Towards the Development of an Intervention to Address Social Determinants of Non-Communicable Disease in Kerala, India: A Mixed Methods Study

 ,
,  , , and
, , and
Abstract
:1. Introduction
1.1. Non-Communicable Disease in India
1.2. Complexity of Social Determinants of NCDs
1.3. Social Intervention Design Considerations
1.4. Literature Review
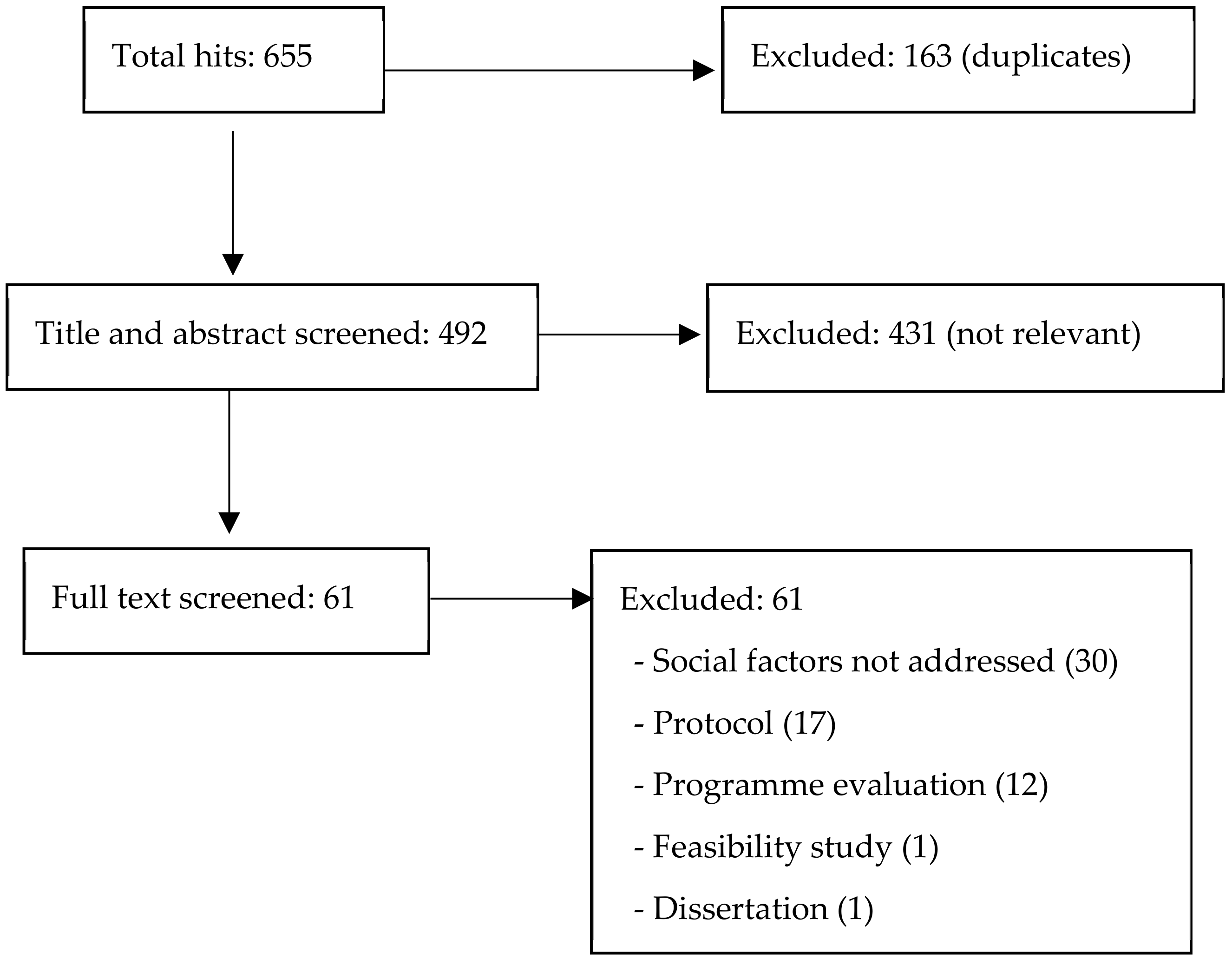
- Studies that examined effectiveness of social interventions that targeted social risk factors of Diabetes, hypertension and CVD;
- Randomised controlled trials;
- Conducted in India;
- Population aged over 30 years;
- Peer-reviewed journal articles;
- Written in English language.
2. Materials and Methods
2.1. Design
2.2. Qualitative Interviews
2.2.1. Community Members
2.2.2. Health Practitioners and ASHAs
2.3. Expert Workshop
2.4. Ethical Approval
3. Results
3.1. Qualitative Interviews
3.1.1. Community Members
3.1.2. Health Practitioners and ASHAs
3.2. Stakeholder Workshop
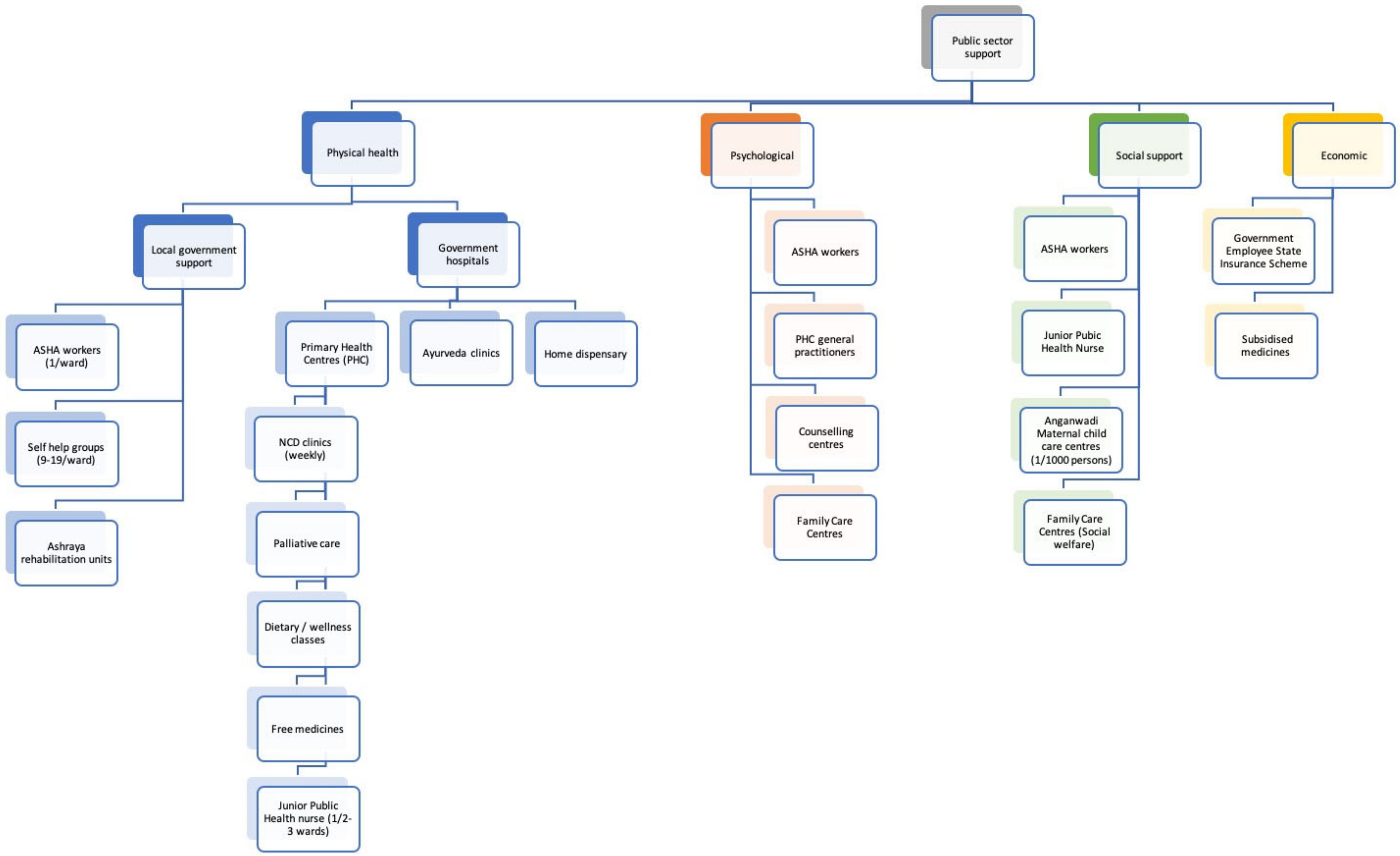
3.3. Mapping Resources in the Community
- Health: religious organisations provide nursing care services for older people, home care for those unable to reach health facilities, postnatal maternal and infant care; NGO’s provide regular medical camps, community-based palliative care and free medications based on need.
- Psychological and social support: at the community level, friends, neighbours and family members provide much social support.
- Economic: private organizations provide medication, medical kits, and a monetary support to the caregivers of people who require home assistance. Financial support is also provided to some in need through religious organisations.
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

References
- Moore, S.; Carpiano, R.M. Introduction to the special issue on “social capital and health: What have we learned in the last 20 Years and where do we go from here?”. Soc. Sci. Med. 2020, 257, 113014. [Google Scholar] [CrossRef] [PubMed]
- Shiell, A.; Hawe, P.; Kavanagh, S. Evidence suggests a need to rethink social capital and social capital interventions. Soc. Sci. Med. 2020, 257, 111930. [Google Scholar] [CrossRef] [PubMed]
- Prabhakaran, D.; Jeemon, P.; Sharma, M.; Roth, G.A.; Johnson, C.; Harikrishnan, S.; Gupta, R.; Pandian, J.D.; Naik, N.; Roy, A.; et al. The changing patterns of cardiovascular diseases and their risk factors in the states of India: The Global Burden of Disease Study 1990–2016. Lancet Glob. Health 2018, 6, e1339–e1351. [Google Scholar] [CrossRef] [Green Version]
- Reddy, M.M.; Kar, S.S. Unconditional probability of dying and age-specific mortality rate because of major non-communicable diseases in India: Time trends from 2001 to 2013. J. Postgrad. Med. 2019, 65, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Anchala, R.; Kannuri, N.K.; Pant, H.; Khan, H.; Franco, O.H.; Di Angelantonio, E.; Prabhakaran, D. Hypertension in India: A systematic review and meta-analysis of prevalence, awareness, and control of hypertension. J. Hypertens. 2014, 32, 1170–1177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jose, A.; Prabhakaran, D. World Hypertension Day: Contemporary issues faced in India. Indian J. Med. Res. 2019, 149, 567–570. [Google Scholar] [CrossRef]
- Daivadanam, M.; Absetz, P.; Sathish, T.; Thankappan, K.R.; Fisher, E.B.; Philip, N.E.; Mathews, E.; Oldenburg, B. Lifestyle change in Kerala, India: Needs assessment and planning for a community-based diabetes prevention trial. BMC Public Health 2013, 13, 95. [Google Scholar] [CrossRef] [Green Version]
- Ramakrishnan, S.; Zachariah, G.; Gupta, K.; Shivkumar Rao, J.; Mohanan, P.P.; Venugopal, K.; Sateesh, S.; Sethi, R.; Jain, D.; Bardolei, N.; et al. Prevalence of hypertension among Indian adults: Results from the great India blood pressure survey. Indian Heart J. 2019, 71, 309–313. [Google Scholar] [CrossRef]
- Geldsetzer, P.; Manne-Goehler, J.; Theilmann, M.; Davies, J.I.; Awasthi, A.; Vollmer, S.; Jaacks, L.M.; Bärnighausen, T.; Atun, R. Diabetes and hypertension in India: a nationally representative study of 1.3 million adults. JAMA Intern. Med. 2018, 178, 363–372. [Google Scholar] [CrossRef]
- Thakur, J.; Prinja, S.; Garg, C.; Mendis, S.; Menabde, N. Social and economic implications of noncommunicable diseases in India. Indian J. Community Med. 2011, 36, 13–22. [Google Scholar] [CrossRef]
- Gupta, R.; Xavier, D. Hypertension: The most important non communicable disease risk factor in India. Indian Heart J. 2018, 70, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Dyson, P.A.; Anthony, D.; Fenton, B.; Stevens, D.E.; Champagne, B.; Li, L.-M.; Lv, J.; Ramírez Hernández, J.; Thankappan, K.R.; Matthews, D.R.; et al. Successful up-scaled population interventions to reduce risk factors for non-communicable disease in adults: Results from the international community interventions for health (CIH) project in China, India and Mexico. PLoS ONE 2015, 10, e0120941. [Google Scholar] [CrossRef] [PubMed]
- Madavanakadu Devassy, S.; Benny, A.M.; Scaria, L.; Nannatt, A.; Fendt-Newlin, M.; Joubert, J.; Joubert, L.; Webber, M. Social factors associated with chronic non-communicable disease and comorbidity with mental health problems in India: A scoping review. BMJ Open 2020, 10, e035590. [Google Scholar] [CrossRef] [PubMed]
- Thakur, J.S.; Jeet, G.; Pal, A.; Singh, S.; Singh, A.; Deepti, S.S.; Lal, M.; Gupta, S.; Prasad, R.; Jain, S.; et al. Profile of risk factors for non-communicable diseases in Punjab, Northern India: Results of a state-wide STEPS survey. PLoS ONE 2016, 11, e0157705. [Google Scholar] [CrossRef] [Green Version]
- Sarma, P.S.; Sadanandan, R.; Thulaseedharan, J.V.; Soman, B.; Srinivasan, K.; Varma, R.P.; Nair, M.R.; Pradeepkumar, A.S.; Jeemon, P.; Thankappan, K.R.; et al. Prevalence of risk factors of non-communicable diseases in Kerala, India: Results of a cross-sectional study. BMJ Open 2019, 9, e027880. [Google Scholar] [CrossRef]
- Patra, S.; Bhise, M.D. Gender differentials in prevalence of self-reported non-communicable diseases (NCDs) in India: Evidence from recent NSSO survey. J. Public Health 2016, 24, 375–385. [Google Scholar] [CrossRef]
- Singh, P.K.; Singh, L.; Dubey, R.; Singh, S.; Mehrotra, R. Socioeconomic determinants of chronic health diseases among older Indian adults: A nationally representative cross-sectional multilevel study. BMJ Open 2019, 9, e028426. [Google Scholar] [CrossRef] [Green Version]
- Madavanakadu Devassy, S.; Webber, M.; Scaria, L.; Thiyagarajan, J.A.; Fendt-Newlin, M.; Joubert, J.; Benny, A.M.; Nannatt, A.; Joubert, L. Social and behavioural risk factors in the prevention and management of cardiovascular disease in Kerala, India: A catchment area population survey. BMC Cardiovasc. Disord. 2020, 20, 327. [Google Scholar] [CrossRef]
- Melita, S.; Manjunatha, H.H.; Anice, G. family support and medication nonadherence among elderly on antihypertensives. Indian J. Public Health Res. Dev. 2019, 10, 294–298. [Google Scholar]
- Havranek, E.P.; Mujahid, M.S.; Barr, D.A.; Blair, I.V.; Cohen, M.S.; Cruz-Flores, S.; Davey-Smith, G.; Dennison-Himmelfarb, C.R.; Lauer, M.S.; Lockwood, D.W.; et al. Social determinants of risk and outcomes for cardiovascular disease: A scientific statement from the American heart association. Circulation 2015, 132, 873–898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christakis, N.A.; Fowler, J.H. The spread of obesity in a large social network over 32 years. N. Engl. J. Med. 2007, 357, 370–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strully, K.W.; Fowler, J.H.; Murabito, J.M.; Benjamin, E.J.; Levy, D.; Christakis, N.A. Aspirin use and cardiovascular events in social networks. Soc. Sci. Med. 2012, 74, 1125–1129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawachi, I.; Colditz, G.A.; Ascherio, A.; Rimm, E.B.; Giovannucci, E.; Stampfer, M.J.; Willett, W.C. A prospective study of social networks in relation to total mortality and cardiovascular disease in men in the USA. J. Epidemiol. Community Health 1996, 50, 245–251. [Google Scholar] [CrossRef]
- Basu, S.; Garg, S. The barriers and challenges toward addressing the social and cultural factors influencing diabetes self-management in Indian populations. J. Soc. Health Diabetes 2017, 5, 71–76. [Google Scholar] [CrossRef] [Green Version]
- Lumagbas, L.B.; Coleman, H.L.S.; Bunders, J.; Pariente, A.; Belonje, A.; de Cock Buning, T. Non-communicable diseases in Indian slums: Re-framing the Social Determinants of Health. Glob. Health Action 2018, 11. [Google Scholar] [CrossRef]
- Marmot, M.; Bell, R. Social determinants and non-communicable diseases: Time for integrated action. BMJ 2019, 364, l251. [Google Scholar] [CrossRef] [Green Version]
- Evans, G.W.; Kim, P. Childhood poverty and health: Cumulative risk exposure and stress dysregulation. Psychol. Sci. 2007, 18, 953–957. [Google Scholar] [CrossRef]
- Rosengren, A.; Hawken, S.; Ounpuu, S.; Sliwa, K.; Zubaid, M.; Almahmeed, W.A.; Blackett, K.N.; Sitthi-amorn, C.; Sato, H.; Yusuf, S. Association of psychosocial risk factors with risk of acute myocardial infarction in 11119 cases and 13648 controls from 52 countries (the INTERHEART study): Case-control study. Lancet 2004, 364, 953–962. [Google Scholar] [CrossRef]
- Byrne, M. Increasing the impact of behavior change intervention research: Is there a role for stakeholder engagement? Health Psychol. 2019, 38, 290–296. [Google Scholar] [CrossRef]
- Thankappan, K.; Shah, B.; Mathur, P.; Sarma, P.; Srinivas, G.; Mini, G.; Daivadanam, M.; Soman, B.; Vasan, R.S. Risk factor profile for chronic non-communicable diseases: Results of a community-based study in Kerala, India. Indian J. Med. Res. 2010, 131, 53. [Google Scholar]
- Sathish, T.; Kannan, S.; Sarma, S.P.; Razum, O.; Sauzet, O.; Thankappan, K.R. Seven-year longitudinal change in risk factors for non-communicable diseases in rural Kerala, India: The WHO STEPS approach. PLoS ONE 2017, 12, e0178949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, D.H.; Rao, K.S.; Fryatt, R. Lumping and splitting: The health policy agenda in India. Health Policy Plan. 2003, 18, 249–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oommen, A.M.; Abraham, V.J.; George, K.; Jose, V.J. Prevalence of risk factors for non-communicable diseases in rural & urban Tamil Nadu. Indian J. Med. Res. 2016, 144, 460–471. [Google Scholar] [CrossRef] [PubMed]
- Rothman, A.J.; Simpson, J.A.; Huelsnitz, C.O.; Jones, R.E.; Scholz, U. Integrating intrapersonal and interpersonal processes: A key step in advancing the science of behavior change. Health Psychol. Rev. 2020, 14, 182–187. [Google Scholar] [CrossRef]
- Alcántara, C.; Diaz, S.V.; Cosenzo, L.G.; Loucks, E.B.; Penedo, F.J.; Williams, N.J. Social determinants as moderators of the effectiveness of health behavior change interventions: Scientific gaps and opportunities. Health Psychol. Rev. 2020, 14, 132–144. [Google Scholar] [CrossRef]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [Green Version]
- Wight, D.; Wimbush, E.; Jepson, R.; Doi, L. Six steps in quality intervention development (6SQuID). J. Epidemiol. Community Health 2016, 70, 520–525. [Google Scholar] [CrossRef] [Green Version]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. Br. Med. J. 2008, 337, 979–983. [Google Scholar] [CrossRef] [Green Version]
- Moore, G.F.; Evans, R.E.; Hawkins, J.; Littlecott, H.; Melendez-Torres, G.J.; Bonell, C.; Murphy, S. From complex social interventions to interventions in complex social systems: Future directions and unresolved questions for intervention development and evaluation. Evaluation 2019, 25, 23–45. [Google Scholar] [CrossRef] [Green Version]
- De Silva, M.J.; Breuer, E.; Lee, L.; Asher, L.; Chowdhary, N.; Lund, C.; Patel, V. Theory of change: A theory-driven approach to enhance the medical research council’s framework for complex interventions. Trials 2014, 15, 267. [Google Scholar] [CrossRef] [Green Version]
- Webber, M. From ethnography to randomized controlled trial: An innovative approach to developing complex social interventions. J. Evid. Based Soc. Work 2014, 11, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Eccles, M.; Grimshaw, J.; Walker, A.; Johnston, M.; Pitts, N. Changing the behavior of healthcare professionals: The use of theory in promoting the uptake of research findings. J. Clin. Epidemiol. 2005, 58, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Hawe, P.; Shiell, A.; Riley, T. Theorising interventions as events in systems. Am. J. Community Psychol. 2009, 43, 267–276. [Google Scholar] [CrossRef]
- Vogel, I. Review of the Use of ‘Theory of Change’ in International Development; Department of International Development: London, UK, 2012. [Google Scholar]
- Prestwich, A.; Sniehotta, F.F.; Whittington, C.; Dombrowski, S.U.; Rogers, L.; Michie, S. Does theory influence the effectiveness of health behavior interventions? Meta-analysis. Health Psychol. 2014, 33, 465–474. [Google Scholar] [CrossRef] [PubMed]
- Madavanakadu Devassy, S.; Fendt-Newlin, M.; Joubert, L.; Webber, M. International capacity-building for practice research in India. In The Routledge Handbook of Social Work Practice Research; Joubert, L., Webber, M., Eds.; Routledge: Abingdon, UK, 2020; pp. 276–285. [Google Scholar]
- Attride-Stirling, J. Thematic networks: An analytic tool for qualitative research. Qual. Res. 2001, 1, 385–405. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Lin, N. Social Capital. A Theory of Social Structure and Action; Cambridge University Press: Cambridge, UK, 2001. [Google Scholar]
- De Vries, D.H.; Bruggeman, J.; Benoni, T.E.; Rwemisisi, J.T.; Kashaija, L.M.; Muhangi, D.; Kaawa-Mafigiri, D.; Pool, R. Social networks for health communication in rural Uganda: A mixed-method analysis of Dekabusa Trading Centre, Luwero County. Glob. Public Health 2020, 1–15. [Google Scholar] [CrossRef]
- Arora, M.; Chauhan, K.; John, S.; Mukhopadhyay, A. Multi-sectoral action for addressing social determinants of noncommunicable diseases and mainstreaming health promotion in national health programmes in India. Indian J. Community Med. 2011, 36, S43–S49. [Google Scholar] [CrossRef]
- Coll-Planas, L.; Nyqvist, F.; Puig, T.; Urrútia, G.; Solà, I.; Monteserín, R. Social capital interventions targeting older people and their impact on health: A systematic review. J. Epidemiol. Community Health 2017, 71, 663–672. [Google Scholar] [CrossRef]
- Flôr, C.R.; Baldoni, N.R.; Aquino, J.A.; Baldoni, A.O.; Fabbro, A.L.D.; Figueiredo, R.C.; Oliveira, C.D.L. What is the association between social capital and diabetes mellitus? A systematic review. Diabetes Metab. Syndr. Clin. Res. Rev. 2018, 12, 601–605. [Google Scholar] [CrossRef]
- Fine, B. Theories of Social Capital: Researchers Behaving Badly; Pluto Press: London, UK; New York, NY, USA, 2010. [Google Scholar]
- Szreter, S.; Woolcock, M. Health by association? Social capital, social theory, and the political economy of public health. Int. J. Epidemiol. 2004, 33, 650–667. [Google Scholar] [CrossRef] [PubMed]
- Granovetter, M.S. The strength of weak ties. Am. J. Sociol. 1973, 78, 1360–1380. [Google Scholar] [CrossRef] [Green Version]
- Sorkin, D.; Rook, K.S.; Lu, J.L. Loneliness, lack of emotional support, lack of companionship, and the likelihood of having a heart condition in an elderly sample. Ann. Behav. Med. 2002, 24, 290–298. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.M.; Creedy, D.; Lin, H.-S.; Wollin, J. Effects of motivational interviewing intervention on self-management, psychological and glycemic outcomes in type 2 diabetes: A randomized controlled trial. Int. J. Nurs. Stud. 2012, 49, 637–644. [Google Scholar] [CrossRef]
- Greaves, C.J.; Sheppard, K.E.; Abraham, C.; Hardeman, W.; Roden, M.; Evans, P.H.; Schwarz, P.; The, I.S.G. Systematic review of reviews of intervention components associated with increased effectiveness in dietary and physical activity interventions. BMC Public Health 2011, 11, 119. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Basic Themes | Organising Themes | Global Theme |
|---|---|---|
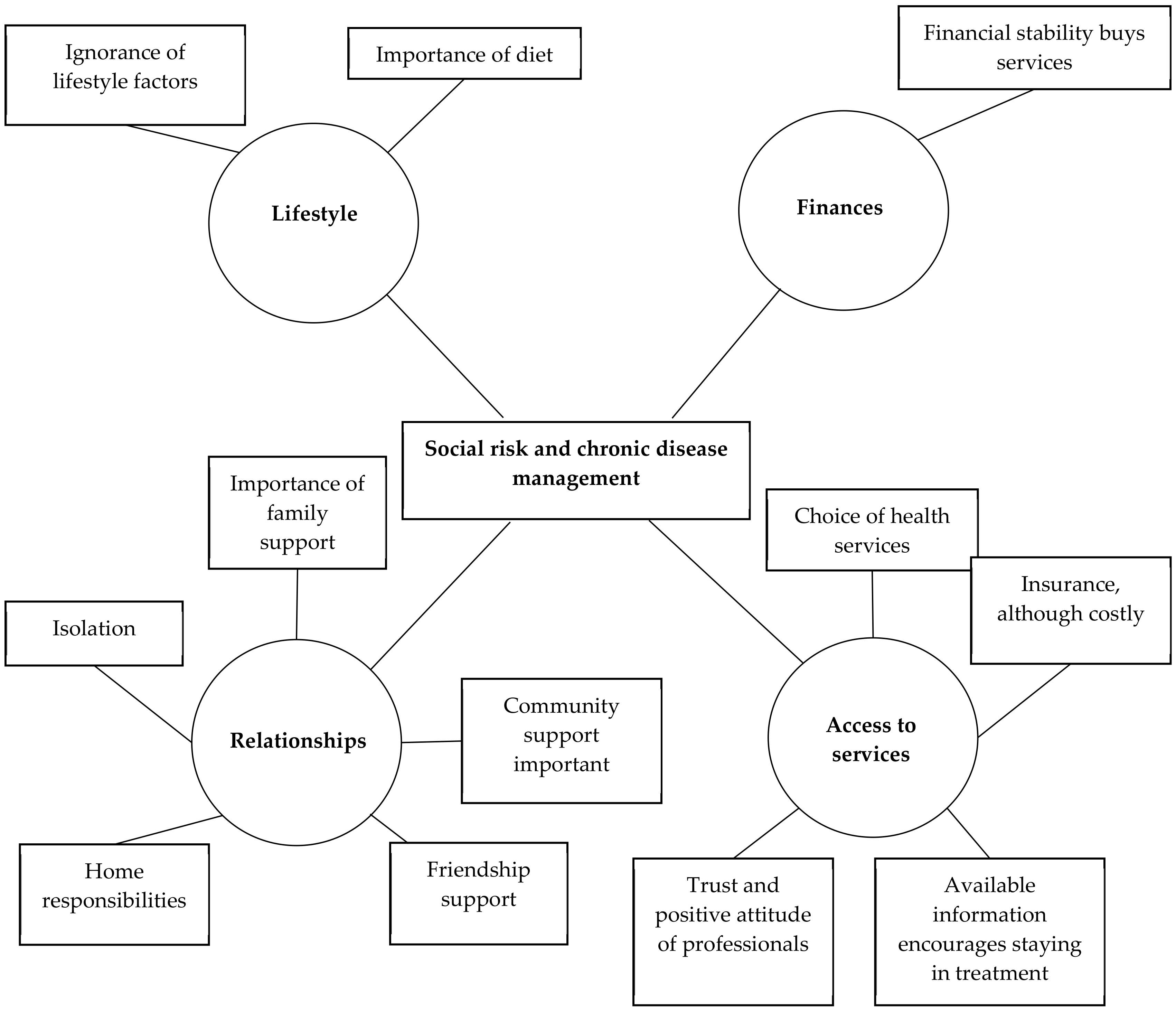
| Group 1—Low Risk | Social Risk and Chronic Disease Management | |
| Individuals are unaware of the health risks and complications Incorrect diet and lack of awareness | Lifestyle | |
| Financial Stability opens way for better choices and accessing quality services | Finance | |
| Lack of immediate family support to buy medicines Community support through health education Support of friends in the form of checking in, buying medicines, etc. | Relationships | |
| Trusting, friendly and positive attitude of healthcare professionals Economic stability results in accessing better quality services and informal support | Access to services | |
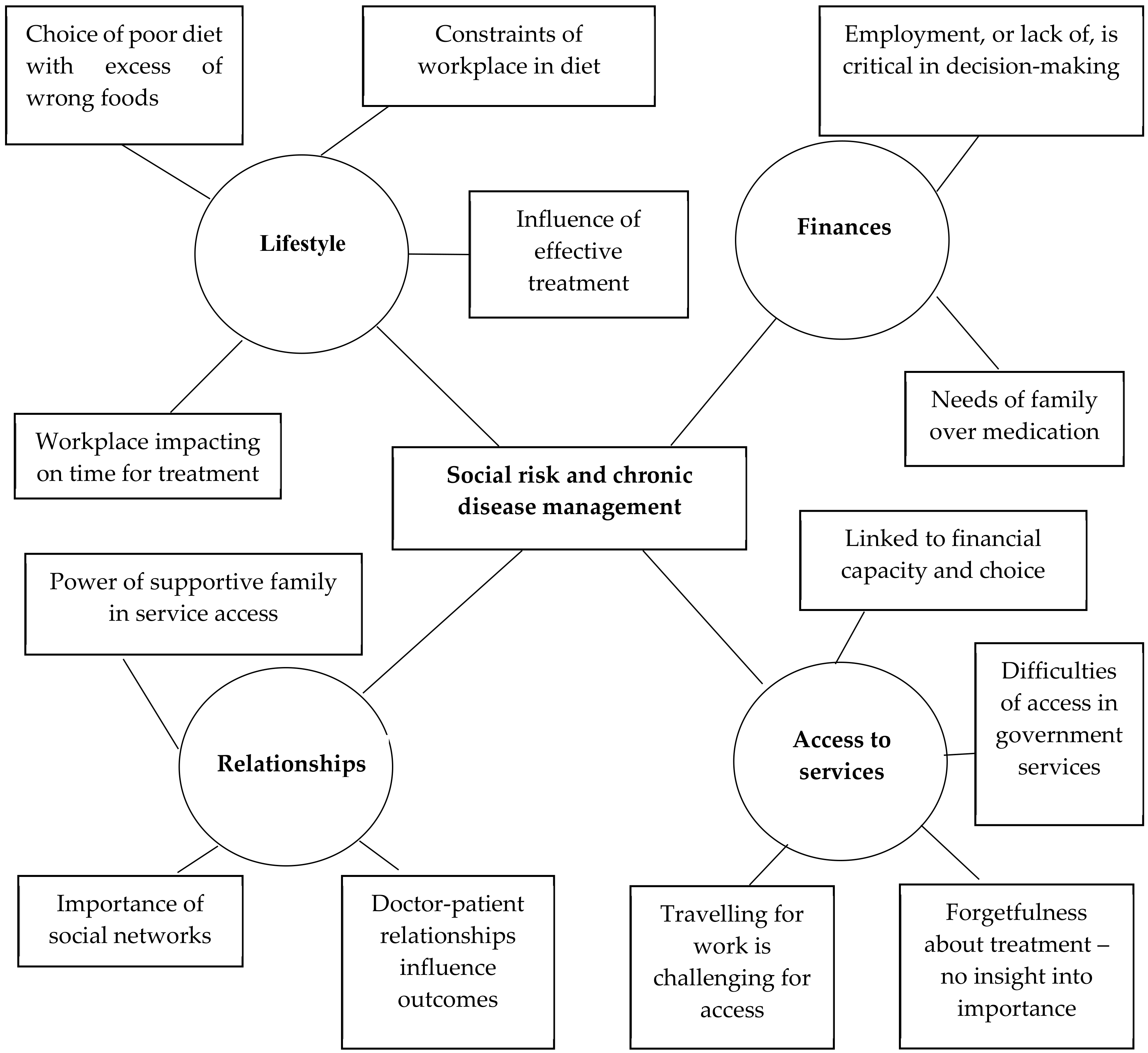
| Group 2—Behavioural Risk | ||
| Job and busy routine leading to non-adherence to following healthy diet Lack of education or knowledge leads to ignorance which, in turn, affects adherence | Lifestyle | |
| Unemployment with lack of stable income Choosing to meet the needs of family over buying medicines for self | Finance | |
| Physical and emotional support from immediate family members Networking by extended family members in the form of referrals and community linkages Positive doctor–patient relationship and involvement of health care professionals | Relationships | |
| Opting for alternative treatments (Ayurveda/homeopathy/naturopathy) Lack of trust towards government doctors Wrong notions such as one gets addicted to medicines together with forgetfulness leads to non-adherence Frequent travel as a barrier to non-adherence | Access to services | |
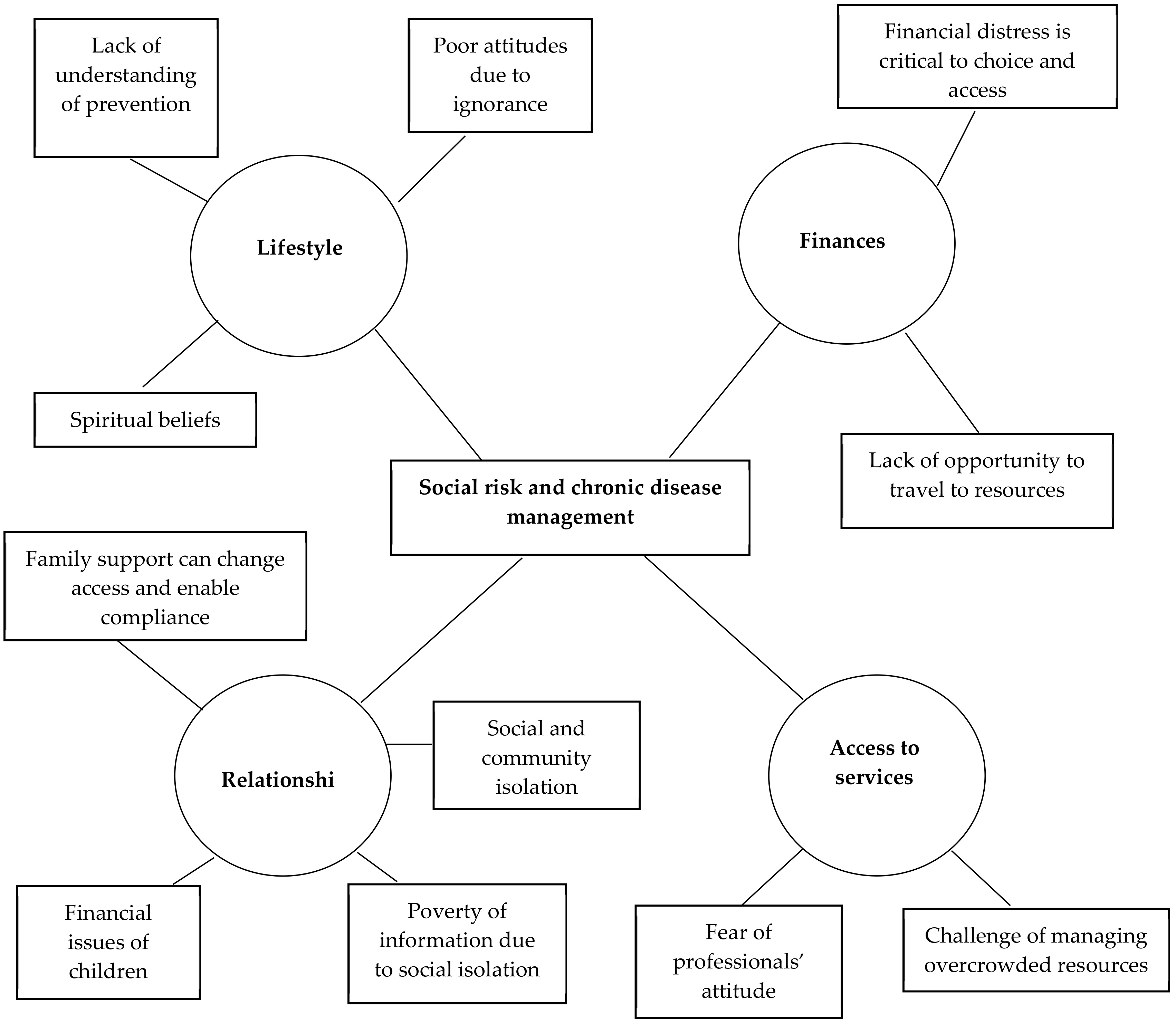
| Group 3—Social Risk | ||
| Awareness about the significance of the illness and complications resulting from non-adherence Spiritual beliefs and ventilation as a source of coping mechanism and restoring hope | Lifestyle | |
| Lack of finances as a reason to settle for government hospitals over private ones Lack of finances leading to inability to follow healthy, balanced diet and to buy medicines Informal support from churches or mosques | Finance | |
| Belief that own children won’t provide support because of financial constraints or conflicting relationships Life events like death of spouse Lack of neighbours and social isolation | Relationships | |
| Lack of transport to reach long distance resources Rude approach from healthcare professionals | Access to services |
| Challenges | Needs |
|---|---|
| Health care providers focus on medical treatment with little time or resources for care The community workforce is grassroots, reaching those in need, but extremely overloaded Assessment and intervention with social relationships a priority of family agencies employing social workers, however links between these agencies and health care providers is not always strong Systematic challenges: little time and resources for care Many government services are being provided but some lack awareness in the community, issues of accessibility for vulnerable populations Challenge for government services is the myth that free medicines or treatment are inadequate | Health care context Move from curative to preventive interventions Increased access to already existing mental health services like the District Mental Health Programme. Health volunteers exist for mental and neurological care, potential for other chronic conditions |
| Community care Strengthen lower-cost parts of this system, leaving clinical as it is but increasing access to ASHAs and social workers. Systems where patients are able get their medicines at their home Systems for coordination across workforce and services | |
| Family support and self-care Generate feasible systems through existing self-help groups to enhance social and emotional support Links are needed between community workers and supportive community programmes such as Kudumbasree, a trusted system of neighbourhood groups for poverty alleviation | |
| Awareness raising Sensitization about the services that are currently available (government services like free medicines, NCD clinics, etc.) Awareness of medication compliance is lacking |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Webber, M.; Joubert, J.; Fendt-Newlin, M.; Madavanakadu Devassy, S.; Scaria, L.; Benny, A.M.; Joubert, L. Towards the Development of an Intervention to Address Social Determinants of Non-Communicable Disease in Kerala, India: A Mixed Methods Study. Int. J. Environ. Res. Public Health 2020, 17, 8636. https://doi.org/10.3390/ijerph17228636
Webber M, Joubert J, Fendt-Newlin M, Madavanakadu Devassy S, Scaria L, Benny AM, Joubert L. Towards the Development of an Intervention to Address Social Determinants of Non-Communicable Disease in Kerala, India: A Mixed Methods Study. International Journal of Environmental Research and Public Health. 2020; 17(22):8636. https://doi.org/10.3390/ijerph17228636
Chicago/Turabian StyleWebber, Martin, Jacques Joubert, Meredith Fendt-Newlin, Saju Madavanakadu Devassy, Lorane Scaria, Anuja Maria Benny, and Lynette Joubert. 2020. "Towards the Development of an Intervention to Address Social Determinants of Non-Communicable Disease in Kerala, India: A Mixed Methods Study" International Journal of Environmental Research and Public Health 17, no. 22: 8636. https://doi.org/10.3390/ijerph17228636