fat and high fat; (3) Cheese: low fat and high fat. |
| Whole Cereals | Whole grain: bread, pasta, rice, and whole breakfast cereals |
| Refined Cereals | Refined grain: bread, pasta, and rice |
| Meat | (1) Red meats: beef, lamb, and organ meats; (2) White meats: poultry and rabbit. |
| Meat products | Hamburger, sausages, and other processed meats |
| Fish | White fish, oily fish, canned fish, and shellfish/seafood |
| Sweets and desserts | Biscuits, cakes, and cookies |
| Olive oil | Olive oil |
| Hydrogenated oil | Butter, margarine, and solid oil |
| Potatoes | Cooked and fried potato |
| Legumes | Peas, beans, lentils, and chickpeas |
| Nuts | Almonds, nuts, pistachios, and other nuts |
| Eggs | Eggs |
| Ready-mademeals | Pizza, soup, lasagna, meatballs, sauces, and other ready-made meals |
| Foods/Food Groups | Occidental Dietary Pattern | Mediterranean Dietary Pattern |
|---|---|---|
| Meat | −0.147 | 0.237 |
| Meat products | 0.416 | 0.376 |
| Fish | −0.352 | 0.263 |
| Dairy Products | −0.075 | 0.063 |
| Vegetables | −0.309 | 0.740 |
| Whole Cereals | −0.183 | 0.504 |
| Refined Cereals | 0.054 | −0.618 |
| Fruits | −0.373 | 0.043 |
| Nuts | −0.059 | 0.323 |
| Legumes | −0.050 | 0.224 |
| Potatoes | 0.342 | 0.319 |
| Olive oil | −0.005 | 0.315 |
| Sweets and desserts | 0.401 | −0.128 |
| Hydrogenated oil | 0.314 | −0.092 |
| Eggs | 0.096 | 0.032 |
| Ready-made meals | 0.373 | 0.207 |
| Reduced GWG | Adequate GWG | Excessive GWG | p-Value | ||||
|---|---|---|---|---|---|---|---|
| n = 170 | n = 205 | n = 128 | |||||
| Age in years, mean (SD) | 31.6 | (5.5) | 31.9 | (5.3) | 31.0 | (4.8) | 0.076 |
| Pre-pregnancy BMI, mean (SD) | 23.3 | (3.9) | 23.6 | (4.0) | 25.5 | (4.2) | <0.001 |
| Pre-pregnancy BMI, n (%) | <0.001 | ||||||
| Underweight (<18.5 Kg/m2) | 19 | (11.2) | 31 | (15.1) | 11 | (8.6) | |
| Normal weight (18.5–24.9 Kg/m2) | 121 | (71.2) | 120 | (58.5) | 47 | (36.7) | |
| Overweight (25–29.9 Kg/m2) | 22 | (12.9) | 40 | (19.5) | 52 | (40.6) | |
| Obesity (≥30 Kg/m2) | 8 | (4.7) | 14 | (6.8) | 18 | (14.1) | |
| GWG (kg), mean (SD) | 8.2 | (2.9) | 12.5 | (2.5) | 17.3 | (3.6) | <0.001 |
| Birth weight (g), mean (SD) | 3310.5 | (379.1) | 3436.5 | (384.8) | 3465.2 | (341.7) | <0.001 |
| Length of gestation (weeks), mean (SD) | 39.4 | (1.2) | 39.5 | (1.2) | 39.8 | (1.2) | 0.013 |
| Marital status, n (%) | 0.312 | ||||||
| Singled, never married | 15 | (8.8) | 11 | (5.4) | 14 | (10.9) | |
| Married | 115 | (67.7) | 147 | (71.7) | 80 | (62.5) | |
| Couple | 40 | (23.5) | 47 | (22.9) | 34 | (26.6) | |
| Educational level, n (%) | 0.173 | ||||||
| Primary | 31 | (18.2) | 33 | (16.1) | 26 | (20.3) | |
| Secondary (unfinished) | 10 | (5.9) | 12 | (5.9) | 4 | (3.1) | |
| Secondary (completed) | 50 | (29.4) | 81 | (39.5) | 54 | (42.2) | |
| University | 79 | (46.5) | 79 | (38.5) | 44 | (34.4) | |
| Smoking during pregnancy, n (%) | 14 | (8.2) | 35 | (17.1) | 29 | (22.7) | 0.002 |
| Kessner index (prenatal care), n (%) | 0.396 | ||||||
| Adequate | 80 | (47.1) | 95 | (46.3) | 71 | (55.5) | |
| Intermediate | 66 | (38.9) | 74 | (36.1) | 38 | (29.7) | |
| Inadequate | 24 | (14.1) | 36 | (17.6) | 19 | (14.8) | |
| Dietary Pattern | GWG | |||
|---|---|---|---|---|
| Crude β-Coefficients | (95% CI) | Adjusted β-Coefficients a | (95% CI) | |
| Occidental dietary pattern | 0.02 | (−0.05, 0.04) | 0.08 | (−0.04, 0.05) |
| Mediterranean dietary pattern | −0.06 | (−0.11, −0.04) | −0.05 | (−0.01, 0.01) |
|
Reduced GWG |
Adequate GWG |
Excessive GWG | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Nutrient | n = 170 | n = 205 | n = 128 | |||||||
| DI a | AI b | EI c | DI a | AI b | EI c | DI a | AI b | EI c | p-Value | |
| Dietary fiber (g/day) | 6.0 | 94.1 | - | 9.3 | 90.7 | - | 9.4 | 90.6 | - | 0.413 |
| Vitamin A (µg/day) | 0 | 58.2 | 41.8 | 0.5 | 59.5 | 40.0 | 0.8 | 62.5 | 36.7 | 0.756 |
| Vitamin B9 (µg/day) | 45.3 | 50.0 | 4.7 | 58.0 | 41.0 | 1.0 | 54.7 | 40.6 | 4.7 | 0.034 |
| Vitamin B12 (µg/day) | 0 | 100.0 | - | 0.5 | 99.5 | - | 1.6 | 98.4 | - | 0.215 |
| Vitamin D (µg/day) | 82.4 | 17.7 | 0 | 89.8 | 10.2 | 0 | 80.5 | 19.5 | 0 | 0.037 |
| Vitamin E (mg/day) | 5.9 | 94.1 | 0 | 2.9 | 97.1 | 0 | 3.1 | 96.9 | 0 | 0.293 |
| Calcium (mg/day) | 0.6 | 87.1 | 12.4 | 0.5 | 88.8 | 10.7 | 0.8 | 82.8 | 16.4 | 0.651 |
| Magnesium (mg/day) | 0 | 0 | 100.0 | 0 | 0 | 100.0 | 0 | 0 | 100.0 | - |
| Iodine (µg/day) | 9.4 | 60.6 | 30.0 | 7.8 | 53.7 | 38.5 | 10.9 | 50.0 | 39.1 | 0.299 |
| Potassium (mg/day) | 0.6 | 99.4 | - | 0 | 100.0 | - | 1.6 | 98.4 | - | 0.197 |
| Selenium (µg/day) | 1.2 | 98.8 | 0 | 1.5 | 98.5 | 0 | 3.1 | 96.1 | 0.8 | 0.314 |
| Reduced GWG OR (95% CI) | Adequate GWG OR (95% CI) | Excessive GWG OR (95% CI) | |
|---|---|---|---|
| Dietary fiber | |||
| Occidental dietary pattern | 0.8 (0.42, 1.35) | 0.6 (0.39, 1.03) | 0.4 (0.15, 1.86) |
| Mediterranean dietary pattern | 3.1 (1.37, 7.07) | 1.6 (0.96, 2.59) | 1.4 (0.72, 2.57) |
| Vitamin A | |||
| Occidental dietary pattern | 0.9 (0.67, 1.10) | 0.7 (0.54, 0.87) | 0.6 (0.44, 0.82) |
| Mediterranean dietary pattern | 1.1 (0.80, 1.36) | 1.2 (0.94, 1.51) | 1.1 (0.78, 1.43) |
| Vitamin B9 | |||
| Occidental dietary pattern | 0.5 (0.44, 0.81) | 0.6 (0.44, 0.77) | 0.8 (0.56, 1.08) |
| Mediterranean dietary pattern | 1.6 (1.22, 2.21) | 2.1 (1.56, 2.79) | 1.7 (1.26, 2.36) |
| Vitamin D | |||
| Occidental dietary pattern | 0.5 (0.32, 0.87) | 0.74 (0.46, 1.19) | 0.91 (0.61, 1.38) |
| Mediterranean dietary pattern | 4.4 (2.50, 7.68) | 4.89 (2.72, 8.77) | 3.02 (1.84, 4.96) |
| Vitamin E | |||
| Occidental dietary pattern | 1.06 (0.62, 1.82) | 1.1 (0.54, 2.06) | 1.00 (0.40, 2.51) |
| Mediterranean dietary pattern | 2.7 (1.26, 5.72) | 1.26 (0.64, 2.50) | 2.75 (0.90, 8.34) |
| Calcium | |||
| Occidental dietary pattern | 0.8 (0.56, 1.09) | 0.8 (0.59, 1.15) | 0.82 (0.65, 1.04) |
| Mediterranean dietary pattern | 1.4 (0.92, 2.13) | 1.20 (0.85, 1.70) | 1.15 (0.80, 1.67) |
| Iodine | |||
| Occidental dietary pattern | 0.8 (0.65, 1.12) | 1.2 (0.93, 1.48) | 1.0 (0.78, 1.35) |
| Mediterranean dietary pattern | 1.3 (0.97, 1.68) | 1.3 (1.02, 1.63) | 1.1 (0.91, 1.43) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cano-Ibáñez, N.; Martínez-Galiano, J.M.; Luque-Fernández, M.A.; Martín-Peláez, S.; Bueno-Cavanillas, A.; Delgado-Rodríguez, M. Maternal Dietary Patterns during Pregnancy and Their Association with Gestational Weight Gain and Nutrient Adequacy. Int. J. Environ. Res. Public Health 2020, 17, 7908. https://doi.org/10.3390/ijerph17217908
Cano-Ibáñez N, Martínez-Galiano JM, Luque-Fernández MA, Martín-Peláez S, Bueno-Cavanillas A, Delgado-Rodríguez M. Maternal Dietary Patterns during Pregnancy and Their Association with Gestational Weight Gain and Nutrient Adequacy. International Journal of Environmental Research and Public Health. 2020; 17(21):7908. https://doi.org/10.3390/ijerph17217908
Chicago/Turabian StyleCano-Ibáñez, Naomi, Juan Miguel Martínez-Galiano, Miguel Angel Luque-Fernández, Sandra Martín-Peláez, Aurora Bueno-Cavanillas, and Miguel Delgado-Rodríguez. 2020. "Maternal Dietary Patterns during Pregnancy and Their Association with Gestational Weight Gain and Nutrient Adequacy" International Journal of Environmental Research and Public Health 17, no. 21: 7908. https://doi.org/10.3390/ijerph17217908