A Meta-Synthesis of Policy Recommendations Regarding Human Mobility in the Context of Climate Change

 and
and 
Abstract
:1. Introduction
2. Methods
2.1. Protocol and Registration
2.2. Definitions
2.3. Search Strategy and Eligibility Criteria
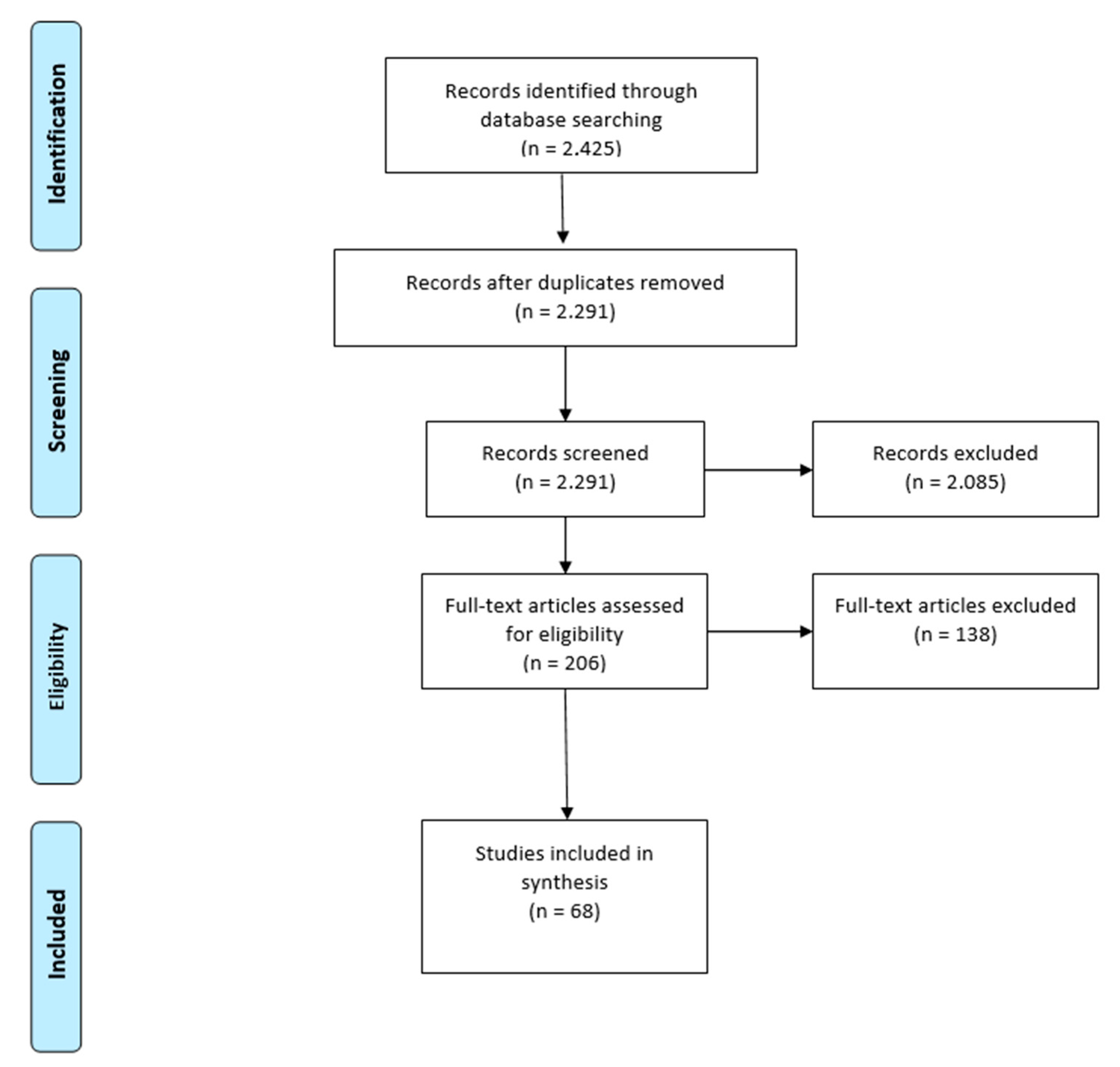
2.4. Literature Selection
2.5. Data Extraction
2.6. Quality Assessment
2.7. Data Analysis and Meta-Synthesis
3. Results
3.1. Included Studies
3.2. Study Settings
3.3. Quality Appraisal
3.4. The Links between Climate Mobility and Health
3.5. Thematic Analysis of Policy Recommendations
4. Discussion
4.1. Study Settings
4.2. Quality Appraisal and Study Design
4.3. Climate Mobilities and Health
4.4. Thematic Analysis of Policy Recommendations
4.5. Limitations
4.6. Future Research Directions
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Future Earth. Human Migration and Global Change—A Synthesis of Roundtable Discussions Facilitated by Future Earth. 2019. Available online: https://futureearth.org/wp-content/uploads/2019/07/synthesis_of_migration_roundtable_discussions_final.pdf (accessed on 29 October 2019).
- Gemenne, F. Why the numbers don’t add up: A review of estimates and predictions of people displaced by environmental changes. Glob. Environ. Chang. 2011, 21, S41–S49. [Google Scholar] [CrossRef]
- Marchiori, L.; Schumacher, I. When nature rebels: International migration, climate change, and inequality. J. Popul. Econ. 2011, 24, 569–600. [Google Scholar] [CrossRef] [Green Version]
- Gray, C.L.; Mueller, V. Natural disasters and population mobility in Bangladesh. Proc. Natl. Acad. Sci. USA 2012, 109, 6000–6005. [Google Scholar] [CrossRef] [Green Version]
- Bohra-Mishra, P.; Oppenheimer, M.; Hsiang, S.M. Non-linear Permanent Migration Response to Climatic Variations but Minimal Response to Disasters. Proc. Natl. Acad. Sci. USA 2014, 111, 9780–9785. [Google Scholar] [CrossRef] [Green Version]
- McLeman, R.A. Climate, and Human Migration: Past Experiences, Future Challenges; Cambridge University Press: Cambridge, UK, 2014. [Google Scholar]
- Intergovernmental Panel on Climate Change IPCC. AR5: Summary for policymakers Climate Change 2014: Impacts, Adaptation, and Vulnerability. Part A: Global and Sectoral Aspects. Contribution of Working Group II to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change; Field, C.B., Barros, V.R., Dokken, D.J., Mach, K.J., Mastrandrea, M.D., Bilir, T.E., Chatterjee, M., Ebi, K.L., Estrada, Y.O., Genova, R.C., et al., Eds.; Cambridge University Press: Cambridge, UK, 2014; pp. 1–32. [Google Scholar]
- Zickgraf, C.; Vigil, S.; de Longueville, F.; Ozer, P.; Gemenne, F. The Impact of Vulnerability and Resilience to Environmental Changes on Mobility Patterns in West Africa; World Bank: Washington, DC, USA, 2016. [Google Scholar]
- Grace, K.; Hertrich, V.; Singare, D.; Husak, G. Examining Rural Sahelian Out-Migration in the Context of Climate Change: An Analysis of the Linkages between Rainfall and out-Migration in Two Malian Villages from 1981 to 2009. World Dev. 2018, 109, 187–196. [Google Scholar] [CrossRef]
- Piguet, E.; Kaenzig, R.; Guélat, J. The uneven geography of research on ‘environmental migration. Popul. Environ. 2018, 39, 357–383. [Google Scholar] [CrossRef]
- International Organisation of Migration. World Migration Report. 2020. Available online: https://publications.iom.int/system/files/pdf/wmr_2020.pdf (accessed on 9 November 2020).
- Adams, H. Why populations persist: Mobility, place attachment, and climate change. Popul. Environ. 2016, 37, 429–448. [Google Scholar] [CrossRef]
- Hirvonen, K. Temperature changes, household consumption, and internal migration: Evidence from Tanzania. Am. J. Agricult. Econ. 2016, 98, 1230–1249. [Google Scholar] [CrossRef] [Green Version]
- Sauerborn, R. A Gaping Research Gap Regarding the Climate Change Impact on Health in Poor Countries. Eur. J. Epidemiol. 2017, 32, 855–856. [Google Scholar] [CrossRef] [Green Version]
- Herlihy, N. Climate change and human health: What are the research trends? A scoping review protocol. BMJ Open 2016, 6. [Google Scholar] [CrossRef]
- Bowen, K.J.; Ebi, K.L. Governing the Health Risks of Climate Change: Towards Multi-Sector Responses. Curr. Opin. Environ. Sustain. Sustain. Gov. Transf. 2015, 12, 80–85. [Google Scholar] [CrossRef]
- Vearey, J.; Hui, C.; Wickramage, C. Migration and Health: Current Issues, Governance and Knowledge Gaps. UN Dig. Libr. 2019, 209–228. [Google Scholar] [CrossRef]
- United Nations. COP 21: Report of the Conference of the Parties on Its twe.pdf. 2017. Available online: https://unfccc.int/resource/docs/2015/cop21/eng/10.pdf (accessed on 20 October 2020).
- United Nations. The Nansen Initiative Global Consultation Conference Report; Geneva 12–13 October 2015; United Nations: New York, NY, USA, 2017. [Google Scholar]
- United Nations. Sendai Framework for Disaster Risk Reduction 2015–2030. 2015. Available online: https://www.undrr.org/publication/sendai-framework-disaster-risk-reduction-2015-2030 (accessed on 20 October 2020).
- Grecequet, M.; DeWaard, J.; Hellmann, J.J.; Abel, G.J. Climate Vulnerability and Human Migration in Global Perspective. Sustainability 2017, 9, 720. [Google Scholar] [CrossRef] [Green Version]
- United National High Commission Refugees. Global Compact for Safe and Orderly Migration. 2018. Resolution Adopted by the General Assembly. Available online: www.un.org/en/ga/search/view_doc.asp?symbol=A/RES/73/195 (accessed on 15 June 2020).
- United Nations High Commission Refugees. Global Compact for Refugees. 2018. Available online: www.unhcr.org/gcr/GCR_English.pdf (accessed on 3 December 2020).
- World Health Organisation. Pacific Island Action Plan on Climate Change and Health’, WHO. 2018. Available online: https://apps.who.int/iris/bitstream/handle/10665/275484/9789290618645-eng.pdf?sequence=1&isAllowed=y (accessed on 17 September 2020).
- World Health Organisation. Climate Change and Health in Small Island Developing States. A WHO Special Initiative. 2018. Available online: https://www.who.int/publications/i/item/climate-change-and-health-in-small-island-developing-states (accessed on 3 December 2020).
- Haddaway, N.R.; Macura, B.; Whaley, P.; Pullin, A.S. ROSES RepOrting Standards for Systematic Evidence Syntheses: Pro Forma, Flow-Diagram and Descriptive Summary of the Plan and Conduct of Environmental Systematic Reviews and Systematic Maps. Environ. Evid. 2018, 7, 7. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Clark, J. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement (Chinese edition). J. Chin. Integr. Med. 2019, 7, 889–896. [Google Scholar] [CrossRef]
- World Health Organisation. Preamble to the Constitution of WHO as Adopted by the International Health Conference. New York, 19 June–22 July 1946; Signed on 22 July 1946 by the Representatives of 61 States (Official Records of WHO, no. 2, p. 100) and Entered into Force on 7 April 1948; WHO: Geneva, Switzerland, 2006. [Google Scholar]
- Intergovernmental Panel on Climate Change IPCC. Annex I: Glossary Global Warming of 1.5 °C. An IPCC Special Report on the Impacts of Global Warming of 1.5 °C Above Pre-Industrial Levels and Related Global Greenhouse Gas Emission Pathways’, in the Context of Strengthening the Global Response to the Threat of Climate Change, Sustainable Development, and Efforts to Eradicate Poverty; Hoegh-Guldberg, O., Jacob, D., Bindi, M., Brown, S., Camilloni, I., Diedhiou, A., Djalante, R., Ebi, K., Engelbrecht, F., Guiot, J., et al., Eds.; IPCC: Geneva, Switzerland, 2018; Available online: https://www.ipcc.ch/sr15/ (accessed on 28 July 2020).
- International Organisation of Migration. Website Glossary; Adapted from World Health Organization, International Organization for Migration’, Government of Spain, Health of Migrants—The Way Forward, Report of a Global Consultation (3–5 March 2010) p 14 (building on J Puebla Fortier, Migrant-Sensitive Health Systems; Background Paper for the Global Consultation on the Health of Migrants, March 2010; IOM Glossary; IOM: Belgrade, Serbia, 2019. [Google Scholar]
- Foresight, U.K. Migration and Global Environmental Change: Future Challenges and Opportunities; UK Government Office for Science: London, UK, 2011.
- Ayeb-Karlsson, S.; Smith, C.D.; Kniveton, D. A Discursive Review of the Textual Use of ‘Trapped’ in Environmental Migration Studies: The Conceptual Birth and Troubled Teenage Years of Trapped Populations. Ambio 2018, 47, 557–573. [Google Scholar] [CrossRef] [Green Version]
- Schwerdtle, P.N.; McMichael, C.; Mank, I.; Sauerborn, R.; Danquah, I.; Bowen, K.J. Health and Migration in the Context of a Changing Climate: A Systematic Literature Assessment. Environ. Res. Lett. 2020, 15, 103006. [Google Scholar] [CrossRef]
- Hong, Q.N.; Pluye, P.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.P.; Griffiths, F.; Nicolau, B. Mixed Methods Appraisal Tool (MMAT), Version 2018; Registration of copyright 1148552; McGill: Montreal, QC, Canada, 2018. [Google Scholar]
- Braun, V.; Victoria, C. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Joanna Briggs Institute. JBI. 2020. Available online: https://joannabriggs.org/ (accessed on 3 December 2020).
- Abah, R.C.; Petja, B.M. Assessment of potential impacts of climate change on agricultural development in the Lower Benue River Basin. Environ. Monit. Assess. 2016, 188, 683. [Google Scholar] [CrossRef]
- Afifi, T.; Liwenga, E.; Kwezi, K. Rainfall-induced crop failure, food insecurity and out-migration in Same-Kilimanjaro, Tanzania. Clim. Dev. 2014, 6, 53–60. [Google Scholar] [CrossRef]
- Ahmed, B.; Kelman, I.; Kamruzzaman, M.; Mohiuddin, H.; Rahman, M.; Das, A.; Fordham, M.; Shamsudduha, M. Indigenous people’s responses to drought in northwest Bangladesh. Environ. Dev. 2019, 29, 55–66. [Google Scholar] [CrossRef] [Green Version]
- Albert, S.; Bronen, R.; Tooler, N.; Leon, J.; Yee, D.; Ash, J.; Boseto, D.; Grinham, A. Heading for the hills: Climate-driven community relocations in the Solomon Islands and Alaska provide insight for a 1.5 C future. Reg. Environ. Chang. 2018, 18, 2261–2272. [Google Scholar] [CrossRef]
- Amstislavski, P.; Zubov, L.; Chen, H.; Ceccato, P.; Pekel, J.F.; Weedon, J. Effects of increase in temperature and open water on transmigration and access to health care by the Nenets reindeer herders in northern Russia. Int. J. Circumpolar Health 2013, 72, 21183. [Google Scholar] [CrossRef]
- Anastario, M.; Shehab, N.; Lawry, L. Increased gender-based violence among women internally displaced in Mississippi 2 years post–Hurricane Katrina. Dis. Med. Public Health Prep. 2009, 3, 18–26. [Google Scholar] [CrossRef] [Green Version]
- Anupama, G.V.; Bantilan, M.; Cynthia, S.; Uttam, K.D.; Haragopal, V. Seasonal Migration and Moving Out of Poverty in Rural India: Insights from Statistical Analysis. Asian J. Agricult. Dev. 2016, 13, 35–54. [Google Scholar]
- Assan, K.; Caminade, J.C.; Obeng, F. Environmental variability and vulnerable livelihoods: Minimising risks and optimising opportunities for poverty alleviation. J. Int. Dev. J. Dev. Stud. Assoc. 2009, 21, 403–418. [Google Scholar]
- Atta Ur Rahman, A.; Akhtar, P.A.; Siddiqui, M.I. Psychological Effects among Internally Displaced Persons (IDPS) Residing in two Districts of Sindh. Med. Forum Monthly 2013, 24, 82–84. [Google Scholar]
- Baker, R.E. Climate change drives increase in modeled HIV prevalence. Clim. Chang. 2020, 163, 1–16. [Google Scholar] [CrossRef]
- Bayar, M.; Aral, M.M. An analysis of large-scale forced migration in Africa. Int. J. Env. Res. Public Health 2019, 16, 4210. [Google Scholar] [CrossRef] [PubMed]
- Behr, J.G.; Diaz, R. Disparate health implications stemming from the propensity of elderly and medically fragile populations to shelter in place during severe storm events. J. Public Health Manag. Pract. 2013, 19, S55–S62. [Google Scholar] [CrossRef] [Green Version]
- Carney, M.A.; Krause, K.C. Immigration/migration and healthy publics: The threat of food insecurity. Palgrave Commun. 2020, 6, 1–12. [Google Scholar] [CrossRef]
- Chen, Y.L.; Lai, C.S.; Chen, W.T.; Hsu, W.Y.; Wu, Y.C.; Wang, P.W.; Chen, C.S. Risk factors for PTSD after Typhoon Morakot among elderly people in Taiwanese aboriginal communities. Int. Psychogeriatr. 2011, 23, 1686. [Google Scholar] [CrossRef] [PubMed]
- Coker, A.L.; Hanks, J.S.; Eggleston, K.S.; Risser, J.; Tee, P.G.; Chronister, K.J.; Franzini, L. Social and mental health needs assessment of Katrina evacuees. Disaster Manag. Response 2006, 4, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Craven, L.K. Migration-affected change and vulnerability in rural Vanuatu. Asia Pac. Viewp. 2015, 56, 223–236. [Google Scholar] [CrossRef]
- Di Giorgi, E.; Michielin, P.; Michielin, D. Perception of Climate Change, Loss of Social Capital and Mental Health in Two Groups of Migrants from African Countries. Ann. dell’Istituto Super. Sanita 2020, 56, 150–156. [Google Scholar] [PubMed]
- Dinkelman, T. Long-run Health Repercussions of Drought Shocks: Evidence from South African Homelands. Econ. J. 2017, 127, 1906–1939. [Google Scholar] [CrossRef] [Green Version]
- Edwards, J.B. The Logistics of Climate-Induced Resettlement: Lessons from the Carteret Islands, Papua New Guinea. Refug. Surv. Quart. 2013, 32, 52–78. [Google Scholar] [CrossRef]
- Etzold, B.; Ahmed, A.U.; Hassan, S.M.; Neelormi, S. Clouds gather in the sky, but no rain falls. Vulnerability to rainfall variability and food insecurity in Northern Bangladesh and its effects on migration. Clim. Dev. 2014, 6, 18–27. [Google Scholar] [CrossRef]
- Grawert, E. Impacts of male outmigration on women: A case study of Kutum/Northern Darfur/Sudan. Ahfad J. 1992, 9, 37. [Google Scholar]
- Gautam, Y. Seasonal migration and livelihood resilience in the face of climate change in Nepal. Mt. Res. Dev. 2017, 37, 436–445. [Google Scholar] [CrossRef] [Green Version]
- Haque, R.; Parr, N.; Muhidin, A. Parents’ healthcare-seeking behavior for their children among the climate-related displaced population of rural Bangladesh. Soc. Sci. Med. 2019, 226, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Haque, R.; Parr, N.; Muhidin, S. Climate-Related Displacement and Antenatal Care Service Utilization in Rural Bangladesh. Int. Perspect. Sex Reprod. Health 2020, 46. [Google Scholar] [CrossRef]
- Haque, M.R.; Parr, N.; Muhidin, S. The effects of household’s climate-related displacement on delivery and postnatal care service utilization in rural Bangladesh. Soc. Sci. Med. 2020, 247, 112819. [Google Scholar] [CrossRef]
- Heaney, A.K.; Winter, S.J. Climate-driven migration: An exploratory case study of Maasai health perceptions and help-seeking behaviors. Int. J. Public Health 2016, 61, 641–649. [Google Scholar] [CrossRef] [PubMed]
- Hori, M.; Schafer, M.J. Social costs of displacement in Louisiana after Hurricanes Katrina and Rita. Popul. Environ. 2010, 31, 64–86. [Google Scholar] [CrossRef]
- Hunter, L.M.; Simon, D.H. Might climate change the “healthy migrant” effect? Glob. Environ. Chang. 2017, 47, 133–142. [Google Scholar] [CrossRef]
- Hutton, D.; Haque, C.E. Patterns of coping and adaptation among erosion-induced displacees in Bangladesh: Implications for hazard analysis and mitigation. Nat. Hazards 2003, 29, 405–421. [Google Scholar] [CrossRef]
- Hutton, D.; Haque, C.E. Human vulnerability, dislocation and resettlement: Adaptation processes of river-bank erosion-induced displacees in Bangladesh. Disasters 2004, 28, 41–62. [Google Scholar]
- Iqbal, M.W.; Donjadee, S.; Kwanyuen, B.; Liu, S. Farmers’ perceptions of and adaptations to drought in Herat Province, Afghanistan. J. Mt. Sci. 2018, 15, 1741–1756. [Google Scholar] [CrossRef]
- Islam, M.R.; Hasan, M. Climate-induced human displacement: A case study of Cyclone Aila in the south-west coastal region of Bangladesh. Nat. Hazards 2016, 81, 1051–1071. [Google Scholar] [CrossRef]
- Islam, M.M.; Sallu, S.; Hubacek, K.; Paavola, J. Migrating to tackle climate variability and change? Insights from coastal fishing communities in Bangladesh. Clim. Chang. 2014, 124, 733–746. [Google Scholar] [CrossRef] [Green Version]
- Jacobson, C.; Crevello, S.; Chea, C.; Jarihani, B. When is migration a maladaptive response to climate change? Reg. Environ. Chang. 2019, 19, 101–112. [Google Scholar] [CrossRef] [Green Version]
- Kabir, M.I.; Rahman, M.B.; Smith, W.; Lusha, M.A.F.; Milton, A.H. Climate change and health in Bangladesh: A baseline cross-sectional survey. Glob. Health Action 2016, 9, 29609. [Google Scholar] [CrossRef]
- Loebach, P.; Korinek, K. Disaster vulnerability, displacement, and infectious disease: Nicaragua and Hurricane Mitch. Pop. Environ. 2019, 40, 434–455. [Google Scholar] [CrossRef]
- Loevinsohn, M. The 2001–03 famine and the dynamics of HIV in Malawi: A natural experiment. PLoS ONE 2015, 10, e0135108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Low, A.J.; Frederix, F.; McCracken, S.; Manyau, S.; Gummerson, E.; Radin, E.; Davia, S.; Longwe, H.; Ahmed, N.; Parekh, B. Association between severe drought and HIV prevention and care behaviors in Lesotho: A population-based survey 2016–2017. PLoS Med. 2019, 16, e1002727. [Google Scholar] [CrossRef] [Green Version]
- McElfish, P.A.; Moore, R.; Woodring, D.; Purvis, R.S.; Maskarinec, G.G.; Bing, W.I.; Hudson, J.O.; Kohler, P.; Goulden, P.A. Social ecology and diabetes self-management among Pacific Islanders in Arkansas. J. Family Med. Dis. Prev. 2016, 2. [Google Scholar] [CrossRef]
- Mertz, O.; Mbow, C.; Reenberg, A.; Diouf, A. Farmers’ perceptions of climate change and agricultural adaptation strategies in rural Sahel. Environ. Manag. 2009, 43, 804–816. [Google Scholar] [CrossRef] [PubMed]
- Messias, D.; Hilfinger, K.; Lacy, E.C. Katrina-related health concerns of Latino survivors and evacuees. J. Health Care Poor Underserved 2007, 18, 443–464. [Google Scholar] [CrossRef]
- Milan, A.; Ruano, S. Rainfall variability, food insecurity and migration in Cabricán, Guatemala. Clim. Dev. 2014, 6, 61–68. [Google Scholar] [CrossRef]
- Molla, N.A.; Mollah, K.A.; Ali, G.; Fungladda, W.; Shipin, O.V.; Wongwit, W.; Tomomi, H. Quantifying disease burden among climate refugees using multidisciplinary approach: A case of Dhaka, Bangladesh. Urban Clim. 2014, 8, 126–137. [Google Scholar] [CrossRef]
- Molla, N.A.; Mollah, K.A.; Fungladda, W.; Ramasoota, P. Multidisciplinary household environmental factors: Influence on DALYs lost in climate refugees community. Environ. Dev. 2014, 9, 1–11. [Google Scholar] [CrossRef]
- Murali, J.; Afifi, T.A. Rainfall variability, food security and human mobility in the Janjgir-Champa district of Chhattisgarh state, India. Clim. Dev. 2014, 6, 28–37. [Google Scholar] [CrossRef]
- Nawrotzki, R.J.; Schlak, A.M.; Kugler, T.A. Climate, migration, and the local food security context: Introducing Terra Populus. Pop. Environ. 2016, 38, 164–184. [Google Scholar] [CrossRef] [PubMed]
- Oyekale, A.S.; Oladele, O.I.; Mukela, F. Impacts of Flooding on Coastal Fishing Folks and Risk Adaptation Behaviours in Epe, Lagos State. Afr. J. Agricult. Res. 2013, 8, 3392–3405. [Google Scholar] [CrossRef] [Green Version]
- Pardhi, A.; Jungari, S.; Kale, P.; Bomble, P. Migrant motherhood: Maternal and child health care utilization of forced migrants in Mumbai, Maharashtra, India. Childr. Youth Serv. Rev. 2020, 110, 104823. [Google Scholar] [CrossRef]
- Penning-Rowsell, E.C.; Sultana, P.; Thompson, P.M. The ‘last resort’? Population movement in response to climate-related hazards in Bangladesh. Global environmental change, extreme environmental events and „environmental migration: Exploring the connections. Environ. Sci. Policy 2013, 27, S44–S59. [Google Scholar] [CrossRef]
- Perez-Saez, J.; King, A.A.; Rinaldo, A.; Yunus, M.; Faruque, A.S.G.; Pascual, M. Climate-driven endemic cholera is modulated by human mobility in a megacity. Adv. Water Res. 2017, 108, 367–376. [Google Scholar] [CrossRef] [PubMed]
- Philibert, A.; Tourigny, C.; Coulibaly, A.; Fournier, P. Birth seasonality as a response to a changing rural environment (Kayes region, Mali). J. Biosoc. Sci. 2012, 45, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Rademacher-Schulz, C.; Schraven, B.; Mahama, E.S. Time matters: Shifting seasonal migration in Northern Ghana in response to rainfall variability and food insecurity. Clim. Dev. 2014, 6, 46–52. [Google Scholar] [CrossRef] [Green Version]
- Rahaman, M.A.; Rahman, M.M.; Bahauddin, K.M.; Khan, S.; Hassan, S. Health Disorder of Climate Migrants in Khulna City: An Urban Slum Perspective. Int. Migr. 2018, 56, 42–55. [Google Scholar] [CrossRef]
- Rakib, M.A.; Sasaki, J.; Matsuda, H.; Fukunaga, M. Severe salinity contamination in drinking water and associated human health hazards increase migration risk in the southwestern coastal part of Bangladesh. J. Environ. Manag. 2019, 240, 238–248. [Google Scholar] [CrossRef] [PubMed]
- Roncoli, C.; Ingram, K.; Kirshen, P. The costs and risks of coping with drought: Livelihood impacts and farmers1 responses in Burkina Faso. Clim. Res. 2001, 19, 119–132. [Google Scholar] [CrossRef] [Green Version]
- Shanthi, B.; Mahalakshimi, P.; Chandrasekaran, V. Assessment of challenges faced by the coastal women due to the impact of climatic change in selected coastal districts of Tamil Nadu, India. Ind. J. Fish. 2017, 64. [Google Scholar] [CrossRef]
- Suckall, N.; Fraser, E.; Forster, P. Reduced migration under climate change: Evidence from Malawi using an aspirations and capabilities framework. Clim. Dev. 2017, 9, 298–312. [Google Scholar] [CrossRef]
- Taiban, S.; Lin, H.n.; Ko, C.C. Disaster, relocation, and resilience: Recovery and adaptation of Karamemedesane in Lily Tribal Community after Typhoon Morakot, Taiwan. Environ. Hazards 2020, 19, 209–222. [Google Scholar] [CrossRef]
- Tschakert, P.; Tutu, R.; Alcaro, A. Embodied experiences of environmental and climatic changes in landscapes of everyday life in Ghana. Emot. Space Soc. 2013, 7, 13–25. [Google Scholar] [CrossRef]
- Van der Geest, K.; Nguyen, K.V.; Nguyen, T.C. Internal migration in the upper mekong delta, viet nam: What is the role of climate related stressors? Asia-Pac. Popul. J. 2012, 29, 25–41. [Google Scholar] [CrossRef]
- Van Der Geest, K.; Burkett, M.; Fitzpatrick, J.; Stege, M.; Wheeler, B. Climate change, ecosystem services and migration in the Marshall Islands: Are they related? Clim. Chang. 2020, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Warner, K.; Afifi, T. Where the rain falls: Evidence from 8 countries on how vulnerable households use migration to manage the risk of rainfall variability and food insecurity. Clim. Dev. 2014, 6, 1–17. [Google Scholar] [CrossRef]
- Wolsko, C.; Marino, E. Disasters, Migrations, and the Unintended Consequences of Urbanization: What’s the Harm in Getting out of Harm’s Way? Popul. Environ. 2016, 37, 411–428. [Google Scholar] [CrossRef]
- Woodhall-Melnik, J.; Grogan, C. Perceptions of Mental Health and Wellbeing Following Residential Displacement and Damage from the 2018 St. John River Flood. Int. J. Env. Res. Public Health 2019, 16, 4174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaman, S.; Sammonds, P.; Ahmed, B.; Rahman, T. Disaster risk reduction in conflict contexts: Lessons learned from the lived experiences of Rohingya refugees in Cox’s Bazar, Bangladesh. Int. J. Dis. Risk Reduct. 2020, 50, 101694. [Google Scholar] [CrossRef] [PubMed]
- Groundswell: Preparing for Internal Climate Migration. Available online: https://openknowledge.worldbank.org/handle/10986/29461 (accessed on 12 December 2020).
- Boas, I.; Farbotko, C.; Adams, H.; Sterly, H.; Bush, S.; van der Geest, K.; Blondin, S. Climate migration myths. Nat. Clim. Chang. 2019, 9, 901–903. [Google Scholar] [CrossRef] [Green Version]
- International Organisation of Migration. IOM and Migration, Environment and Climate Change (MECC). 2020. Available online: https://environmentalmigration.iom.int/iom-and-migration-environment-and-climate-change-mecc (accessed on 25 October 2020).
- Farbotko, C.; Dun, O.; Thornton, F.; McNamara, K.E.; McMichael, C. Relocation planning must address voluntary immobility. Nat. Clim. Chang. 2020, 10, 702–704. [Google Scholar] [CrossRef]
- Abubakar, I.; Aldridge, R.W.; Devakumar, D.; Orcutt, M.; Burns, R.; Barreto, M.L.; Hargreaves, S. The UCL–Lancet Commission on Migration and Health: The health of a world on the move. Lancet 2018, 392, 2606–2654. [Google Scholar] [CrossRef] [Green Version]
- Ebi, K.L. Mechanisms, policies, and tools to promote health equity and effective governance of the health risks of climate change. J. Public Health Policy 2020, 41, 11–13. [Google Scholar] [CrossRef]
- Barnett, J. Global environmental change II: Political economies of vulnerability to climate change. Prog. Human Geogr. 2020. [Google Scholar] [CrossRef]
- McMichael, C. Human mobility, climate change, and health: Unpacking the connections. Lancet Planet. Health 2020, 4, e217–e218. [Google Scholar] [CrossRef]
- Warner, K.; Van der Geest, K. Loss and damage from climate change: Local-level evidence from nine vulnerable countries. Int. J. Glob. Warm. 2013, 5, 367–386. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Migration (Population) | Climate Change (Exposure) | Health (Outcome) |
|---|---|---|
| Population movement Displacement Population displacement Forced displacement Internal displacement Seasonal migration Permanent migration Planned relocation Migrant Mobility Internally Displaced Persons Refugee | Climate variability Global warming Weather variability Greenhouse effect Sea level rise Environmental disaster Natural disaster Drought Climate hazard | Well being Disease: NCD, Communicable, Infectious Epidemiolog Lifestyle Co-benefits Mortality Morbidity Climate sensitive disease Nutrition: Malnutrition, Undernutrition Psychosocial Dehydration Health Services: Water and Sanitation, Food Security |
| Criterion | Inclusion | Exclusion |
|---|---|---|
| Population | Engaging in/affected by mobility response. Any country. Any population. | Not human mobility: plant or animal. |
| Exposure | Climate change, variability, or natural hazard influencing mobility responses. | Other migration drivers (e.g., political, economic, social, demographic) with no reference to climate or environmental change. Hazard not relatable to climate change (e.g., volcano/earthquake) |
| Outcome | Health-related: either a direct measure of health outcome (i.e.,—disease prevalence) or an indirect measure of health (i.e., food security and water/sanitation/hygiene—[WaSH]). Access to healthcare. Psychosocial health. | No health outcome. Not human health; animal/plant. Social determinants of health; income, livelihood, employment, education. |
| Nexus | Includes climate change, migration, and health. | Focus on two elements (dyad) of the nexus (i.e., climate-health, climate-migration). Focus on OneHealth, Planetary Health, Environmental Health. |
| Study Type | Peer-reviewed empirical research. All designs: quantitative, qualitative, mixed methods, modeling. | Not empirical, systematic review, viewpoint, editorial, book chapter, grey literature, dissertation, conference proceeding, report. |
| Time | 1990–2020 (August). | Outside this timeframe. |
| Language | Full text available in English or German. | Other languages. |
| Reference | Title | Research Setting | Focus of the Study | Study Design and QA |
|---|---|---|---|---|
| Abah and Petja (2016) [37] | Assessment of potential impacts of climate change on agricultural development in the Lower Benue River Basin | Nigeria & Cameroon | (Mobility) Rural-Urban migration. (Climate) Rainfall & temperature variability, floods & droughts, heat stress, surface water trends. (Health) Infectious disease, HIV/AIDS. | Modelling Unable to assess using MMAT |
| Adams (2016) [12] | Why populations persist: mobility, place attachment and climate change | Peru | (Mobility) Trapped populations/immobility. (Climate) Temperature extremes, excessive precipitation, abrupt seasonal weather changes & drought, glacial retreat. (Health) Temperature extremes, excessive precipitation, abrupt seasonal weather changes & drought, glacial retreat. | Quantitative. Analytical: Cross-sectional survey *** |
| Afifi, Liwenga and Kwezi (2014) [38] | Rainfall-induced crop failure, food insecurity and out-migration in Same-Kilimanjaro, Tanzania | Tanzania | (Mobility) Seasonal migration & temporal migration. (Climate) Rainfall variability, floods & droughts, water shortages. (Health) Food insecurity. | Mixed methods; Expert interviews & quantitative descriptive survey. Participatory research approach ** |
| Ahmed, Kelman… Shamsudduha (2019) [39] | Indigenous people’s responses to drought in northwest Bangladesh | Bangladesh | (Mobility) Seasonal migration. (Climate) Drought. (Health) Food security, Water security, Water-borne disease. | Mixed methods: Household survey & participatory rural appraisal (qualitative). **** |
| Albert, Bronen… Grinham (2018) [40] | Heading for the hills: climate-driven community relocations in the Solomon Islands and Alaska provide insight for a 1.5 °C future | Solomon Islands & Alaska | (Mobility) Relocation: Supported and Unsupported. (Climate) Sea level rise, reduced Arctic sea ice, melting permafrost, sea-level rise, erosion & flooding. (Health) Access to health care facilities, health & safety risks, water borne disease, vector borne disease, dietary adaptation. | Qualitative case studies **** |
| Amstislavski, Zubov… Weedon (2013) [41] | Effects of increase in temperature and open water on transmigration and access to health care by the Nenets reindeer herders in northern Russia | Northern Russia | (Mobility) Inhibition (delaying) regular transmigration. (Climate) Temperature increase, reduction of ice-rich permafrost & glaciers, changes in hydrological cycles. (Health) Access to health care facilities, risks of injury. | Quant. non-rand. Water body & temp. data, migrant health care records. *** |
| Anastario, Shehab, and Lawry (2009) [42] | Increased GBV Among Women Internally Displaced in Mississippi 2 Years Post–Hurricane Katrina | Mississippi, USA | (Mobility) Forced displacement. (Climate) Hurricane. (Health) Sexual & physical violence, suicidal ideation & attempts, depression. | Quant. non-rand. Successive cross-sectional surveys. ***** |
| Anupama, Deb…Vajjha (2016) [43] | Seasonal Migration and Moving Out of Poverty in Rural India: Insights from Statistical Analysis | Rural India | (Mobility) Temporary/seasonal migration. (Climate) Drought. (Health) HIV/AIDS, water-borne disease, general & sexual health, social issues. | Quant. non-rand. ** |
| Assan, Caminade and Obeng (2009) [44] | Environmental variability & vulnerable livelihoods: Minimising risks & optimising opportunities for poverty alleviation | North Eastern Ghana | (Mobility) Temporary migration, circular migration. (Climate) Erratic and declining mean rainfall. (Health) Food insecurity. | Mixed methods. 1° & 2° quantitative/qualitative. *** |
| Atta Ur Rahman, Akhtar and Siddiqui (2013) [45] | Psychological Effects among Internally Displaced Persons (IDPS) residing in two districts of Sindh | Sindh, Pakistan | (Mobility) Forced displacement. (Climate) Flood. (Health) Mental disorders. | Descriptive cross-sectional study. * |
| Ayeb-Karlsson, Kniveton, Cannon (2020) [32] | Trapped in the prison of the mind: Notions of climate-induced (im)mobility decision-making and wellbeing from an urban informal settlement in Bangladesh | Bangladesh | (Mobility) Immobility. (Climate) Multiple climate-hazards. (Food) Sense of belonging and mental health. | Q-methodology & discourse analysis. **** |
| Baker (2020) [46] | Climate change drives increase in modeled HIV prevalence | Sub Saharan Africa | (Mobility) Migration. (Climate) General climate change and temperature. (Health) HIV. | Modelling |
| Bayar and Aral (2019) [47] | An Analysis of Large-Scale Forced Migration in Africa | African region | (Mobility) Forced Migration. (Climate) Multiple climate-hazards. (Health) Public health and wellbeing as a component of human security. | Modelling |
| Behr and Diaz (2013) [48] | Disparate Health Implications Stemming from the Propensity of Elderly & Medically Fragile Populations to Shelter in Place During Severe Storm Events | North Carolina, USA | (Mobility) Forced displacement, immobility. (Climate) Hurricane. (Health) Access to the support system, medical records, medical regimens, nutrition. | Quant. desc. ** |
| Carney and Krause (2020) [49] | Immigration/migration & healthy publics: the threat of food insecurity | USA, Dominican Republic, Italy | (Mobility) International migration. (Climate) Climate change. (Health) Food Insecurity. | Qualitative: Ethnography. ** |
| Chen, Lai… Chen (2011) [50] | Risk factors for PTSD after Typhoon Morakot among elderly people in Taiwanese aboriginal communities | Taiwan | (Mobility) Relocation. (Climate) Typhoon. (Health) PTSD, injury/death, self-perceived health. | Quant. desc. ***** |
| Coker, Hanks… Franzini (2006) [51] | Social and Mental Health Needs Assessment of Katrina Evacuees | Houston, USA | (Mobility) Forced displacement/evacuation. (Climate) Hurricane. (Health) NCDs, PTSD. | Quant. desc. ** |
| Craven (2015) [52] | Migration-affected change and vulnerability in rural Vanuatu: Migration-affected change in rural Vanuatu | Vanuatu | (Mobility) Seasonal migration. (Climate) Rainfall variability. (Health) Health financing, food security. | Qualitative; Interviews & focus groups. *** |
| Di Giorgi, Michielin and Michielin (2020) [53] | Perception of climate change, Loss of social capital and mental health in two groups of migrants from African countries | Italy | (Mobility) International migration. General climate change. (Health) Social Capital. Mental Health. | Quant. non-rand. Semi-structured interviews. ** |
| Dinkelman (2017) [54] | Long-Run Health Repercussions of Drought Shocks: Evidence from South African Homelands | South Africa | (Mobility) Multiple types of migration, internal migration, labour migration. (Climate) Drought. (Health) Disability (visual, hearing, speech, mental, physical). | Quant. non-rand. Analytical. *** |
| Edwards (2013) [55] | The Logistics of Climate-Induced Resettlement: Lessons from the Carteret Islands, Papua New Guinea | Carteret Islands, PNG | (Mobility) Forced displacement, relocation. (Climate) Sea-level rise, King tides, storm surge, floods. (Health) Food insecurity, mental health. | Qualitative; Case study interviews. * |
| Etzold, Ahmed…Neelormi (2014) [56] | Clouds gather in the sky, but no rain falls. Vulnerability to rainfall variability and food insecurity in Northern Bangladesh and its effects on migration | Northern Bangladesh | (Mobility) Labour migration (permanent, seasonal, temporary), immobility. (Climate) Rainfall variability. (Health) Food insecurity. | Mixed Methods. Interviews. Focus Groups. Questionnaires. * |
| Grawert (1992) [57] | Impacts of male outmigration on women: A case study of Kutum/Northern Darfur/Sudan | Western Sudan | (Mobility) Out-migration. (Climate) Drought. (Health) Food insecurity. | Qualitative; Case study. * |
| Grecequet, DeWaard…Abel (2017) [21] | Climate Vulnerability and Human Migration in Global Perspective | Global | (Mobility) Multiple types of migration. (Climate) Multiple climate-hazards. (Health) Mortality from climate-sensitive diseases, vector-borne disease, health (together with food, water, ecosystem services). | Modelling |
| Gautam (2017) [58] | Seasonal Migration and Livelihood Resilience in the Face of Climate Change in Nepal | Nepal | (Mobility) Seasonal migration, labour migration. (Climate) Drought, rainfall variability. (Health) Food insecurity. | Mixed Methods **** |
| Haque, Parr, Muhidin (2019) [59] | Parents’ healthcare-seeking behavior for their children among the climate-related displaced population of rural Bangladesh | Bangladesh | (Mobility) Forced Displacement. (Climate) Multiple climate-hazards. (Health) Child health care. Parental health-seeking behaviour. | Quant. non-rand. Analytical. ***** |
| Haque, Parr, Muhidin (2020) [60] | Climate-related displacement, impoverishment and healthcare accessibility in mainland Bangladesh | Bangladesh | (Mobility) Forced Displacement. (Climate) Flood and riverbank erosion. (Health) Access to health care. Access to WASH. | Quant. non-rand. Analytical. ***** |
| Haque, Parr, Muhidin (2020) [61] | The effects of household’s climate-related displacement on delivery and postnatal care service utilization in rural Bangladesh | Bangladesh | (Mobility) Forced Displacement. (Climate) Multiple climate-hazards. (Health) Delivery at a health centre. Post-natal care service utilization. | Quant. non-rand. Analytical. ***** |
| Heaney and Winter (2016) [62] | Climate-driven migration: an exploratory case study of Maasai health perceptions and help-seeking behaviour | Tanzania | (Mobility) Rural - urban migration. (Climate) Drought. (Health) Help seeking behaviour, health care utilisation, food insecurity, water insecurity. | Qualitative; Case study with interviews. ***** |
| Hori and Schafer (2010) [63] | Social costs of displacement in Louisiana after Hurricanes Katrina and Rita | Louisiana, USA | (Mobility) Forced Displacement/evacuation. (Climate) Hurricane. (Health) Access to primary health care. | Quant. non-rand. Cross-sectional retrospective. *** |
| Hunter and Simon (2017) [64] | Might climate change the “healthy migrant” effect? | Mexico & USA | (Mobility) International migration. (Climate) Rainfall variability. (Health) Self-assessed health, adult height (early life nutritional & health conditions). | Quant. non-rand. Retrospective. ** |
| Hutton and Haque (2003) [65] | Patterns of Coping and Adaptation Among Erosion-Induced Displacees in Bangladesh: Implications for Hazard Analysis & Mitigation | Bangladesh | (Mobility) Forced displacement. (Climate) Riverbank erosion. (Health) Psychological distress. | Quant. desc. * |
| Hutton and Haque (2004) [66] | Human Vulnerability, Dislocation and Resettlement: Adaptation Processes of River-bank Erosion-induced Displacees in Bangladesh | Bangladesh | (Mobility) Involuntary migration, erosion-induced displacement, rural-urban migration. (Climate) Flooding/river-bank erosion. (Health) Health problems, household hunger. | Quant. desc. *** |
| Iqbal, Donjadee… Liu (2018) [67] | Farmers perceptions of and adaptations to drought in Herat Province, Afghanistan | Herat province, Afghanistan | (Mobility) Labour migration. (Climate) Drought. (Health) Food insecurity, malnutrition. | Quant. desc. **** |
| Islam and Hasan (2016) [68] | Climate-induced human displacement: a case study of Cyclone Aila in the south-west coastal region of Bangladesh | Bangladesh | (Mobility) Forced displacement. (Climate) Cyclone. (Health) Food insecurity, malnutrition. | Mixed Methods * |
| Islam, Sallu… Paavola (2014) [69] | Migrating to tackle climate variability and change? Insights from coastal fishing communities in Bangladesh | Bangladesh | (Mobility) Rural – Urban migration (Island to mainland). (Climate) Climate variability. (Health) Physical fitness, access to WASH. | Mixed Methods *** |
| Jacobson (2019) [70] | When is migration a maladaptive response to climate change? | Cambodia | (Mobility) Migration. (Climate) Rainfall variability, drying, increased mean average temperature. (Health) Food security. | Quant. desc. ***** |
| Kabir, Rahman… Milton (2016) [71] | Climate change and health in Bangladesh: a baseline cross-sectional survey | Bangladesh | (Mobility) Forced displacement. (Climate) Cyclones, floods, salinity. (Health) Infectious diseases, malaria, dengue, pneumonia, diarrhoea, height & weight, access to health care facilities. | Quant. non-rand. ** |
| Loebach and Korinek (2019) [72] | Disaster vulnerability, displacement, and infectious disease: Nicaragua and Hurricane Mitch | Nicaragua | (Mobility) Forced displacement. (Climate) Hurricane. (Health) Infectious disease. | Quant. non-rand. ***** |
| Loevinsohn (2015) [73] | The 2001-03 Famine and the Dynamics of HIV in Malawi: A Natural Experiment | Malawi | (Mobility) Rural—urban migration. (Climate) Change change and variability. (Health) HIV. | Quant. desc. Retrospective natural experiment **** |
| Low, Frederix… Schwitters (2019) [74] | Association between severe drought & HIV prevention & care behaviors in Lesotho: A population-based survey | Lesotho | (Mobility) Internal, labour and circular migration. (Climate) Drought. (Health) HIV. | Quant. desc. ***** |
| McElfish, Moore… Peter (2016) [75] | Social Ecology and Diabetes Self-Management among Pacific Islanders in Arkansas | Arkansas, USA | (Mobility) Migration. Climate Change. (Health) Type 2 diabetes (language, translation, treatment, diabetes self-management). | Qualitative; Case study ***** |
| Mertz, Mbow… Diouf (2009) [76] | Farmers’ Perceptions of Climate Change and Agricultural Adaptation Strategies in Rural Sahel | Senegal (savanna) | (Mobility) Migration. (Climate) Climate variability (wind, rain, dust storms). (Health) Health, reduced solidarity. | Qualitative; Focus group ***** |
| Messias and Lacy (2007) [77] | Katrina-Related Health Concerns of Latino Survivors and Evacuees | USA | (Mobility) Evacuation. (Climate) Hurricane. (Health) Hunger, environmental health risks, sleep disturbance, access to healthcare. | Qualitative; Narrative research ***** |
| Milan and Ruano (2014) [78] | Rainfall variability, food insecurity and migration in Cabricán, Guatemala | Guatemala | (Mobility) Seasonal & permanent migration. (Climate) Rainfall variability. (Health) Food security (threat of local livelihoods). | Qualitative; Narrative research **** |
| Molla, Mollah… Tomomi (2014) [79] | Quantifying disease burden among climate refugees using multidisciplinary approach: A case of Dhaka, Bangladesh | Dhaka, Bangladesh | (Mobility) Migration. (Climate) Flood/river erosion, drought. (Health) DALYs los, diarrhea, asthma, morbidity. | Quant. desc. ***** |
| Molla, Mollah...Ramasoota (2014) [80] | Multidisciplinary household environmental factors: Influence on DALYs lost in climate refugees community | Dhaka, Bangladesh | (Mobility) Migration. (Climate) Flood/river erosion, drought. (Health) DALYs lost, diarrhea, asthma. | Quant. desc. *** |
| Murali and Afifi (2014) [81] | Rainfall variability, food security and human mobility in the Janjgir-Champa district of Chhattisgarh state, India | Chhattisgarh state, India | (Mobility) Seasonal & permanent migration. (Climate) Rainfall variability. (Health) Food insecurity, living quality in the city. | Mixed Methods; Case Study & Survey **** |
| Nawrotzki, Schlak and Kugler (2016) [82] | Climate, migration, and the local food security context: introducing Terra Populus | Burkina Faso & Senegal | (Mobility) International migration. (Climate) Heat waves, droughts, floods. (Health) Food security, child stunting & wasting. | Quant. desc. ***** |
| Oyekale, Oladele and Mukela (2013) [83] | Impacts of flooding on coastal fishing folks and risk adaptation behaviours in Epe, Lagos State | Nigeria | (Mobility) Migration. (Climate) Flooding. (Health) Malaria, typhoid, cholera, diarrhea, dysentery, influenza, tuberculosis. | Quant. desc. ** |
| Pardi, Jungari…Bomble (2020) [84] | Migrant motherhood: Maternal and child health care utilization of forced migrants in Mumbai, Maharashtra, India | India | (Mobility) Forced Migration. (Climate) Drought. (Health) Maternal Child Health care utilisation, immunisation. | Qualitative * |
| Penning-Rowsell… Thompson (2013) [85] | The ‘last resort’? Population movement in response to climate-related hazards in Bangladesh | Bangladesh | (Mobility) Temporary evacuation. (Climate) Hazard events & disasters. (Health) Ill-health, lack of space & hygiene. | Qualitative *** |
| Perez-Saez, King… Pascual (2017) [86] | Climate-driven endemic cholera is modulated by human mobility in a megacity | Dhaka, Bangladesh | (Mobility) Urban migration. (Climate) El Nino Southern Oscillation (ENSO). (Health) Cholera. | Modelling |
| Philibert, Tourigny… Fournier (2013) [87] | Birth seasonality as a response to a changing rural environment (Kayes Region, Mali) | Mali | (Mobility) Seasonal migration. (Climate) Climate and rainfall. (Health) Births registered in primary health care facilities. | Quant. desc. **** |
| Rademacher-Schulz… Mahama (2014) [88] | Time matters: shifting seasonal migration in Northern Ghana in response to rainfall variability and food insecurity | Northern Ghana | (Mobility) Seasonal & labour migration. (Climate) Rainfall variability. (Health) Livelihood, food security. | Mixed Methods * |
| Rahaman, Rahman... Hassan (2018) [89] | Health Disorder of Climate Migrants in Khulna City: An Urban Slum Perspective | Khulna City, Bangladesh | (Mobility) Slum migration. (Climate) Climatic disasters (flooding, cyclone, storm surges, sea level rise, river erosion). (Health) Waterborne diseases, undernutrition, micronutrient deficiencies, diarrhea, malaria. | Qualitative ** |
| Rakib, Sasaki…Fukunaga (2019) [90] | Severe salinity contamination in drinking water and associated human health hazards increase migration risk in the southwestern coastal part of Bangladesh | Bangladesh | (Mobility) Migration. (Climate) Sea level rise - Groundwater salinization. (Health) Hypertension, Cardiovascular disease, Renal disease, Diarrhoea, Respiratory disease, Skin disease, Access to healthcare and cost of healthcare. | Mixed Methods *** |
| Roncoli, Ingram and Kirshen (2001) [91] | The costs and risks of coping with drought: livelihood impacts and farmers’ responses in Burkina Faso | Burkina Faso | (Mobility) Migration. (Climate) Scarce and irregular rainfall, infertile and degraded soils, drought. (Health) Livelihood, food security. | Mixed Methods ** |
| Shanthi, Mahalakshimi and Chandrasekaran (2017) [92] | Assessment of challenges faced by the coastal women due to the impact of climatic change in selected coastal districts of Tamil Nadu, India | Tamil Nadu, India | (Mobility) Urban migration. (Climate) Unusual rainfall, floods, cyclones, change in water quality. (Health) Livelihood, health. | Quant. desc. *** |
| Suckall, Fraser and Forster (2017) [93] | Reduced migration under climate change: evidence from Malawi using an aspirations and capabilities framework | Malawi | (Mobility) Internal migration. (Climate) Climate stresses (droughts) and shocks (sudden flooding). (Health) Food shortage. | Mixed Methods * |
| Taiban, Lin and Ko (2020) [94] | Disaster, relocation, & resilience: recovery and adaptation of Karamemedesane in Lily Tribal Community after Typhoon Morakot, Taiwan | Taiwan | (Mobility) Forced Relocation. (Climate) Typhoon. (Health) Food security (food sovereignty), cultural preservation (social capital, mental health). | Qualitative. In-dept interviews and participant observation. *** |
| Tschakert, Tutu and Alcaro (2013) [95] | Embodied experiences of environmental and climatic changes in landscapes of everyday life in Ghana | Ghana | (Mobility) Rural - urban migration. (Climate) Environmental and climatic change (unpredictable and shifting rainfall). (Health) Well-being, distress. | Qualitative; Phenomenology ***** |
| Van der Geest, Nguyen and Nguyen (2014) [96] | Internal migration in the upper mekong delta, viet nam: what is the role of climate related stressors? | Vietnam | (Mobility) Internal migration. (Climate) Climate-related stressors (floods, storms, rainfall). (Health) Food insecurity. | Mixed Methods *** |
| Van der Geest, Burkett... Wheeler (2020) [97] | Climate change, ecosystem services and migration in the Marshall Islands: are they related? | Marshall Islands | (Mobility) International migration. (Climate) Sea-level rise, drought, extreme heat. (Health) Access to healthcare, Water security. | Mixed Methods **** |
| Warner and Afifi (2014) [98] | Where the rain falls: Evidence from 8 countries on how vulnerable households use migration to manage the risk of rainfall variability and food insecurity | Guatemala, Peru, Ghana, Tanzania, Bangladesh, India, Thailand & Vietnam | (Mobility) Migration. (Climate) Rainfall variability. (Health) Food insecurity (food production & market food availability). | Mixed Methods **** |
| Wolsko and Marino (2016) [99] | Disasters, migrations, and the unintended consequences of urbanization: What’s the harm in getting out of harm’s way? | Shishmaref, Alaska | (Mobility) Planned relocation. (Climate) Erosion, wind, ice melt, floods. (Health) Mental health status. | Qualitative; Ethnography ** |
| Woodhall-Melnik and Grogan (2019) [100] | Perceptions of mental health & wellbeing following residential displacement & damage from the 2018 St. John River Flood | Canada | (Mobility) Residential displacement. (Climate) Flood. (Health) Mental health, well-being. | Qualitative ***** |
| Zaman, Sammonds… Rahman (2020) [101] | Disaster risk reduction in conflict contexts: Lessons learned from the lived experiences of Rohingya refugees in Cox’s Bazar, Bangladesh | Bangladesh | (Mobility) Forced displacement. Trapped populations. (Climate) Landslides, tropical cyclones, flash-flooding. (Health) Infectious disease outbreaks. Access to healthcare. Food and water security. | Mixed Methods *** |
| Theme | Illustrative Quote |
|---|---|
| 1. Avoid the universal promotion of migration as an adaptive response to climate risks. Prevent forced migration by investing in climate change adaptation, disaster risk reduction and sustainable development. Consider planned relocation as a last resort. | ‘The policy implication is that governments should not make assumptions a priori about whether a location is undesirable and promote migration as a blanket solution to the negative impacts of climate change’—Quantitative descriptive, Peru [12]. |
| 2. Preserve cultural and social ties of mobile populations. Strengthen governance of socio-ecological systems. | ‘Developing government frameworks that can draw on the strengths of the community-led approaches to relocation whilst also providing a mechanism for communities to stay intact will be an important step forwards for Small Island Developing States (SIDs) facing these climate pressures’—Qualitative case studies, Alaska & Solomon Islands [40]. |
| 3. Enable participation of migrants in their sites of relocation and resettlement. Support the self-sufficiency of both incoming and host communities by supporting new livelihoods, developing social networks, and integrating cultural considerations. | ‘As to the migrants, their value added to the areas of destination should be maximized by involving them in activities that match their skills (e.g., farming and construction), so that they actively contribute to the overall welfare of the new areas on one hand and to the well-being of themselves and their families on the other’—Mixed methods, Tanzania [38]. |
| 4. Strengthen health systems and reduce barriers for migrants to access health care. | ‘Relocation of local health facilities with basic and emergency care provisions to areas in which the displaced have resettled, reinforcement of Family Planning services, and extension of coverage of the Maternity Allowance benefits in the displacement prone mainland riverine areas are recommended policy responses’—Cross sectional survey, Bangladesh [59]. |
| 5. Provide migrants with the requirements and the determinants for good health. | ‘The rights of these displaced people, including the right to health, are often poorly protected in practice. More vigorous application of existing human instruments is needed, as well as clarification and possibly re-definition of the rights of those displaced’—Qualitative study, Bangladesh [89]. |
| 6. Integrate health into loss and damage assessments. Consider people at higher risk, including those that are immobile or trapped. | ‘The findings outlined a long line of climate-induced non-economic losses and damages that people faced through the rural-urban move from the island, and through the displacement in the slum. These included the loss of identity, honour, sense of belonging, physical and mental health or wellbeing’—Mixed Methods, Bangladesh [32]. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nayna Schwerdtle, P.; Stockemer, J.; Bowen, K.J.; Sauerborn, R.; McMichael, C.; Danquah, I. A Meta-Synthesis of Policy Recommendations Regarding Human Mobility in the Context of Climate Change. Int. J. Environ. Res. Public Health 2020, 17, 9342. https://doi.org/10.3390/ijerph17249342
Nayna Schwerdtle P, Stockemer J, Bowen KJ, Sauerborn R, McMichael C, Danquah I. A Meta-Synthesis of Policy Recommendations Regarding Human Mobility in the Context of Climate Change. International Journal of Environmental Research and Public Health. 2020; 17(24):9342. https://doi.org/10.3390/ijerph17249342
Chicago/Turabian StyleNayna Schwerdtle, Patricia, Julia Stockemer, Kathryn J. Bowen, Rainer Sauerborn, Celia McMichael, and Ina Danquah. 2020. "A Meta-Synthesis of Policy Recommendations Regarding Human Mobility in the Context of Climate Change" International Journal of Environmental Research and Public Health 17, no. 24: 9342. https://doi.org/10.3390/ijerph17249342